
Abstract
Disturbed grief, operationalized as persistent complex bereavement disorder (PCBD), correlates with yet differs from posttraumatic stress disorder (PTSD) and depression symptoms. However, knowledge about temporal associations among these symptoms is limited. We aimed to enhance our understanding of the etiology of loss-related distress by examining temporal associations among PCBD, PTSD, and depression symptom levels. Dutch people (N = 172) who lost significant other(s) in a plane disaster completed questionnaires for PCBD, PTSD, and depression 11, 22, 31, and 42 months after the disaster. Cross-lagged analyses revealed that changes in PCBD symptom levels have a greater impact on changes in symptom levels of PTSD and depression than vice versa. Our findings contradict the notion that PTSD and depression symptoms should be addressed before grief in treatment. Pending replication of our findings in clinical samples, we tentatively conclude that screening and treatment of grief symptoms has potential value in preventing long-lasting distress.
Persistent complex bereavement disorder (PCBD) is included as condition for further study in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM–5; American Psychiatric Association, 2013). PCBD symptoms encompass grief reactions, including preoccupation with the deceased and feeling numbed since the loss, that persist for at least 1 year after the death of a significant other and cause significant impairments in functioning. A meta-analysis suggests that 9.8% of people confronted with the nonviolent loss (e.g., illness) of a significant other is at risk for developing clinically relevant grief reactions (henceforth referred to as PCBD; Lundorff, Holmgren, Zachariae, Farver-Vestergaard, & O’Connor, 2017). Experiencing the death of someone significant that happens unexpectedly and/or has a violent cause heightens the risk of PCBD and comorbid posttraumatic stress disorder (PTSD) and depression (Boelen, de Keijser, & Smid, 2015; Currier, Holland, & Neimeyer, 2006; Kaltman & Bonanno, 2003). This combination of symptoms also has been referred to as traumatic grief (Smid et al., 2015).
PCBD shares symptoms with PTSD (e.g., reexperiencing, avoidance symptoms; Maccallum & Bryant, 2019; Maercker & Znoj, 2010; Nickerson et al., 2014; O’Connor, Lasgaard, Shevlin, & Guldin, 2010) and depression (e.g., sad mood, emptiness, fatigue, and suicidal ideation; Boelen, van den Bout, & de Keijser, 2003; Boelen, Reijntjes, Djelantik, & Smid, 2016; Djelantik, Smid, Kleber, & Boelen, 2017; Maccallum, Malgaroli, & Bonanno, 2017; Shear et al., 2011). Reexperiencing symptoms in PCBD differ from those in PTSD such that for PCBD, reexperiencing comprises both positive and negative memories, whereas for PTSD, reexperiencing of negative memories is key (Maercker & Znoj, 2010). Furthermore, avoidance in PCBD serves to avert painful thoughts and feelings related to the irreversibility of the loss, whereas avoidance in PTSD is used to prevent thoughts and memories related to the traumatic event and the recurrence of threat or danger. Depression often coincides with inactivity, whereas yearning in PCBD seems to be associated with passivity as well as activity, such as searching behavior (Stroebe & Schut, 1999). In addition, a sad mood in depression is related to low self-esteem, whereas a sad mood in PCBD is related to longing for the deceased (Shear et al., 2011).
