
Abstract
This study investigated the relationship between symptoms of sleep disorders, anxiety, and depression in a sample of 871 emerging adults (aged 18-25 years, 74% women, 78% White/Caucasian). Utilizing secondary data from a study of US college students, we examined the cross-sectional associations between self-reported sleep disorder symptoms and their comorbidity on mental health outcomes. Regression analyses revealed significant associations between total sleep disorder symptoms and symptoms of both anxiety and depression. MANOVA results indicated a dose-dependent-like relationship between the number of self-reported sleep disorders and increasingly higher levels of anxiety and depressive symptoms. These findings are correlational and based on data from self-report, non-clinical measures, but are nevertheless supportive of continued investigation of sleep assessments in youth mental health settings and interventions targeting sleep problems for a range of psychological symptoms. Future research should explore specific symptom comorbidity patterns across a broader range of psychological disorder-related symptoms.
Emerging adulthood (EA) is a pivotal period of development marked by a multitude of life transitions, self-exploration, and the onset of new responsibilities and independence. This period is characterised by a series of transitions in various life domains such as living arrangements, relationships, education, and employment, rendering it a particularly unstable period in one’s lifespan (Arnett, 2014). These transitions, although normative, often brew a level of instability and uncertainty which, in turn, can precipitate significant mental health challenges (Arnett et al., 2014).
EA is also accompanied by significant changes in sleep patterns due to developmental shifts in physiological processes at this life stage. The most common change in late adolescence is a biological delay in sleep timing, often leading to sleep deprivation, and increasing risk for later development of sleep disorders such as insomnia (Colrain & Baker, 2011). Variations in sleep duration, onset latency, timing, and consolidation are normal in adolescence, however persistent problems in any of these processes can have adverse consequences for mental health. For instance, insomnia and other sleep disorders have been correlated with an elevated risk for depression, anxiety, and stress-related disorders in both adults (Baglioni et al., 2011) and youth (Marino et al., 2021). A meta-analysis of longitudinal and treatment studies in adolescents showed that sleep problems were predictive of later depression, with limited evidence of a relationship in the opposite direction (Lovato & Gradisar, 2014). Peltz et al. (2017) reported bidirectional associations between sleep problems and symptoms of anxiety in a diary-based study of US college students. Reviews by Freeman et al. (2020) and Alvaro et al. (2013) similarly report bidirectional associations between sleep and mood. The evidence is clear that sleep and mental health problems commonly co-occur and are highly likely to influence each other in a bidirectional manner.
The high level of comorbidity between sleep problems and adverse psychological outcomes is fully realised in the transdiagnostic model of sleep disturbance (Harvey, 2016), with the two processes proposed to be causally linked via common effects on emotion regulation and shared neurobiological substrates. Yoo et al. (2007), for example, showed that emotion regulation was impaired under conditions of sleep deprivation via loss of functional connectivity between the amygdala and pre-frontal cortex structures. Overlapping genes have also been shown to confer polygenic risk for both sleep problems and depressive symptoms via their regulation of synaptic function (Moyses-Oliveira et al., 2024). A systematic review and meta-analysis of randomised controlled trials investigating the efficacy of psychological interventions for improving sleep in young adults provided additional support for transdiagnostic mechanisms by showing that such interventions not only improved sleep, but also reduced symptoms of anxiety and depression (Kodsi et al., 2021). Finally, the Transdiagnostic Sleep and Circadian Intervention for Youth (TranS-C), a modular treatment strategy based on Harvey’s model, has demonstrated moderate success in managing sleep problems in young people (e.g., Dolsen et al., 2023).
Despite broad recognition of the associations between sleep and mental health problems in young people, a comprehensive analysis of the mental health burden accumulated across multiple, interacting sleep disorders is lacking in this population. Most studies focus on specific sleep disorders in isolation and rarely consider the cumulative impact of multiple sleep disorders on adverse psychological outcomes. This is despite the fact that co-existing sleep disorders are common and represent a complex scenario for both diagnosis and clinical management (Appleton et al., 2018; Sweetman et al., 2023).
