
Abstract
Suicide is a leading cause of death for undergraduate students, with there being a crucial need to understand sources of suicide prevention for this population. While the benefits of compassion toward others appear to align with the psychological targets of recovery from suicidal ideation, little is known about the potential role of compassion for others in undergraduate students’ recovery process. The purpose of this qualitative study was to explore the experience and impact of compassion toward others, as it relates to undergraduate students’ recovery from suicidal thinking. We interviewed six undergraduate students about their experiences of compassion toward others and its impact on recovery. Using data analyses methods from interpretative phenomenological analysis, six superordinate themes emerged, including: sense of meaning and purpose, reciprocity, positive self-concept, non-judgement and acceptance, social connection, and the cost of compassion. Implications for counseling, limitations, and future directions for research are discussed.
Each year, over 700,000 people worldwide die by suicide, with suicide being among the leading causes of death for persons aged 15–29 years (World Health Organization, 2021). Emerging adulthood, the developmental period that spans roughly from the ages of 18–29 (Arnett, 2018), is thus a time of significant suicide risk. Among emerging adults, undergraduate students may be especially vulnerable to suicide. In a recent meta-analysis that examined college student samples across North America, Asia, and Europe, approximately one quarter of students reported suicidal ideation, of which more than two thirds had occurred within the preceding year (Mortier et al., 2018). These rates represented higher levels of suicidal ideation than has been reported in the general adult population (Mortier et al., 2018).
Suicide in Undergraduate Students
As Klonsky and May (2015) theorized in their three-step framework for explaining suicide, suicidal ideation can be understood as stemming from an individual’s perceived pain and hopelessness, compounded by a sense of disconnectedness from people and from other sources of meaning and purpose. With regard to interpersonal processes associated with suicide, Joiner (2007) theorized that a low sense of belonging, combined with feelings of burdensomeness, may contribute to a person’s desire to end their life. For O’Connor et al. (2016), key triggers of suicidal thinking include feelings of defeat and humiliation, followed by a sense of entrapment. At any point along the path to suicide, a number of risk and protective factors may increase the likelihood of a suicide attempt (Klonsky & May, 2015). Furthermore, suicidal ideation and behaviors occur in the context of the external environment and stressful life events (O’Connor et al., 2016).
Several factors may heighten the risk of suicide in undergraduate students. Some potential triggers relate to the natural developmental tasks of emerging adulthood more generally. Arnett (2018) described emerging adulthood as “the age of possibilities” (p. 21), where individuals explore options in education, work/career, and romantic relationships. During this period, most individuals are intensely immersed in the process of forging a cohesive identity and clarifying their worldview. Although emerging adulthood is commonly a time of great optimism and sense of purpose, it is also one of considerable instability and change (Arnett, 2018). In the midst of such instability, mental health may take a toll. Indeed, emerging adults are at an age where many mental health issues, such as depression and anxiety, first appear (Kessler et al., 2007; Macalli et al., 2021).
Emerging adults who make their way to university face a unique set of compounding challenges that, for many students, may negatively affect mental health and increase the risk of suicide (Assari et al., 2018; Horwitz et al., 2020; Liu et al., 2019). University offers rich opportunities to develop social relationships, become more independent, and explore new ideas. However, academic pressures and the financial burden of funding a university education can be major sources of stress for students (De Luca et al., 2016; Eells, 2017; Seeman et al., 2017). High-achieving students may hold themselves up to unrealistic standards, based on personal or familial expectations; and the strain of meeting such expectations may increase suicidal ideation (Eells, 2017). Low grades may also be a risk factor in suicide (De Luca et al., 2016; Seeman et al., 2017). Perceived failure to achieve personal goals or live up to expectations may diminish self-esteem (Zafar et al., 2012) and result in feelings of hopelessness (Chang, 2017). Both hopelessness and perceived failure have been associated with suicidal thoughts and behaviors among college students (Dhingra et al., 2019; Gulec Ovekcin et al., 2017; Macalli et al., 2021).
Another predictor of suicide in this population is social isolation (De Luca et al., 2016; Goncalves et al., 2014). For undergraduates, attendance at university often means living away from family and friends for the first time, as well as developing new friendships in a large university environment (Boddy, 2020). Students may struggle with loneliness and lack of connectedness and belonging, factors believed to play a central role in triggering thoughts of suicide (Joiner et al., 2009; Klonsky & May, 2015). Of further concern is the high rate of substance use in undergraduate populations. In the United States, rates of binge drinking and alcohol-related mental health problems are higher among college students than among emerging adults not attending college (Skidmore et al., 2016). Whether motivated by a desire for social connection or used as a means of coping with stress, substance use may increase suicidal behaviors in undergraduates and impair academic performance (Assari, 2018; Giordano & Cashwell, 2014).
In light of these and other factors that contribute to suicide risk in undergraduate students, it is crucial to understand sources of suicide prevention and recovery. Much has been researched on clinical treatments for suicidal ideation and behaviors, with mixed results (Harrod et al., 2014; Mortier et al., 2018). What has received less attention, however, are positive coping strategies and processes that arise more spontaneously in the course of people’s everyday lives (Stanley et al., 2021). In addition, a better understanding is needed on the subjective perspectives and lived experiences of individuals who have recovered from suicidal ideation and behaviors (Kabir et al., 2023; Wayland et al., 2020; White, 2015). Qualitative research, including phenomenological studies on people’s lived experiences, provide a window into people’s thoughts, feelings, and intentions in ways that do not rely on pre-existing categorizations, biases, and assumptions about phenomena (Smith et al., 2009; Wayland et al., 2020). Instead, as Hornstein et al. (2013) have stated, themes that arise from phenomenological research “emerge directly from the data of experience…[rather than being] imposed on the data, regardless of how well or how poorly it fits” (p. 31). Thus, qualitative research on participants’ perspectives on recovery from their experience of being suicidal adds an essential dimension to suicide research and may improve prevention efforts.
