
Abstract
Sleep-related academic impairment is a common issue among college students and may be influenced by psychological and behavioral health factors. This study used cross-sectional data from the Spring 2021 American College Health Association-National College Health Assessment III (ACHA-NCHA III) to examine whether psychological distress, loneliness, and substance use were associated with academic impairment due to sleep difficulties among U.S. college students aged 18–24 (N = 798). Logistic regression showed that psychological distress, loneliness, and elevated risk scores for alcohol and cannabis use were significantly associated with sleep-related academic impairment. Tobacco use was marginally associated. Demographic factors did not show significant associations. These findings suggest that mental health and substance use are important, intersecting contributors to academic impairment linked by sleep problems. Interventions that address mental health, reduce substance use risk, and promote healthy sleep may be particularly beneficial in improving academic outcomes and overall student well-being on college campuses.
Keywords
Introduction
The health and well-being of college students in the United States (U.S.) continue to be a significant public health concern (Prati, 2021). Mental health disorders are the leading cause of disability worldwide among individuals under 24 years of age, contributing to a substantial burden of disease during this developmental stage (Erskine et al., 2015; GBD 2019 Mental Disorders Collaborators, 2022). This vulnerability was intensified by the COVID-19 pandemic, which disrupted academic routines, social connections, and daily life activities (Clabaugh et al., 2021; Lipson et al., 2019). Given that data for this study were collected during 2021—when many campuses were still affected by COVID-19 disruptions—this context is essential for understanding fluctuations in student mental health, sleep routines, and substance use patterns.
College students are particularly vulnerable to these challenges due to the developmental demands of “emerging adulthood,” a phase characterized by identity exploration, emotional instability, and newfound autonomy alongside heightened exposure to substance use (Arnett, 2000; O'Malley & Johnston, 2002; Skidmore et al., 2016). Previous studies have identified psychological distress, sleep disturbances, and social isolation as key drivers of poor health in this population (Jones et al., 2019; NIDA, 2020). Notably, mental health conditions and substance use are closely related, often exhibiting a bidirectional association. Evidence suggests that mental health symptoms increase the likelihood of substance use, while substance use is frequently linked to greater mental health challenges and poorer sleep-related academic functioning (Jones et al., 2019; NIDA, 2020). Together, these factors contribute to elevated vulnerability during this life stage (Fakier & Wild, 2011).
The Self-Medication Hypothesis offers a useful framework for interpreting these patterns, suggesting that substances such as alcohol, tobacco, and cannabis may be used as maladaptive coping mechanisms for psychological distress, ultimately worsening emotional regulation and sleep quality (Khantzian, 1997). Furthermore, the Biopsychosocial Model provides a comprehensive framework for understanding how biological, psychological, and social factors converge to influence students’ mental health, sleep, and academic functioning (Engel, 1977), particularly in emerging adults facing academic, interpersonal, and developmental stressors. While this study does not establish causal directionality, it examines these correlational patterns to better understand their co-occurrence in emerging adulthood.
Within this framework, loneliness—the subjective perception of social isolation—has emerged as a critical determinant of health. Loneliness is associated with increased psychological distress and elevated substance use, and meta-analytic evidence demonstrates its role in prolonged sleep latency and daytime dysfunction (Griffin et al., 2020; Hom et al., 2020). Additionally, loneliness may exacerbate mental health conditions such as depression and anxiety, while simultaneously increasing vulnerability to maladaptive coping strategies like alcohol and cannabis use (Lamis et al., 2014; Sy et al., 2024). These isolation-related risks were further amplified by social network disruptions during the COVID-19 pandemic (Lee et al., 2020). Although substance use tends to rise during this period and correlates with deteriorating mental health (Bonar et al., 2021; Groshkova et al., 2020; Tseng et al., 2023), few studies have investigated how these domains jointly contribute to academic impairment, particularly regarding the differential impacts of specific substances (Blows et al., 2022; NIDA, 2020).
Sleep health is frequently compromised among college students, with profound implications for academic success (Altevogt & Colten, 2006). Prior research consistently links poor sleep quality and mental health challenges to reduced cognitive functioning, lower grades, and increased risk of academic failure (Eisenberg et al., 2009; Gaultney, 2010; Gilbert & Weaver, 2010; Pires et al., 2016). Sleep problems—such as poor quality, insufficient duration, and insomnia—correlate with mental health issues like anxiety and depression. Furthermore, these sleep difficulties are often linked to social isolation and substance use, particularly alcohol consumption (Evans et al., 2021; Maziarz & Askew, 2022). Substance use can further exacerbate these problems, leading to decreased academic engagement and performance (Arria et al., 2013).
Crucially, this study extends the current literature in three specific ways. First, rather than focusing on sleep quality in isolation or distal outcomes like GPA, we examine Sleep-Related Academic Impairment (SRAI) as the primary outcome. This allows us to capture the functional consequence of sleep disturbance—the student’s own recognition that sleep is hindering their work—which serves as a more proximal indicator of academic risk than grades alone. Second, we disentangle the role of loneliness from general psychological distress. While often comorbid, treating loneliness as a distinct predictor allows us to assess the unique contribution of social isolation to academic impairment. Third, we simultaneously model the risks of alcohol, cannabis, and tobacco to determine if these substances differentially contribute to the perception that sleep is impairing academic performance, providing a more granular understanding of how specific polysubstance behaviors interact with sleep to shape academic outcomes.
