
Abstract
The transition to adulthood, including mental health, has been a focus of research; however, little is known about the mental health outcomes of emerging adults with high incidence diagnoses including ADHD and specific learning disabilities (SLD). This scoping review describes the current state of the research on our understanding of both positive and negative mental health outcomes in these populations. Results of this scoping found an emphasis on emerging adults with ADHD (78%) over those with SLD (12%) or with ADHD and SLD (10%), and over half focused on those who attended postsecondary institutions despite low percentages of these populations going on to postsecondary education. Studies included frequently provided limited information on race or ethnicity, sex or gender, or ADHD or SLD subtypes. Additionally, there was greater focus on negative mental health outcomes (e.g., anxiety, depression) than positive mental health outcomes (e.g., wellbeing, flourishing). We end by discussing implications for future research.0020.
Introduction
Emerging adulthood, which is a distinct life stage between adolescence and adulthood, requires important tasks including forming identity, attaining academic training, and exploring potential career paths (Arnett et al., 2014). Additionally, the newly found freedom during this time can bring instability and challenges including challenges that may not have been experienced by previous generations. In particular, economic uncertainty has created unique financial difficulties for this age group, which directly impacts decisions related to housing, family life, attending postsecondary, and entering the labor market (Hallquist et al., 2011; Terriquez & Gurantz, 2015). Although emerging adulthood is a relatively new distinction in the lifespan, the mental health challenges of emerging adulthood are well documented. One in five emerging adults experiences a mental illness, and the rate of substance use disorders is twice that of adults aged 26 and older (Rosenberg, 2016).
Attention Deficit Hyperactivity Disorder and Specific Learning Disabilities
The transition to adulthood can be a stressful period, and these difficulties can be intensified for those with common neurodevelopmental diagnoses such as attention deficit hyperactivity disorder (ADHD) and specific learning disorder (SLD), which both have high prevalence rates. The prevalence rate for ADHD is 5%–15% (American Psychiatric Association [APA], 2022) It is important to note that only 10% of individuals with ADHD experience remission in adulthood (Sibley et al., 2022), and prevalence rates in adulthood are around 2.5% (Farone et al., 2021). ADHD is a neurodevelopmental disorder which involves difficulty with sustaining attention, behavioural inhibition, and hyperactivity (APA, 2022). An ADHD diagnosis should specify whether presentation is predominantly inattentive (I), hyperactive-impulsive (H), or combined (C). While causality remains a question in ADHD research, correlational studies have found higher rates of ADHD in those with a first degree relative with ADHD, certain genetic variants, higher exposure to adversity (e.g., low income, family conflict, and maltreatment), maternal substance misuse in pregnancy, and low birth weight (Thapar et al., 2012). Evidence also suggests that sex may influence ADHD presentation and prevalence. For example, males tend to present with more externalizing symptoms in ADHD, while females present with more internalizing symptoms (Rucklidge, 2010). Recent studies have also identified potential racial disparities in ADHD diagnosis, such that the intersection of race, socioeconomic status, and discrimination may exacerbate ADHD symptoms—particularly in Black youth (Cenat et al., 2021).
The rate of SLD is about 7% (APA, 2022), with half of all 15–24-year-olds in Canada with a disability reporting an SLD (Statistics Canada, 2012). SLD is characterized by difficulties in learning and may include a specification of impairment in reading (e.g., decoding, fluency, or comprehension), also known as dyslexia; writing (e.g., difficulty in spelling, grammar, or punctuation), or mathematics (e.g., number sense, calculation, or mathematical reasoning; APA, 2022), also known as dyscalculia. Common risk factors for SLD include low income, history of neonatal jaundice, born by Caesarean, developmental delay in walking, and history of learning difficulties in parents (Görker et al., 2017). When examined concurrently, ADHD and SLD have shared neuropsychological and genetic factors, which may at least partially explain their high degree of comorbidity between these diagnoses which have an estimated co-occurrence rate of 31%–45% (Pham & Riviere, 2015). Less is known, however, about how these diagnoses affect mental health during the transition to adulthood.
