
Abstract
Caring for a parent during emerging adulthood may be a disruptive and non-normative experience. Despite the growing prevalence of emerging adult (EA) caregivers, there remains limited research. We explored the experiences of EAs caring for parents living with advanced disease. Interviews were conducted with 12 EA daughters and analyzed using constructivist grounded theory. The core category was identified as negotiating accelerated adulthood, a dynamic interplay between feeling more of an adult than before and the paradoxical feeling of I’m not where I should be. Prior to the core category, participants’ caregiving role is assumed. Availability of support influenced participants’ process of negotiating accelerated adulthood. Findings highlight the uniqueness and developmental impact of this experience. Results suggest an interplay of different factors with how the role is assumed, appraised, and experienced by EA daughters. Greater awareness of these experiences may inform the development of tailored interventions and strategies for EA caregivers.
Background
The experience of disease poses profound burden on informal caregivers who provide necessary support for their loved ones. Informal caregivers have contributed 5.7 billion hours of unpaid support annually, at a striking estimate of $97.1 billion or 4.2% of Canada’s GDP (Fast et al., 2023). Beyond support provision, caregivers experience significant changes to daily living and social or familial roles, leading to impairment in psychosocial, occupational, and economic functioning (Adelman et al., 2014).
The overall demand for caregivers continues to rise, in part due to the aging population, prolonged life expectancy with increasing health needs, and overwhelmed public healthcare system (Dattani et al., 2023; Haley & Elayoubi, 2023). Along with broader societal trends (e.g., later childbearing, smaller families), these factors have shifted the societal landscape of caregiving, and young and emerging adults (ages 18–29) are increasingly assuming caregiving roles to meet the growing need (Bleakney, 2014; Chadi & Stamatopoulos, 2017). In Canada, approximately one-quarter of emerging adults are caring for a loved one with a long-term health condition, disability, or aging needs, comprising the “hidden army” of young carers (Bleakney, 2014; Stamatopoulos, 2015). Caregiving during emerging adulthood may be less normative and represent a distinct experience compared to other life stages. Emerging adulthood is marked by significant psychosocial and cognitive transitions (Arnett, 2000; Arnett et al., 2014), typically characterized with five key features: (1) identity exploration, (2) instability, (3) self-focus, (4) feeling “in-between” adolescence and adulthood, and (5) optimism about the future. Caregiving responsibilities, which require a significant investment of time and other resources, may impede the typical emerging adult trajectory, making explorations of identity, autonomy, and new possibilities more challenging.
Indeed, previous researchers have found that emerging adults providing general care experience a number of challenges, including higher levels of parentification (i.e., role reversal within the family system whereby the child assumes roles and responsibilities typically performed by their parent (Hooper & Doehler, 2012)), anxiety, depression, smoking, and financial strain compared to older adult caregivers and similarly aged non-caregivers (Boumans & Dorant, 2018; Greene et al., 2017; Grenard et al., 2020; Koumoutzis et al., 2021). Previous research has also highlighted the negative impact of caregiving on critical tasks that define this period, including differentiating from family of origin, time spent with close others, and professional development (Dellmann-Jenkins et al., 2001). Although there has been promising attention towards the experiences of emerging adult caregivers, this population remains relatively understudied (e.g., compared to middle-aged or older adult caregivers) and researchers have called for greater attention to this “distinct carer cohort” (Day, 2015; Kent, 2020). Recent reviews highlight gaps in the literature, including differentiating between relationship type, severity or type of illness of the care receiver, and importantly, how such factors may impact caregiver outcomes (Chevrier et al., 2022; D’Amen et al., 2021).
One subgroup that has received limited attention is emerging adults who are caring for a parent with advanced disease (i.e., an incurable and life-limiting disease that progresses over time and impacts functioning). In addition to the demands of caregiving, these emerging adults are also facing the anticipated loss of a parent, which may further disrupt the developmental transition and significantly impact well-being during this life stage. In a qualitative study of bereaved Israeli caregivers (20–35 years old at the time of caregiving) the identified themes included modes of taking on and performing the caregiving role, feeling like “life was on hold,” and the impact of caregiving on self-development (Goldblatt et al., 2019). In another study in the United States, young adults (18–35 years old) caring for a parent with advanced cancer during the COVID-19 pandemic experienced lower caregiving efficacy, well-being, and bereavement compared to pre-pandemic (Kastrinos et al., 2023). Although these studies suggest that caring for a parent with advanced disease can be atypical and disruptive to emerging adult development, they rely on retrospective data (i.e., interviews with bereaved caregivers) and cover a broader age range than what is typically considered emerging adulthood. An examination of the advanced disease caregiving experience during emerging adulthood and among those who are currently living this experience is needed to better ground the findings within the developmental context and limit the impact of long-term recall and processing. Further exploration in more diverse samples is also needed.
The Current Study
Taken together, the research to date highlights the challenges caregivers face and further identifies emerging adults caring for a parent with advanced disease as a unique population who remain underrepresented in the literature. Despite calls to examine the emerging adult caregiving experience from a developmental perspective (Chevrier et al., 2022), there is limited literature on this specific population. A qualitative approach is well suited to explore in-depth how emerging adult caregivers experience this time of life while in the caring role. The goal of this qualitative study was to explore the experiences of emerging adults caring for a parent living with advanced disease.
Methods
Study Design
We used constructivist grounded theory to understand the experiences of emerging adults caring for parents living with advanced disease and develop a conceptual framework (Charmaz, 2014). A social constructivist paradigm was chosen based on its interpretive approach and ability to gain insight into the phenomenon and complex subjective experience of caregiving in emerging adulthood. This framework emphasizes the co-construction of “reality,” experiences, and meanings throughout the interview process and within the participants’ sociocultural contexts (Charmaz, 2014; Guba & Lincoln, 1994). It inherently acknowledges the researcher’s own subjectivity and involvement in the co-construction and interpretation of the data, rather than an objective observer. Interviews were conducted and analyzed by the first author (ET) who acknowledged her positionality as an East Asian woman, holding predominantly Western cultural values, who is within the same age range as emerging adult participants, and has personal caregiving experience albeit not within the context of caring for a parent. ET is a clinical psychology graduate student with significant experience working in the field of end-of-life care and bereavement. She was well positioned to engage with emerging adult participants to permit exploration and co-construction of meaning in the context of caregiving. As a supervisor, researcher, and clinical psychologist specializing in emerging adult wellbeing, AG offered guidance on positioning the caregiving experience within the developmental context of emerging adulthood, informed by a commitment to understanding the nuanced needs of this demographic. RN is a clinical psychologist with expertise in family caregivers of cancer patients.
