
Abstract
This study investigated sex differences in indicators of mental health (anxiety, depression) and cardiovascular health (e.g., physical activity levels, heart rate, VO2 max) in a sample of cannabis-using undergraduates. The sample included 209 participants (65% female) who completed two daily diaries for 14 days on their mobile devices; half of whom (n = 100) also wore a Fitbit Charge 4. Females (vs. males) reported significantly more psychological distress at baseline; greater use of cannabis to cope with symptoms of both physical and mental ill-health; and more risks to cardiovascular health. Discriminant function analysis revealed that the variables that significantly distinguished females from males were: 1. Lower VO2 max percentile; 2. Fewer “moderate-to-very active” minutes of physical activity; 3. Higher depression scores plus poorer perceptions of mental health and physical health. Findings from this study suggest that female emerging adults who use cannabis regularly may be uniquely vulnerable to cannabis-related risks.
Cannabis is the most used drug in the world (UNODC World Drug Report, 2023). An estimated 219 million people or 4.3% of the global adult population, used cannabis in 2021. As cannabis use increases so does risk for cannabis use disorder (CUD). Conservative estimates suggest that CUD occurs in about 10% of regular users and up to one-third of those who use daily. A recent systematic review by Leung et al. (2020) suggests the prevalence may be twice that high with risk for CUD among emerging adults (18-24-year-olds) who engage in regular (weekly or daily) use of cannabis even higher. In 2023, more than one-third of adults aged 18–24 years (38.4%) reported using cannabis in the previous 12 months, as compared to 34.5% of 25–44 years 15.5% of adults aged 45 years and older; almost one in 10 (8.7%) reporting daily or almost daily cannabis use in the previous 12 months (Statistics Canada, 2024). In addition to risk for CUD, regular cannabis use poses other potential harms to emerging adults. Regular use has been found to affect brain maturation and to negatively impact cognitive functioning, especially learning and memory; and to increase risk of mental health problems, such as increased anxiety and psychosis (see Harris-Lane et al., 2021).
Cannabis research struggles to keep apace of its burgeoning use and is challenged by knowledge gaps in the impact of routes (smoking, eating) and modes of administration (e.g., blunts, bongs); measurement issues (e.g., relative percentage of tetrahydrocannabinol or THC and cannabidiol or CBD); as well as the differential effects of race and sex (see Streck et al., 2019). The present study was designed to examine sex differences in cannabis use and impacts in a sample of emerging adults. This stage of development is characterized by increased identity explorations, self-focus, instability, optimism, as well as a sense of feeling in-between adolescence and adulthood (Arnett, 2015). Many emerging adults navigate this transition at university where they strive to balance increasing personal agency with decreasing external (family, institutional) supports. This transition can be intense and full of opportunities, including increased drug use. Research shows that emerging adults with a pronounced sense of being caught in-between adolescence and adulthood are particularly prone to excessive substance use, in part because they think their use is transitory and won’t persist into adulthood (Smith et al., 2014).
Sex Differences in Cannabis Use and Indicators of Mental Health
Globally, most cannabis users are male (∼70%), with females comprising approximately 42% of cannabis users in North America. In Canada, more males use cannabis than females (52% vs. 49% in the 20-24-year-old age group (Canadian Cannabis Survey, 2021). Interestingly, usage decreased significantly between 2021 and 2022 for both sexes although the decrease was not significant for females (CCSA, 2022). With cannabis, like all other drug types, the sexes tend to differ in age of initiation, frequency of use, dosage, and addiction risk (Calakos et al., 2017). Generally, females (vs. males) use drugs less frequently and at lower doses to begin, but increase their use faster, escalate more rapidly to addiction (known as ‘telescoping’), report more frequent and severe cannabis withdrawal symptoms (see CCS, 2021; Cooper, 2018).
Self-medication is a well known motivational factor for cannabis use and a significant risk factor for CUD. Self-medication refers to the use of cannabis to reduce symptoms of physical or psychological distress. Wallis et al. (2022) investigated this high risk behaviour in a sample of 290 young American adults (aged 18–25; 45.6% female) and found that 76% indicated that they used cannabis to reduce problems, such as anxiety, sleep, depression, pain, loneliness, social discomfort, and concentration. Female (vs. male) participants showed higher rates of self-medication and a greater tendency to self-medicate for anxiety. Withdrawal symptoms of insomnia and loss of appetite were significant predictors of self-medication.
A recent study by Asselin et al. (2022) examined self-medication with cannabis in a sample of 489 adults (>21 years; median age = 34 years; 48% female) in the province of Quebec. About 25% reported exclusive medical use of cannabis. Self-medication targets included: anxiety (70%), insomnia (56%), pain (53%), depression (37%), ADHD (26%), headache/migraine (28%), muscle spasticity (17%), and bowel disease (11%). Two-thirds (66%) self-medicated for 2-to-5 conditions or symptoms; 21% treated six or more conditions. Men were more likely to self-medicate for ADHD and shyness; women were more likely to self-medicate for nausea. Almost one-third (32%) reported THC dosage >20%. Smoking was by far the main route of administration (81%).
It is not surprising that females (vs. males) are more apt to use cannabis to manage symptoms of psychological distress. Cross-nationally, it is well known that females have a higher lifetime prevalence of mood or anxiety disorders than males (Riecher-Rossler, 2017). Females’ increased risk is considered to be “true” as opposed to a sampling or reporting bias (see Eaton et al., 2012) and presumed to arise from a complex interplay of biopsychosocial factors, such as sex hormones, physiological responses to stress, higher rates of interpersonal stressors, experienced violence, childhood sexual abuse, lack of equality and discrimination (see Hartung & Lefler, 2019; Riecher-Rössler, 2017).