Although research has shown that some disturbed grief symptoms resemble symptoms of PTSD and depression, studies employing, for instance, factor or latent class analysis have shown that these syndromes are correlated but distinguishable (Boelen, van de Schoot, van den Hout, de Keijser, & van den Bout, 2010; Bonanno et al., 2007; Lenferink, de Keijser, Smid, Djelantik, & Boelen, 2017; Li & Prigerson, 2016; Nickerson et al., 2014; O’Connor et al., 2010). However, knowledge about the temporal associations between these symptoms is limited. Gaining more insight in these associations is important for our understanding of the etiology of postloss distress and could inform us about symptoms that need to be dealt with first in treatment of comorbid loss-related symptoms. To our knowledge, only two studies have examined associations between PCBD and PTSD symptom levels over time. One study did so using four waves of data and lower level mediation analysis in elderly spousal bereaved people (O’Connor, Nickerson, Aderka, & Bryant, 2015). Another study examined these associations in a community sample of bereaved people using two waves of data and cross-lagged panel analysis (Djelantik, Smid, Kleber, & Boelen, 2018). Findings from both studies indicated that changes in PCBD symptom levels have a greater impact on changes in PTSD symptom levels than vice versa. These findings are important in attesting to the predictive validity of PCBD and run counter to prevailing notions that in treatment of combined symptoms of grief and traumatic distress, traumatic distress needs to be targeted before disturbed grief reactions should be addressed (Lindy, Green, Grace, & Titchener, 1983; Raphael & Martinek, 1997; Sprang, 2001). However, it should be noted that both prior studies, examining reciprocal relationships, relied on nonclinical bereaved samples (Djelantik et al., 2018; O’Connor et al., 2015). Therefore, caution is warranted in generalizing these findings to clinical samples.
Although these findings are important, it is yet unclear to what extent they generalize to people who have lost a significant other as a result of a violent cause. This distinction is important given research findings suggesting that people exposed to a violent loss are over 5 times more likely to develop comorbid PCBD and PTSD reactions (vs. resilient response) than people exposed to a nonviolent loss (Djelantik et al., 2017). The temporal relationship between PCBD and depression also has not been explored in prior research; consequently, it is still unclear whether increases in PCBD symptom levels precede worsening of depression symptom levels or whether elevated depression symptom levels predict an exacerbation of grief reactions. Accordingly, we examined the reciprocal associations among symptom levels of PCBD, PTSD, and depression in a nonclinical sample of people who suffered one or multiple significant losses in a plane disaster in 2014.
Aims of the Study
We are the first to investigate the temporal relationship between self-reported PCBD and PTSD symptom levels in people exposed to a violent loss of a significant other. We expanded prior work by also exploring the reciprocal associations between PCBD and depression and the reciprocal associations among PCBD, PTSD, and depression symptom levels. In line with previous findings (Djelantik et al., 2018; O’Connor et al., 2015), we expected that changes in PCBD symptom levels would predict changes in PTSD symptom levels but not vice versa. Because no prior studies have examined the temporal associations between PCBD and depression symptom levels, no specific hypotheses were formulated regarding these associations over time.
Method
Participants
The MH17 disaster took place on July 17, 2014. In total, 298 people were on board when the airplane was shot down in Ukrainian airspace. All people, including 193 Dutch people, died. Dutch adult people who had lost one or multiple family member(s) and/or friend(s) in this disaster were invited to take part in this longitudinal online survey study. Four waves of data are included in this study. One prior study based on these four waves of data has been published, in which we used latent class growth modeling to examine individual differences in longitudinal symptom profiles (Lenferink, Nickerson, de Keijser, Smid, & Boelen, 2018). People were recruited using a variety of strategies, including invitations sent by peer support and governmental support organizations, media attention, and snowball sampling (for details, see our earlier work; Lenferink et al., 2017).
In total, 172 people completed at least one wave and were included in the analyses. The majority of the participants were women (n = 102, 59.3%), and about two thirds (n = 117, 68.4%) had at least a university degree. The participants’ mean age at the time the disaster took place was 51.55 (SD = 15.51) years. Fifty-four people (31.8%) lost one significant other. Most people lost multiple significant others; 58 people (34.1%) lost two, 22 people (12.9%) lost three, 32 (18.8%) lost four, 2 people (1.2%) lost five, and 2 people (1.2%) lost six significant others. Regarding relationship to the deceased, for people who suffered multiple losses, the most intimate relationship to the deceased was reported here, ordered from child, through spouse, through parent, through sibling, through other not previously specified significant other (see Lenferink et al., 2017). Forty-eight people (28.4%) lost at least a child, 2 people (1.2%) lost at least a spouse, 15 people (8.9%) lost at least a parent, 48 people (28.4%) lost at least a sibling, 30 people (17.8%) lost at least another family member, 12 people (7.1%) lost at least a friend, and 14 people (8.3%) lost other than spouse, family member, or a friend (e.g., neighbor or colleague). The mean PCBD, PTSD, and depression scores fell within the subclinical range (see Table 1; for more details about clinical cutoffs, see Lenferink et al., 2018).