Role of Compassion in Suicide Prevention
One potential strategy for suicide prevention that merits greater attention is compassion. Compassion can be conceptualized as a connected triad (Gilbert, 2009b), with compassion being from others, toward others, and/or toward oneself (i.e., self-compassion). Although compassion is shaped to some extent by culture (e.g., individualistic vs. more collectivist cultures; Koopmann-Holm & Tsai, 2017), a number of core elements can be found across cultures. Strauss and colleagues (2016) described compassion as “awareness of someone’s suffering, being moved by it…, and acting or feeling motivated to help” (pp. 17-18). Similarly, Gilbert (2014) conceptualized compassion as motivation consisting of two main processes, namely engagement and action. Engagement includes noticing and feeling for a person who is suffering; tolerating those feelings without avoiding them; and being understanding and non-judgmental toward the person suffering. Action refers to the desire to alleviate the suffering and taking action to do so. In contemporary research, compassion is typically differentiated from empathy in that the latter refers more narrowly to the ability to mentalize or take another person’s perspective, whereas compassion includes the additional elements of emotional resonance, distress tolerance, non-judgment, and action-based processes (Gilbert, 2014). Furthermore, from a psychoevolutionary approach, Gilbert (2009b, 2014) explained the crucial role of compassion in activating brain centers associated with contentment, affiliation, and decreased feelings of threat.
Although some studies have pointed to the potential benefits of compassion for suicide prevention, most existing research has focused on the relationship between suicide and self-compassion (Chesin & Jeglic, 2022; Hasking et al., 2019; Kelliher-Rabon et al., 2018). For example, a study by Kelliher-Rabon and colleagues (2018) found that university students who had high levels of anxiety and depression and who practiced self-compassion were less likely to engage in suicidal behaviors. Similarly, Hasking et al. (2019) found that self-compassion mediated the relationship between negative affect and suicidal ideation in an undergraduate student sample. Compassion received from others has also been found to reduce the risk of suicide, as evident in a recent qualitative study on factors that facilitated self-disclosure and help seeking in adult survivors of attempted suicide (Frey et al., 2018). For some participants, willingness to disclose suicidal intent to a friend or family member depended in part upon participants’ trust in the confidant to respond with compassion (Frey et al., 2018).
These and other studies on the role of self-compassion and compassion from others in reducing suicidal ideation and behaviors have made important contributions to understanding the role of compassion in preventing suicide. Some individuals, however, may fear self-compassion and have difficulty extending compassion toward themselves in times of distress (Gilbert et al., 2014; Kirby et al., 2019). Additionally, many people struggle with accepting compassion from others, perhaps due to feelings of shame and unworthiness, or from fear of being perceived as weak (Gilbert et al., 2014; Kirby et al., 2019). Although fear may also occur when extending compassion toward others, such fears are often less severe compared to fears of self-compassion and accepting compassion from other people (Kirby et al., 2019). Furthermore, although a person can be highly compassionate toward others while being low in compassion toward themselves (Kirby et al., 2019; López et al., 2018), the practice of extending compassion outward may help a person become more self-reassuring in the face of their own emotional pain (Hermanto et al., 2016). Stated differently, for some individuals, compassion toward others may serve as a gateway to self-compassion (Kirby et al., 2019).
In the existing literature, there is growing evidence on the benefits of compassion toward others on mental health and well-being. Of particular relevance in the current context are studies pointing to the positive impact of compassion toward others on strengthening a sense of social connection (Cosley et al., 2010; Crocker & Canevello, 2012; Hutcherson et al., 2008), increasing a sense of meaning and purpose (Chan et al., 2022; Crocker & Canevello, 2012; Mongrain et al., 2011), and fostering hope (Hsaio et al., 2020). Given the role of hope, social connection, and emotional pain in suicidal ideation (Joiner, 2007; Klonsky & May, 2015), it seems plausible that practicing compassion toward others may be helpful in decreasing suicidal ideation and preventing suicide in undergraduate students. The study of compassion toward others, as a strategy that emerges in everyday lived experience and that has the potential to ward off suicide, may contribute to suicide prevention. To date, however, there has been a lack of research on this important topic.
Present Study
The purpose of this phenomenological qualitative study was to gain an in-depth, contextualized understanding of compassion toward others as an aspect of undergraduate students’ recovery from suicidal ideation. In approaching this topic, we were particularly interested in understanding this phenomenon based on participants’ own lived experiences, beliefs, and truths, rather than defining personal experience based upon previously established categorizations and a priori theory. As indicated above, providing participants with the opportunity to describe their personal experiences and share how they make sense of them provides crucial insights into prevention and may also help in the development of strategies, tools, and clinical interventions that take subjective perspectives into account. Furthermore, in the exploration of novel topics, phenomenological research can open up important new directions for inquiry (Smith et al., 2009).
Our main research question was: What are the lived experience and role of compassion toward others in the process of recovering from suicidal ideation? More specifically, we explored students’ lived experience and the perceived impact of compassion toward others on the recovery process, as well as the perceived role of compassion toward others on the longer-term prevention of suicide. Our emphasis throughout was on participants’ perspectives and meaning making. In conducting this study, our goal was to contribute to knowledge and understanding of compassion and suicidal ideation in young adults and to bridge the literature in these two areas.
Method
To accomplish our research aims, we utilized interpretative phenomenological analysis (IPA), which is an approach used to study meaning and lived experience in the context of psychological and social phenomena (Smith et al., 2009). IPA is built upon the theoretical assumptions of phenomenology, hermeneutics, and idiography. Phenomenology is the study of lived experience and how people make sense of their experience. With IPA, the researcher attempts to go beyond predefined theory and societal assumptions; rather, the focus is on the meaning of experience, as perceived by the participant (Jones, 2001; Smith et al., 2009). Hermeneutics is the study of interpretation. Two concepts, the hermeneutic circle and the double hermeneutic, are particularly important in IPA. The hermeneutic circle is an interpretative technique whereby the researcher repeatedly shifts between parts and whole of a text. Small units of meaning, such as a word or clause, are interpreted in the context of the larger unit (e.g., sentence, paragraph, etc.) in which they are located; and, conversely, large meaning units make sense because of the small units of which the larger unit is comprised (Gyollai, 2020). In IPA, the double hermeneutic is described as a process of dual interpretation, whereby a participant interprets their experience of the world, while at the same time the researcher interprets the participant’s attitudes and perception of the world (Smith et al., 2009). Finally, idiography refers to IPA’s attention to particularities and subjectivities within an individual case. With IPA, small sample sizes are typically preferred over larger ones, in order to capture the meaning of the phenomenon in rich detail. Although analysis eventually moves from a specific case to patterns across all cases, the nuances of each individual case are still vital and considered in the findings (Smith et al., 2009). Furthermore, IPA is built upon social constructionist assumptions about the nature of being (ontology) and reality (epistemology). An IPA social constructionist stance assumes that when studying human meaning and experience, there is no single objective reality or way of knowing; rather, truth and reality are subjective and open to interpretation (Smith et al., 2009). Thus, the goal of IPA is not to uncover a universal truth that generalizes to a population. Instead, the researcher interprets the subjective perspectives of participants.