Using data from the 2002 and 2012 Canadian Community Health Survey’s Mental Health Component, repeated cross-sectional surveys of nationally representative samples of Canadians 15 years of age and older (n = 43,466), Halliday et al. (2019) found significant sex differences in the strength of the association between cannabis use and psychological distress. Females who used cannabis regularly (i.e., more than once per month) reported higher levels of psychological distress, including suicidal thoughts and attempts. Rabiee et al. (2020) examined the association between cannabis use, depression, and anxiety, across three Swedish cohorts born during periods of time in which cannabis potency would have increased (1955/65, 1970/75, 1980/1993). They found an association between cannabis use and anxiety in both the oldest and youngest cohorts, and between cannabis use and depression in the youngest cohort. Moreover, the association between cannabis use and depression was more pronounced among females in the youngest cohort (i.e., examined between 2000 and 2015). In sum, cannabis use appears to exacerbate females’ pre-existing risk for psychological distress (vis-à-vis males) and this risk may be increasing over time with increased potency of cannabis.
The frequency of cannabis use among females (vs. males) also increases risk for psychological distress. According to Canadian Cannabis Surveys (2021), as 12-month cannabis use increases, mental health ratings decrease. Statistics Canada (2024) found that, among daily users of cannabis, 8% women and 4% of men reported a mental health condition. The more frequent the cannabis use, the greater the proportion of daily users reporting a mental health disability, especially among females. Indeed, among daily using females, 43% reported a mental health disability versus 7% of females who had not consumed cannabis in the past month. This 36-percentage point difference dwarfed a seven-percentage point difference for males.
While the direction is unclear as to whether cannabis use leads to diminished mental health or whether individuals with poor mental health use cannabis to alleviate their symptoms, the link is concerning given that females (vs. males) are already predisposed to report more psychological distress, greater sensitivity to cannabis (Nia et al., 2018); increased risk for “telescoping” (Arkell et al., 2022); and more intense withdrawal symptoms during abstinence (Cooper et al., 2018).
Using cannabis to reduce psychological and physical distress, referred to as self-medication, is a significant risk factor for cannabis use disorder. To better understand this high-risk behavior, a sample of 290 young adults (ages 18–25; 45.6% female) were recruited from two U.S. universities in January and February of 2020 to complete a survey about their cannabis use and self-medication. Results: seventy-six percent endorsed using cannabis to reduce problems such as anxiety, sleep, depression, pain, loneliness, social discomfort, and concentration. When predicting reasons for self-medication with cannabis, logistic regression models showed that lower CUDIT-R scores, experiencing withdrawal, living in a state where cannabis was illegal, and being female were all associated with higher rates of self-medication. Withdrawal symptoms were tested to predict self-medication with cannabis, and only insomnia and loss of appetite were significant
Cannabis Use, Mental Health, and Cardiovascular Health
Cannabis use also has been linked to poor cardiovascular health. Research shows that cannabis use impacts both heart rate and blood pressure with heart rate increases ranging from 20%–100% in healthy individuals (Goyal et al., 2017). An increased heart rate can limit the heart’s ability to fill completely between contractions which, in turn, can compromise its ability to supply blood and oxygen to the rest of the body. The body’s ability to utilize oxygen (volume of oxygen or VO2) is a well-established prognostic marker of mental and physical health (Klepin et al., 2019). VO2 max levels indicate the maximum amount of oxygen the body can utilize during exercise. High VO2 is associated with increased lifespan, reduced risk for stroke, heart disease, diabetes, and cancer, as well as reduced anxiety and depression in clinical and non-clinical samples (Bang-Kittleson et al., 2022; de Sousa Junior et al., 2021). Low VO2 max is associated with greater risk of heart disease, and specific types of cancer (McTiernan et al., 2019).
One study compared heart rate in high THC, low THC, and placebo groups, and found that heart rate peaked 5 minutes after cannabis use, with both high and low THC groups showing significantly higher heart rates than placebo (105 bpm, 91 bpm, and 72 bpm, respectively). Heart rate remained significantly higher in both THC groups (vs. placebo) for more than 4 hours post cannabis use (see Brands et al., 2019).
Other indicators of negative cardiovascular health linked to cannabis use include heart arrhythmias and dysrhythmias (Richards et al., 2020). Studies have identified a temporal relationship between cannabis use and atrial fibrillation (Page et al., 2020) and increased risk of stroke (Jouanjus et al., 2017; Piano, 2017a). Indeed, one study found that cannabis use more than doubled (2.4×) one’s risk for a transient ischemic attack (TIA) (Jouanjus et al., 2017). A recent retrospective study found that frequent cannabis use (weekly or more) more than tripled (3.3×) the risk of stroke or TIA as compared to less frequent or no cannabis use (Page et al., 2020). Cannabis use has been linked to increased risk of myocardial infarction (MI) (Jouanjus et al., 2017). Lahda et al. (2021) found that both frequent cannabis consumption and smoking as primary mode of use increased risk of MI. In a sample of young adults, Piano (2017) found a 4.8-fold increased risk of MI within the first hour after use among cannabis (vs. non-cannabis) users. The risk remained high in the second-hour post-use with a 1.7-fold increase among cannabis users versus non-users.
Symptoms of cardiovascular disease, such as heart palpitations and shortness of breath, overlap with symptoms of psychological distress. This overlap presents challenges to a bifurcated health system where primary care practitioners in the medical system may overlook or lack adequate time to assess psychological factors - causal or correlates - of cardiovascular disease. For example, depression is three times higher in patients with cardiovascular disease but underdiagnosed in medical settings. Depression increases the risk (and poor prognosis) for cardiovascular disease largely through its impact on lifestyle, such as smoking, poor diet and treatment compliance, and decreased physical activity (see Chaddha et al., 2016).