Means, Standard Deviations, and Correlations of PCBD, PTSD, and Depression Symptom Levels at W1 to W4
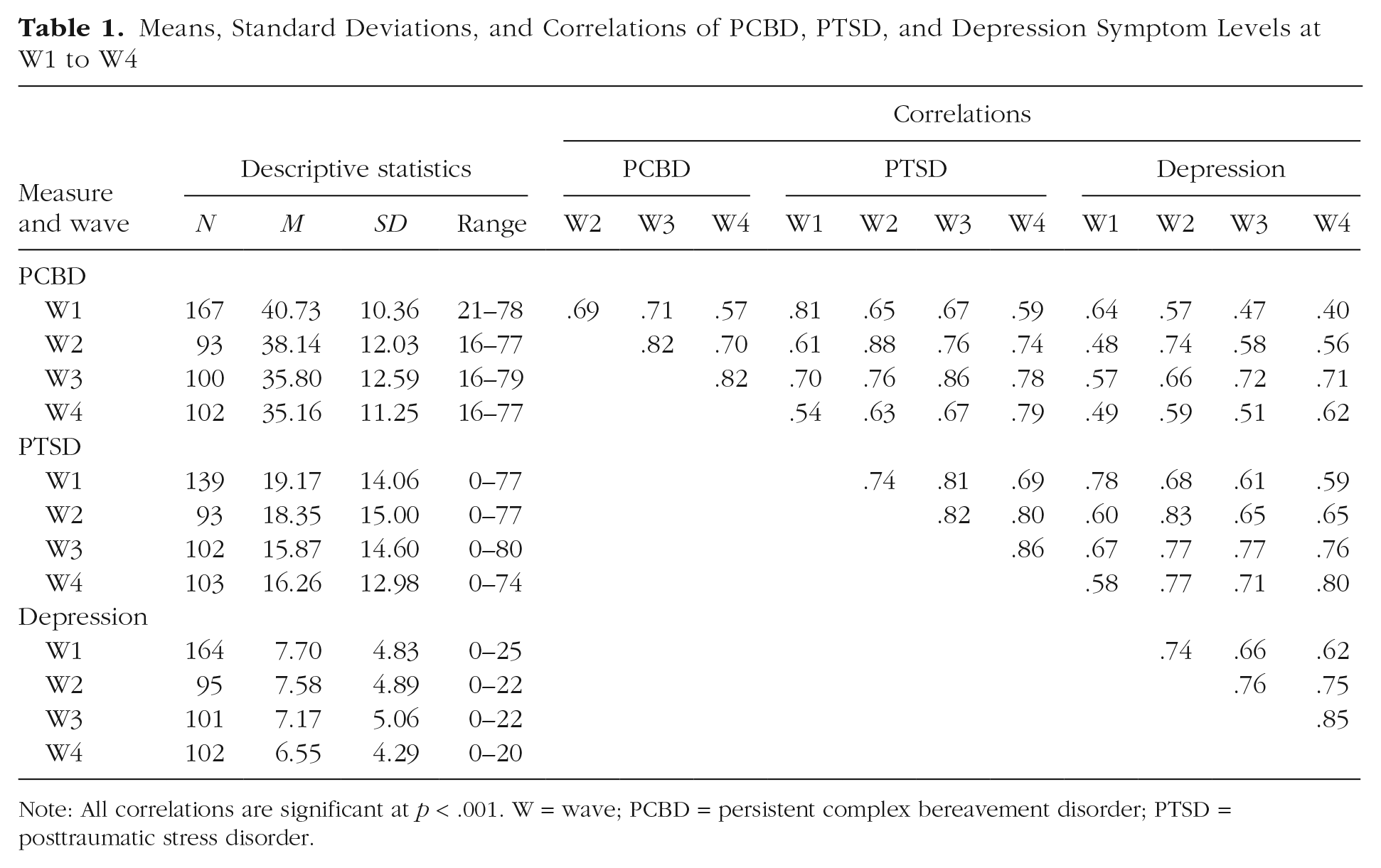
Note: All correlations are significant at p < .001. W = wave; PCBD = persistent complex bereavement disorder; PTSD = posttraumatic stress disorder.