This study aims to address these gaps by analyzing associations between self-reported use of alcohol, tobacco, and cannabis; psychological distress; loneliness; and sleep difficulties among a geographically representative sample of U.S. college students. We hypothesize that higher levels of substance use, psychological distress, and loneliness will each be independently associated with greater sleep difficulties. Understanding these relationships is critical to informing targeted campus health interventions and improving student well-being in the post-pandemic era.
Materials and Methods
Data Sources
This study utilized data from the Spring 2021 American College Health Association–National College Health Assessment III (ACHA-NCHA III) Reference Group dataset, collected between January and May 2021. The data collection period coincided with significant COVID-19 pandemic disruptions, providing a timely opportunity to assess the immediate impacts on student health behaviors, including psychological distress, loneliness, substance use, and sleep-related academic impairment. This timeframe is particularly relevant to the study’s hypotheses, as it reflects a critical stage of the pandemic during which many U.S. campuses were experiencing disruptions to academic routines, housing stability, and mental health services. The ACHA-NCHA III is a nationally administered, web-based survey assessing college students’ health behaviors, habits, and perceptions. We utilized the national reference group dataset, which aggregates data from institutions using probability sampling or census designs. The reference group is well-suited to address the current study’s research questions due to its focus on the same behavioral and psychosocial factors—such as sleep-related academic impairment, psychological distress, loneliness, and substance use—that are central to the study’s theoretical framework and hypotheses.
Participants and Procedures
The Spring 2021 ACHA-NCHA III Reference Group includes responses from 96,489 students at 137 U.S. postsecondary institutions. Each institution selected a random sample of enrolled students aged 18 and older, and participation was voluntary. From this pool, a subset of 6,943 students completed all variables relevant to the broader study. To focus the analysis on emerging adults and ensure consistency with the research objective, the sample was restricted to respondents aged 18–24. Of the eligible age-restricted participants, approximately 11.5% were excluded due to incomplete data on the primary dependent variable or key predictors. To assess the nature of missingness, Little’s MCAR test was conducted and yielded a statistically significant result (χ2 = 52.81, df = 31, p = .012), suggesting that the data were not Missing Completely at Random (MCAR). We therefore assumed that missingness was plausibly Missing at Random (MAR) conditional on observed study variables. Primary analyses used listwise deletion for transparency and to maintain comparability with the main manuscript results. To evaluate whether findings were sensitive to the missing-data strategy, we conducted a sensitivity analysis using multiple imputation (MI; m = 20 imputations) including all variables from the fully adjusted model (psychological distress, loneliness, tobacco/alcohol/cannabis risk, age, sex/gender, year in school, enrollment status, and race/ethnicity). The pooled MI estimates were substantively consistent with the complete-case results (see Supplemental Table S4), supporting the robustness of the primary findings to the method of handling missing data. The final analytic sample included 798 participants. While the sample is not weighted to represent all U.S. college students, it retains diversity in age, sex, race/ethnicity, and institutional characteristics. Descriptive statistics indicate that the analytic sample is broadly comparable to the full reference group on key demographics. Potential biases include differential response rates across institutions and underrepresentation of students not currently enrolled full-time. Additionally, responses may be subject to recall or social desirability bias; however, the anonymity of the survey and use of validated instruments (e.g., K6+, ASSIST) mitigate concerns about measurement validity.
Measures
Dependent Variable
Academic Impairment Due to Sleep Difficulties
Academic impairment related to sleep difficulties was assessed using a single item from the ACHA-NCHA III survey: “Within the last 12 months, how have sleep difficulties affected your academic performance?” Response options were measured on a 4-point ordinal scale: (1) Did not experience this issue, (2) Did not affect academic performance, (3) Negatively impacted academic performance, and (4) Delayed progress toward degree completion. For the main analysis, this variable was dichotomized as “no academic impact” (responses 1 or 2) versus “academic impact” (responses 3 or 4). This binary transformation aligns with prior research practices and facilitates interpretable modeling of perceived academic consequences. We selected this variable as the primary outcome to capture the functional impairment associated with sleep disturbance, rather than sleep pathology alone. Unlike distal measures such as Grade Point Average (GPA), which reflect the culmination of academic performance, this item assesses the proximal, subjective experience of sleep as a barrier to academic success. This operationalization allows for the identification of students who may be ‘functionally struggling’—experiencing significant academic friction due to sleep—even if their grades have not yet precipitously dropped.
Supplementary Sleep-Related Indicators
To address the limited operationalization of sleep in the primary measure, we included three additional sleep-related indicators in supplementary analyses to provide a more multidimensional view of sleep health. These included: (1) weekday sleep duration, based on hours reported during a typical school week; (2) daytime sleepiness, based on the number of days in the past week feeling tired or sleepy during the day; and (3) perceived restfulness, based on how many days in the past week the respondent felt well rested. Each variable was recoded into binary indicators using empirically supported cutoffs: fewer than 7 hr of weekday sleep, feeling tired or sleepy during the day on ≥3 days/week, and feeling rested on <3 days/week. These binary variables were modeled separately using logistic regression to assess consistency of associations across different dimensions of sleep.