Given that cardiovascular disease is the leading cause of premature death among Canadian women (top three being ischemic heart disease, stroke, and heart failure); it is concerning that so little is known about whether the indicators of cardiovascular disease vary by sex (see Norris et al., 2020). According to the Heart and Stroke Foundation of Canada (2018), two-thirds of the research on cardiovascular disease is focused on males. A better understanding of cannabis use among females (especially female emerging adults), and its impact on cardiovascular health and mental health, is much needed.
Sex Differences in Cannabis Use and Physical Activity
Regular physical activity is essential for maintaining good mental and cardiovascular health. Exercise is known to reduce symptoms of psychological distress, depression, and anxiety (see meta-analytic review by Singh et al., 2023), and to protect against the development of mental disorders (Anderson & Shivakumar, 2013; DeWolfe et al., 2020). Moreover, physical activity appears to moderate the impact of cannabis use (see Wade et al., 2020). A longitudinal study of young adult males found better mental health outcomes in those who maintained regular physical activity routines and fewer cannabis use disorder diagnoses in those who adopted new exercise routines (Henchoz et al., 2014). Another study of adult non-treatment seeking individuals (n = 12, 75% female) with cannabis use disorder showed reduced cannabis use and craving after 10 × 30-min treadmill exercise sessions over two weeks (Buchowski et al., 2011). Wade et al. (2019) found that higher aerobic fitness level moderated the impact of cannabis use on visual memory, executive function, and psychomotor speed.
Regular physical activity reduces one’s risk of suffering a sudden heart attack or other life-threatening cardiac event. It does this by modifying risk factors for cardiovascular disease via lowering blood pressure, reducing inflammation, helping to maintain healthy body weight, reducing stress hormones, functioning like a β-blocker to slow the heart rate and lower blood pressure, and improving muscle efficiency to pull oxygen out of the blood (see Johns Hopkins Medicine, 2023).
Unfortunately, females, especially female emerging adults, are less apt to engage in physical activity than their male counterparts (DeWolfe et al., 2020). Indeed, across the lifespan, females report significantly less participation in physical activity; in part because they perceive more barriers (vs. benefits) to physical activity (see Sabourin et al., 2011). Barriers can be internal, such as greater sensitivity to arousal-related sensations (Galbraith et al., 2022); and/or external, such as lack of time, appropriate space to exercise. While many (40%) post-secondary students fail to engage in the minimum amount of physical activity recommended to obtain such health benefits (150 minutes of moderate-to-vigorous physical activity per week; Government of Canada, 2022); females fail to meet these guidelines significantly more often than their male counterparts (De Wolfe et al., 2020). Consequently, females are missing the many physical and mental health benefits of exercise (Stathopoulou et al., 2006; Warburton et al., 2006).
Present Study
This study of cannabis-using emerging adults investigated sex differences in indicators of mental health (anxiety, depression) and cardiovascular health (e.g., physical activity levels, heart rate, VO2 max); self-perceptions of health and self-medication to manage symptoms of physical and mental health (e.g., pain, sleep, appetite). The following predictions were proffered: H1. Females (vs. males) would report more symptoms of psychological distress at baseline; poorer perceptions of mental and physical health; and greater use of cannabis to manage symptoms of physical and mental health. The number and type of self-medication targets (i.e., sleep, pain, anxiety, depression) was expected to be similar across sexes. H2. Females (vs. males) would report more indicators of poor cardiovascular health (high HR, low VO2max) plus lower levels of moderate-to-vigorous physical activity. H3. Females would be distinguished from males by more indicators of poor mental health and poorer perceptions of health (both physical and mental); lower levels of moderate-to- vigorous physical activity (PA) and VO2 max; and significantly higher heart rates (HR).
Methods
Participants
Participants were undergraduate students at a small university in rural Nova Scotia. Inclusion criteria required that participants be 18 and 25 years of age and using cannabis at least two times per week. This study was part of a larger longitudinal ecological momentary assessment study. All 209 participants completed two daily diaries for 14 days via a MetricWire application on their mobile devices. MetricWire was selected for use in this study because it leverages the ubiquity and immediacy of cell phones, especially among emerging adults, to improve response rates and minimize research fatigue, while providing data storage and analytics. Approximately half (n = 100) of the participants also wore a Fitbit Charge 4 pedometer. Most participants were in their first (35.0%) or second (31.6%) year of study; with fewer in their third (20.2%), fourth (9.1%), fifth or higher (4.0%) year of study.
Procedure
Participants were recruited through advertising posters around campus and email invitations to all students. Interested participants completed a short survey to determine eligibility (i.e., self-reported cannabis use at least two times per week, between 18 and 25 years of age, and possession of a mobile device). Eligible participants completed an online baseline survey of substance use history and behaviours. Participants downloaded the MetricWire application on their mobile device and, in this way, would receive random notifications twice daily to complete their daily diaries. Participants were given their personal login information for the application, guided through the registration process, and asked to go through a sample survey prior to the 14 days of diaries starting. Fitbit participants were asked to wear the device throughout the 14-day study period. Compensation up to $125 in Amazon gift cards ($25 for the baseline survey, $1.79 per survey or $25 per week, an additional $25 for completing 80% of the daily diaries as an incentive to complete as many as possible and finally $25 to those wearing the Fitbit) was given to the participants in the study.
Measures
Baseline Demographics and Cannabis Use
Participants were asked to provide basic demographic data (sex, year of study), as well as information on their cannabis use: preferred product type and strength, mode of administration, quantity, and frequency. This information is detailed in MacDonald-Spracklin et al. (2024).
Baseline Measures of Mental Health Patient Health Questionnaire
The PHQ-9 is a multipurpose screening tool for severity of depression (Kroenke et al., 2001). As a severity measure, the PHQ-9 score can range from 0 to 27, since each of the 9 items can be scored from 0 (not at all) to 3 (nearly every day). Question 9 is a single screening question on suicide risk. An additional item inquires as to: “How difficult have these problems made it for you to do your work, take care of things at home, or get along with other people?” with options ranging from: 1 = not difficult at all to 4 = extremely difficult. A PHQ-9 score ≥10 has a sensitivity of 88% and a specificity of 88% for major depression; 10-14 = moderate depression; 15-19 = moderately severe; and 20-27 = severe.