Emerging adulthood is characterized by increased mental illnesses, and individuals with ADHD experience increased rates of psychiatric comorbidity including mood and anxiety disorders (Anastopolous et al., 2018; Biederman et al., 2012; Hinshaw et al., 2012; Meinzer et al., 2016), autism spectrum disorder (Antshel et al., 2013; Antshel & Russo, 2019; Zablotsky et al., 2020), oppositional defiant disorder and conduct disorder (Connor et al., 2010; Hazell, 2010; Noordermeer et al., 2017), and substance use disorders (Abecassis et al., 2017; Wilens et al., 2011). ADHD in emerging adults is also associated with risky sexual behavior (e.g., increased sexual partners and pregnancies; Flory et al., 2006), higher levels of criminal activity and arrests (Barkley et al., 2010), and issues with finances due to compulsive spending (Black et al., 2012). Further, they have higher rates of obesity, allergies, asthma, diabetes, and sleep disturbances (Farone et al., 2021). Many of the negative consequences associated with ADHD may be due to the impulsivity characteristic of this population, as this symptom typically persists into adulthood even after others subside (APA, 2022). Individuals with ADHD also experience difficulties with executive functioning in the domains of planning, organization, attention, inhibitory control, and working memory that negatively affect their functioning and quality of life (Abecassis et al., 2017; APA, 2022; Sjöwall & Thorell, 2022). These skills are important for successful academic and occupational performance, making the challenges of emerging adulthood even more difficult for these individuals (Awh et al., 2006; Miller et al., 2012). During postsecondary education, individuals with ADHD experience more challenges compared to peers including lower GPAs and higher dropout rates (Abecassis et al., 2017; Fedele et al., 2010) and are less prepared for the demands of postsecondary education (Canu et al., 2021). Further, students with ADHD are less likely to pursue higher education in the first place, with only 8% in one study (Hechtam et al., 2016) and 29.5% of individuals in another study (Kuriyan et al., 2013) attending a 4-year college program. In one study only 33.9% of adults with ADHD were employed compared with 59% of controls, and the rates of full-time employment are lower for those with ADHD at all education levels (Biederman & Farone, 2006). Further, they earn less than controls at all education levels with the exception of those who did not complete high school (Biederman & Farone, 2006).
Similarly, individuals with SLDs also experience poorer mental health outcomes including increased stress, substance use disorders, anxiety, depression, and suicidal ideation (Aro et al., 2019; Wilson et al., 2009). Beyond mental health outcomes, statistics from the National Centre for Learning Disabilities indicated that more than half of individuals with SLD report having been involved with the criminal justice system (Cortiella & Horowitz, 2014). Emerging adults with SLDs tend to leave high school unprepared to face postschool environments (Newman et al., 2011). Few attend postsecondary training, with only 15.5% (Sanford et al., 2011) to 21% (Cortiella & Horowitz, 2014) of individuals with SLDs pursuing a 4-year degree, and those who pursue postsecondary education experience lower rates of degree completion, impacting their overall employability (Cortiella & Horowitz, 2014). Consequently, individuals with SLD are twice as likely to remain unemployed compared to the general population (Horowitz et al., 2017). One systematic review found that those with SLD were more likely to be successfully employed if they had strong math skills and active parent involvement in their education (Sharfi & Rosenblum, 2014), suggesting that there are areas for which focused interventions could improve outcomes.
Positive Mental Health
Mental health is generally seen as “a state of mental well-being that enables people to cope with the stresses of life, realize their abilities, learn well and work well, and contribute to their community” (World Health Organization, 2022, para. 1). Furthermore, mental health can be defined as the presence of psychological well-being, and not simply the absence of a mental illness (Tang et al., 2019). Instead of dichotomous categories of “mentally healthy” and “mentally ill,” mental health is better conceptualized as a continuum recognizing that those living with a mental illness or other mental health diagnosis, such as ADHD and SLD, can have positive mental health (e.g., Dual Continuum Model by Keyes et al. [2010]).
Although research has often focused on negative mental health outcomes, including mental illnesses and other challenges regarding wellbeing, enhancing mental health has been increasingly emphasized in recent years. Regarding emerging adulthood specifically, studies have found that finding purpose in life (Hill et al., 2016), having higher self-confidence and lower negative self-evaluations (Matud et al., 2022), and maintaining strong friendships and romantic relationships (Camirand & Poulin, 2022) promote psychological wellbeing during emerging adulthood. In contrast, factors such as career indecision (Viola et al., 2016), casual sexual relationships (Claxton & van Dulmen, 2013), and growing up in a low-income household (Lucas-Thompson & Hostinar, 2013) decreases wellbeing in emerging adulthood. Unfortunately, emerging adults with ADHD and SLDs report lower levels of positive mental health than their peers, including higher levels of mental illnesses diagnoses, such as depression, anxiety, and conduct disorders, as well as substance use issues (Abecassis et al., 2017; Goldston et al., 2007; Harris-Lane et al., 2021). Considering the high prevalence rates of SLD and ADHD among emerging adults and the higher rates of mental health challenges in these populations, it is important to gain a better understanding of the research on both the positive and negative mental health outcomes for these individuals. Findings from this review will inform future work to augment positive mental health and mitigate negative mental health outcomes.