The aim of the current study, therefore, was to investigate the relationships between symptoms of multiple sleep disorders, anxiety, and depression in a large sample of emerging adults (aged 18-25 years old). We first hypothesised a positive association between the total burden of sleep disorder symptoms and symptoms of both anxiety and depression (H1). We also hypothesised that the cumulative impact of increasingly higher levels of sleep disorder symptom comorbidity would predict increasingly higher levels of anxiety and depressive symptoms (H2).
Method
Sample and Study Design
This study analysed data from the Assessing Nocturnal Sleep/Wake Effects on Risk of Suicide (ANSWERS) Phase 1 Survey which was conducted 2020-2021 at the University of Arizona. The original study examined sleep disorder symptoms and mental health symptoms in a cohort of students recruited from the undergraduate psychology course in which they were enrolled, and through campus flyers and emails (N = 971; Tubbs et al., 2022). There were no specified exclusion criteria and data were collected through an online survey. The dataset from the original study was made available through the National Sleep Research Resource (NSRR; Zhang et al., 2018) and facilitated the current study’s focus on associations between symptoms of various sleep disorders and mental health outcomes in emerging adults. The University of Arizona IRB approved the original study and the publication of data in an open science repository (Ref. 2005675654). Express permission was granted from NSRR to use the original data for the current study.
Participants for the current study (N = 871; 73.7% women) were selected based on the age criterion of 18-25 years (M = 19.61 years, SD = 1.26 years), thus representing the EA demographic. The sample was predominantly White/Caucasian (77.8%), heterosexual (82.8%), and high school educated (95.8%).
Measures
Centre for Epidemiological Studies Depression Scale-Revised (CESD-R; Eaton et al., 2004)
CESD-R assesses the frequency of depressive symptoms via 20 items rated on a 4-point scale (0 = Rarely or some of the time, 3 = Most or all of the time). Items address the respondent’s experience of depressive symptoms such as hopelessness or restlessness during the past week. Total scale scores range from 0 to 60, with higher scores indicating higher levels of depression. Internal reliability of the scale in the current study was acceptable (α = .79).
Generalized Anxiety Disorder-7 Questionnaire (GAD-7; Spitzer et al., 2006)
GAD-7 measures the frequency of anxiety symptoms over the previous 2 weeks using 7 items that are rated on a 4-point scale (0 = Not at all, 3 = Nearly every day). The items address symptoms such as nervousness, worry, and irritability. Total scale scores range from 0 to 21, with higher scores indicating higher levels of anxiety. Internal reliability of the scale in the current study was excellent (α = .92).
Sleep Disorder Symptom Checklist-25 (SDSCL-25; Klingman et al., 2017)
SD-SC-L-25 is a screening tool for 13 diagnosable sleep disorders (e.g., Insomnia disorder, Obstructive Sleep Apnea, Narcolepsy). Respondents rate the frequency with which they experienced specified sleep patterns and disturbances over the past year on a 5-point scale (0 = Never, 4 = Frequently). Internal reliability of the scale in the current study was good (α = .85). We used the scores on the SDSCL-25 to derive two variables of interest for the current study.
Sleep Disorder Symptom Total (SDS)
This variable represents aggregate sleep disorder symptom frequency and is calculated by summing all SD-SCL-25 item scores. Higher SDS scores indicate presence of more frequent and severe sleep disorder symptoms.
Sleep Disorder Comorbidity (SDC)
This variable indicates the number of distinct sleep disorders a participant screened positive for. As per the SD-SCL-25 scoring guide, a positive screen for any individual sleep disorder was indicated by the presence of at least one clinically relevant symptom occurring frequently (3 or more times a week) within the cluster of symptoms assigned to that disorder (Klingman et al., 2017). For example, a positive screen for Obstructive Sleep Apnoea required presence of either “snoring” or “stopping breathing during sleep” on 3 or more occasions per week, plus endorsement of at least one of the following daytime consequences: “daytime sleepiness or fatigue”, “inappropriately falling asleep”, or “sleep problems interfere with daytime function”. Participants’ scores were categorized into four levels (0, 1, 2, 3 or more), with each level representing a count of the number of sleep disorders they each screened positive for.