Procedures
The first assessment (referred to as Wave 1, or W1) took place from May 2015 through January 2016. The second assessment (W2) took place from April 2016 through December 2016. The third assessment (W3) took place from February 2017 through May 2017. The fourth assessment (W4) took place from January 2018 through March 2018. The mean time since loss was 10.73 months (SD = 1.77) for W1, 21.91 months (SD = 1.47) for W2, 31.31 months (SD = 0.98) for W3, and 41.66 months (SD = 0.59) for W4. In total, 66 participants (38.4%) completed all four waves. A local ethical board approved this study. All participants provided written informed consent.
Measures
PCBD symptoms as defined in DSM–5 (American Psychiatric Association, 2013) were assessed with 16 items of the 18-item Traumatic Grief Inventory–Self Report (TGI-SR; Boelen & Smid, 2017). The frequency of each symptom (e.g., “I had trouble accepting the loss”) during the previous month was rated on a scale ranging from 1 (never) through 5 (always). In the instruction, we referred to “the loss of your loved one(s) because of the plane crash” as the anchor event. Total score ranged from 16 to 80. The TGI-SR has adequate psychometric properties (Boelen, Djelantik, de Keijser, Lenferink, & Smid, 2019; Boelen & Smid, 2017). Cronbach’s αs in the current study were greater than .88 for each wave.
PTSD symptoms as per DSM–5 (American Psychiatric Association, 2013) were assessed 1 with the 20-item PTSD Checklist for DSM–5 (PCL-5; Blevins, Weathers, Davis, Witte, & Domino, 2015; Boeschoten, Bakker, Jongedijk, & Olff, 2014). Participants rated to what extent they experienced each symptom (e.g., “In the past month, how much were you bothered by: ‘Trouble remembering important parts of the stressful experience?’”) during the preceding month, on a scale ranging from 0 (not at all) through 4 (extremely). In the instruction, we referred to “the loss of your loved one(s) because of the plane crash” as the anchor event. The PCL-5 has adequate psychometric properties (Blevins et al., 2015; Krüger-Gottschalk et al., 2017). Cronbach’s αs in the current study were greater than .91 for each wave.
Symptoms of depression were assessed with the 16-item Quick Inventory of Depressive Symptomatology–Self Report (QIDS-SR; Rush et al., 2003). The frequency of each symptom (e.g., “Feeling irritable”) during the preceding 7 days was rated on scales with four answer options ranging from 0 through 3. 2 As recommended by Rush et al. (2003), the nine items were summed to yield a total depression score. Psychometric properties of the QIDS-SR are adequate (Rush et al., 2003). Cronbach’s αs in the current study were greater than .75 for each wave.
Statistical analyses
Three series of cross-lagged panel models were conducted, using Mplus Version 8 (Muthén & Muthén, 2017), to test the reciprocal relationships among symptom levels of PCBD, PTSD, and/or depression (represented by summed scores on the TGI-SR, PCL-5, and QIDS-SR, respectively) across the four waves. In the first round of analyses, we included only PCBD and PTSD data, the second round focused on PCBD and depression data only, and the third round included PCBD, PTSD, and depression data. Each cross-lagged model consisted of autoregressive paths to take into account symptom persistence over time (e.g., the associations between PCBD symptom levels at W1, W2, W3, and W4). On the basis of previous research (Boelen et al., 2010; Bonanno et al., 2007), we also took into account associations among PCBD, PTSD, and depression symptom levels at each wave by allowing these distress measures to correlate in the model (e.g., PCBD at W1 with PTSD at W1 in the first round of analyses). Cross-lagged effects were estimated to test the predictive effect of a distress measure at one wave (e.g., symptom levels of PCBD at W1) to the other distress measure at a subsequent time point (e.g., symptom levels of PTSD at W2) while controlling for the autoregressive effects and associations among the distress measures at each wave.