Participants
Emerging adults were recruited via online social media and university-affiliated platforms, relevant community organizations, and hospital websites. Eligibility criteria included: being 18–29 years old, sufficiently fluent in spoken English, residing in Canada, and currently providing unpaid support for a parent living with an advanced disease (i.e., an incurable and life-limiting disease that progresses over time and impacts functioning). Interested participants were asked to complete pre-screening eligibility questions. Based upon responses received, a purposeful sampling strategy was used to identify and capture a diverse range of experiences and identities. Participants received an honorarium in the form of a $20 gift card.
Data Collection
One-on-one, semi-structured interviews were conducted online via Microsoft Teams between January 2023 and July 2023 by the first author. Interviews began with broad open-ended questions about the experience of caring for a parent with advanced disease, their current wellbeing, and their parent’s illness journey. Probes then followed about the impact of caregiving on their developmental tasks (e.g., What are your personal goals (e.g., in life, career, relationships)? How has caring for [Parent] affected your ability to pursue your own identity and goals?), identity, values and worldview, and thoughts about the future (e.g., What do you think of when you think of the future? Have you discussed these thoughts with [Parent]?); the impact of disease and caregiving on their relationships with their ill parent, other family members and friends (e.g., How has your relationship with [Parent] changed at all since their diagnosis? Have your relationships with others changed over time?); their coping and wellbeing; challenging and rewarding aspects of caregiving; and their support needs. Participants completed demographic questions prior to the interview to help determine the heterogeneity of the sample and inform ongoing sampling decisions. This study was approved by the University of Toronto Research Ethics Board (#43126). All participants provided informed consent.
Data Analysis
Constructivist grounded theory methodology was employed (Charmaz, 2014). Analysis began with initial coding where the transcript was reviewed line by line to inductively identify and highlight codes. Next, focused coding allowed for organization and categorization of codes into themes. Ongoing constant comparison was used to identify similarities and differences between and within participant accounts and categories. Finally, theoretical coding accounted for connections between the data and broader themes to construct a theoretical model. To facilitate theoretical sampling (i.e., “seeking and collecting pertinent data to elaborate and refine categories in your emerging theory” (Charmaz, 2014, p. 192)) and data collection in the later stages of the analytic process, data were collected and analyzed simultaneously. For example, interview questions were modified over time to refine and probe further about themes that emerged in earlier interviews. In later interviews, participants were asked about emerging common themes from earlier interviews (e.g., difficulty relating with peers, the impact of culture on caregiving expectations and their own caregiving experience) and the developing theory and whether they resonated with their experience. This also offered opportunity for constructive feedback and refinement of the theoretical model to achieve resonance, an important quality criterion for constructivist grounded theory studies (Charmaz, 2014). Data collection and theoretical sampling continued until theoretical saturation was achieved in the emerging theory (i.e., “when the complete range of constructs that make up the theory is fully represented by the data” (Starks & Trinidad, 2007)).
To enhance rigour and trustworthiness of data, memo writing and reflexive journaling were documented throughout the data collection and analysis phases (Lincoln & Guba, 1985). Member checking techniques were employed to verify findings with participants, aligned with the principle of co-construction. Informal member checking was conducted throughout the interview, including paraphrasing, asking for clarification of intended meaning, confirming interpretations, and summarizing at the end to confirm understanding and offer opportunities for clarification. This question-answer validity technique allowed for clarification of intended meaning while maintaining contextual nuances (Roller & Lavrakas, 2015). Reflexivity (i.e., gaining “methodological self-consciousness” (Charmaz, 2017)) is critical to achieving credibility, one of the main quality criteria for constructivist grounded theory studies as proposed by Charmaz (2014). To promote a strong reflexive stance throughout the analytic process, ET held regular meetings with senior team members (AG, RN) and consulted at a qualitative seminar group to refine themes; critically review biases, discrepancies, and positionalities; and consider alternative interpretations. Ongoing collaborative team discussions and member checking helped to achieve a consensual, co-constructed interpretation of the data.
All interviews were audio-recorded and transcribed verbatim using a machine transcription service (temi.com). All transcripts were de-identified and verified for accuracy. Transcripts were managed using NVivo12 qualitative data analysis software. Descriptive statistics were analyzed to characterize the sample.
Results
Participants
Participant Characteristics (n = 12).