Analysis
Hypotheses were addressed using multiple regression analyses for assessing the associations between SDS and symptoms of anxiety and depression, respectively (H1), and MANOVA for assessing the impact of sleep disorder symptom comorbidity on symptoms of anxiety and depression (H2). Power calculations using p < .05, β = .80, and N = 871 indicated that small effect sizes (at minimum) could be detected for all analyses. Examination of the dataset revealed no missing values. Four multivariate outliers were identified using Mahalanobis’ distance scores (2 male, 2 female) and were excluded from further analyses. Shapiro-Wilk tests indicated violations of normality for the Anxiety, W (867) = .934, p < .001, Depression, W (867) = .986, p < .001, and SDS, W (867) = .979, p < .001, variables, all with a slight positive skew. Common transformations corrected the skew, however given there was no meaningful difference in statistical outcomes between analyses using transformed and untransformed variables, the raw data were used in all analyses. The robustness of regression and MANOVA analyses against violation of the normality assumption, especially in large samples, increased confidence in the decision to use the raw data. Nevertheless, nonparametric Kruskal-Wallis H tests were used as follow-up tests to the MANOVA to account for the non-normality of scores for both the Anxiety and Depression variables. Due to commonly observed differences in sleep, depression, and anxiety between men and women (see, for example, de Zambotti et al., 2018; Essau et al., 2018; Kuehner, 2017), participant sex (male, female) was employed as a covariate or moderator as appropriate in all analyses. Alpha for statistical significance was set at p < .01 for all analyses. SPSS Version 29.0 was used to conduct all screening procedures and hypothesis testing analyses.
Results
Descriptive Statistics and Correlations for Depression, Anxiety, and Sleep Disorder Symptom Scores
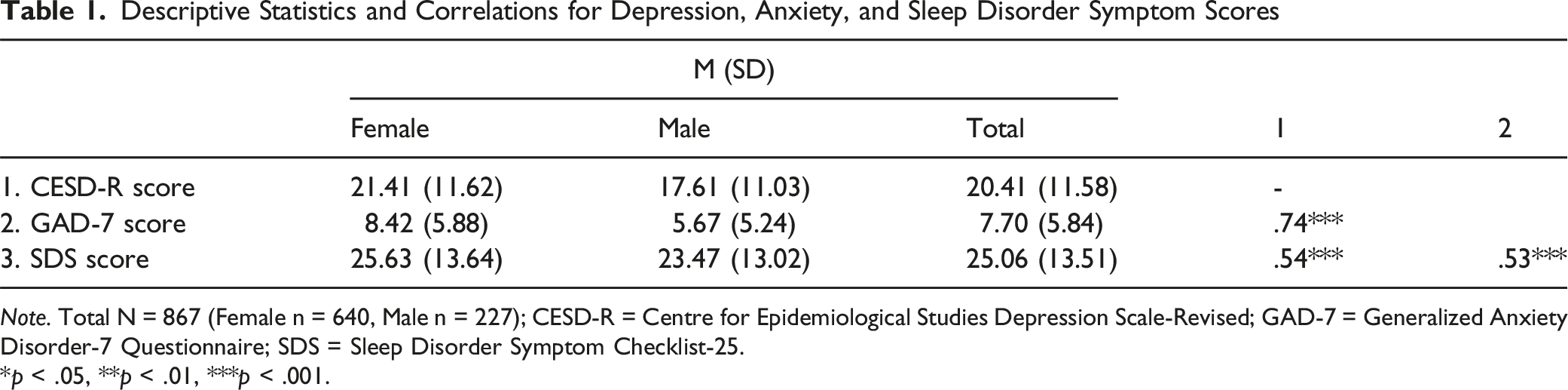
Note. Total N = 867 (Female n = 640, Male n = 227); CESD-R = Centre for Epidemiological Studies Depression Scale-Revised; GAD-7 = Generalized Anxiety Disorder-7 Questionnaire; SDS = Sleep Disorder Symptom Checklist-25.
*p < .05, **p < .01, ***p < .001.