In accord with recommendations put forth by Little (2013), the most parsimonious cross-lagged model was preferred (i.e., a model with reduced set of estimated parameters that fits the data well). We therefore compared the statistical fit of the unconstrained model (Model 1) with increasingly constrained models (i.e., assuming associations are equal) in consecutive steps. In Model 2, we constrained the autoregressive paths to be equal for the distress measures separately. In Model 3, we constrained the autoregressive paths plus the cross-lagged effects of PCBD on PTSD and depression and of PTSD and depression on PCBD, and in the last round of analyses of PTSD on depression and of depression on PTSD, to be equal. In Model 4, we also constrained the associations between the distress measures at the same wave to be equal across the waves. Selection of the most parsimonious model was based on the following fit statistics: root mean square error of approximation (RMSEA) values less than .08 represent acceptable fit and those .05 represent excellent fit and comparative fit index (CFI) and Tucker-Lewis index (TLI) values greater than .90 indicate acceptable fit. In a final round of analyses, we added covariates to the final models simultaneously by regressing the baseline symptom levels on these covariates. On the basis of a systematic review and meta-analysis from Heeke, Kampisiou, Niemeyer, and Knaevelsrud (2019), we included gender (0 = man, 1 = woman), kinship to the deceased (0 = other than child/spouse, 1 = child/spouse), and educational level (0 = lower than university, 1 = university) as covariates. Missing data on symptom levels of PCBD, PTSD, and depression were handled using full information maximum likelihood estimation. All significance tests were two-tailed (α = .05).
Results
Preliminary analyses
Participants who completed W1 but did not complete W2, W3, or W4 did not significantly differ from those who did complete these waves in terms of background characteristics, except that those who did not complete W2, W3, or W4 were more distantly related to the deceased than those who did complete these waves. There were also no significant differences in symptom levels of PCBD and PTSD. However, participants who did not complete W3 and W4 had lower depression levels than those who did complete these waves (see our prior work for more details; Lenferink et al. 2018).
Table 1 shows means, standard deviations, and score ranges of and correlations among symptom levels at all waves. PCBD, PTSD, and depression symptoms were significantly and positively correlated at each time point.
Cross-lagged models
The fit indices of each cross-lagged model are shown in Table S1 in the Supplemental Material available online. The models in which we constrained both the autoregressive and cross-lagged effects to be equal (Model 3) yielded the best fit, as indicated by the lowest RMSEA values and acceptable CFI and TLI values, and were therefore selected as our final models.
Temporal associations among symptom levels of PCBD, PTSD, and depression
Figures 1, 2, and 3 show the standardized autoregressive and cross-lagged effects of the final models. In Table S2 in the Supplemental Material, the unstandardized final model results are shown. PCBD symptom levels significantly predicted PTSD symptom levels at a subsequent time point but not vice versa (see Fig. 1). PCBD symptom levels significantly predicted depression symptom levels at a subsequent time point but not vice versa (see Fig. 2). Figure 3 shows that PCBD and depression symptom levels significantly predicted PTSD symptom levels at a subsequent time point. PTSD symptom levels significantly predicted depression symptom levels at a subsequent time point. PTSD and depression symptom levels did not significantly predict PCBD symptom levels at a subsequent time point. In an additional round of analyses, we included the covariates gender, educational level, and kinship to the deceased into the cross-lagged models. This analysis did not lead to meaningful differences in the results, namely, the same significant cross-lagged effects were found. 3

PCBD and PTSD symptoms over time: standardized autoregressive and cross-lagged effects. Correlations between symptoms at same wave are not shown. Dashed lines represent nonsignificant associations. PCBD = persistent complex bereavement disorder; PTSD = posttraumatic stress disorder. Asterisks indicate significant associations (*p < .05, **p < .01, ***p < .001).

PCBD and depression symptoms over time: standardized autoregressive and cross-lagged effects. Correlations between symptoms at same wave are not shown. Dashed lines represent nonsignificant associations. PCBD = persistent complex bereavement disorder. Asterisks indicate significant associations (*p < .05, **p < .01, ***p < .001).