Participants
Prior to participant recruitment, this study was reviewed and approved by the Research Ethics Board (REB) at the University of Alberta in Edmonton, Canada. All participants were recruited through announcements in the University’s Undergraduate Student listserv and the University’s Undergraduate Research Initiative Facebook page. Students who were interested in participating in the study were invited to email the first author, who sent the study information and consent form. Inclusion criteria included: (a) age 18 to 29; (b) fluency in English; (c) past experience of suicidal thoughts and/or behaviors, as well as being free of symptoms for at least one year; (d) belief that compassion toward others aided in the recovery, based on the participant’s own interpretations of what compassion meant to them; and (e) willingness and ability to articulate personal experiences.
Common Themes.
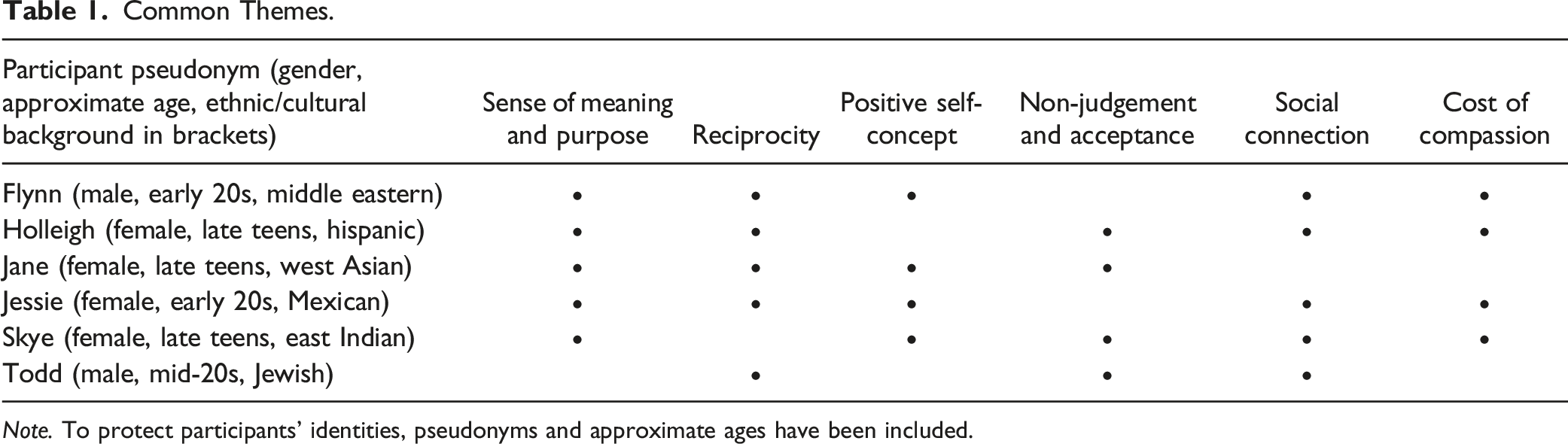
Note. To protect participants’ identities, pseudonyms and approximate ages have been included.
Data Collection
Individual semi-structured interviews, lasting approximately 45 minutes, were conducted with each participant. Due to the COVID-19 pandemic, all interviews occurred remotely: five interviews were conducted through a secure video conferencing platform while the remaining interview occurred over the telephone. To protect confidentiality and minimize disturbances, participants were asked to choose a quiet, private location for the interviews; similarly, the researcher who conducted the interviews (first author) did so in a quiet and private location. In keeping with Smith et al.’s (2009) guidelines for constructing IPA interview protocols, the interview questions were designed to elicit detailed descriptions and examples of the phenomenon of interest, from the participant’s lived experience. Additionally, the protocol attended to context, sequencing, and avoidance of leading questions. Questions were refined through several discussions between the first author and her research supervisor. In IPA, further revisions to the interview protocol sometimes occur between participant interviews (Smith et al., 2009). However, no revisions to the protocol were deemed necessary based on the clarity and richness of data produced. In this study, the final interview protocol consisted of five open-ended questions aimed at eliciting detailed descriptions of times when the participant acted compassionately toward others during the participant’s recovery from suicidal symptoms; how compassion toward others influenced the participant’s recovery; and what compassion toward others meant for the participant (see Appendix A). Although the questions provided structure for the interview, the interviews took on a conversational tone, and the researcher followed relevant directions in the conversation as it unfolded. In the unanticipated event that the interview activated distressing feelings for the participant, a list of counseling referrals was made available. No signs of distress were apparent or indicated. All interviews were video-recorded (for the online interviews) or audio-recorded (for the telephone interviews) and transcribed verbatim, with identifying or potentially identifying information removed. The transcripts were then emailed to each participant, who reviewed the transcript for accuracy and completeness. Within two weeks, individual follow-up interviews were conducted (average of 20 minutes duration) in order to clarify the researchers’ understanding of what the participant had said in the first interview. The follow-up interview also provided participants with the opportunity to discuss any further thoughts or questions that had arisen for them. All participants received a $25 gift card as a token of appreciation for their participation in the study.
Data Analysis
Data analysis followed IPA guidelines as suggested by Smith and colleagues (Pietkiewicz & Smith, 2014; Smith et al., 2009; Smith & Shinebourne, 2012) and Larkin et al. (2006). In accordance with the theoretical underpinnings and methods of IPA, we sought patterns both within cases and across cases, while still incorporating the nuances specific to each individual. Data analysis began with a careful reading and re-reading of each initial and follow-up interview transcript, to gain a holistic and contextualized understanding of the participant’s meaning and experience. During this process, the first author wrote memos (i.e., analytic comments) on salient descriptive, linguistic, and conceptional features of the data. The next step was detailed coding of each transcript. Coding involved the first author’s creation of brief labels to capture relevant meaning in data excerpts (i.e., words, phrases, sentences, paragraphs, etc. that related to the research question). At this stage, analysis occurred at a relatively low level of conceptual abstraction. To help organize the codes, the qualitative data analysis software package, Atlas.ti (version 8.4.4; Scientific Software, 2012), was used. After initial coding of the transcript, the codes were reviewed by the second author to check that they fit the data, made sense, and were clear; and codes were revised where appropriate. Low-level coding then proceeded to the development of initial themes, which represented high-level patterns of meaning in the data. A code was grouped into a theme if it was conceptually similar to other codes within the theme, while at the same time differing from codes in other themes. For example, within one case, the codes “CTO [compassion toward others] gave purpose in life,” “CTO as participant’s goal in life,” “CTO through contributing to the community,” and “suicidality recovery [SR] through love of volunteering” were grouped into the theme “Meaning and purpose through helping others”; and “CTO gave participant more positive view of self,” “CTO led to self-compassion,” and “SR through acceptance of self” were grouped under “Enhanced positive regard for self.” Additional peer review helped in the construction of strong, well-founded themes. The same process of memoing, coding, and theme development was repeated for the remaining interview transcripts. Once themes were finalized for each case, we identified common patterns across participants, based on thematic similarities and differences. In IPA there is no universal threshold for determining the number of cases in which a theme must appear in order for it to be deemed a common or superordinate theme. Smith et al. (2009) suggest that this threshold be determined by the researchers, based on the particulars of the research study and the characteristics of the data. For the purposes of the present analysis, we chose a relatively conservative approach of deeming a theme “common” or “superordinate” if it appeared in at least half of the participant cases.