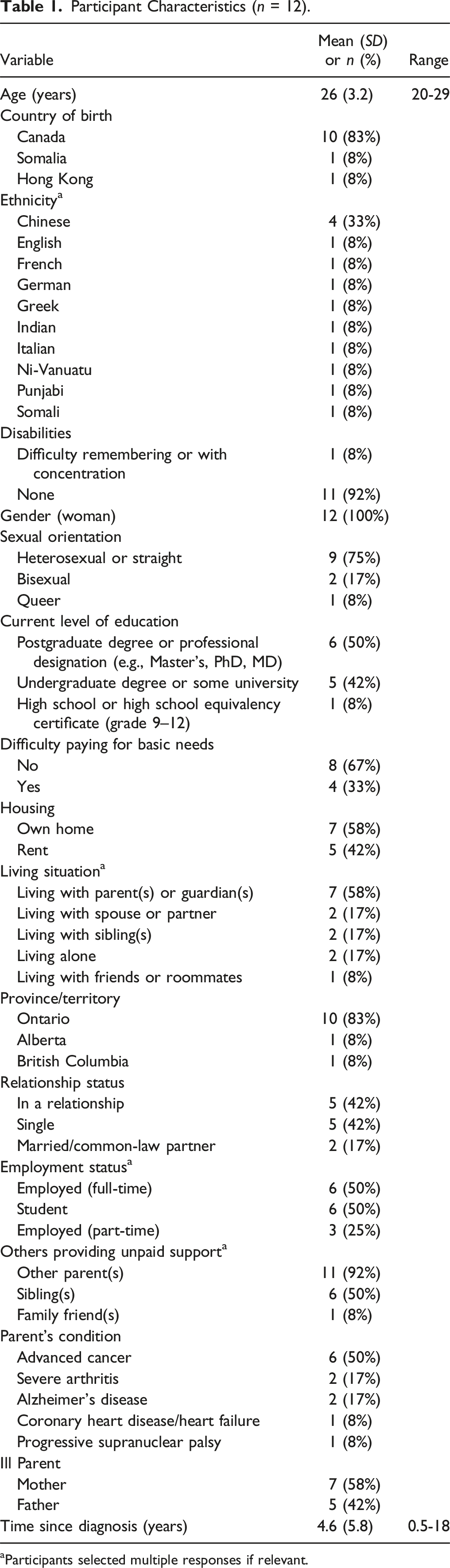
aParticipants selected multiple responses if relevant.
Findings
The findings highlight the dynamic experience of emerging adults caring for a parent with an incurable, terminal illness. The analysis identified negotiating accelerated adulthood as the core category, representing the perceived uniqueness of participants’ caregiving experience within their developmental context. This central phenomenon emerged as participants felt like more of an adult than before while also struggling with the paradoxical feeling of I’m not where I should be. Prior to the core category, participants’ caregiving role is assumed following their parent’s diagnosis. The contextual factor of availability of support influenced participants’ process of negotiating accelerated adulthood. The core category and its associated characteristics formed the dynamic conceptual model of parental caregiving in emerging adulthood, which is illustrated in Figure 1 and described below. The model of parental caregiving in emerging adulthood.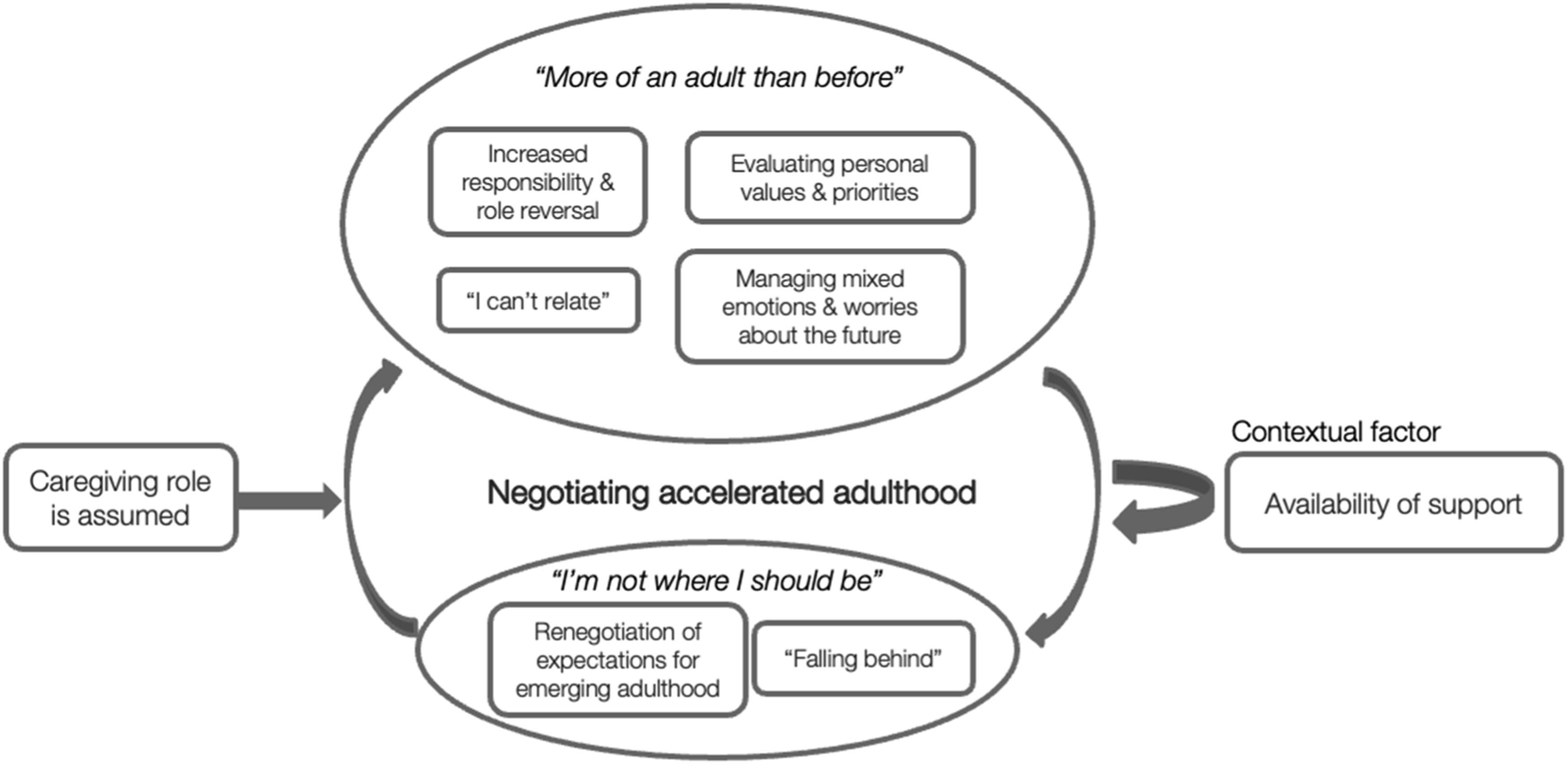
Negotiating Accelerated Adulthood
The core category was identified as negotiating accelerated adulthood. After assuming their caregiving role, participants experienced many aspects of caregiving as catalysts towards an “accelerated” sense of adulthood. At the same time, they struggled with some elements of their experience that made them feel developmentally “behind” or “stuck,” given the perceived boundaries imposed by caregiving. The negotiation between these two “paradoxical” states (i.e., between feeling “more of an adult than before” and feeling “not where they should be”) within a sense of accelerated adulthood emerged as the core experience. This was described by participants as feeling “mostly adult” while in some ways feeling “more like a child.” One participant shared this duality further: “I still feel like there's some parts of my life where I feel very much like a kid or not really like an adult. I guess just with the whole moving out piece, still living with my mom or my parents, I still feel like a bit of a kid [laughs] […] but I don't know, with this experience, I definitely feel like I don't know many people my age that have had to deal with this, even people older than me. I definitely feel like I have some type of life experience now that makes me feel more adult-like.” (P5)
Another participant shared similar reflections on her progress of reaching adulthood: “In some ways, yes. And I think just caregiving as well is just such a- the way that it reverses your role with your parent, you can't help but feel like you're more of an adult than you were before you had to do all of that stuff. So yes. In some ways, weirdly, it's almost like the first time in my life where I've kind of reflected and felt like I'm not at the point in my life where I feel like I should be […] it's almost made me I guess self-conscious about some of the things that are considered like quote unquote adult, like milestones, and whether or not I'm kind of behind on those, just because I guess I feel so aged in a different way.” (P6)
“More of an Adult than before”
The feeling of being “more of an adult than before” and needing to “grow up all of a sudden” was described by participants in various aspects of their lives: “I entered adulthood earlier than expected” (P12). The interrelated elements of this experience were: (1) increased responsibility and role reversal; (2) evaluating personal values and priorities; (3) I can’t relate; and (4) managing mixed emotions and worries about the future.
Increased Responsibility and Role Reversal
Participants described assuming unexpected and additional “responsibility” and experiencing “role reversal” in their family context. These responsibilities were perceived to reflect their broader preoccupation of needing to support their family and prepare for the future.