Current Scoping Review
To our knowledge, there has not been a comprehensive review of the academic literature pertaining to the mental health of emerging adults with ADHD and SLD specifically. Although Linden and Stuart (2020) examined mental health and wellbeing in postsecondary students broadly, we found no studies focusing mental health outcomes for emerging adults with ADHD and/or SLD or including those who did not go on to postsecondary education. Emerging adulthood is a particularly vulnerable time for this population, as they are at an increased risk for negative mental health outcomes and challenges related to attaining the milestones of this stage of life. Consequently, identifying factors that promote positive mental health and those that increase the risk for negative mental health outcomes in these populations is necessary to promote better outcomes for these individuals. The purpose of this scoping review was to describe the current research regarding both the positive and negative aspects of mental health of emerging adults with ADHD and/or SLD, both describing the current research and identifying gaps in the current literature (Arksey & O’Malley, 2005).
Methods
This scoping review utilized the Arksey and O’Malley’s (2005) framework for conducting scoping reviews: (a) identifying the research question, (b) identifying relevant studies, (c) study selection, (d) charting the data, and (e) collating, summarizing, and reporting the results. The optional sixth stage, consultation exercise, was not included.
Identifying the Research Question
We created several research questions related to the mental health of emerging adults with ADHD and/or SLD to understand the continuum of wellbeing experiences. 1. What contributes to positive mental health outcomes for emerging adults with SLD and/or ADHD who do or do not attend postsecondary institutions? 2. What contributes to negative mental health outcomes for emerging adults with SLD and/or ADHD who do or do not attend postsecondary institutions? 3. Are there differential mental health outcomes for different groups of emerging adults with SLD and/or ADHD? (e.g., university/work force, disability/not, ethnicity/race, gender, rural/urban, in care/in home, national/international, protective/risk factors)
Identifying Relevant Studies
Search Terms.
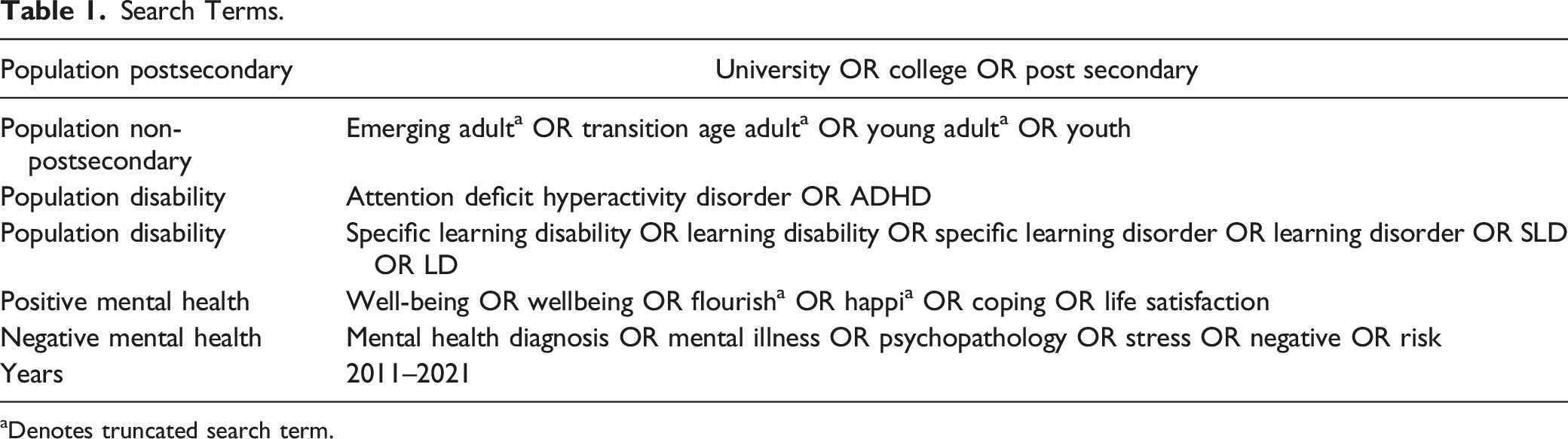
aDenotes truncated search term.