Association Between SDS and Symptoms of Anxiety and Depression
SDS and Anxiety Symptoms
Multiple Regression Analysis Summaries for Sleep Disorder Symptom Scores and Participant Sex Predicting Anxiety and Depression Symptom Scores
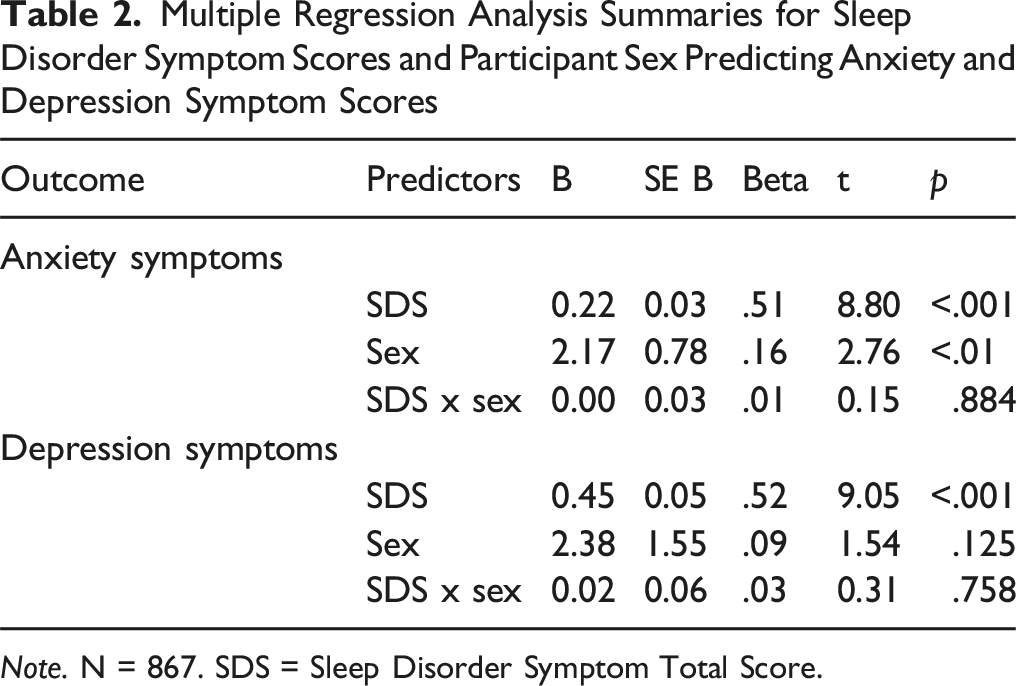
Note. N = 867. SDS = Sleep Disorder Symptom Total Score.
SDS and Depression Symptoms
The regression model for depression scores was also statistically significant, F (3,863) = 127.39, p < .001, accounting for 30.7% of the total variance. Table 2 shows that SDS was a significant independent predictor of depression scores, explaining 6.55% unique variance. Participant sex was not a significant predictor of depression scores. There was also no significant interaction between SDS and participant sex on depression scores.
Relationship Between SDC and Symptoms of Anxiety and Depression
Based on symptoms counts, 164 participants screened positive for a single sleep disorder, 149 screened positive for two sleep disorders, and 92 screened positive for three or more sleep disorders. The remaining 462 participants did not screen positive for any sleep disorders.