Social Anxiety Disorder Severity Scale
The SAD-D-10 is a 10-item measure of severity of symptoms of social anxiety (social phobia) in individuals aged 18 years and older (Craske et al., 2013). This scale addresses the limitations of other social anxiety measures as it is dimensional, time efficient, and assesses a broad range of symptoms. Each item asks the individual to rate the severity of their social anxiety symptoms during the past 7 days on a 5-point scale (0 = Never; 1 = Occasionally; 2 = Half of the time; 3 = Most of the time; and 4 = All of the time). The total score can range from 0 to 40, with higher scores indicating greater severity. LeBeau et al. (2016) found that individuals seeking help for social anxiety had a mean SAD-D-10 score of 25.7. With a non-clinical sample of Australian university students, Rice et al. (2021) found 25.7 or above (vs. below) indicated significantly poorer mental health.
Mini-Social Phobia Inventory
The Mini-SPIN is a 3-item screening tool for social anxiety disorders that asks participants to assess feelings of avoidance and fear of embarrassment over the past 7 days (Seeley-Wait et al., 2009). In the present study, participants were asked to indicate the frequency of each item on a 4-point scale ranging from 1 = not at all, 2 = several days, 3 = more than half the days, to 4 = nearly every day. The score was calculated by summing the 3 items, with scores of 9 or higher being potentially indicative of problems with social anxiety. [NOTE: Typically, Mini-Spin is scored on a 5-point Likert scale from 0 (not at all), 1(a little bit), 2 (somewhat), 3 (very much), 4 (extremely) with scores above 6 being indicative of social anxiety].
Panic Attack Questionnaire
The present study used two questions from the PAQ (Norton et al., 2008). First, respondents were provided with the definition of a panic attack (i.e., A panic attack is the sudden onset of intense fear or terror, often associated with feelings of impending doom, that is not a result of a real danger. Some of the most common symptoms experienced during an attack are dizziness, shortness of breath, chest pain or discomfort, and trembling or shaking.). Participants then were asked to indicate if they had EVER had a panic attack (lifetime). If they responded YES, then they were asked to estimate how many panic attacks they had experienced in the past year.
Baseline Measure of Self-Medication for Physical and Health Purposes
First, participants were asked to self-rate both their physical and mental health on a scale ranging from 1 = excellent, 2 = very good, 3 = average, 4 = fair, 5 = poor, or 6 = prefer not to say (see Hammond et al., 2018). Participants then were asked a series of questions to assess their use of cannabis for managing (coping with) physical health issues (i.e., headaches/migraines, pain, nausea/vomiting, lack of appetite, seizures, muscle spasms, to treat cancer, problems sleeping, other conditions to be specified, or never) and mental health issues (anxiety, depression, ADHD, PTSD, Bipolar/mania, psychosis, schizophrenia, drug/alcohol use, other to be specified, or never. Participants also were asked if they ever used cannabis for pain relief instead of prescription medications (e.g., opioids).
Indicators of Cardiovascular Health
Indicators of cardiovascular health were assessed with the Fitbit Charge 4 (FBC4) pedometer. Physical activity was measured in metabolic equivalents of task or METs. One MET equals approximately 3.5 mL of oxygen consumed per kilogram of body weight per minute. Typically, <1.0 METs = sedentary; 2.0–3.0 METs = light activity, 3.0–6.0 METs = moderate activity; and >6.0 METs = vigorous activity. In the present study, FITBIT participants were assessed by the percentage of time spent at each level of exertion (sedentary, light, moderate, vigorous). Heart rate (HR) data was collected intra-day, minute-by-minute. HR for the hour during which participants reported using cannabis was included in the analysis. VO2 Max is an indicator of fitness measured in millilitres of oxygen used in 1 minute per kilogram of body weight. The maximum amount of oxygen a body can utilize during exercise considering age, weight, sex, resting and active heart rates. VO2 max data was collected intra-day, minute-by-minute. VO2 max for the hour in which participants reported using cannabis was included in the analysis. Support for use of wearable fitness devices to assess VO2 max is provided by Bayshtok et al. (2023) who found that Apple Watch data on peak VO2 functioned as a surrogate index of cardiac fitness. Also, Freeberg et al. (2019) compared the accuracy of the FBC2 VO2 max to a maximal exercise test (gold standard) and non-exercise VO2 max prediction equation and found that the FBC2 provided a consistent, unbiased prediction (albeit overestimating) of VO2 max levels in 30 young, healthy men and women.
Data Analytic Strategy
Analyses were conducted using R version 4.1.3 (R Core Team, 2022) with package lmerTest version 3.1–3 (Kuznetsova et al., 2017) for the multilevel model analysis. A priori power analysis using G*Power version 3.1 (Faul et al., 2009) to determine the minimum sample size adequate for testing the study hypothesis indicated that to achieve 95% power for detecting a medium effect size (0.25) at a significance criterion of α = .05 was N = 112 for discriminant function analysis with two groups (females vs. males) and 11 dependent variables: generalized, social, and panic anxiety; depression; minutes of moderate-to-vigorous exercise; resting heart rate; VO2 max; self-ratings of mental and physical health; number of mental and physical self-medication targets.
Results
Most participants reported using cannabis daily or almost daily (54.5%) while others reported using 5-6 times per week (12.8%), 3-4 times per week (17.2%), and twice a week (15%). Females consumed cannabis less frequently than males and were more apt to use moderate versus more potent strength products. The Fitbit sample (n = 100) did not differ significantly from the non-Fitbit sample (n = 106) in year of study (p = .57), age of first use of cannabis: X age = 16.4 (1.57) versus 16.7 (1.70), F = 1.17, p = .42; or frequency of cannabis use during past 30 days (p = .66).