Independent Variables
Psychological Distress
Psychological distress was measured using the Kessler Psychological Distress Scale (K6+, a six-item screener with added clinical cutoffs), a validated screening tool for serious mental illness. This self-report instrument captures symptoms such as depression, anxiety, and behavioral impairment experienced in the past 30 days (Surkalim et al., 2022). Total scores range from 0 to 24, with higher scores indicating greater psychological distress. Internal reliability in the current sample was high (Cronbach’s α = .89). Participants were categorized into one of three levels based on their total score: (1) No or low psychological distress, (2) Moderate psychological distress, and (3) Serious psychological distress.
Loneliness
Loneliness was assessed using the UCLA Three-Item Loneliness Scale (Hughes et al., 2004), a brief measure of subjective social isolation. Respondents indicated how often they experienced feelings such as being left out or isolated using a 3-point scale (1 = hardly ever, 2 = some of the time, 3 = often). Scores range from 3 to 9, with higher scores indicating greater perceived loneliness. Internal reliability in the current sample was acceptable (Cronbach’s α = .79). The scale has been validated among college student and young adult populations and is widely used in national surveys assessing social isolation and well-being.
Substance Use
Substance use was measured using the Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST), based on the World Health Organization’s Version 3.0 questionnaire (Patten et al., 2000). Participants reported past-three-month and lifetime use of substances including tobacco (e.g., cigarettes, e-cigarettes, hookah, chew), alcohol (e.g., beer, wine, liquor), and cannabis (e.g., marijuana, edibles, vaped cannabis). Each substance was scored based on the WHO’s ASSIST scoring system and categorized into risk levels: Tobacco and Cannabis: Low (0–3), Moderate (4–26), High (27–39); Alcohol: Low (0–10), Moderate (11–26), High (27–39) (WHO, 2010). These risk categories indicate potential for harmful use or dependence (Chassagne et al., 2022; Smith et al., 2023; Taylor et al., 2023). ASSIST has been widely applied and validated in U.S. college student populations, supporting its appropriateness for this study. Its cross-cultural design and established use in American college settings provide confidence in its applicability. Furthermore, our analysis focused on relative risk categorization, which preserves interpretability across diverse student populations.
Covariates: Demographic Characteristics
Demographic variables included sex (female, male, Non-binary), age (18, 19, 20, 21, 22, 23, 24), race/ethnicity (White, American Indian or Native Alaskan, Asian or Asian American, Black or African American, Hispanic or Latino/a/x, Other), year in school (1st-year undergraduate to 5th-year or more), and enrollment status (full-time, part-time, or other). These variables were included as covariates in multivariable models.
Statistical Analysis
All analyses were conducted using SAS statistical software (version 9.4; SAS Institute Inc., Cary, NC, USA). Descriptive statistics were generated using weighted frequencies and percentages for categorical variables and means with standard deviations for continuous variables. Chi-square tests were used to assess bivariate associations among key variables.
Final analyses focused on multivariable logistic regression models, which examined associations between psychosocial and behavioral predictors and the primary dependent variable: academic impairment due to sleep difficulties (dichotomized as no academic impact [responses 1–2] vs. academic impact [responses 3–4]). Models included psychological distress, loneliness, ASSIST-based substance use risk, and demographic covariates. All regression models accounted for the complex survey design of the ACHA-NCHA III dataset using SAS PROC SURVEYLOGISTIC, incorporating stratification, clustering, and post-stratification weighting. This approach enabled population-representative estimates and improved precision. Variance inflation factors (VIFs) were assessed to detect multicollinearity, with all VIFs <2 indicating acceptable levels. To provide a more multidimensional view of sleep-related challenges, supplementary logistic regression models were conducted using three additional binary dependent variables: (1) weekday sleep duration (<7 hr), (2) daytime sleepiness (≥3 days/week), and (3) perceived restfulness (<3 days/week). Each model used the same predictor set and survey design adjustments as the primary analysis. All statistical tests were two-sided, with significance defined as p < .05.