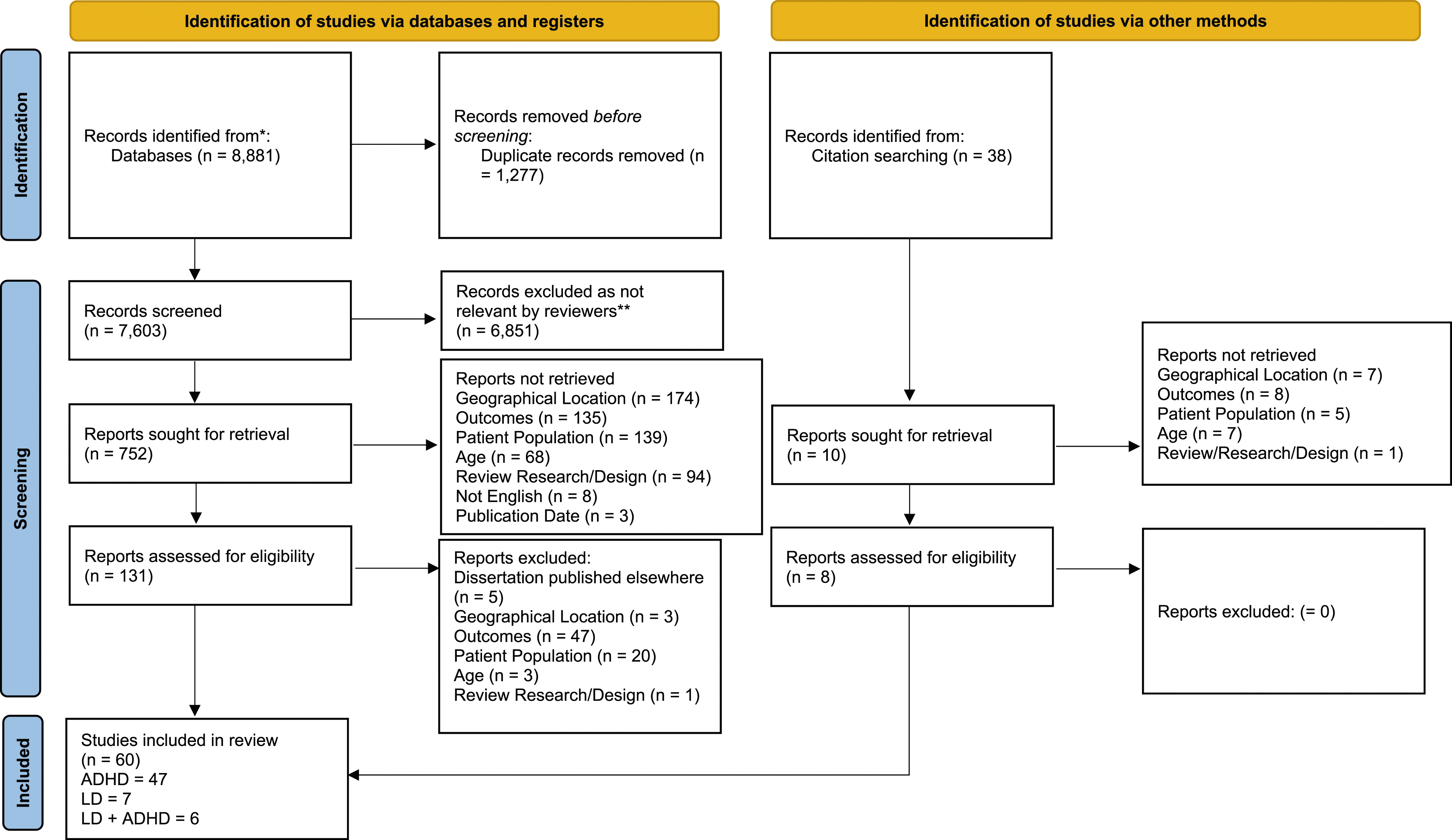
PRISMA diagram results (from Page et al., 2021).
Study Selection
To be included, articles had to measure mental health outcomes in emerging adults with ADHD and/or SLD. As many studies were longitudinal or included broader age ranges, studies were included if at least 50% of the participants were between the ages of 18 and 29 for outcomes reported at any timepoint. Additionally, articles had to indicate that participants had a diagnosis of ADHD and/or SLD, rather than only symptoms of those disorders; however, studies with self-reported diagnoses were included.