Participants detailed increased financial responsibilities, including finding employment, contributing to their families’ bills, and budgeting. Many described changes to their families’ financial situation as the illness impacted their parents’ ability to work, particularly when the ill parent was the main provider. As one participant shared: “Financial situations have been difficult because he hasn't been in work. And so we've been spending less money wherever we can, like not opening the light for very long, like using the food bank. So I guess those parts of daily life have changed [...] We also had to look into getting part-time jobs and it's not a huge thing right now, because the rest of my family is like, don't get into jobs, just study [...] it's kind of felt like we were alone as teenagers, and we had to deal with this ourselves because my mom was still in like a lot of denial. I learned how to do taxes and budgeting and then my brother learned how to drive and yeah, just a lot of those adult stuff.” (P9, currently living at home with parents and sibling, completing undergraduate studies, working part-time)
Providing emotional support for their parent was described as “challenging” and “draining,” but also necessary: “It’s definitely changed from that standpoint where I feel like I’m much more of an emotional support to her” (P5). For some, providing emotional support was more difficult if their parent was “stubborn,” “tough” and “stoic.” Some participants also expressed feeling more “protective” of their parent.
Participants also described a broader shift in their familial roles to take over other caregiving responsibilities from their ill parent, including caring for siblings, another parent, and grandparents. Some described assuming their ill parent’s role as the “main” figure of the family. One participant reflected on her role as a “second guardian” and needing to “raise” her younger sibling with cerebral palsy, in addition to caring for her mother. Another participant shared her challenges with navigating the additional responsibility of needing to assume a “parental figure” for her younger sibling who had previously relied on their mother in many ways.
Evaluating Personal Values and Priorities
Participants described how caring for a parent with a life-limiting illness “put things in perspective” and led them to “not want to take life for granted” and “existential thinking”: “It made me grow up and re-evaluate. I don’t have time to waste on things” (P7). This process of reflection and re-evaluation was perceived to shift their own priorities and values: “My dad's diagnosis just made me- it almost was like, I was just underwater, and it feels like someone just pulled my head out of a pool. And it was like, this is the reality of the world. I had to grow up, but I just feel like, again, priorities shifted so much, and it was sort of like, a lot of these things- oh, what bar am I gonna go to on a Saturday night? Like that does not matter.” (P3)
Some participants expressed feeling more “confident” and having more “motivation” to find meaning in life and pursue their own goals. Caregiving “opened the door to explore my identity and path” and “pushed me to be more successful than I thought I could be.” Importantly, participants shared how caregiving helped deepen their existential and emotional experience, “cement beliefs,” and strengthen their existing values. Some expressed feeling more connected to and found comfort in their religious beliefs, spiritual health, or “cultural upbringing”: “I think that my mom being sick has really made me do a very deep dive into my [Culture], which has been actually quite transformative. And it resonates with me in such a deep way now that I don't think I had an experience previously […] this just really forced me to jump into it and reconnect with my family and learn my language […] building that cultural connection has been a huge, huge part of my life over the past couple of years. And something that's made me feel more connected to her, and much more, much more proud of where I come from.” (P6, currently alternating between living alone and in parents’ home)
However, others expressed their “disrupted” sense of faith and a sense of unfairness (e.g., “My mom is such a good person [crying] and it’s not fair that she doesn’t get to live as long as other people who aren’t as nice or generous or strong as she is” (P4)).