Results
Descriptive Characteristics
Sociodemographic Characteristics of the Analytic Sample (N = 798) Among U.S. College Students Aged 18–24
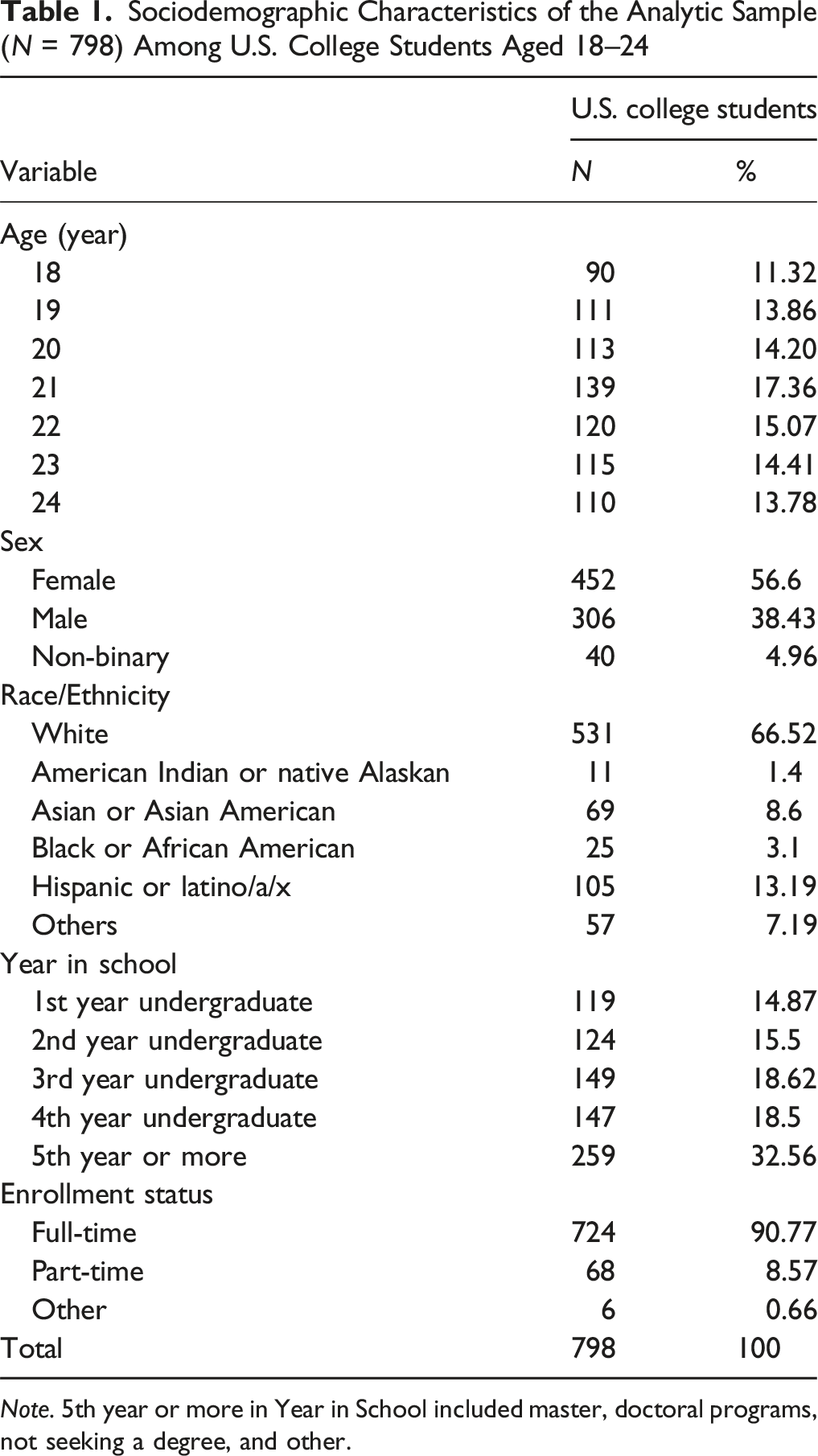
Note. 5th year or more in Year in School included master, doctoral programs, not seeking a degree, and other.
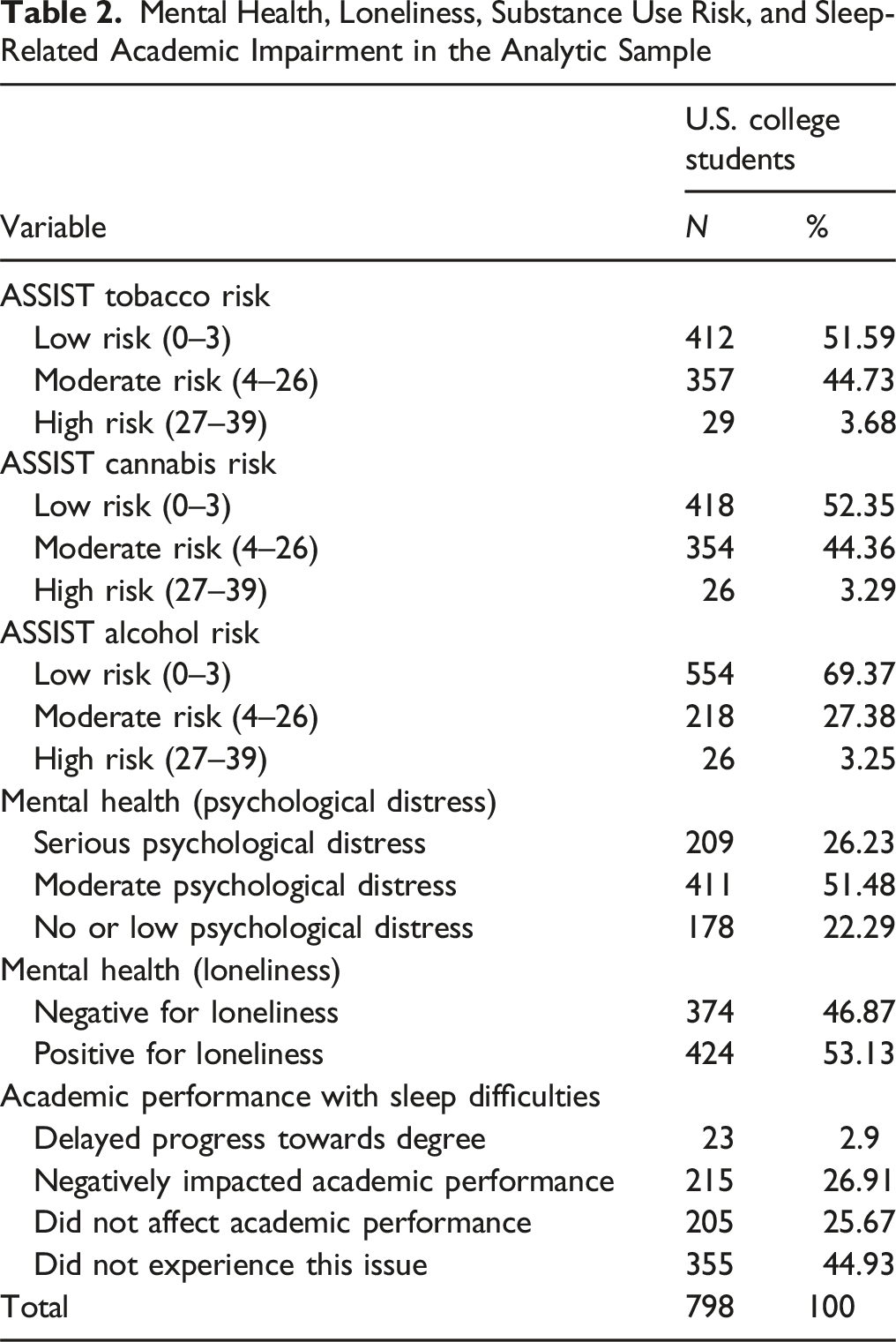