Data Extraction
There were 60 studies included in the review: 47 ADHD only, 7 SLD only, and 6 ADHD and SLD. The data extracted from these articles included author(s), date of publication, article title, journal of publication, population characteristics (e.g., sample size, sex, race, ethnicity), study design, and main findings. The reviewers collaboratively examined studies to extract and organize findings.
Results
Summary of research exploring ADHD only (N = 47).

Notes. NR = not reported; CS = community sample; WP = workplace; PS = post secondary; SA = substance abuse; PALS = Pittsburgh ADHD Longitudinal Study; MTA = Multimodal Treatment of Attention Deficit Hyperactivity Disorder Study; ADD Health = National Longitudinal Study of Adolescent to Adult Health; OR = odds ration.
adissertation †reported separately by group °demographics from another study.
bwhen participants chose more than one, numbers do not equal 100%.
Summary of research exploring LD only (N = 7).
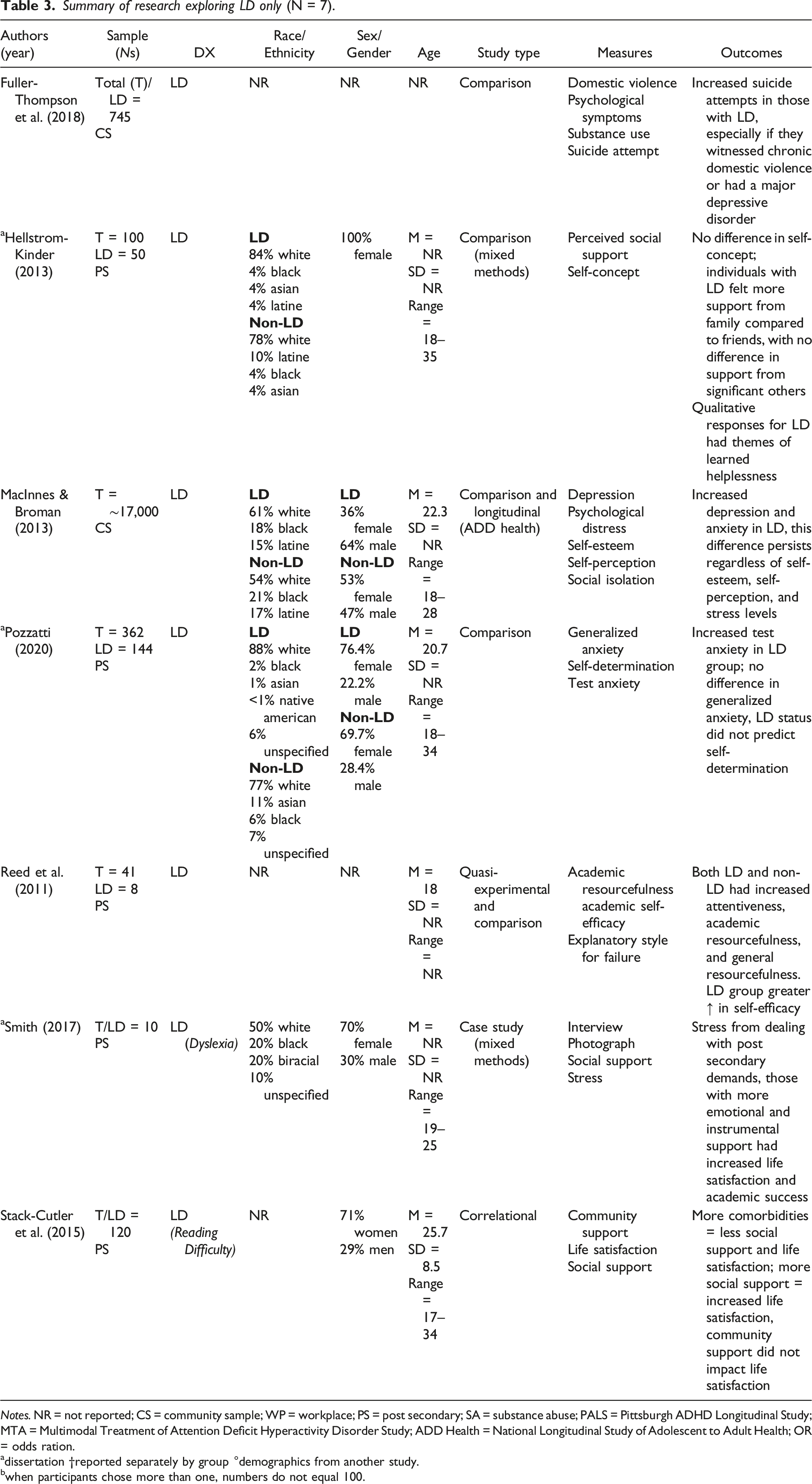
Notes. NR = not reported; CS = community sample; WP = workplace; PS = post secondary; SA = substance abuse; PALS = Pittsburgh ADHD Longitudinal Study; MTA = Multimodal Treatment of Attention Deficit Hyperactivity Disorder Study; ADD Health = National Longitudinal Study of Adolescent to Adult Health; OR = odds ration.
adissertation †reported separately by group °demographics from another study.
bwhen participants chose more than one, numbers do not equal 100.