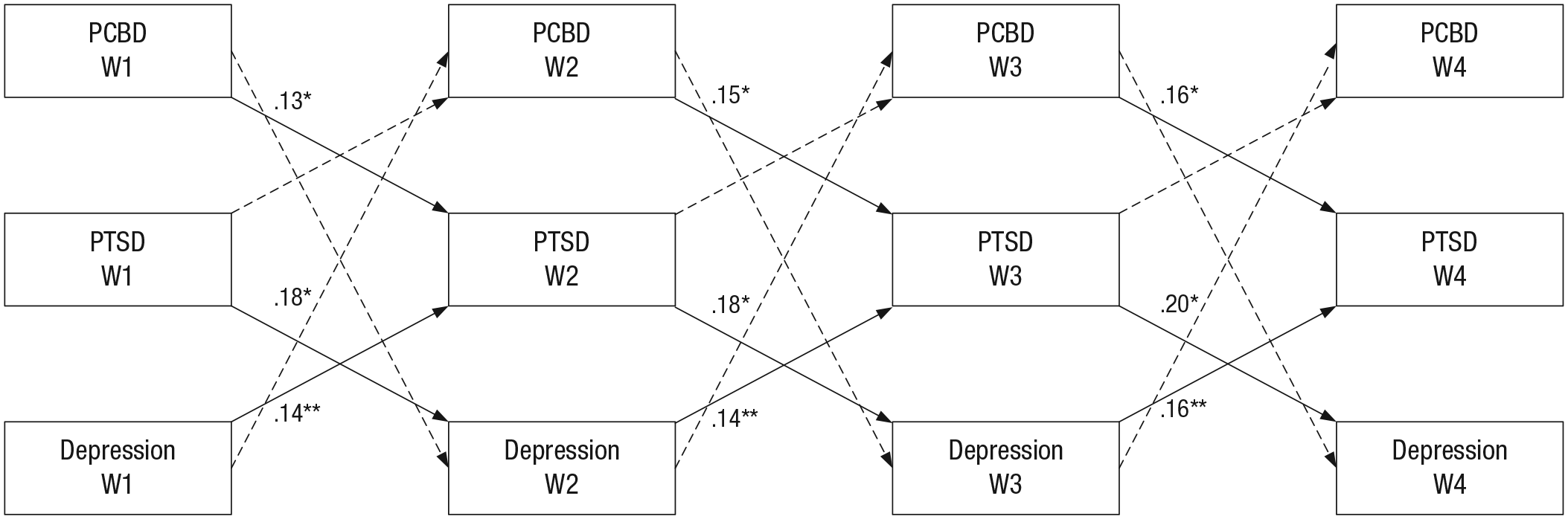
PCBD, PTSD, and depression symptoms over time: standardized cross-lagged effects. Autoregressive effects and correlations among symptoms at same wave are not shown. Dashed lines represent nonsignificant associations. PCBD = persistent complex bereavement disorder; PTSD = posttraumatic stress disorder. Asterisks indicate significant associations (*p < .05, **p < .01, ***p < .001).
Discussion
In this study, we examined temporal associations, using four waves of self-report questionnaire data, among symptom levels of PCBD, PTSD, and depression in people who experienced the loss of significant others because of a plane disaster. A first main finding was that symptom levels of PCBD predicted PTSD symptom levels, whereas conversely, PTSD symptom levels did not predict PCBD symptom levels. This finding accords with results from two prior recent studies (Djelantik et al., 2018; O’Connor et al., 2015). Although these prior studies mostly relied on people who experienced a nonviolent death, used different time intervals between the measurement occasions, and used different instruments to tap PCBD and PTSD (Djelantik et al., 2018; O’Connor et al., 2015), the consistency between our findings and these prior studies supports the robustness of these findings. Although our significant cross-lagged effects were relatively small, our findings run counter to frequently cited claims that symptoms of traumatic distress that may emerge following loss block the alleviation of symptoms of grief (Lindy et al., 1983; Raphael & Martinek, 1997; Sprang, 2001). However, our study, as well as prior studies examining reciprocal associations between psychopathology symptom levels (Djelantik et al., 2018; O’Connor et al., 2015), were not focused exclusively on bereaved people with clinically relevant psychopathology levels. Pending replication of the findings in clinical samples, caution should be applied in generalizing our findings to clinical samples.