Prioritizing Meaningful Relationships
One notable area of reflection from participants was their strengthened relational values, such as valuing family, “time spent” with loved ones, and “quality” relationships: “It’s developed this sense of, every moment’s precious. You really are grateful for and value the time that you have together” (P1). The intensity of the illness and caregiving experience prompted a re-evaluation of their relationships and social networks. They felt their accelerated maturation led them to “strengthen” or “deepen” relationships with those perceived to be most valued: “The [illness] gave me a lot more sympathy for my mom, and not just in terms of her being sick, but it made me kind of see the world through her eyes a lot more, which has been really interesting [starting to cry] […] It's made me, I don't know, weirdly just realize how much of who she is [crying], that has really shaped me, as a person. I think that before I never really gave it a ton of thought. And now that she's sick, I realize how much of her qualities or things that I take, and that's been kind of a nice thing to realize. And it's nice to know that, despite the fact that she is going to pass away in coming years, I've realized how much she kind of lives on through me. And I really appreciate the fact that I've had her as an influence in my life and how she takes on challenges. That's been really, really meaningful.” (P6)
Participants appreciated being able to have more “open” and “meaningful” conversations with their close others. They acknowledged the need to “rely on others” and appreciated having a “community of support.” At the same time, other relationships weakened due to their decreased capacity to maintain them or needing to “distance” from them. Caregiving helped to clarify their social network and “weed out” people they were unable to rely on. The experience of focusing and re-configuring their social support network was captured concisely by one participant: “As time has gone on, it has strengthened my relationships in that those people who ask how she is when I see them are the people I remain close to. But folks who can't engage with it aren't necessarily a part of my life.” (P1)
“I Can’t Relate”
Participants described being unable to relate to their friends and same-aged peers in the same way as before, reflecting a significant relational and developmental change. They felt they needed to “grow up all of a sudden” and “become an adult earlier.” Many felt disconnected from their peers who have not had to “deal with” or “think about” such “mature” “life experiences.” As one participant shared: “I can't relate. As I'm getting older, it's differing a little bit, but when my mom was first diagnosed, I was I think 23, and I couldn't relate to my friends at all. I remember almost two months after she was diagnosed, being forced to go to my friend's birthday party […] and just like not feeling it and everyone around me like just seeming happy and carefree and not asking me the question that I wanted to be asked. And it just felt strange.” (P1)
Similarly, participants discussed being unable to relate to their peers’ interests and priorities. One participant reflected on how her “outlook on everything is very different to that of my contemporaries” and shared her difficulty with connecting with peers on “trivial things”: “I know we’re technically 21, but they’re more like teenagers or twenties. And I feel like what I do is like, I’m 30, like I am aged – the things I think about, the things that I consider, how I act just in general […] their interests and the things that they do, and the things that they talk about generally are not what I talk about. Yes, I will have a good gossip about what’s going on in our friend group. I’m not [laughs], I’m not like 70, but they’re more bothered about their Instagram likes and making TikToks […] I’d say overall I’m accelerated by like five or so years.” (P7, currently living with roommates, completing undergraduate studies)
Managing Mixed Emotions and Worries about the Future
The “mixed” emotions experienced by participants was acknowledged as one of the most “challenging” aspects of caregiving. They described a range of feelings from “stages of grief,” “anger,” and “anxiety,” to being “depressed,” “hopeless,” “overwhelmed” “emotionally exhausted,” “detached,” “in denial,” and “numb.” One participant shared this “constant fluction of emotions”: “…between guilt and anger and sadness and grief, and times of wanting to move on with my life, but being so scared to do that because what if I miss her last X months. Or getting upset that she's in so much pain. And sometimes with her, because that will be 60% of our conversations, then me being like, I'm such an asshole. Like, why do I feel that way? Or I just got out of a 7 year relationship and I thought my mom could be around to see me get married and then like [starting to cry] what if that doesn't happen? And then there are times where I'm like, well, her disease has come so far. We've had her for 3 more years than we were told we were gonna have her. And then I'm like, so why not 11 years? So it's just all over the map, basically is what I'm trying to tell you [laughing while crying]. All over the map. Name an emotion, I've had it.” (P1, currently single, living alone)
Participants described how “constant thinking” about the future was particularly “hard.” One participant elaborated on her worries about being able to support her father as his Alzheimer’s disease progresses: “I would say it’s more worrying about the future, about what it will become. So it’s kind of like feeling kind of anxious all the time. Always thinking, always thinking” (P10).
Participants detailed challenges with navigating uncertainty and “not knowing,” anticipatory grief of losing their parent, and thoughts of the future without them. One participant shared how she was grieving the possibility of her mother being there for her future wedding, with her future children, and continued connection to their culture: “That really hurts to think about, like getting married […] and also having children cause I want kids […] I guess in some ways I feel robbed of that experience, and being able to give that to my future children” (P6, currently single, living alone).
“Not Where I Should be”
Although participants resonated with many aspects of feeling “more adult” and “aged,” this was often countered and contextualized with a sense of being “not where I should be.” This captured the experience of being unable to pursue tasks that were perceived to be typical of emerging adulthood. The interrelated elements of this experience were: (1) renegotiation of expectations for emerging adulthood and (2) “falling behind.”
Renegotiation of Expectations for Emerging Adulthood
Participants shared how their personal goals and expectations for this life stage were re-negotiated in some ways, given the circumstances of caregiving and their parent’s illness. They described needing to “balance” between caregiving and exploring their own goals when making decisions about their academics, careers, relationships, dating, and living situations. Caregiving was perceived to impact this overall “period of exploration”: “I'm in my mid-twenties, and what I have been told have been, a period of exploration, a period of growth, a period of innovation rather too. And I feel like there are times where I feel like I have to consider how am I gonna take care of my parents, but also do what I can do into advancing my own career and all that […] I think also stability-wise, wanting to find one that can lead into growth, but also has a decent salary, but also knowing that, in this economy and everything, I don't think it makes sense for me to take one that's just for self-fulfillment, and I struggle with that.” (P2, currently living with parents, in a relationship, working full-time)
Another participant shared how her “overwhelming” caregiving responsibilities impacted her academic performance, decision to take a few years off from school, and her capacity to consider her personal goals: “I never really got the time to actually sit down and think about any terms of even relationship or goals or anything […] It is sometimes very overwhelming and draining that I haven’t explored anything that I wanna do” (P11).