Summary of research exploring both ADHD and LD (N = 6).
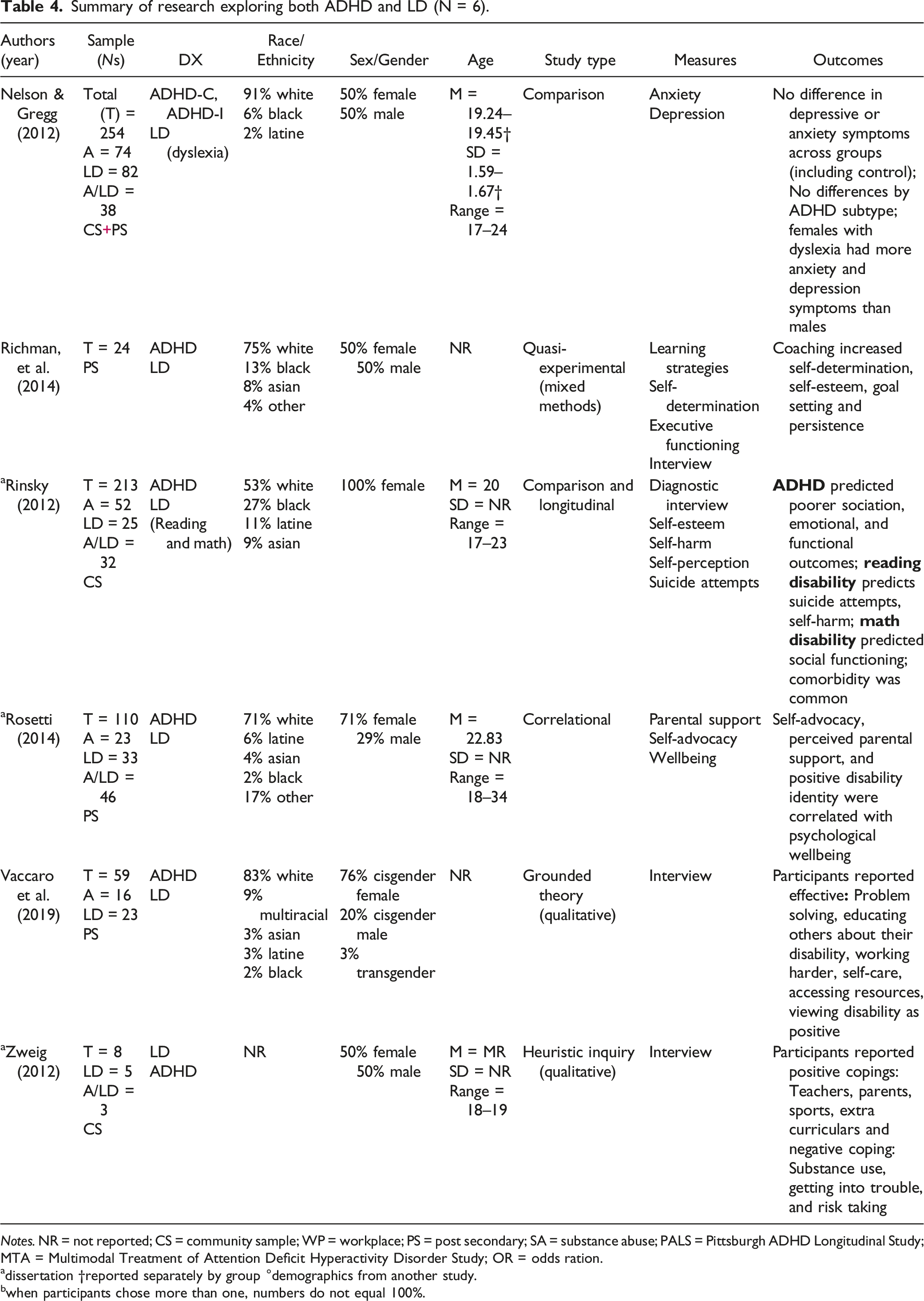
Notes. NR = not reported; CS = community sample; WP = workplace; PS = post secondary; SA = substance abuse; PALS = Pittsburgh ADHD Longitudinal Study; MTA = Multimodal Treatment of Attention Deficit Hyperactivity Disorder Study; OR = odds ration.
adissertation †reported separately by group °demographics from another study.
bwhen participants chose more than one, numbers do not equal 100%.