Expanding on prior work, ours was the first to study temporal associations between PCBD and depression symptom levels. These associations mirrored the outcomes of the analyses with symptoms of PCBD and PTSD such that results indicated that PCBD symptom levels significantly predicted depression symptom levels later in time, whereas depression symptom levels did not predict subsequent PCBD symptom levels. This finding complements treatment studies indicating that grief-specific treatment effectively reduces PCBD and depression symptom levels, whereas depression-based treatments, such as interpersonal psychotherapy or use of antidepressants, are less effective in reducing PCBD symptom levels (Reynolds et al., 1999; Shear et al., 2014). Furthermore, the finding that PCBD symptoms predicted depression symptoms contradicts claims that alleviation of depressive symptoms enables bereaved people to grieve more effectively (Zisook, Shuchter, Pedrelli, Sable, & Deaciuc, 2001).
We also found that PCBD symptoms no longer predicted depression symptoms at a subsequent time point once PTSD symptoms were taken into account in the last round of analyses. In general, prior research also has shown that taking multiple outcomes into account may yield a greater understanding of psychological responses after bereavement than studies examining a limited number of possible responses (Infurna & Luthar, 2017; Lenferink et al., 2018). More specifically, this result suggests that PTSD symptoms rather than PCBD symptoms predict depression symptoms over time. Yet, we also found that PCBD and depression symptoms predicted PTSD symptoms, whereas PTSD symptoms also predicted depression symptoms at consecutive waves of assessment. The bidirectional associations between PTSD and depression symptoms over time also has been found in people exposed to stressful events other than traumatic losses (Cheng, Liang, Fu, & Liu, 2018; Horesh, Lowe, Galea, Uddin, & Koenen, 2015). Consequently, our findings may indicate that an increase in PCBD symptoms predicts worsening of an intertwined cluster of PTSD and major depressive disorder symptoms over time. Our study yielded no evidence that PTSD and depression symptom levels predict later PCBD symptom levels in the first 3 to 4 years after the traumatic loss of significant others. These findings offer first evidence suggesting that it might be relevant to focus more on PCBD rather than PTSD and depression in screening and treating psychopathology among people heading toward the first anniversary of the unnatural death of a loved one. When our findings are replicated in clinical samples, that finding would suggest that identification and treatment of elevated PCBD severity in this period may help to prevent the exacerbation of PTSD and depression levels at later periods in the bereavement process.
For each round of analyses, we found that constraining the autoregressive and cross-lagged effects to be equal across the waves yielded the best statistical fit. This finding indicates that over time, the predictive value of prior symptom levels remains quite stable on average. In other words, it seems unlikely that the strength of the temporal associations among PCBD, PTSD, and depression change in the first 4 years after the traumatic loss of a significant other.
The finding that increased PCBD symptoms seem to precede increases in PTSD and depression symptoms (and not vice versa, as has been argued previously; Lindy et al., 1983; Raphael & Martinek, 1997; Sprang, 2001; Zisook et al., 2001) might be explained from at least two theoretical perspectives. First, from the perspective of stress sensitization theory, it could be argued that over time, people become more sensitized to stress after confrontation with a life stressor. In other words, levels of stress needed to trigger onset of affective symptoms dramatically decrease after each trigger (Monroe & Harkness, 2005; Post, 2016; Stroud, 2018). From this perspective, bereaved people with elevated PCBD levels might be more prone to experience a worsening of PTSD and depression symptoms after confrontation with loss-related stimuli (Smid et al., 2015). For instance, the plane disaster that caused the death of their loved one(s) in the current sample has repeatedly received media attention, which in turn could have led to elevated distress levels (Neria et al., 2007; van der Velden, van der Meulen, Lenferink, & Ijzermans, 2018). Exposure to these stressors might be particularly harmful for those with elevated PCBD symptoms. Second, from the perspective of cognitive-behavioral models of disturbed grief (Boelen, van den Hout, & van den Bout, 2006), it could be argued that persistent yearning for the lost person’s presence and difficulties accepting his or her absence keep the person away from processing the most distressing and traumatizing features of the circumstances of the loss and consequently maintain PTSD symptoms (e.g., intrusive memories) resulting from the insufficiently processed memories of the circumstances (Boelen, 2010, 2017). Integration of information about the loss, including the relationship with the deceased and the loss-related thoughts, memories, and feelings, with existing autobiographical knowledge has been argued to be critical for recovery from loss from a cognitive-behavioral perspective (Boelen et al., 2006). From this same cognitive-behavioral perspective, avoidance of social and occupational activities out of the belief that they are not fulfilling anymore since the loss (i.e., depressive avoidance) might play a role (Boelen & van den Bout, 2010). That is, over time, social withdrawal may fuel depressive symptoms (Hong, Hasche, & Bowland, 2009). Consequently, those who have more difficulty in reengaging in meaningful social activities after the plane disaster might be more at risk to develop elevated depression symptoms.