Methodological Integrity
We used several methods to strengthen the methodological integrity and trustworthiness of our study. To reduce the impact of pre-existing biases on data collection and analysis, the first author engaged in a rigorous process of bracketing (Smith et al., 2009). This involved reflecting on and writing about prior assumptions and beliefs that might influence interpretation of the data, and, where it made sense to do so, putting aside our assumptions as much as possible in approaching participants and the interview transcripts. Regular peer reviews with the second author helped ensure that the researchers’ codes and themes fit the data rather than reflecting pre-existing conceptualizations of the phenomenon of interest. Furthermore, we engaged in member checking (Creswell & Poth, 2018) by sending the participants transcripts of their interviews for review. Brief follow-up interviews with participants provided an opportunity for them to verify the accuracy and completeness of the transcripts; follow-up interviews also allowed participants to clarify and elaborate on points raised in the first interview, as well as allowing the researchers to clarify their understanding of the interview data. Finally, an audit trail of methodological processes, interpretive decisions, and revisions (e.g., changes to codes and themes, based on peer reviews) was maintained throughout the study and retained after the study’s completion. Due to the sensitive nature of the interview data, the data are not publicly available and have been stored in accordance with ethical and REB requirements.
As part of methodological integrity and reporting standards of qualitative research, it is important for researchers to acknowledge their backgrounds or situatedness in relation to the study topic (Levitt et al., 2018), as this allows the reader to better understand the study’s context. The first author (HA) completed her graduate degree in counseling psychology, under the supervision of the second author (JVV). In addition to multiple years of training and practice in counseling, HA has extensive experience volunteering on distress lines in a large Western Canadian city. JVV is a researcher, instructor, and registered psychologist who has been conducting research in the area of compassion for more than a decade.
Findings
In the sections that follow, we briefly summarize participants’ experiences of suicidal ideation, as revealed in the interview data. Turning to the main question of how participants experienced compassion toward others as a salient aspect of recovery, we then provide detailed descriptions and supporting data excerpts to represent the themes that emerged across participant cases. Consistent with IPA, our interpretations are grounded and contextualized in participants’ lived experiences of compassion toward others, as a salient aspect of the recovery process. The specific accounts that participants shared in the interviews were consistent with how participants appeared to conceptualize compassion more broadly. For instance, when asked to define what compassion toward others meant to them in general, participants described it as noticing another person’s suffering or vulnerability; experiencing caring and concern; seeing from the other person’s perspective, otherwise framed as “stepping into other people’s shoes”; and emotionally relating to the person’s pain. Furthermore, compassion toward others meant wanting to reduce the person’s suffering, as well as taking action to help the person struggling (e.g., through acts of kindness). As Jessie stated, compassion toward others was “noticing any sort of suffering in somebody and reaching out in kindness and concern and wanting to alleviate that suffering.” For Holleigh, the recipient of compassion “can be people that are close to you, it can be strangers,” and a person being compassionate “cares about these people and acts accordingly.” Similarly, Flynn regarded compassion toward others as “treat[ing] someone you barely know, your friends, your neighbors, or even someone [like] a stranger, if they need help, be there for them.”
Participants’ Experiences of Suicidal Ideation
In mentioning their previous experiences of being suicidal, participants recalled having been in a “dark place” (Flynn) or “bad state of mind” (Todd) where they had repeated thoughts of “doing something” to end their life (Jane), “wanting to die” (Syke), “just disappearing…and leaving the world,” (Holleigh) and having “no other option” to suicide (Jessie). A suicide attempt and subsequent hospitalization was reported by one participant (Jane). Participants described how the experience of suicide was associated with feelings of life being devoid of meaning, purpose, and hope. In Skye’s words, “I saw everything as ‘What’s the point?’” A sense of worthlessness and harsh self-judgment went hand-in-hand with thinking that it would not matter to other people if the participant were dead. For example, Holleigh stated, “I felt like it didn’t matter if I was there,” and “It was very easy to feel like I was kind of a waste of space.” All participants described a sense of social isolation, alienation, and withdrawal. As Flynn stated, “You don’t feel like there’s anyone there to help you, …no one there to understand you,…[which is] why the dark thoughts happen.”
Common Themes
Six common themes were evident in the majority of cases: (a) sense of meaning and purpose; (b) reciprocity; (c) positive self-concept; (d) non-judgement and acceptance; (e) social connection; and (f) cost of compassion. Each theme, while related to other themes, represents a distinct aspect of participants’ experiences of compassion toward others as part of the process of recovering from suicidal ideation. Table 1 shows the occurrence of each central theme across the participant cases.
Sense of Meaning and Purpose
From the perspective of five participants, compassion for others represented a source of meaning and purpose, which helped to reduce suicidal ideation. As participants recognized the meaning and value that their compassion had in the lives of other people, their own lives became more meaningful. Additionally, a sense of meaning came through reflecting on how their death by suicide would negatively impact family members and friends. For instance, Skye described the impact of helping her brother, who had been suffering from serious mental health problems: “I was able to do something for somebody, and…what I did meant something to somebody else. Like, there was some point of being alive. At that point what I thought [was] that somebody would care if I wasn’t.” Similarly, Flynn experienced compassion toward a friend struggling with depression and academic concerns. Being among the few people who knew of his friend’s issues, Flynn felt “very responsible” for her well-being. His feelings of compassion and sense of responsibility for his friend motivated him to keep living.