Some participants felt “hesitant to pursue the next steps,” “guilty,” or unable to prioritize their own goals and dreams. As one participant shared: “My [other parent] has, since the beginning, found the situation pretty overwhelming, and so I feel very guilty if I were to go anywhere now and sort of leave him to deal with everything. I think I put a lot of pressure on myself to stay […] [My partner] has been really understanding with it, and has said, if I'm not ready to move out, then obviously there's no pressure and he understands. But I don't know, maybe I'm just anxious about the situation or overthink it, but sometimes I feel like maybe he might be a little bit disappointed, not in my choice, but I guess in the overall situation, that it sort of put us back from moving in together.” (P5, currently living with parents, in a relationship, working full-time)
“Falling Behind”
Participants also felt that they did not have the same opportunities for exploration, freedom, and self-focus as their peers, further threatening a sense of “falling behind.” This included feeling “self-conscious,” requiring more resources or capacity to pursue their goals, and wishing for more “real-life experiences”: “She's never stopped me or anything. It's just my own guilt sometimes. I mean, she is like Asian mom, so sometimes she does kind of guilt trip you, right? But I think I would've done more, and been more free and hung out with more of my friends and just experienced more, like travelled more, gone to more concerts and parties, if my mom was healthier.” (P8, currently living with parents, in a relationship, working full-time)
For some, there was also “frustration” or regression in their relationships with their parent, which was challenging to navigate as they moved towards adulthood. One participant described the added complexity of not wishing to separate and the potential for loss: “You would think that I would feel like more adult because I'm taking on more of like a caregiver role or household management role. But in some ways, I feel more like a child [laughs], just because I've been back living at home and returned to those old dynamics that you experienced when you were a child […] emotionally I felt kind of resistant towards adulthood, I guess? Just because I think that symbolically, it's sort of relates to that separation from your parents and stuff like that. And so I don't really wanna be like separated from my mom [crying].” (P4, currently living with parents and sibling, in a relationship, completing graduate studies)
Caregiving Role is Assumed
Following their parent’s diagnosis, participants assumed their caregiving role and responsibilities. They detailed a range of care tasks, including providing practical support (e.g., booking and facilitating medical appointments, translating at appointments, transportation, mobility support), household management (e.g., preparing meals, cleaning, laundry, managing finances), personal care (e.g., assisting with bathing, dressing, toileting), and emotional support.
Participants described this transition into caregiving as “automatic” and coming “very naturally.” Some participants ascribed the natural progression of them taking on this role to their “personality” or emotional capacity. Others shared practical reasons, including having a flexible schedule, siblings that lived further away, or another parent take on more work. Some reflected on their unique relationship with their ill parent that influenced them to take on a caregiving role: “Because I’m more like him, he always tells me, when you’re older, you gotta make sure to take care of your mom and your brother” (P2).
Many expressed difficulty identifying with the term “caregiver,” although they resonated with the experience of caregiving. For some, the difficulty was related to how they perceived their role as a “duty” or “mandatory” and described this “responsibility” within their cultural or religious context: “In our culture, the girl does all the household work. It’s not really expected of a man at all. It is sometimes very overwhelming and draining” (P11). One participant described her motivation to “step up” and take care of her family: “In Islam, it's not a woman's responsibility or the mother's responsibility to earn money. So when we did have this sort of conversation with our mom before, she's kinda like, it's not my responsibility, I'm not gonna do it […] I feel like me and my brother can step up.” (P9, currently living at home with parents and sibling, completing undergraduate studies, working part-time)
Participants described their caregiving responsibilities and constant “stress” about their parent as “always at the back of my mind”: “Once [the diagnosis] happens, that’s just a role to me I feel like I’ve taken on. And it never goes away […] I think it’s like you’re almost preparing yourself for when the inevitable decline happens” (P3). They shared how they navigated their lives and made decisions within the context of caregiving, as this role was perceived to transcend all aspects of their lives.
Availability of Support
The contextual factor of availability of support significantly influenced participants’ process of negotiating accelerated adulthood and their ability to balance caregiving and their own development. Types of support included having supportive relationships, others to coordinate care with, therapeutic support, institutional accommodations, and personal interests and hobbies.
Some participants reported having limited support and wished for more flexibility from institutions and “proactive” support from family and friends, although they also did not want to “overburden” close others. Some described assuming a larger caregiving role when their ill parent, other parent, or siblings were too busy, “in denial,” or “overwhelmed.” For those with less support, it seemed to exacerbate both feelings of being “more of an adult” and “not where I should be.” For one participant, the lack of support was perceived to increase her sense of adulthood while also widening the developmental gap with her peers: “I would say both yes and no. Yes, in terms of, cause I know my other friends, they didn't know how to cook or clean or taking care of anybody whatsoever. So in terms of that, like taking care of somebody and paying for the bills and managing a household, I am like an adult. But I say no because I don't have any real life experience outside of my family or my house. Whereas they do. They know different places, they've gone exploring, they've visited other countries. They've picked up hobbies. Some of them are already married. So yeah, I say like both. For me it's a yes and no. I feel like I am an adult cause I feel like I already raised people, so I'm so tired.” (P11)
Another participant, who is an only child, referred to her limited family support as her extended family lived in India. This was further complicated by cultural stigma and her mother’s reluctance to seek support from friends: “She thinks it’s frowned upon. She’s afraid that they’ll think, ‘Oh, you have a daughter, why isn’t she taking care of you kind of thing’” (P8). The minimal support available was perceived to impact her need to assume many adult responsibilities and feeling like she “missed out so much” in her “youth.”