Mental Health, Loneliness, Substance Use Risk, and Sleep-Related Academic Impairment in the Analytic Sample
Fully Adjusted Logistic Regression Predicting Academic Impairment due to Sleep Difficulties Among U.S. College Students Aged 18–24
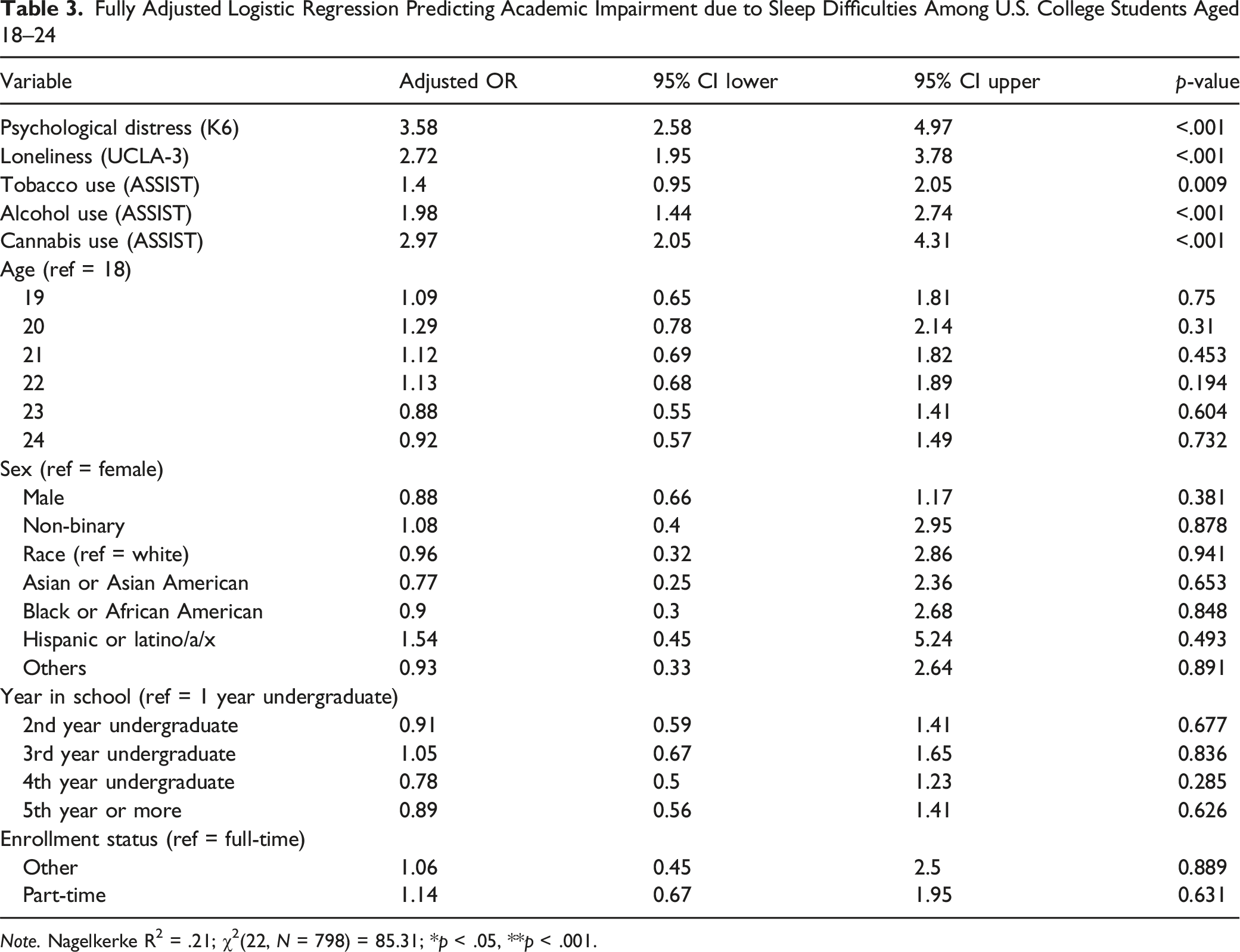
Note. Nagelkerke R2 = .21; χ2(22, N = 798) = 85.31; *p < .05, **p < .001.