With these distributions in mind, three primary areas of interest emerged from this scoping review in relation to the types of studies represented: (1) the samples that were utilized in the research and the related issues, (2) the methodologies of the studies, and (3) contributors to both positive and negative mental health, as well as differential mental health outcomes reported in the studies between population type (ADHD, SLD only, and ADHD and SLD).
Study Samples
Of the studies included in this review, 57% (n = 34) drew from postsecondary samples. In examining differences across populations, 65% (n = 26) of those with ADHD, 71% of those with SLD only (n = 5), and 50% of those ADHD and SLD (n = 3) were from postsecondary samples. This focus on postsecondary samples is noteworthy, given that only 8% (Hechtman et al., 2016) to 30% (Kuriyan et al., 2013) of individuals with ADHD and 15.5% (Sanfore et al., 2011) to 21% (Cortiella & Horowitz, 2014) of individuals with an SLD enter postsecondary education. Of the remaining studies, 35% predominantly utilized community samples (n = 21), one of which noted being a predominantly rural sample (Babinski et al., 2017); although this demographic information was not available in other studies. Two studies utilized a combined postsecondary and community sample, with the remaining studies (all ADHD) coming from clinical settings (n = 2; Biederman et al., 2014; Wilens et al., 2011), a twin study (n = 1; Elkins et al., 2020), and archival research from medical claims (n = 1; Babinski et al., 2020).
In terms of diagnostic information, studies frequently did not differentiate between, or provide information on, the number of participants with each subtype of ADHD or SLD. Rather, researchers used these labels as general diagnostic categories. Of those that differentiated between ADHD subtypes (n = 8; 17%), half found differences between the groups (n = 4; Anastopoulos et al., 2018; Canu et al., 2014; Hinshaw et al., 2012 Swanson et al., 2014) while the other half did not (n = 4; Anastopoulos et al., 2021; Landberg et al., 2014; Miller et al., 2012; Nelson, 2013). In addition, only two studies had a primary focus or research question aimed at comparing an ADHD-only sample with a sample with ADHD and a previously diagnosed comorbidity, despite an 80% prevalence of comorbid psychiatric disorders among adults with ADHD (Choi et al., 2022). Of these two studies, one explored comorbid anxiety and depression (Strand, 2016), and the other examined those with comorbid bipolar disorder (Biederman et al., 2014). However, 19 studies assessed additional mental illness symptomology, typically with the intention of identifying correlates or prevalence rates within a general ADHD sample.
For SLD only, two of the seven articles focused on reading difficulties (Smith, 2017; Stack-Cutler et al., 2015), one provided some information on disability, although some of the definitions that were provided (e.g., auditory, visual, and organizational difficulties) did not match DSM criteria for SLD (Reed et al., 2011), and none of the studies incorporated comorbidities. Of the six studies looking at both SLD and ADHD, one examined ADHD subtypes compared to dyslexia (Nelson & Gregg, 2012), another compared those with ADHD, reading, and math disabilities (Rinsky, 2012), and two compared those with either ADHD or SLD rather than studying those who had both diagnoses (Reed et al., 2015; Vaccaro et al., 2019). While there was limited inclusion of comorbidities, many studies across population types included symptoms of other disorders as mental health measures and outcomes, including anxiety, depression, oppositional defiant disorder, conduct disorder, antisocial personality disorder, substance use disorders, and eating disorders.
One noticeable sample issue was the limited information provided on ethnicity and race, with a considerable number of researchers not reporting race/ethnicity at all (n = 21; 35%) or only reporting the percentage of White participants (n = 11; 18%). Many of the remaining 28 studies, provided information on the percentage of Black, Latine, Asian, and White participants in their sample, while only some provided more detailed demographics in including less represented groups (e.g., Indigenous, specific Asian populations, or multiracial). Overall, White individuals were the most represented across studies (n = 36 studies with >50% White sample of those that reported race/ethnicity), with Black and Asian populations often following as the next most represented groups. In other words, of the studies that reported race/ethnicity, 92% had a predominantly White sample. Some studies opted to include a breakdown of race/ethnicity across ADHD (n = 6) and SLD (n = 3) versus controls; although the ethnic breakdowns between groups was similar.