Other participants reported feeling “supported” and expressed feeling “grateful” for their “support systems.” Those with greater supports in place seemed to feel less burdened with care responsibilities, allowing them to maintain a more manageable balance between caregiving and pursuit of their own goals: “We were really lucky in that we had support systems everywhere […] I was really lucky in that it never really felt like I was overburdened. There was always somebody else who could pick up the slack a little bit” (P3). The negotiation of reaching “accelerated” adulthood seemed to be less constrained, where they felt more “sheltered” or “protected” from needing to be an adult and maintained more flexibility to pursue their goals: “I think it got to a point where my parents decided to stop telling me things. Not because they want to keep things from me, but I think when I’m away [at school], knowing too much, can be a lot […] I think they just want me to be a person who doesn't have to deal with this as much. But if anything was intensely happening, I'd probably find out. But I'm sure there's a lot of other stuff going on in the background, it's just, they don't really talk about it. But I kind of respect that decision cause I know my mom doesn't wanna freak me out […] I get to see her and spend time with her and we get to do things, and I don't know, I don't think about it too much just because they've kind of done that.” (P7, currently living with roommates, completing undergraduate studies)
Discussion
The present study explored the experience of caring for a parent with advanced disease during emerging adulthood through a developmental perspective. This is aligned with increasing calls to understand, recognize, and support emerging adult caregivers given their growing prevalence and distinct set of challenges (Day, 2015; Joseph et al., 2020; Kent, 2020). The core phenomenon emerged as negotiating accelerated adulthood, whereby caregivers experienced the dynamic tethering between two paradoxical states: feeling more of an adult than before while feeling like I’m not where I should be.
Caring for a parent with advanced disease during emerging adulthood may result in an atypical developmental experience marked by alignment with some aspects of emerging adult development but not others. Caregiving at this life stage may be considered less normative, as the death of a parent is much less expected in emerging adulthood compared to in older adulthood (Tekcan et al., 2012). Our findings extend emerging adulthood developmental theory (Arnett et al., 2014) by offering nuanced insight into the conceptions of adulthood and the feeling of being in-between for caregivers. Rather than feeling in-between adolescence and adulthood, the current conceptualization suggests that emerging adult caregivers experience an accelerated sense of adulthood, while being constrained in their capacity to pursue normative developmental tasks (e.g., identity exploration, self-focus, hope for the future). This juxtaposition is similar to other work exploring the experiences of emerging adults who have been exposed to unique experiences during this critical stage of development, such as those seeking substance use treatment (Goodman et al., 2016).
The feeling of being more of an adult than before was dominant in participants’ discourse, including increased responsibility and role reversal, evaluating personal values and priorities, being unable to relate, and managing mixed emotions and worries about the future. These elements reflect accelerated identity development, a critical task of emerging adulthood, which may be the underlying essence in the feeling more of an adult than before. This may be understood within the complex reciprocal relationship between identity development and trauma. Traumatic events may impact identity by causing individuals to re-evaluate their roles, goals, and values, and one’s identity may also impact how traumatic events are interpreted, and experienced (Berman et al., 2020). Emerging adults in this study were presented with new opportunities for identity exploration, sensemaking, and re-evaluation in their caregiving reality, which challenged previous ways of understanding themselves and the world.
Consistent with previous findings, we identified an increased responsibility and role reversal throughout their caregiving experience (Boumans & Dorant, 2018; Chevrier et al., 2022; Day, 2015). Parents often continue to play an influential role in emerging adulthood, and the establishment of an equal parent-child relationship is an important criterion for achieving adulthood (Arnett, 2001; Nelson et al., 2007). However, the premature role reversal reported by the current participants suggests that they experienced a quicker shift into an egalitarian parent-child relationship, further supporting our model of accelerated adulthood. They also highlighted their older subjective age (i.e., “I can’t relate” with their age peers). This captures both the loneliness of the experience and the catapult forward into more mature life experiences. It may also be helpful to consider increased responsibility and perceived burden in light of the caregiving stress appraisal model proposed by Yates and colleagues (1999), which draws upon the caregiving stress model (Pearlin et al., 1990) and the appraisal model (Lawton et al., 1989, 1991). The model considers “overload” a secondary appraisal, with the assumption that caregivers can identify their level of overload by assessing their experience and ability to provide care. The Yates’ model may be expanded to consider variation in this appraisal for younger caregivers compared to those in middle or late adulthood (D’Amen et al., 2021), as they may differ in their level of stress appraisal, metacognition capability, and sense of mastery.
Prioritizing meaningful relationships was also perceived to foster a sense of accelerated adulthood. In another study, emerging adult caregivers similarly identified the strengthening of family relationships as a rewarding aspect of caregiving (Pope et al., 2018). This is consistent with the idea that, as individuals age, they reconfigure their social networks to prioritize their most rewarding and satisfying relationships and reduce contact with less close others (Luong et al., 2011). This “selective pruning process” has been conceptualized under socioemotional selectivity theory, positing that one’s time perspective (i.e., perceived time remaining in life) influences their emotional goals and social preferences as they age (Carstensen et al., 1999, 2003). It is possible that emerging adult caregivers reconfigure their social networks in relation to their accelerated sense of aging, as well as in response to their heightened salience of mortality with their parent’s illness (Vail et al., 2012). Death awareness may motivate participants towards re-evaluating their values, while also triggering worries about the future and anticipatory grief (Coelho & Barbosa, 2017; Vail et al., 2012).
The paradoxical experience of I’m not where I should be included the renegotiation of expectations for emerging adulthood and “falling behind” given the constraints imposed by caregiving. These reflect a sense of increased familial obligation and decreased autonomy, during a stage typically marked by exploration, self-focus, optimism, and separation from family of origin in Western cultures (Arnett et al., 2014). It may be unsurprising that this sensed contradiction was accompanied by feelings of guilt and hesitancy to prioritize their own needs. Indeed, the impact of guilt on caregiver distress and burden has been documented elsewhere (Losada et al., 2010; Stamatopoulos, 2018). Similar findings have shown that disruptions to normative developmental tasks (e.g., during COVID-19) or non-autonomously motivated decisions during emerging adulthood impact psychosocial functioning (Hall & Zygmunt, 2021; Jaramillo & Felix, 2023; Kins et al., 2009). Awareness of these conflicting aspects of experience may be useful when planning psychotherapeutic support and interventions for emerging adult caregivers.