The MANOVA revealed that combined sleep disorder symptom count had a significant multivariate effect on both anxiety and depression scores, Pillai’s trace = .159, F (6, 1718) = 24.69, p < .001, η2 = .079. Men and women also differed significantly on both anxiety and depression scores, Pillai’s trace = .031, F (2, 858) = 13.83, p < .001, η2 = .031; women scored higher than men on both outcome variables. The interaction between participant sex and sleep disorder symptom count was not significant. Figures 1 and 2 provide an overview of the estimated marginal means at each level of the independent variable. Estimated Marginal Means for Depression Scores by Participant Sex and Level of Sleep Disorder Symptom Comorbidity. Note. Error bars represent 95% confidence intervals. Means and standard deviations for male and female participants at each level of sleep disorder symptom comorbidity are as follows: 0 sleep disorders, male = 14.75 (10.13), female = 17.17 (10.13); 1 sleep disorder, male = 16.00 (8.53), female = 22.90 (10.51); 2 sleep disorders, male = 23.88 (10.70), female = 26.32 (11.59); 3 sleep disorders, male = 29.14 (10.90), female = 30.61 (10.99) Estimated Marginal Means for Anxiety Scores by Participant Sex and Level of Sleep Disorder Symptom Comorbidity. Note. Error bars represent 95% confidence intervals. Means and standard deviations for male and female participants at each level of sleep disorder symptom comorbidity are as follows: 0 sleep disorders, male = 4.21 (4.35), female = 6.25 (5.05); 1 sleep disorder, male = 5.14 (4.33), female = 9.21 (5.67); 2 sleep disorders, male = 9.09 (5.87), female = 10.99 (5.76); 3 sleep disorders, male = 10.67 (5.92), female = 8.42 (5.88)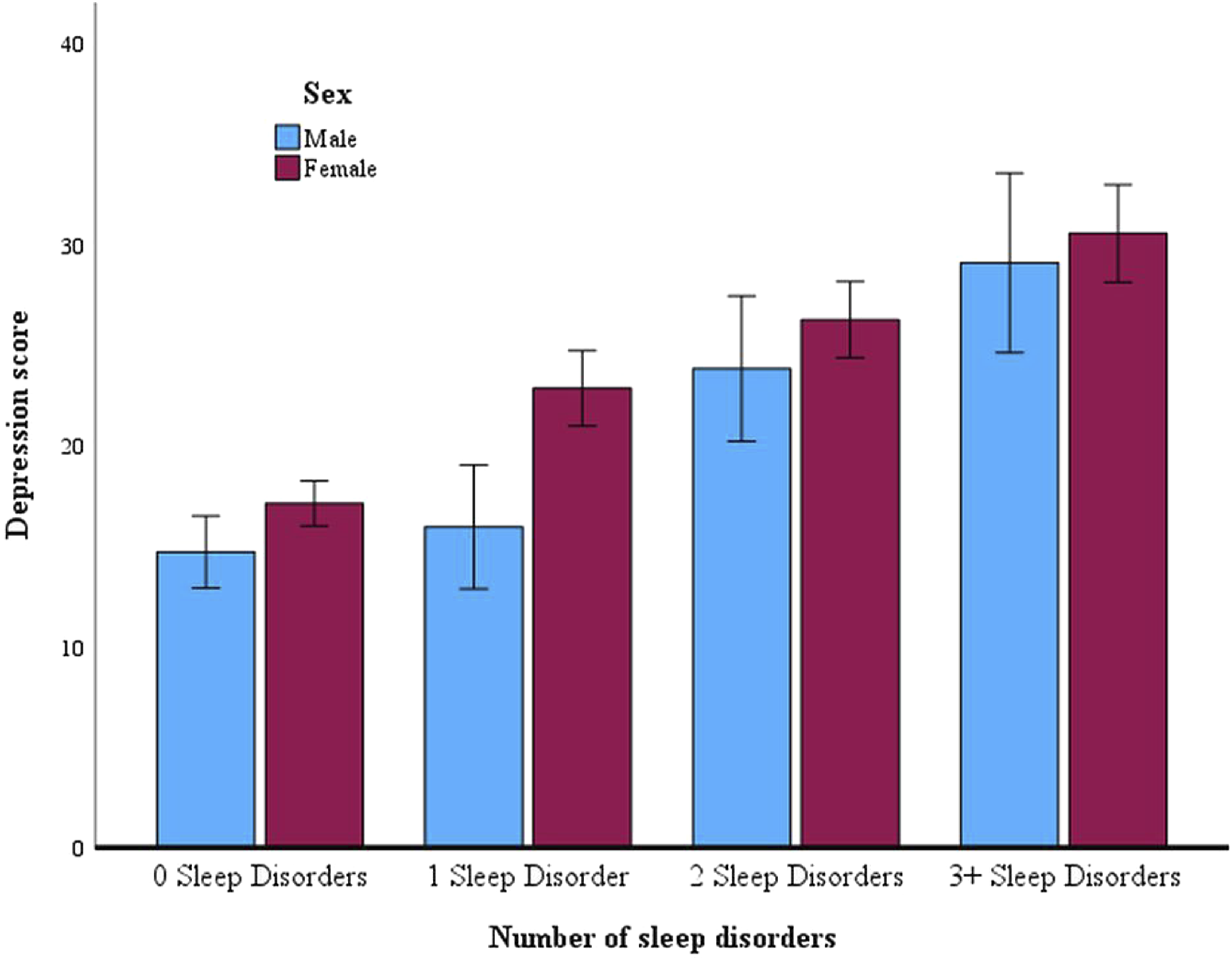
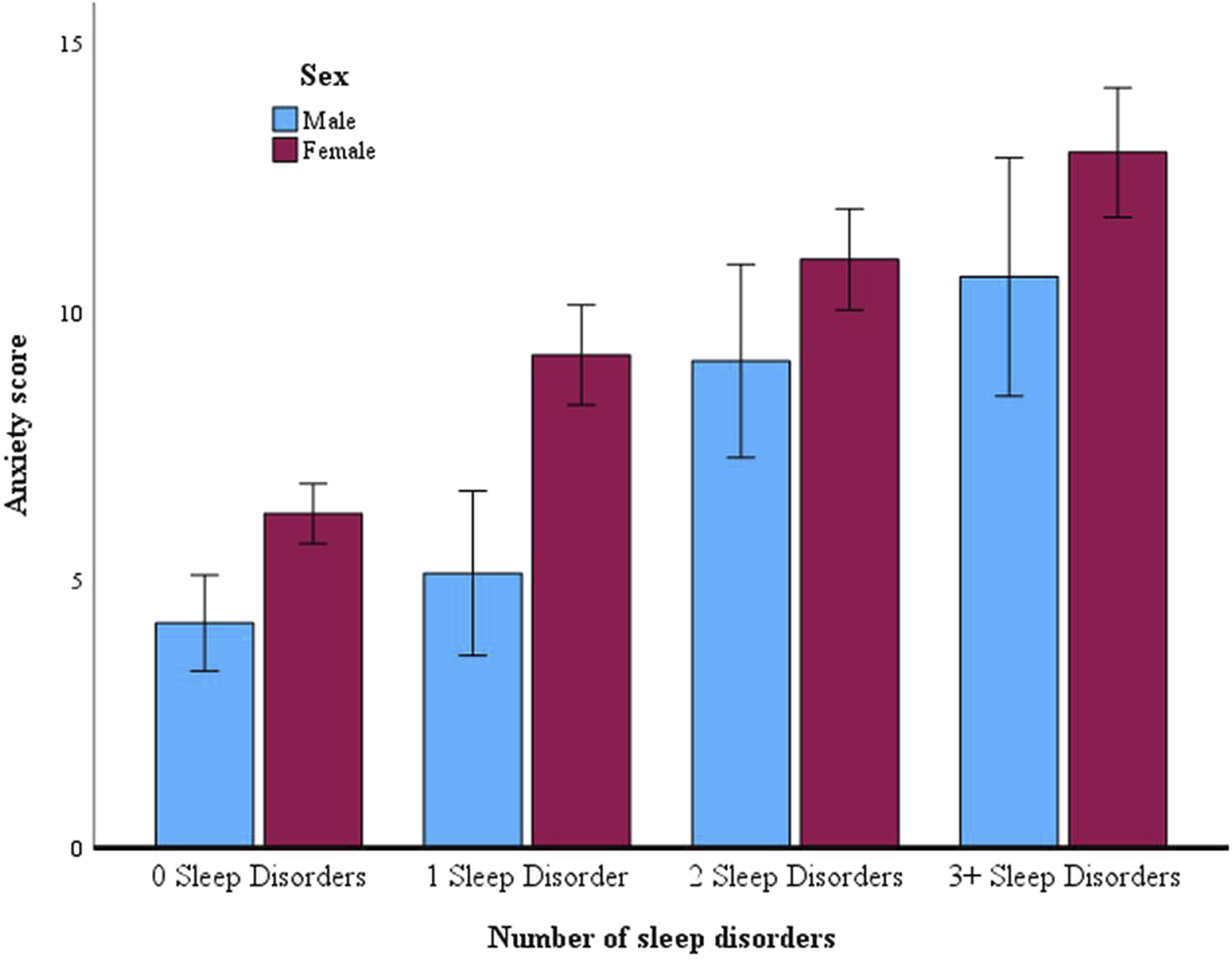
SDC and Symptoms of Anxiety
Follow-up tests showed a significant effect of sleep disorder symptom count on anxiety scores, Kruskal-Wallis H = 150.01, p < .001. Post-hoc pairwise comparisons showed significant differences between all groups, with the exception of the comparison between the group that screened positive for 2 sleep disorders and the group that screened positive for 3+ sleep disorders. The group that screened positive for 0 sleep disorders had the lowest mean anxiety scores, and these scores increased progressively with greater comorbidity of sleep disorder symptoms.