Multivariable Logistic Regression Predicting Academic Impairment due to Sleep Difficulties
An initial multivariable linear regression using the full dataset (N = 6,943) showed that psychological distress, loneliness, and alcohol and tobacco use risk scores were significantly associated with self-reported sleep difficulties (R2 = .1183, p < .0001). However, due to concerns about construct validity and measurement precision, the present study re-focused on academic impairment attributable to sleep difficulties using logistic regression with dichotomous dependent variables. The logistic regression analysis identified variables significantly associated with academic impairment due to sleep difficulties. Psychological distress (AOR = 3.58, 95% CI [2.58, 4.97], p < .001), loneliness (AOR = 2.72, 95% CI [1.95, 3.78], p < .001), and alcohol use (AOR = 1.98, 95% CI [1.44, 2.74], p < .001) were strongly associated. Cannabis and tobacco use also showed significant associations. No demographic variables reached statistical significance. Multicollinearity diagnostics indicated acceptable levels of collinearity across associated variables, with all variance inflation factors (VIFs) below 2. Given the analytic sample size (N = 798) and the lack of excessive multicollinearity, the logistic regression model estimates are considered stable and interpretable.
Supplementary Analyses of Additional Sleep Related Variables
To further explore the robustness of our findings and address concerns about the limited operationalization of the sleep construct, we conducted supplementary logistic regression analyses using three additional sleep-related indicators: (1) weekday sleep duration (<7 hr), (2) daytime sleepiness (≥3 days/week), and (3) perceived restfulness (<3 days/week). Each dependent variable was modeled separately using the same set of associated variables as the main analysis.
For weekday sleep duration, serious psychological distress significantly increased the odds of sleeping less than 7 hr on weekdays (AOR = 2.15, 95% CI [1.50, 3.09], p < .001), as did self-reported loneliness (AOR = 1.62, 95% CI [1.12, 2.34], p = .010). High-risk alcohol use was also associated with short sleep duration (AOR = 1.45, 95% CI [1.01, 2.09], p = .045), whereas tobacco and cannabis risk were not statistically significant associated variables.
In the model predicting daytime sleepiness, serious psychological distress again emerged as a strong associated factor (AOR = 2.80, 95% CI [1.95, 4.02], p < .001), followed by loneliness (AOR = 1.75, 95% CI [1.20, 2.55], p = .003), and high-risk alcohol and cannabis use (AOR = 1.60 and 1.50, respectively; p < .05). Tobacco use was not significantly associated.
For perceived restfulness, students with serious psychological distress had over three times the odds of feeling unrested (AOR = 3.10, 95% CI [2.10, 4.58], p < .001). Loneliness (AOR = 1.85, 95% CI [1.25, 2.74], p = .002), and high-risk alcohol and cannabis use (AOR = 1.70 and 1.55, respectively; p < .05) were also significantly associated with this dependent variable. Tobacco use again did not reach statistical significance. Full regression tables for these supplementary analyses are provided in Supplemental Tables S1 to S3.
Discussion
This study examines the mechanisms connecting student health to academic outcomes by focusing on the functional impairment attributable to sleep. Our results demonstrate that this impairment is significantly amplified by a cluster of psychosocial and behavioral factors. A distinct finding of this work is the robust, independent role of loneliness (AOR = 2.72), which predicted sleep-related impairment even after controlling for serious psychological distress. This suggests that the subjective experience of isolation acts as a unique stressor that may degrade the restorative value of sleep for academic functioning. Furthermore, our analysis differentiates the functional costs of substance use; while alcohol and cannabis use were associated with clear sleep-related impairment, tobacco use was not. This distinction adds nuance to the ‘Self-Medication Hypothesis’ in the college context, suggesting that the sedative or intoxicating effects of alcohol and cannabis may have a more direct interference with the sleep-academic interface than nicotine.