Hypothesis Testing H1: Indicators of Mental Health
Descriptive Statistics by Sex.
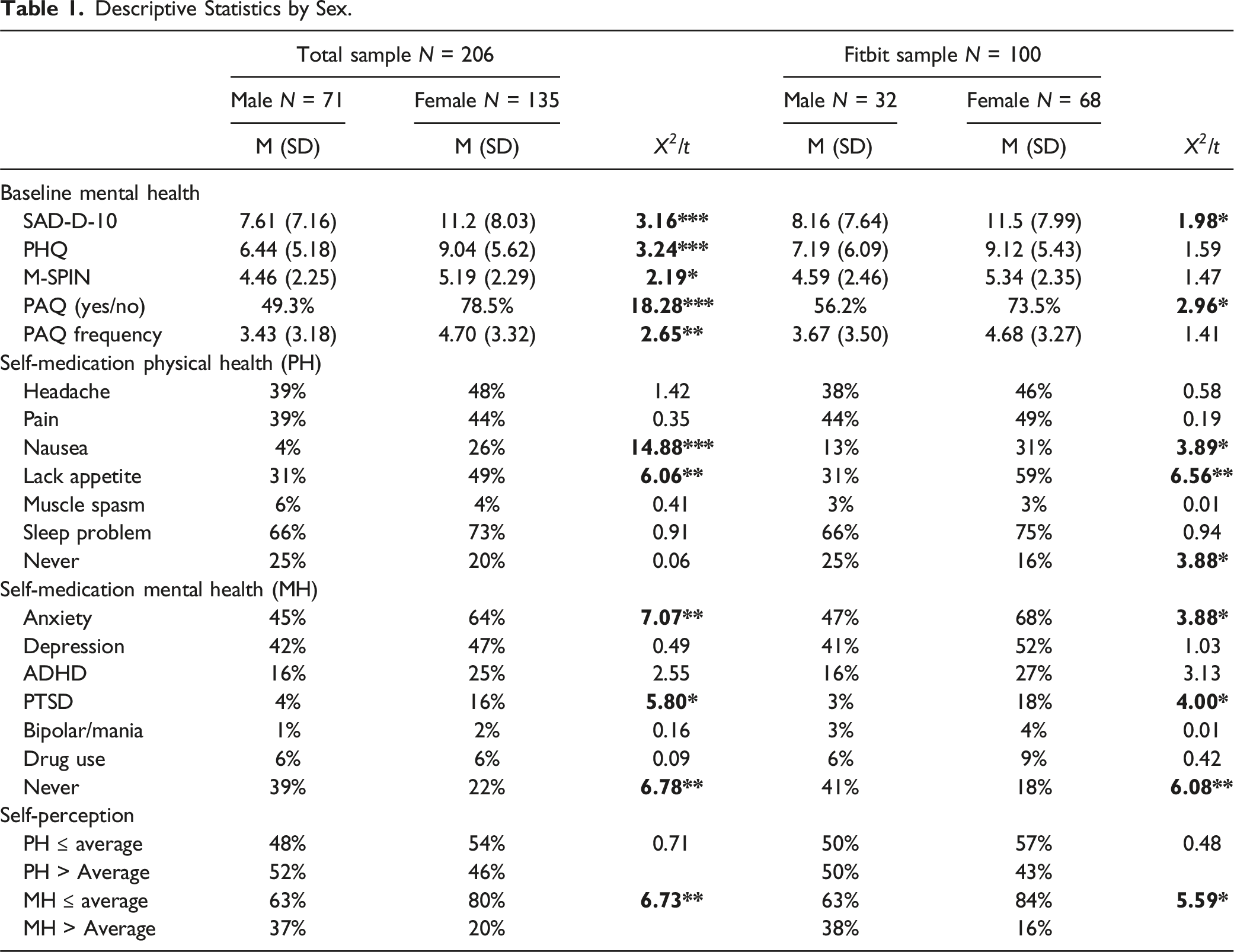
As predicted, the most frequently reported targets of self-medication (i.e., sleep, pain, anxiety, depression) were similar for both sexes. The two groups differed significantly, however, in proportion within each group that endorsed specific targets for self-medication. Females (vs. males, respectively) were significantly more apt to use cannabis to treat symptoms of nausea (31% vs. 13%), lack of appetite (59% vs. 31%); anxiety (68% and 47%); and PTSD (18% vs. 3%). By comparison, males (vs. females) were significantly more apt to claim that they NEVER used cannabis for self-medication purposes. See Table 1.
To test for sex differences in self-perceptions of physical and mental health, cells were collapsed into “at or below average” (poor, fair, average) and “above average “(very good, excellent). There were no sex differences in perceptions of physical health for either the total or FITBIT sample. Significant sex differences did emerge in perceptions of mental health for both the total and FITBIT samples, with females (vs. males) more apt to report their mental health as being at or below average, and males more apt to perceive it as being above average (X 2 = 9.15, p = .002 and X 2 = 7.66, p = .006, respectively).
Hypothesis Testing H2: Indicators of Cardiovascular Health in Fitbit Sample
Resting heart rates for the Fitbit sample, averaged over the 2-week study period, are included in Table 1. Females’ average heart rates were significantly higher than males. For both females and males, resting heart rate was inversely correlated with VO2 max levels (−.62 and −.35, respectively); in turn, VO2 max was inversely correlated with moderate-to-very active minutes of exercise (−.21 and −.40, respectively).