Participants perceived their caregiving role as a natural responsibility or obligation which was related to some difficulty with identifying as a caregiver. This is aligned with findings of caregiving as a perceived familial obligation or part of a “normal” familial relationship (Smyth et al., 2011, p. 145), being “chosen” (Goldblatt et al., 2019, p. 535), and non-identification or resistance to the label (Lewis, 2017; Struckmeyer, 2015). This finding may also suggest the fixed integration of caregiving into their emerging identity (Bolas et al., 2007; Goldblatt et al., 2019).
The availability of support was an important contextual factor. Those with less support experienced intensified extremes and greater constraints, while those with greater support had more flexibility in their negotiation of accelerated adulthood. This finding may be contextualized within the caregiving stress appraisal model (Yates et al., 1999). Higher levels of emotional support were shown to be indirectly associated with decreased overload (i.e., appraisal of their caregiving situation) through mastery, as well as directly associated with lower risk of depression (Yates et al., 1999). The impact of emotional support on caregiver wellbeing is also relevant for young caregivers (D’Amen et al., 2021). Emerging adults with limited support may require careful consideration when developing tailored interventions and policies. Interventions may consider focusing on addressing emotional support needs or developing skills to elicit desired emotional support from close others to improve caregiver wellbeing.
Furthermore, our results shed light on the complex intersection of gender, culture, and personality with how the caregiving role is assumed, appraised, and experienced by emerging adults. For example, some participants perceived caregiving as a cultural or gendered obligation, highlighting the ethno-cultural context of one’s duty to care. Caregiving has historically been considered a part of “women’s work” in societies throughout the world (Esplen, 2009), and gendered caregiving norms may be socialized and internalized (Revenson et al., 2016). Substantial literature suggests that caregiving is gendered, and women are more likely to provide care, be burdened with caregiving responsibilities, and experience negative impacts on their wellbeing (e.g., Fast et al., 2023; Hequembourg & Brallier, 2005; Revenson et al., 2016; Wray, 2024). There is also support for a pattern of gendered intergenerational care, where women are most likely to provide “sandwich caregiving” (i.e., providing unpaid care to both children and care-dependent adults) (Wray, 2024) and daughters are more likely to provide care for elderly parents than sons (Grigoryeva, 2017; Vergauwen & Mortelmans, 2021). This seems to be especially relevant in cultural contexts characterized by stronger family and gender norms (Vergauwen & Mortelmans, 2021). However, some researchers have found a more equal gender distribution of emerging adult caregivers (Flinn, 2018) and no gender differences in willingness to provide care (Canell & Caskie, 2022), raising questions about the impact of gender on the assumption and experience of parental caregiving responsibilities in emerging adults. In addition to assumption of caregiving roles, the interplay of identity characteristics also impacted participants’ perceived burden, availability of support, role expectations, and belief in or abandonment of religion or culture. Previous research suggests that feeling burdened by caregiving depends on subjective meanings of caregiving and identities embodied within gender roles and cultures (Liu et al., 2022; Martin, 2000). This is consistent with a meta-ethnographic model of cultural caregiving motivations, which emphasizes how cultural self-identity shapes one’s motivation and willingness to provide care (Zarzycki et al., 2022). Others reflected on the impact of their personality, unique relationship with their parent, and practical concerns on assuming their caregiving role. Similarly, prior research has shown the impact of factors including proximity to parent, personal values, gender, and parental expectations on the differential assumption of caregiving responsibilities among siblings (Pillemer & Suitor, 2014). Taken together, our insights suggest that identity and psychological factors may intersect and influence the experience of caregiving and of negotiating accelerated adulthood in emerging adulthood.
Limitations and Future Directions
Several limitations of the study should be considered. Firstly, there is potential for self-selection bias, whereby our findings may not capture the experiences of those who are most distressed or uncomfortable sharing their experience. This may be linked to our inability to recruit men or non-binary emerging adults. Future research using an intersectional lens is needed to explore the intersections of different identities, including gender, and its impact on caregiver experience and outcomes. Moreover, it is important to acknowledge the co-construction of meaning between the researcher and participants within the sociocultural contexts of the sample. Although this is a strength of using a social constructivist lens, this also limits the transferability of findings to those with different experiences, including gender, type of diagnosis, family structures, and living situations. A constructivist view of grounded theory and the involvement of one main coder may inherently include potential for researcher bias and subjective interpretations. Although reliability between coders is an important criterion within a positivist epistemological framework, perhaps focusing on its underlying goal of fostering reflexivity may be more appropriate in the current study where we have adopted a constructivist epistemological approach. Strong reflexivity is critical to achieving credibility, one of the main quality criteria for constructivist grounded theory studies as proposed by Charmaz (2014). Ongoing efforts to promote reflexivity and rigour included verifying interpretation with participants, staying as close as possible to participants’ words and discourse, memo writing, reflexive journaling, and regular meetings with senior team members.
Conclusion
Emerging adult caregivers represent a hidden yet growing demographic group amidst a growing worldwide population of aging adults living longer with incurable and terminal illnesses. Our findings highlight the perceived uniqueness of the experience and developmental trajectory of emerging adult caregivers. This furthers our understanding of emerging adulthood developmental theory by shedding light on the heterogeneity of emerging adulthood experience. Our findings also highlighted the interplay of different factors with how the caregiving role is assumed, appraised, and experienced by emerging adult daughters. Greater awareness of the unique developmental trajectory and the impact of intersecting identities, psychological features, and contextual factors may help to inform the development of tailored interventions and strategies to support emerging adults caring for parents with advanced disease.
Footnotes
Acknowledgements
We sincerely thank all participants in this study who generously shared their time and personal experiences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Canada Research Chair in the Psychology of Emerging Adulthood (CRC- 2020-00005) and Vanier Canada Graduate Scholarship (186866).
Transparency and Openness Statement
The data used in this manuscript are not publicly available due to the protection of participants’ identities but are available from the corresponding author on reasonable request and following application to and approval from the University of Toronto Research Ethics Board. No aspects of the study were pre-registered.