Substance Use and Sleep-Related Academic Impairment
Consistent with our hypotheses, high-risk alcohol and cannabis use were significantly associated with sleep-related academic impairment. These findings align with research linking alcohol misuse to fragmented sleep and daytime dysfunction. The strength and consistency of these associations suggest alcohol prevention and intervention programs may be an important strategy for improving sleep health and, consequently, academic outcomes. Our finding that cannabis use predicts academic impairment contrasts with prior mixed literature, where some studies suggest sleep benefits from specific cannabinoids (e.g., CBD) while others note adverse effects from chronic use (Babson et al., 2017). Our results underscore the complexity of cannabis-related sleep disturbances, suggesting that future research must clarify the distinct roles of dosage, frequency, and chemical composition (e.g., THC vs. CBD) in shaping academic outcomes. Although tobacco use did not reach statistical significance, it exhibited a positive trend consistent with literature linking nicotine to sleep disruption. Future studies with larger samples of high-frequency users may be needed to clarify this relationship.
Psychological Distress and Sleep-Related Academic Impairment
Psychological distress emerged as the most robust factor associated with academic impairment related to sleep difficulties. The high prevalence of moderate to serious psychological distress within our sample underscores its substantial burden on college students’ well-being and academic performance. Our findings align with previous research describing a bidirectional relationship between psychological distress and sleep problems among young adults. Poor sleep may exacerbate symptoms of anxiety and depression, while increased psychological distress can negatively impact sleep quality and duration. These findings have important implications for interventions on campuses. They suggest that addressing psychological distress such as through scalable mental health programs may significantly improve students’ sleep health, thereby enhancing academic outcomes. Given the robust association even after adjusting for covariates, strategies targeting mental health should be prioritized as critical elements of broader wellness initiatives in higher education.
Loneliness and Sleep-Related Academic Impairment
Loneliness also demonstrated a strong, independent association with sleep-related academic impairment. More than half of students in our sample screened positive for loneliness, indicating widespread perceived social isolation. This aligns with existing evidence highlighting loneliness as a significant predictor of disrupted sleep patterns, reduced sleep quality, and impaired academic functioning. The persistence of this relationship after adjusting for demographic and behavioral factors emphasizes loneliness as a distinct risk factor warranting targeted intervention. College campuses may benefit from programs fostering social connectedness, peer support, and community integration to reduce loneliness and subsequently improve sleep health and academic success. Future longitudinal research should examine bidirectional associations and investigate whether loneliness functions as a mediator or serial mediator between psychological distress and sleep deficits, or as a moderator that amplifies the academic risks of substance use. Untangling these complex pathways will be critical for tailoring interventions to the most vulnerable students.
Demographic Considerations
When adjusting for psychological and behavioral factors, our analysis revealed no statistically significant demographic differences (e.g., sex, age, race/ethnicity, year in school, or enrollment status) associated with sleep-related academic impairment. While descriptive statistics indicated demographic variation in psychological distress and sleep experiences, these differences did not persist when examined within fully adjusted models. This finding suggests that psychosocial and behavioral factors may overshadow demographic characteristics when considering sleep-related academic impairment. Rather than tailoring interventions strictly based on demographic attributes, campus-based strategies could benefit from a universal approach addressing shared psychological vulnerabilities such as distress and loneliness. Nonetheless, future studies should examine nuanced demographic intersections (e.g., socioeconomic status, intersectionality of identity) that may reveal hidden subgroup vulnerabilities.
Research Implications
The implications of using Sleep-Related Academic Impairment as a primary metric are two-fold. First, it validates the student’s subjective experience as a clinical indicator; when a student reports that sleep is hindering their work, this perception is strongly correlated with tangible risks like high-risk substance use and loneliness. Second, the consistency of our findings across the supplementary outcomes (sleep duration, daytime sleepiness, and restfulness) suggests that SRAI is a reliable proxy for broader sleep health deficits. Therefore, given the consistent associations observed across these supplementary sleep indicators intervention approaches should move beyond singular targets (e.g., sleep education alone) and instead address interlocking domains of mental health, sleep hygiene, and substance use. For example, brief behavioral sleep interventions such as digital cognitive behavioral therapy for insomnia (CBT-I) programs and sleep hygiene modules have demonstrated efficacy in improving sleep quality and daytime functioning among college students (Hershner & O'Brien, 2018). These interventions may be effectively embedded within first-year orientation, residential life programming, or campus wellness platforms.
In parallel, campus-wide mental health promotion strategies—such as universal mental health screenings, stigma-reducing campaigns, and embedded counseling models—can help identify students experiencing psychological distress earlier in the academic cycle (Pedrelli et al., 2015). To address loneliness, institutions may benefit from implementing structured peer-connection initiatives such as mentoring programs, student affinity groups, or “community pods” designed to promote belonging and interpersonal support. An innovative and potentially scalable model is the deployment of academic wellness navigators—trained liaisons who proactively guide students to resources. To succeed, this model requires robust multidisciplinary collaboration where academic advisors, counselors, and student life staff coordinate to bridge the gap between academic affairs and student health. This approach integrates upstream academic support with psychosocial care and may reduce common barriers to accessing services, especially for at-risk students reluctant to self-refer. Importantly, the lack of significant demographic variation in our findings suggests that sleep-related academic impairment is not confined to specific student subgroups. Accordingly, future interventions should be designed for universal accessibility, with the flexibility to accommodate intersectional identities, varied life circumstances, and differing levels of readiness to engage.