Several limitations need to be kept in mind while interpreting our findings. In the current study, we focused on PCBD levels according to the DSM–5 (American Psychiatric Association, 2013). Findings from recent studies suggest that PCBD per DSM–5 and prolonged grief disorder (PGD) as defined in the 11th edition of the International Classification of Diseases (ICD-11; World Health Organization, 2018) perform differently when it comes to identification of clinical cases as well as concurrent and prospective validity (Boelen, Lenferink, Nickerson, & Smid, 2018; Maciejewski, Maercker, Boelen, & Prigerson, 2016; Mauro et al., 2017). Therefore, our findings do not necessarily generalize to disturbed grief as represented by PGD ICD-11 criteria. Furthermore, the majority of our sample was exposed to multiple losses simultaneously caused by a man-made disaster, and most people were highly educated and reported subclinical psychopathology levels. These demographics limit the generalizability to people confronted with other types of loss and with lower educational levels and clinical levels of psychopathology. Lastly, we used self-report questionnaire data instead of clinical diagnostic interviews. As a result, we were unable to formally diagnose PCBD, PTSD, and depression. Furthermore, because we used self-report questionnaire data, the reported symptom levels might be overestimated (see Engelhard et al., 2007).
Notwithstanding these limitations, our findings show that changes in PCBD levels in people exposed to a traumatic loss 3 to 4 years earlier precede change in PTSD and depression levels and not vice versa. This finding runs counter to the widely held notion in the literature on grief treatment that PTSD and depression symptoms interfere with (and thus precede) grief reactions and that among people getting stuck in recovery from loss, these symptoms should be addressed before targeting the grief. When our findings are replicated in clinical bereaved samples, our findings point to the value of screening and treatment of PCBD symptoms after the violent loss of a significant other in preventing long-lasting comorbid symptoms of PCBD, PTSD, and depression.
Supplemental Material
Lenferink_Supplemental_Materials – Supplemental material for Reciprocal Associations Among Symptom Levels of Disturbed Grief, Posttraumatic Stress, and Depression Following Traumatic Loss: A Four-Wave Cross-Lagged Study
Supplemental material, Lenferink_Supplemental_Materials for Reciprocal Associations Among Symptom Levels of Disturbed Grief, Posttraumatic Stress, and Depression Following Traumatic Loss: A Four-Wave Cross-Lagged Study by Lonneke I. M. Lenferink, Angela Nickerson, Jos de Keijser, Geert E. Smid and Paul A. Boelen in Clinical Psychological Science
Footnotes
Acknowledgements
We thank Eline Piersma and Daniëlle Trip for their support with data collection. We also thank Victim Support the Netherlands for their support with recruiting participants.
Action Editor
Erin B. Tone served as action editor for this article.
Author Contributions
L. I. M. Lenferink and P. A. Boelen designed the study. L. I. M. Lenferink collected the data. L. I. M. Lenferink and A. Nickerson conducted the statistical analyses. L. I. M. Lenferink and P. A. Boelen wrote the draft of the manuscript. All authors critically reviewed and improved draft versions of the manuscript. All of the authors approved the final manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared that there were no conflicts of interest with respect to the authorship or the publication of this article.
Funding
The Victim Fund subsidized this work.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.