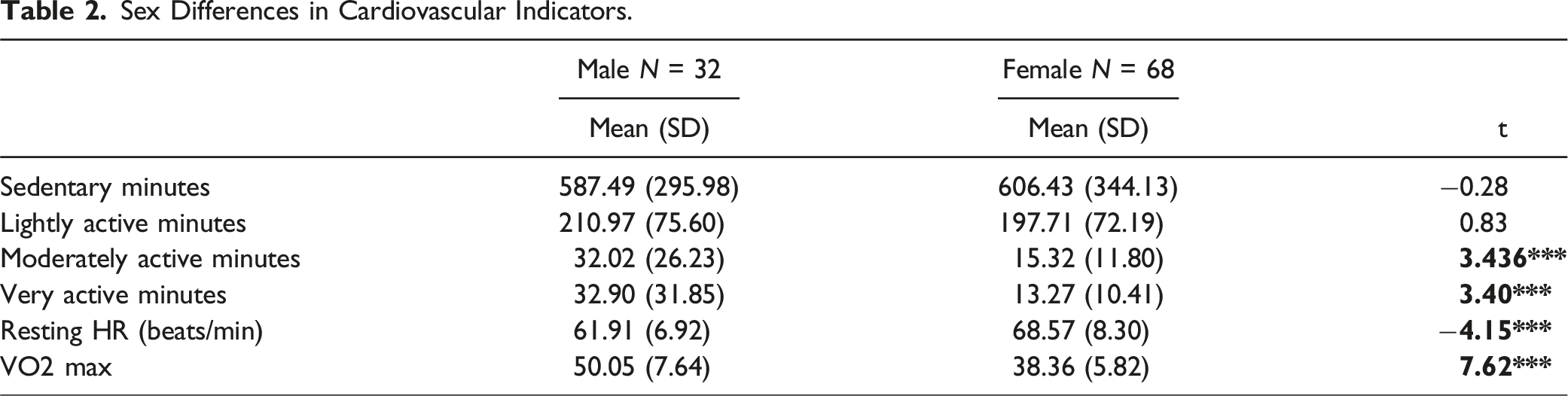
The average VO2 max level for the Fitbit sample was 42.3 mL/kg/min (SD = 8.48), with males averaged a significantly higher VO2 max than females (50.1 vs. 38.4, respectively). Most notably, VO2 levels for females fell at the 30th percentile for females between the ages of 20–24 years, while the average VO2 levels for males fell at the 70th percentile for males between the ages of 20–24 years (see Hoffman et al. for Statistics Canada, 2019). Females and males did not differ significantly in time spent in sedentary pursuits but differed significantly at every other level of physical activity. Females engaged in significantly fewer minutes of light activity, moderate activity, and vigorous activity than males. See Table 1.
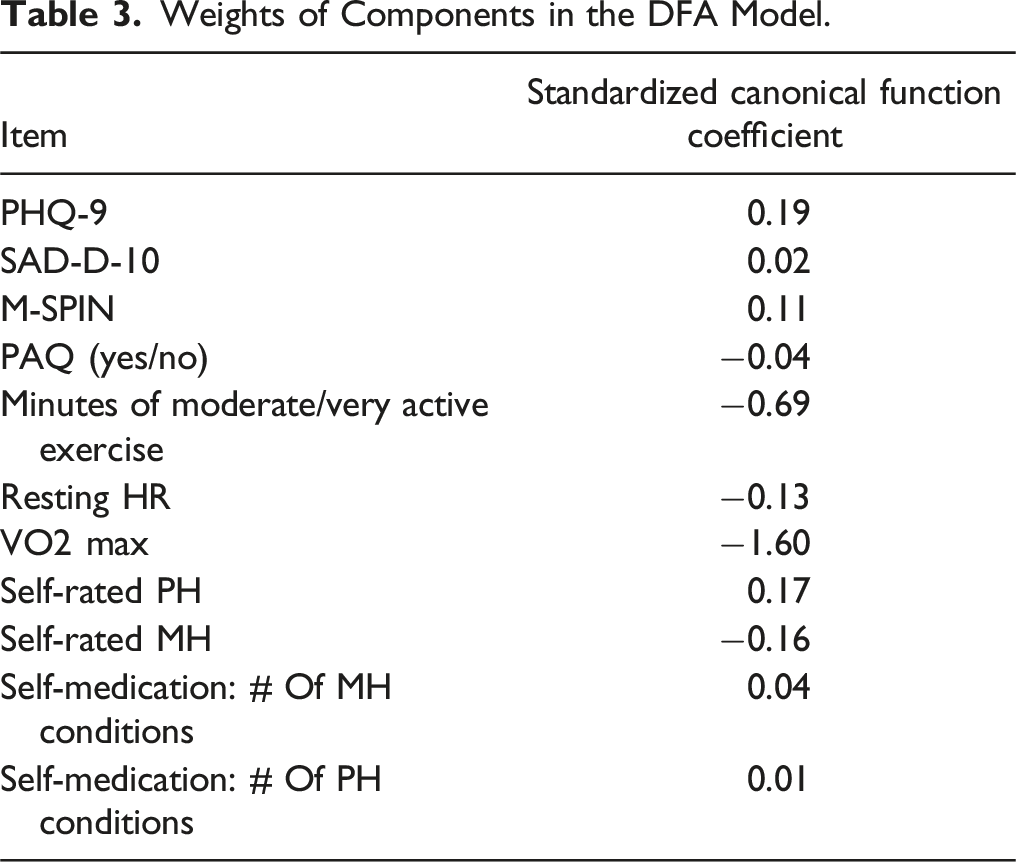
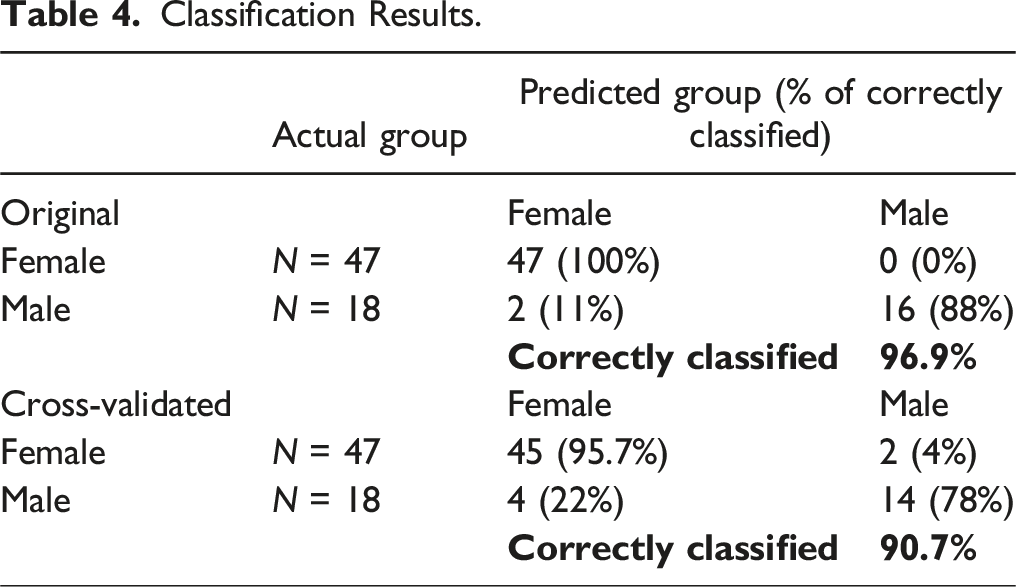
Hypothesis Testing H3: Discriminant Function Analysis
Of particular interest to the present study was identifying which indicators of mental and cardiovascular health could best discriminate between male and female cannabis-users. Linear discriminant analysis with 11 dependent variables (i.e., key indicators of mental health and cardio fitness). Only 65 cases had complete biometric data.
Sex Differences in Cardiovascular Indicators.
Weights of Components in the DFA Model.
Classification Results.
Discussion
This study investigated sex differences in indicators of mental and cardiovascular health in a sample of cannabis-using emerging adults. Consistent with the preponderance of literature to date (e.g., Prieto-Arenas et al., 2022), males used more cannabis, more often, and at greater levels of potency than females. Despite males’ greater use of cannabis, the scientific evidence to date indicates that the associated negative consequences (e.g., increased risk of CUD, mental health symtoms) are greater for females. The true picture of sex and gender differences in cannabis use and impacts remains to be seen, however, and awaits further research that can disentangle the myriad of biopsychosocial factors at play, such as sex differences in gonadal hormones, sex differences in stress and HPA functioning, sex dimorphisms in cannabinoid receptors, sex differences in types of interpersonal stressors, sex differences in equality and discrimination, etc. These factors are especially pertinent for emerging adults for whom regular cannabis use can negatively impact brain maturation and cognitive functioning and increase risk of mental health problems (see Harris-Lane et al., 2021).
Consistent with Hypothesis 1, females (vs. males) reported significantly more psychological distress (anxiety, depression) at baseline; greater use of cannabis to cope with symptoms of both physical (i.e., nausea, lack of appetite) and mental ill-health (i.e., anxiety, PTSD); poorer perceptions of their mental health. Consistent with Hypothesis 2, females (vs. males) revealed more risks to cardiovascular health, including higher resting heart rate, lower VO2 max, and less engagement in moderate-to-vigorous activity. Consistent with Hypothesis 3, the variables that significantly distinguished females from males were: 1. reduced VO2 max; 2. fewer “moderate-to-very active” minutes of physical activity; 3. Higher depression scores plus poorer perceptions of mental health and physical health. We discuss each of these variables as potential targets for enhancing the mental and cardiovascular health and resilience of cannabis-using, emerging female adults.