SDC and Symptoms of Depression
Follow-up tests showed a significant effect of sleep disorder symptom count on depression scores, Kruskal-Wallis H = 146.74, p < .001. Post-hoc pairwise comparisons showed significant differences between all groups. Depression scores were significantly lower for the group that screened positive for 0 sleep disorders compared to the groups that screened positive for 1, 2, and 3 or more sleep disorders. Depression scores increased progressively with greater comorbidity of sleep disorder symptoms.
Discussion
This study explored the relationship between symptoms of sleep disorders, anxiety, and depression in a US college-based sample of emerging adults. Two specific hypotheses were supported; a positive association was found between the total burden of sleep disorder symptoms and levels of both anxiety and depressive symptoms (H1), and increasing levels of sleep disorder symptom comorbidity were associated with progressively higher levels of anxiety and depressive symptoms (H2).
Sleep Disorder Symptoms and Mental Health
Multiple regression analyses showed that anxiety and depressive symptoms were both associated with total sleep disorder symptoms. These positive associations are consistent with previous findings in supporting an important role for sleep problems across various adverse mental health outcomes, including those in young people (e.g., Marino et al., 2021). These and similar findings have now been replicated numerous times across a variety of populations and using a variety of methods. The findings are supportive of transdiagnostic frameworks in which sleep and mental health problems are causally linked (see, for example, Harvey, 2016). While our findings cannot be used to support specific linking mechanisms, nor the direction of causality between sleep and mental health problems, they nonetheless add to the evidence base supportive of further testing and refinement of comprehensive assessments and interventions targeting sleep health in youth mental health settings (e.g., TranS-C, Harvey, 2016, and cognitive-behavioural therapy for insomnia, CBTi, Perlis et al., 2005).
Participant sex emerged as a significant predictor of anxiety, with women reporting higher levels than men in this sample. This disparity in anxiety prevalence between the sexes is also consistent with prior studies (e.g., Essau et al., 2018). Whether these differences play a role in the association between sleep problems and anxiety symptoms is not as well defined in the extant literature. Indeed, we did not find that participant sex affected these associations in our analyses – sex was a wholly independent predictor of anxiety symptoms. On the basis of these findings it would appear that the shared neurobiological processes underlying vulnerability to symptoms of sleep disorders and anxiety operate largely independently of the hormonal, psychosocial, and cultural differences experienced by men and women.
Sleep Disorder Symptom Comorbidity and Mental Health
The results indicate a clear pattern of increasingly elevated levels of anxiety and depression symptoms among individuals who screened positive for increasing numbers of comorbid sleep disorders. This observation also aligns with the broader literature that has consistently highlighted the relationship between sleep problems and adverse mental health outcomes. Notably, our findings suggested a dose-dependent-like relationship whereby the mental health burden on individuals escalated with increasing numbers of comorbid sleep disorder symptoms. The findings therefore provide further evidence, albeit indirectly, in support of the transdiagnostic framework linking sleep and mental health problems. Shared neurobiological substrates between sleep and mental health problems, one of the proposed mechanisms underlying the transdiagnostic framework (Harvey et al., 2011), is entirely consistent with the concomitant increase in symptoms found in the current study.