Limitations
Several limitations should be noted. First, the cross-sectional design precludes causal inferences and direct comparisons to pre-pandemic periods; longitudinal work is needed to determine directionality and mediating mechanisms. Second, reliance on self-reported data introduces potential recall and social desirability biases, although validated instruments (e.g., K6+, ASSIST) were used to mitigate measurement error. Third, the primary outcome was a single-item measure. While we included supplementary indicators (duration, sleepiness, restfulness) to enhance robustness, these do not fully capture objective sleep physiology. Fourth, the sample was predominantly non-Hispanic White, female, and aged 18–24, limiting generalizability to diverse or non-traditional student populations. Fifth, missing data were handled via listwise deletion. Although Little’s MCAR test was significant (
Conclusion
This study offers important insights into the associations among psychological distress, loneliness, and substance use in shaping sleep-related academic impairment among U.S. college students. Drawing on a large national dataset, we identified psychological distress and loneliness as the strongest associated factors, with high-risk alcohol and cannabis use also significantly related to students’ academic impairment linked to sleep difficulties.
The breadth and severity of these challenges—particularly the widespread prevalence of psychological distress and perceived social isolation—underscore the urgent need for comprehensive, multidimensional campus-based responses. Specifically, institutions of higher education should consider implementing integrated approaches that combine evidence-based mental health screenings, brief behavioral sleep interventions (e.g., digital CBT-I or sleep hygiene modules), and peer-facilitated resilience training. Additionally, social connectedness initiatives—such as structured “community pods,” peer mentorship programs, or residential-based outreach—may reduce loneliness while fostering protective peer networks. To address substance use risks, harm reduction education and motivational interviewing approaches could be embedded into academic advising or first-year seminars.
Importantly, campuses might explore innovative delivery models such as “academic wellness navigators”—trained student or staff liaisons who can connect at-risk students with mental health, sleep, and substance use resources through proactive outreach. These models leverage existing support infrastructure while reducing stigma and barriers to care. Furthermore, given the lack of significant variation across demographic characteristics, interventions should be universally accessible but designed with flexibility to meet the needs of diverse student identities and lived experiences. As colleges continue to adapt in the wake of the COVID-19 pandemic, building resilient, student-centered support ecosystems is more essential than ever. Future research should investigate the longitudinal effectiveness of these strategies, explore digital and peer-led interventions for mental health and sleep improvement, and identify protective mechanisms, such as belongingness or emotion regulation, that support sustained students’ academic performance and student well-being.
Supplemental Material
Supplemental material - Academic Impairment From Sleep Difficulties: The Role of Substance Use, Psychological Distress, and Loneliness in U.S. College Students
Supplemental material for Academic Impairment From Sleep Difficulties: The Role of Substance Use, Psychological Distress, and Loneliness in U.S. College Students by Sunghyun Chung, Molly J. Gutilla, Monica Keele, Jeonghui Park, Dohyun Chung, and Adam E. Barry in Emerging Adulthood
Supplemental Material
Supplemental material - Academic Impairment From Sleep Difficulties: The Role of Substance Use, Psychological Distress, and Loneliness in U.S. College Students
Supplemental material for Academic Impairment From Sleep Difficulties: The Role of Substance Use, Psychological Distress, and Loneliness in U.S. College Students by Sunghyun Chung, Molly J. Gutilla, Monica Keele, Jeonghui Park, Dohyun Chung, and Adam E. Barry in Emerging Adulthood
Footnotes
Ethical Considerations
This study utilized de-identified, publicly available secondary data from the American College Health Association–National College Health Assessment (ACHA-NCHA). The dataset contains no personally identifiable information, and all responses were collected anonymously.
Consent to Participate
Participation in the original survey was voluntary, with informed consent obtained through an email invitation and reaffirmed at the start of the survey. In accordance with U.S. federal regulations, the use of such de-identified secondary data is considered exempt from Institutional Review Board (IRB) review. A statement describing this exemption has been included in the Methods section of the manuscript.
Consent for Publication
Not applicable. This study used secondary, de-identified data from the American College Health Association–National College Health Assessment (ACHA-NCHA), and no individual participant data are reported.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article. The data that support the findings of this study are available from The ACHA-National College Health Assessment (NCHA) but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of The ACHA-National College Health Assessment (NCHA).
Transparency and Openness Statement
The data used in this study were obtained from the American College Health Association National College Health Assessment (ACHA-NCHA) and are not publicly available due to data use restrictions imposed by the data provider. Researchers may request access to the data directly from the American College Health Association (https://www.acha.org). The analysis code and study materials are deposited at ![]() ; however, access is restricted due to data use agreements. This study was not pre-registered.
; however, access is restricted due to data use agreements. This study was not pre-registered.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.