On average, females in the present study revealed significantly lower VO2 max levels than males. While not entirely surprising to find VO2 max levels lower for females than males, it was surprising that the average VO2 level for this sample of cannabis-using females fell at the 30th percentile for females between the ages of 20–24 years. In other words, 70% of females of the same age would be expected to score higher. Given the mental and physical health risks associated with low VO2max, this finding is particularly concerning for this sample of cannabis-using emerging adult females. By comparison, the average VO2 level for males fell at the 70th percentile for males between the ages of 20–24 years (Hoffman et al. for Statistics Canada, 2019).
In addition to sex, VO2 max levels can vary by age (declining for both sexes over time), weight, active and resting heart rates. While resting heart rates for females in the present study were significantly higher than males, both were lower than normal (68.5 and 61.0, respectively). The average heart rate for adult females ranges between 78 and 82 beats, while adult males ranges between 70 and 72 beats per minute. The sex difference in heart rate is largely attributable to heart size, which is typically smaller in females than males (Prabhavathi et al., 2014). As expected, heart rate and VO2 max were inversely correlated for both females and males although the magnitude of shared variance was substantially higher for females (38% vs. 22%, respectively).
One of the best ways to improve VO2 max is to engage in physical activity at or near maximum heart rate. Females (vs. males) in the present study engaged in fewer minutes of physical activity at every level – light, moderate, and vigorous. This finding fits with a growing body of evidence that females across the lifespan, but especially emerging adult females, participate in significantly less physical activity. Lack of participation in physical activity limits females’ ability to access its myriad cardiovascular health benefits (e.g., higher VO2 max, lower heart rate), mental health benefits (e.g., reducing depression), and protection against the development of mental disorders (Anderson & Shivakumar, 2013). Moreover, physical activity appears to moderate the impact of cannabis use (see Wade et al., 2019, 2020). A longitudinal study of young adult males found better mental health outcomes in those who maintained regular physical activity routines and fewer cannabis use disorder diagnoses in those who adopted new exercise routines (Henchoz et al., 2014). Another study of adult non-treatment seeking individuals (n = 12, 75% female) with cannabis use disorder showed reduced cannabis use and craving after 10 × 30-min treadmill exercise sessions over two weeks (Buchowski et al., 2011). Wade et al. (2019) found that higher aerobic fitness level moderated the impact of cannabis use on visual memory, executive function, and psychomotor speed. Because female emerging adults are already at increased risk for various forms of psychological distress (Naragon-Gainey, 2010), the importance for this population to be facilitated access to the benefits of physical activity is paramount.