For some participants, the sense of purpose that came from compassion counteracted thoughts of being a burden on others. This was apparent, for example, in the case of Jessie: “When you’re…not in a good place…you just think, ‘Oh, people are better off without me, you don’t need me,’…[and] ‘I’m making their lives worse.’” However, when Jessie saw the impact that her compassion had on other people, she became aware of her importance in others’ lives: “Helping others and [being] actually able to help them in a way, it just helps you realize, oh, maybe I’m making a positive impact on their life.” A similar sentiment was expressed by Holleigh, who found meaning in possible opportunities to be there for other people in the future: The way I rationalize that is maybe you’re not doing anything for anyone right now, but just because you’re not doing that right now doesn’t mean that you will not in the future,…like, if you choose to just disappear and then five years down the road there’s someone that you could have helped if you had stuck around…You don’t know what the future has in store.
Reciprocity
Although the main focus of this study was on participants’ experiences of compassion toward others, it was evident from participants’ accounts that compassion was frequently experienced as part of a mutual process of give and take. Both compassion toward and from others reinforced each other and appeared to facilitate participants’ recovery. Most commonly, the giving and receiving of compassion occurred simultaneously within friendships, which at their core were characterized by two-way reciprocal exchanges. Jane, for instance, described how she and a friend who also struggled with suicidal ideation acted compassionately toward each other: “[We] were both really invested in each other’s lives,… [we] made decisions based on each other. I would do something for the sake of her, and she would do something for the sake of me.” From Jane’s perspective, reciprocal acts of compassion helped “push aside intrusive suicidal thoughts” for both women. Similarly, reciprocity featured strongly in Jessie’s experience of compassion. Given Jessie’s reputation as a compassionate person, her friends often elicited her support during times of distress. At the same time, Jessie was drawn to her friends due to their compassionate natures. As Jessie stated, knowing that she and her friends could rely on each other for compassion “feels nice…, reassuring like, you have people that you want to be in your life…forever.” For both Jessie and Jane, the experience of compassion as part of a reciprocal process helped them feel supported, reassured, and more invested in the future.
In some cases, compassion from others was both unexpected and unbidden. For example, Flynn supported his friend through mental health challenges that were much “worse” than his own. Although Flynn had not expected his friend to reciprocate, he later found himself on the receiving end of his friend’s compassionate listening, encouragement, and advice. Another example can be gleaned from Todd. While in the throes of suicidal thinking, Todd derived considerable strength from helping friends and family members with their personal problems. In the process of extending compassion toward the people in his life, he found that they were eager to express compassion toward him as well: Through talking with other people, they’re kind of reiterating how like, what I’m going through is transitory, and once I find the [university] program that I really enjoy…I’m going to enjoy school better, I’m going see life in a better way.
Regardless of whether compassion from others was expected, participants were open to receiving it. Knowing that other people cared enough about them to express genuine compassion gave the participants a reason to stay alive.
Positive Self-Concept
In addition to strengthening participants’ sense of meaning and purpose, compassion toward others promoted a positive shift in self-concept. From the perspective of most participants, being a helper became a central aspect of their identity as well as a source of pride and self-worth. A more positive self-concept helped reduce the negative self-perceptions that had fueled suicidal thinking. Such a shift was evident with Flynn. During his struggles with suicidal ideation and depression, Flynn discovered that some of his friends shared similar issues. The more that Flynn was able to help his friends, the prouder he felt about himself: “If you need help,…if something happens, you know, I’m that guy, and I feel like I always take pride in that.” Over time, the pride that came from being a helper diminished the sense of shame that Flynn had felt when suicidal. Skye experienced a similar transformation through the power of helping. During periods of suicidal ideation, Skye suffered from intense shame and self-blame, which exacerbated thoughts of suicide. However, as she practiced compassion toward others, she began noticing and appreciating positive qualities in herself. Describing how compassion toward others figured into her interpersonal relationships at work, Skye stated: “When I saw [children at her workplace] who were having a bad day… start smiling and talking to me or start connecting with me…and next time they would come to me for help,…it just seemed like they trusted me more.” In addition to perceiving herself as a compassionate person, Skye found that she became less prone to blaming herself for negative events in her life: Before, if I had a fight with one of my friends or something then I’d just be like, oh, I’m not a likeable person…Now it’s just like, okay, we’re just different, it’s not going to work out or whatever. Like, I don’t really care as much.
As evident in the above quote, compassion toward others helped promote resiliency through a more robust sense of self.
Non-judgement and Acceptance
Several participants explained how compassion toward others during the recovery process meant being less judgmental and more accepting of other people. Jane, for instance, reflected on how she shifted from being a “very judgmental person” to approaching others with openness and understanding. Through her own personal struggles, she became more attuned to the painful feelings and mental health challenges that often lay hidden behind people’s “masks.” Jane’s awareness of other people’s suffering allowed her to set aside her pre-existing beliefs and opinions about others; instead, she attempted to adopt a more accepting stance. This new stance not only improved Jane’s interpersonal relationships, but it also helped her find a sense of inner peace. The movement toward greater non-judgement and acceptance was echoed by Skye, who described herself as initially defaulting to automatic negative judgements of other people. During her period of recovery, and especially while helping her brother through a mental health crisis, she began to question her assumptions about what lay beneath the surface of people’s behaviors. As she developed greater empathy toward others, she made a more conscious effort to give people the benefit of doubt. Furthermore, she experienced greater enjoyment in being around people and engaging in acts of kindness, however small: “If saying a few words can make someone’s day better, why not?”
In addition to becoming less judgmental of others, some participants indicated that compassion toward others helped them become more accepting of themselves. Holleigh described herself as having been very self-critical while experiencing thoughts of suicide. During the recovery process, she actively practiced compassion and nonjudgment toward others, regardless of their behaviors or circumstances. She noticed, however, that she continued to judge herself harshly. Awareness of this dissonance opened up the possibility of accepting herself “a little.” Speaking about her more recent feelings about herself, Holleigh explained, “There are some things I don’t like about myself still, and there will always be, and that’s okay. But I think for the majority of it I am happy with who I am.” Like Holleigh, Todd also struggled with negative self-judgement during times of considering suicide. This tendency was particularly acute when he compared himself to social media images of his friends and acquaintances, who appeared happy and successful. However, as Todd learned about the personal struggles of his friends and family and responded with compassion, he began easing his criticisms of himself. As Todd stated, everyone suffers, “they’re just not posting [it] on Instagram.”