The increasing mental health burden associated with increasingly higher numbers of sleep disorder symptoms is also consistent with a recent study investigating the effects of comorbid insomnia and sleep apnoea (COMISA) symptoms on mental health. Kalra et al. (2024), using cross-sectional data from a nationally representative sample of 5,834 US participants, showed that risk of suicidal ideation and self-harm was more likely to be reported by those experiencing symptoms consistent with COMISA than those experiencing symptoms of either sleep disorder alone. They propose that the combination of insomnia and sleep apnoea has a synergistic effect on worsening mental health. Our study does not address specific symptoms, nor their interaction, but, again, the results are consistent with such a synergistic model in which greater sleep disorder symptom load is associated with worsening mental health outcomes.
Limitations
Due to the cross-sectional nature of the study, causal inferences and the direction of the relationship between sleep problems and mental health outcomes cannot be determined. Previous literature suggests this relationship is bidirectional (e.g., Alvaro et al., 2013). Further research employing longitudinal designs is warranted (see also Wellcome Trust, 2022). It is also worth noting that the measures used in this study are based on self-report and therefore not designed to provide a comprehensive clinical diagnosis of anxiety, depression, and sleep disorders. The SDS-CL-25 in particular is a newly revised instrument for sleep disorder screening and not yet validated against gold standard measures of physician and polysomnography diagnosis. Wearables or nearables as more objective measures of sleep disturbance alongside the self-report SDS-CL-25 used in the current study would provide greater confidence in future study outcomes. Relatedly, the sleep disorder comorbidity variable was created specifically for the current study and calculated by summing the number of sleep disorders a participant screened positive for, as per the SDS-CL-25 interpretation guidelines. While this method efficiently measures the quantity of positively screened sleep disorders, it does not provide insights into specific types of disorders. This lack of granularity in the sleep disorder comorbidity variable potentially masks differential interactions of various sleep disorder symptoms on mental health. Finally, caution should be exercised when generalising findings from the current study as the convenience sample was non-clinical, college-based, and lacked cultural diversity. Data were also collected during a global pandemic in which individuals’ sleep, social routine, and mental health may have been adversely affected. It is possible that these pandemic-associated disruptions exacerbated the magnitude of the reported relationships.
Conclusions and Implications
This study’s findings support previous literature in recognising the intricate and multi-faceted relationship between sleep problems and mental health outcomes in emerging adults. The observed association between sleep disorder symptom comorbidity and mental health in emerging adults incrementally advances debate around the need for a more holistic approach to mental health screening that recognises the interconnected nature of sleep disorders and mental health. The association between cumulative sleep disorder symptoms and worsening mental health supports clinical research suggesting that interventions targeting common sleep problems could potentially alleviate a range of mental health symptoms, thus aligning with transdiagnostic approaches which advocate for interventions that address shared underlying processes and risk factors across disorders (Harvey, 2016).
To advance clinical understanding, future research should explore specific sleep symptom comorbidity patterns. COMISA, for example, may be especially strongly associated with adverse mental health outcomes. It would also be beneficial to explore the associations between comorbid sleep disorder symptoms and mental health outcomes beyond anxiety and depression. Hypomania, substance use, and self-harm are particularly relevant outcomes in emerging adults. Brief interventions that are potentially more suitable to adolescent and young adult populations (e.g., single-session interventions; Carpi et al., 2025) should continue to be trialled for their effectiveness in potentially managing both sleep and mental health concerns. Finally, interdisciplinary collaboration is encouraged in primary and preventative health settings to enhance early detection and intervention (see, for example, Benjamin et al., 2023), ultimately improving the overall well-being of young people experiencing sleep and mental health problems during a pivotal period of development.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Transparency and Openness Statement
The data used in this manuscript are available for download from the National Sleep Research Resource (![]() ) subject to the completion of online request and approval. The analysis code is not openly available but can be provided upon request to the corresponding author. No aspects of the study were pre-registered.
) subject to the completion of online request and approval. The analysis code is not openly available but can be provided upon request to the corresponding author. No aspects of the study were pre-registered.