A recent systematic review by Singh et al. (2023) examined the effects of physical activity on psychological distress, including depression and anxiety. This meta-review included 97 systematic reviews, 1039 unique RCTs, and over 128,000 participants. Results showed that physical activity provided positive impacts across all studies and was 1.5 times more effective in some cases than counselling or medication in tackling depression. Indeed, some of the greatest benefits were seen in people with depression, pregnant and postpartum women, and otherwise healthy individuals. All modes of physical activity (i.e., aerobic, resistance, yoga, mixed-mode exercise) were effective but moderate and higher intensity levels rendered greater benefits. Interestingly, data showed that the largest benefits appeared to come from shorter interventions, with small weekly durations of physical activity being more effective than longer. Singh et al. (2023) concluded that exercise should be considered as a first option treatment for depression and anxiety.
The evidence is clear that physical activity can mitigate the negative cardiovascular and mental health impacts of cannabis use. Given that more states are moving toward the legalization of cannabis, identifying factors that can mitigate risk becomes increasingly important especially for emerging adults. This developmental stage is marked by instability as emerging adults seek to navigate the transition between adolescence and adulthood (Arnett, 2015). The self-focus and optimism required for successful navigation can impede their ability to accurately assess the short- and long-term risks of opportunities, such as drug use. More public health and marketing initiatives should be directed at emerging adults to heighten their awareness of the risks of regular cannabis use and the particular risks for both males and females. Messaging would benefit from a harm reduction approach, such as encouraging delay or reduction of use so as to avoid impact on brain maturation; choosing low-potency products (low THC and/or high CBD content) and less risky ways of use than smoking. Emerging adults also could benefit from education about risk assessment, generally, and how the more risk factors you bring to a situation (e.g., predilection to anxiety, family history of psychosis) and the more risks you assume in the situation (e.g., combining cannabis and alcohol use), the more likely you are to harm your health. Of course, promoting physical activity and providing more opportunities for emerging adults to participate in physically active endeavours could render many benefits for individuals and society.
Limitations
Findings of the present study must be considered in light of certain limitations. First, data collection for this study was impacted by the COVID-19 pandemic. The imposition of public health guidelines on social gatherings and events, including university classes, may have altered substance use patterns for this sample of undergraduates. Second, some participants did not wear their Fitbit consistently and some data had to be excluded from the analysis. Despite removal of these participants, the sample size was higher than expected for indices of cardiovascular functioning. Third, we were unable to assess levels of THC versus CBD in cannabis products, which could have impacted participants’ reporting. For example, research suggests that THC may trigger more anxiety symptoms but cause more sedation, while CBD may reduce the anxiety impact of THC and yield more potent analgesic and anti-inflammatory properties (see Dannon et al., 2004). Fourth, the present study used an abbreviated version of the PAQ (Norton et al., 2008) with one Yes/No item inquiring about history of panic (lifetime) and a second item asking about number of panic attacks in past-year. Given our findings (i.e., relationship between panic, heart rate, and VO2 max), future research would benefit from a better-defined timeline and assessment of panic attack characteristics, as well as including measures of generalized anxiety and anxiety sensitivity (i.e., specific fear of physiological sensations). Fifth, the generalizability of present results is limited by the present sample being predominantly Caucasian, cis-gender, emerging adults attending a small rural university in Atlantic Canada.
Finally, there are limitations to using Fitbits to measure VO2 max. The gold standard for assessing VO2max is maximal exercise testing in controlled conditions. The Fitbit used in the present study (FBC4) predicts VO2max in mL/kg/min by calculating a “cardio fitness score” based on the relationship between running pace and heart rate (HR). The more accurate the indices, the more accurate the scores. For example, wearing the tracker while sleeping would provide a better resting heart rate estimate. Predicting VO2max with a wrist worn device offers the advantages of being cheaper, more accessible, and less strenuous testing methodology, and empirical assessment of accuracy is beginning to accrue. In a recent study, Bayshtok et al. (2023) found evidence to support the utility of peak VO2 measurements via wearable devices (e.g., Apple Watches) in early identification and screening of cardiac fitness for the general population and those at increased risk of cardiovascular disease.
Conclusions
Findings from this study suggest that female emerging adults who use cannabis regularly may be uniquely vulnerable to cannabis-related risks. This sample of female undergraduates showed potentially greater risk for cardiovascular ill-health (i.e., lower VO2, higher heart rate) and mental ill-health (i.e., depression) as compared to males. Moreover, as compared to males, these females showed diminished levels of physical activity; a known strategy for reducing indicators of both physical and mental ill-health and enhancing resilience (see Singh et al., 2023). Given that females (vs. males), in the absence of cannabis, are predisposed to greater risk for cardiovascular disease (Ezekowitz et al., 2020) and psychological distress (e.g., depression, anxiety), cannabis may pose unique consequences for emerging female adults. Findings of this study confirm the need to learn more about cannabis use impacts on females, and to promote physical activity as a potential buffering agent against potential deleterious effects of regular cannabis use among this at-risk population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council (430-2019-00726) and Canadian Centre for Substance Use and Addiction (Closing the Gaps).
Transparency and Openness Statement
The raw data, analysis code, and materials used in this study are not openly available but are available upon request to the corresponding author. No aspects of the study were pre-registered.