Social Connection
From the perspective of five participants, compassion toward others facilitated a movement from social isolation to a place of greater social connection and belonging. This change was an important aspect of participants’ recovery process. Todd, for example, described himself as being a naturally introverted person who appreciated solitude. As part of his struggles with suicidal ideation, Todd entered a prolonged and painful period of social isolation. One day, he offered to drive his partner’s father to a surgical appointment. What was originally meant as a favor to his partner became a turning point for Todd. Throughout the car ride, he witnessed his partner’s father being in extreme physical pain. Todd then realized that he was not the only person facing adversity and that “just being able to help someone else” was a welcome respite from his own emotional turmoil. With these realizations came that additional insight that social isolation had been making Todd’s pain worse: “After that experience, I realized that it [social isolation] wasn’t helping. So, I had to, I wanted to change it.” Despite being a self-described introvert, he increasingly initiated contact with his friends and family and engaged in more social interactions. Over time, Todd’s mental health improved. Jessie, too, challenged herself to overcome tendencies and behaviors that had contributed to social isolation. Jessie’s tendency toward solitude was exacerbated by her “feeling like a burden” on other people in her life. As part of her experience of compassion toward others, she connected with friends, acquaintances, and strangers, coaxing her out of isolation. Throughout the experience, Jessie realized that she was not a burden; others needed her, and she needed others.
For most participants, social connection and compassion toward others reinforced each other in an upward spiral of recovery. Compassion appeared to be a spark that helped participants break through social isolation by motivating them to actively strengthen social connections; and through increased social engagement, participants experienced further opportunities for practicing compassion. This dynamic was evident in the case of Holleigh, who recalled the sense of isolation she experienced after she and her family had moved to a new country, where Holleigh had no friends and was challenged to learn a new language. The lack of social interaction outside of her family contributed to her suicidal ideation. However, part of what kept suicide at bay was spending many nights listening to her sister’s problems, as well as helping her mother to learn English. The experience of feeling “useful” to her family gave her the strength and confidence to expand her social network to people outside of her family. Holleigh’s motivation to make a positive difference in others’ lives, combined with her desire to forge a place of social belonging, eventually led to her creating a mobile application that helped individuals connect socially in their communities.
Cost of Compassion
All participants perceived compassion toward others as being predominantly beneficial for recovery. However, four participants indicated that compassion also had potential disadvantages in the recovery process. At times, participants felt distress, overwhelmed, or exhausted from being compassionate toward others. Jessie, for instance, described how compassion was at times “exhausting, like, mentally and emotionally having to constantly be there for someone and having to constantly listen…to their problems.” She further explained: “[It] affected me because them being sad would make me sad,” and she spent many sleepless nights worrying about her friends. Similarly, Skye noted how supporting her brother through his mental health difficulties caused her distress: “[It] wasn’t like showing compassion…was negative; it was just…some of the things that I had to listen to, they weren’t helpful for me.”
For some participants, the costs and benefits of compassion were influenced by the perceived gratitude—or lack thereof—shown by the recipient. This was true for Holleigh, who found it easier to express compassion to individuals who were grateful for her efforts: “It feels better to help someone that actually…is thankful…They don’t even have to do anything back…They just have to be thankful or show their appreciation.” On the other hand, in friendships where compassion was consistently one-sided, some participants felt exploited. Flynn, for example, recalled feeling “used” by a friend at university: This person that I met who also lived on my floor that year…and we just talked. She had her own issues going on mentally and whatnot, and I was there to help, like, “If you need anything if you want to talk.” And then, over time, it’s when you realize that person was just using you, I guess maybe this is one way compassion became unhealthy.
As the above examples illustrate, while participants appreciated the benefits of compassion toward others, they also acknowledged and honored the importance of their own needs.
Another way of framing the above is through the lens of self-care. More specifically, participants recognized that their recovery depended in part on their ability to balance compassion toward others with attention to their own mental health needs. For instance, to cope with the emotional exhaustion of supporting her friends, Jessie learned “when to take a step back and take care of myself.” Although knowing her limits remained difficult, Jessie had “gotten better” at acknowledging and tending to her own needs. Sometimes tending to her needs meant “recharging my social batteries.” However, Jessie required a balance between alone time and social connection so as not to fall back into isolation. The balance could be challenging; nonetheless, Jessie felt that she could not help her friends if she was not caring for herself.
Discussion
This qualitative study investigated the lived experience and impact of compassion for others, as a salient aspect of students’ recovery from suicidal ideation. From the perspectives of the six undergraduates who participated in the study, compassion was conceptualized as awareness of another’s person’s suffering; caring, concern, and emotional resonance; and action or desired action to help. Students’ interpretations of compassion were congruent with how compassion is currently defined in the literature (see Gilbert, 2014; Strauss et al., 2016).
Six common themes appeared across participants’ accounts of compassion toward others and its role in promoting recovery. The first theme, sense of meaning and purpose, represents how making a positive difference to others through compassionate action motivated participants to stay alive. This theme relates to Klonsky and May’s (2015) three-step suicide framework, where an individual’s disconnection from aspects of life that provide a sense purpose may contribute to the suicide process. Furthermore, as Hill et al. (2016) have asserted, a sense of purpose is increasingly recognized as an important aspect of healthy development during emerging adulthood. Thus, our findings raise the possibility that compassion toward others helped reduce participants’ risk of suicide, while at the same time promoting the achievement of key developmental tasks. In the present study, the feelings of purposefulness that arose through compassion were also accompanied by a sense of responsibility to family and friends, especially when participants reflected on how their suicide would negatively impact the people left behind. These findings align with previous research pointing to a positive relationship between compassion and a sense of responsibility to others (Leedham et al., 2020) and to the protective role of the latter in suicide prevention across diverse populations (Wang et al., 2022). In addition, some participants in our study described how an increased sense of purpose went hand in hand with greater feelings of hope. The perceived effect of compassion on hope and suicidal ideation is not surprising, given the existing literature on the interconnectedness of hope and purpose (Spandler & Stickley, 2011), along with their roles in preventing suicide (Bryan et al., 2019; Klonsky & May, 2015; Sun & Long, 2013). What is novel in the current study, however, is qualitative evidence pointing to a potential link between undergraduate students’ compassion toward others and recovery from suicidal ideation, through an increased sense of purpose and hope. Future research may help tease out these potential mechanisms of change.
The second theme, reciprocity, encapsulates the mutuality that most participants experienced in the giving and receiving of compassion, especially in their friendships. Several participants indicated that expressing compassion toward others strengthened participants’ ability to receive compassion in return, further helping to reduce suicidal ideation. As mentioned earlier, compassion can be thought of as part of a flow or triad consisting of compassion toward others, compassion from others, and compassion from oneself (Gilbert, 2014). According to previous research, an individual’s facility with one direction of compassion does not necessary translate into facility with other directions; many people are more open to expressing compassion toward others and less tolerant of accepting compassion from others (Best et al., 2021; Cunha et al., 2021). However, the literature also suggests that although some directions of the compassion flow might be difficult for individuals to access initially, the experience with one direction of the flow can act as a gateway for being more open to another direction (Kirby et al., 2019). The current findings on the relationship between compassion toward others and receptiveness to compassion from others are especially important given that being open to receiving help from compassionate others can be a powerful step in the process of recovery for adult survivors of suicide attempts (Frey et al., 2018).
In the third theme, positive self-concept, participants attributed reductions in suicidal ideation to compassionate behaviors, partly through the influence of such behaviors on participants’ conceptualizations of themselves. Participants’ beliefs about themselves shifted in a positive direction, such that they noticed and took pride in who they were as compassionate individuals. The development of a positive self-concept is a key feature of emerging adulthood (Arnett, 2018); and undergraduate students who struggle with achieving a positive identity may be more susceptible to suicide (Joiner et al., 2009; Kuper et al., 2018; Rasmussen et al., 2018; Turner et al., 2010). Some studies have pointed to compassion toward others as a potential strategy for improving self-concept across a range of populations, including undergraduate students (Mongrain et al., 2011; Piferi & Lawler, 2006). The present study helps bridge the research on suicidal ideation, self-concept, and compassion by showing how, from the perspectives of previously suicidal undergraduates, compassion toward others may help reduce suicidal ideation through improvements in self-concept. Future testing of these relationships in undergraduate student populations is clearly warranted.
Nonjudgement and acceptance, the fourth theme in our findings, refers to participants’ perceptions of themselves as becoming less judgmental and more accepting of other people, as part of the experience of being compassionate toward others. These findings are consistent with the literature, where non-judgement has been recognized as an important element of compassion and is associated with feelings of well-being (Gilbert, 2009a; Neff, 2003). Findings from the current study add to the existing research by highlighting potential relationships between compassion toward others, nonjudgment, and recovery from suicidal ideation. Some participants also described how expressing compassion toward others allowed participants to reframe their own experiences through a non-judgmental lens. Self-acceptance, in turn, further reduced suicidal ideation. This is in keeping with research on the important roles that both self-acceptance and self-compassion may play in preventing suicide among emerging adults and undergraduate populations (Kelliher-Rabon et al., 2018; Williams et al., 2006). Moreover, our findings support the view of compassion as part of a multi-directional flow in the specific and unique context of undergraduate students recovering from suicidal thinking (Gilbert, 2014; Kirby et al., 2019).
A fifth theme that spanned the majority of participants’ accounts of how compassion toward others helped in the recovery process was social connection. Through acting compassionately toward others, participants experienced less social isolation and a greater sense of belonging. Not only do these findings align with previous research on the crucial roles of social connection and belongingness in suicide ideation among emerging adults (Joiner et al., 2009), but they extend existing research by showing how compassion toward others may be a useful strategy for strengthening these factors among suicidal undergraduates. In addition, some participants described how social connection was accompanied by reduced feelings of being a burden on others. Feelings of burdensomeness were connected to the earlier theme of purpose, where participants realized that others needed and valued them, thereby challenging thoughts of burdensomeness. This finding is consistent with Joiner’s (2007) Interpersonal Theory of Suicide and with research that associates diminished burdensomeness with less severe suicidal ideation in young adult populations (Joiner et al., 2009). A potentially fruitful direction for future studies would be to test burdensomeness, social connection, and belonging as potential mediators in the relationship between compassion toward others and suicidal thinking.
The final theme, cost of compassion, highlights how compassion toward others, despite its perceived benefits for recovery, was not without potential drawbacks. Participants discussed how compassion for others occasionally impacted their recovery negatively, especially when the participants neglected their own self-care or felt exploited by the recipient of compassion. In literature on the relationship between compassion toward others and self-compassion, it has been suggested that compassion toward others may at times be used as an unhealthy mechanism for avoiding one’s emotional pain and needs (Gerber et al., 2015; Gilbert et al., 2017). Although this potentially negative side of compassion toward others did not emerge as a theme in the current study, this could be a fruitful avenue for future inquiry, especially given how emotional pain feeds into the suicide process (Klonsky & May, 2015). It may also be useful to consider the current findings on the costs of compassion in the context of the literature on compassion fatigue and compassion satisfaction. Turgoose et al. (2017) defined compassion fatigue as the experience of emotional and physical exhaustion from helping others, leading to diminished compassion and empathy, as well as the inability or unwillingness to persist in carrying others’ suffering. Compassion satisfaction, on the other hand, refers to the rewarding feelings that arise from helping others (Slocum-Gori et al., 2013). Regular self-care practices and having strong social support are among the factors that influence compassion satisfaction (Ray et al., 2013). Although most research regarding compassion fatigue and satisfaction focuses on healthcare workers, especially those working with trauma survivors (Turgoose et al., 2017), it is possible that these phenomena might also occur in individuals who are recovering from suicidal ideation and expressing compassion in their personal lives. The potential roles of compassion fatigue and compassion satisfaction in the recovery process are an important direction for future research.
Clinical Implications
Although the focus of this study was not on the experience of therapy, our findings may nonetheless sensitize clinicians to the therapeutic potential of compassion toward others, while also generating ideas and possible strategies for working with undergraduate students struggling with suicidal ideation. We offer the following recommendations tentatively, with the caveat that research on compassion-based clinical interventions for suicidal undergraduates and other populations is required.
Given the power of compassion to increase a sense a purpose for the participants, clinicians might consider exploring with their clients how their lives may gain greater purpose and meaning through the intentional and focused practice of compassion. For instance, based on the unique interests and contexts of each client, the client might decide to volunteer as a helper on campus (e.g., through a peer support group) or in the wider community. More informal opportunities for achieving purpose could also be discussed, such as reaching out to friends in need and offering assistance. Clients might additionally benefit from seeking opportunities to extend kindness to acquaintances and strangers. The above practices may have the further advantage of increasing clients’ sense of social connection and belonging.
The theme of reciprocity also points to potential strategies for counseling suicidal students. In our findings, some participants experienced compassion toward others as part of a compassion flow between themselves and their friends. Therefore, it might be helpful to explore and monitor clients’ willingness to be on the receiving end of compassion. As part of this exploration, practitioners might initiate discussion about cultural norms and other cultural factors that may have a bearing on the client’s help-seeking behaviors. Another important topic for potential exploration might be specific fears and beliefs that may be contributing to clients’ reluctance to accept compassion from others (see Gilbert et al., 2011). An example of such a limiting belief can be gleaned from our study, where some participants perceived themselves to be a burden on people in their personal lives. Therapists might also recommend that suicidal clients practice compassion for others, as a means of improving how clients view and relate to themselves. For instance, in a classic cognitive behavioral exercise from compassion-focused therapy (Gilbert, 2009b, 2014), clients are invited to imagine themselves as having positive qualities of compassion. Clients are then encouraged to practice acting in a manner consistent with that image, as well as directing the compassionate qualities of that image inward, toward themselves. Through such compassion practices, a client might notice a shift in their self-concept and self-compassion (Gilbert, 2014). In another compassion-focused intervention aimed at reducing self-judgement (Falconer et al., 2014), clients are invited to focus on the suffering of another person and asked how they might approach that person in a nonjudgmental way. The same exercise would then be repeated, but with the client focusing on themselves. After the exercise, the client is asked whether they noticed a shift in their judgements toward others as well as themselves.
In addition, clinicians should be aware of the risk of compassion fatigue for clients in their practice of compassion toward others. It could be important to inform clients about possible signs of compassion fatigue and monitor these signs, in the wider context of the recovery process. The practitioner and client might collaborate on developing a self-care plan that fits with the client’s needs and that strikes an appropriate balance between supporting others and supporting oneself.
Limitations and Future Directions
A number of limitations should be considered when interpreting findings from this study. For one, as with all IPA studies, the findings represent the researchers’ interpretations of participants’ interpretations and are not meant to represent statistically-derived generalizations that apply to the wider population. Quantitative research could expand upon the current study through testing the findings therein.
Second, due to COVID-19 public health mandates, all interviews took place either via video conferencing or telephone instead of in-person. Such communication methods may have resulted in a less complete understanding of the participants’ experiences, as nuances in participants’ expressions (e.g., body language, thoughtfulness, emotional reactions, etc.) were more difficult to detect, especially over the telephone.
Another limitation relates to the inclusion criteria. As part of the screening process, participants were asked to confirm that they had experienced suicidal thinking and/or behaviors in the past. For ethical reasons, participants were not explicitly asked for specific details on their experience of being suicidal; rather, the main scope of the interviews was on recovery, with the specifics of suicidal ideation and behaviors emerging based on what participants spontaneously decided to share in the interview. Although a careful reading of the interview transcripts allowed us to gather some information on the nature of past suicidal ideation that was evident in all participant accounts of recovery, only one participant spontaneously disclosed a suicide attempt. Thus, based on participant accounts and self-reports, the scope of our findings is limited to suicidal ideation. We also did not include formal measures of past symptoms of suicide. Thus, we were limited in our ability to differentiate between various forms of suicidal ideation and behaviors in our analysis of the role of compassion toward others in the recovery process. Perhaps the participants’ experiences with compassion for others might have differed depending on the specific nature and severity of symptoms. The question of how compassion toward others related to where students were at in the process of suicide would be a potentially fruitful direction for future research provided that appropriate safeguards are in place. To assess the stability and resources of potential participants, additional screening measures (e.g., mental health symptoms, available supports) could be used as part of the recruitment process. Furthermore, the inclusion criteria required that participants be free of suicidal thoughts and behaviors for at least one year. However, we did not set an upper limit on the length of time that participants were required to be symptom-free. Therefore, some participants may have experienced symptoms more recently than others, possibly impacting participants’ memory of their experience. The recovery period, as interpreted and experienced by participants, also varied within the sample. It is possible that longer periods of recovery may have provided more opportunities for compassion. Additionally, participants needed to be willing and able to articulate their experiences of compassion for others, and how it aided in recovery from suicidal thoughts and/or behaviors. Although the inclusion of rich informants made sense given our research purposes and fit with IPA standards (Smith et al., 2009), it meant that the study did not capture the perspectives of individuals who either struggled with compassion for others, or who were unable or unwilling to provide accounts of their experience.
The current study included perspectives of self-identified women and men and did not tease apart potential differences in experience between genders. However, gender may influence both suicide (Lamis & Lester, 2013) and compassion toward others (Gilbert et al., 2017). Furthermore, missing from the sample were participants who self-identify as LGBTQ+ and gender-divergent. Given the high rates of suicidal ideation and behaviors among LGBTQ + students (Liu et al., 2019), many of whom are faced with multiple forms of marginalization and discrimination on campus, this area requires further attention.
A notable strength of this study was the cultural and ethnic diversity in the sample. In predominantly White campuses and communities, students from visible minority groups may face racial discrimination and other factors related to minority stress, which may increase the risk of suicide (Pillay et al., 2021). Furthermore, the experience of compassion may vary from culture to culture (Koopmann-Holm & Tsai, 2017). Future researchers should further explore the role of compassion toward others in reducing suicidal ideation and behaviors across different cultures (e.g., comparisons between individualistic and collectivist cultures) and within specific cultures and sub-subcultures. Research on the experience and meaning of compassion toward others as part of recovery is also needed with emergent adults who are not students, as well as other age groups. Finally, it would be important to research how the six themes that emerged from this study could be incorporated into clinical interventions for suicidal undergraduates, and to what effect.
Conclusion
With suicide being a major cause of death in emerging adulthood (Mortier et al., 2018), research on prevention strategies is crucial. Findings from our qualitative study suggest that for some emerging adults, compassion toward others may be a helpful strategy for reducing suicidal ideation. Based on the experiences and perspectives shared by this study’s six participants, it appears that compassion directed outwardly may help counteract the sense of hopelessness, isolation, and low self-esteem associated with suicidal thinking, through fostering positive ways of relating to others and oneself. This study also highlighted how compassion directed toward others may at times adversely impact emotional well-being. As research on strategies for helping students recover from suicidal ideation continues to evolve, compassion merits further attention as a potential means of preventing suicide in this population.
Supplemental Material
Supplemental The Lived Experience and Impact of Compassion for Others in Undergraduate Students’ Recovery From Suicidal Ideation
Supplemental Material for The Lived Experience and Impact of Compassion for Others in Undergraduate Students’ Recovery From Suicidal Ideation by Hailey N. A. Allegro and K. Jessica Van Vliet in Emerging Adulthood.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Open Practices
The interview protocol used for this study is included in Appendix A. Due to the sensitive nature of the data and and the privacy requirements approved by the institutional research ethics board, the data are not openly available. Questions related to the data and related materials may be directed to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
Appendix
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.