Regarding other demographic information, only a small portion of studies did not report any information on sex or gender (n = 7; 12%). Of the remaining studies, 16 were a primarily male/men sample, 22 were primarily female/women, and four studies had an equal gender split. Other studies utilized only female/women (n = (9) or male/men (n = (2) samples. Overall, there was a slightly higher percentage of females represented across all the studies included in this review compared with typical prevalence rates for ADHD (male:female ratio of 2.28:1; Ramtekkar et al., 2010). This remained true for SLD despite there being relatively little difference in prevalence across genders for SLD (APA, 2022). In terms of age, although all studies met the criteria that at least 50% of the participants were between the ages of 18 and 29 for outcomes reported at one timepoint, studies were often missing data on one or more of the common descriptive statistics of mean, standard deviation, and range (n = 45; 75%). However, from the ranges that were reported, the studies included data from ages 15 to 41, with most participants generally falling within the 18–25 range. Some longitudinal studies that were interested in outcomes over time only reported the demographic information at one timepoint, which may or may not have been the period during emerging adulthood (i.e., often at the first time point, when they were children, as emerging adulthood may not have been the primary focus of the research). In this case, researchers typically provided the follow-up timing (e.g., 2-year follow-up, 10-year follow-up), and (approximate) ages were able to be calculated accordingly.
Methodology of Studies
Many different methodologies were utilized in the studies included in this review, including a variety of both quantitative and qualitative designs. The majority of the studies utilized some form of comparison design, including group comparisons with cross-sectional data (ADHD n = 15; SLD n = 3; ADHD/SLD n = 1), group comparisons with portions of longitudinal data (i.e., only one timepoint included in this review; ADHD n = 6), or group comparisons within a longitudinal design (i.e., also include comparisons over time; ADHD n = 14; SLD n = 1; ADHD/SLD n = 1). There were also a few studies that included both comparison and correlational designs (ADHD n = 3) or correlational designs (LD n = 1; ADHD/SLD n = 1). It is important to note that for comparison studies, researchers commonly had a smaller subsample of participants with ADHD alongside a larger comparison group, which resulted in significantly different group sizes in some research (e.g., Biederman et al., 2012, Total N = 651, ADHD N = 165; Buchanan, 2011, Total N = 317, ADHD N = 34; Mochrie et al., 2020, Total N = 1,748, ADHD N = 198). Some studies only included participants with ADHD and/or SLD in their recruitment (e.g., Anastopoulos & King, 2015; Biederman et al., 2014; Field et al., 2013), with some exploring comparisons within that population specifically (e.g., between subtypes, between genders).
Although most studies used a quantitative design, several studies utilized qualitative methods, either exclusively, or in combination with quantitative methods (n = 6; e.g., Parker et al., 2011; Stamp et al., 2014). There were also quasi-experimental (ADHD n = 4; LD n = 1; ADHD/SLD n = (1) and experimental (i.e., randomized control trials; ADHD n = (2) designs, which investigated the effectiveness of cognitive behavioural therapy (CBT) and mentoring program for students with ADHD (Anastopoulos et al., 2021; Anastopoulos & King, 2015), ADHD coaching (Field et al., 2013; Parker et al., 2011), and an ADHD self-help website (Glickman, 2014).
Several papers utilized data from larger studies that collected data from children with and without ADHD over time (i.e., longitudinally), who were young adults during the later timepoints of the study (e.g., utilizing data from the Program for Academic Learning Skills [PALS] program [n = 6], the National Longitudinal Study of Adolescent Health [ADD Health] = n = 2], the Multimodal Treatment of Attention Deficit Hyperactivity Disorder [MTA] study [n = 2]). This longitudinal approach, especially for those that used data from larger studies or programs (i.e., secondary data), appeared to result in limitations to inquiries that focused specifically on the young adulthood population only, as full demographics were rarely re-collected across timepoints, and the persistence of an ADHD diagnosis into emerging adulthood was sometimes unclear. Studies often utilized demographic data from the complete initial sample (i.e., first timepoint of longitudinal data), collected when the participants were young, rather than the subsample(s) that were the focus of their analyses. This information was rarely updated or reported for later timepoints, making it unclear if participant demographics and diagnoses remained consistent over time (e.g., unsure if certain genders or ethnicities were more likely to complete the study into adulthood). Regarding re-assessment of ADHD diagnosis in longitudinal studies, a significant proportion either did not re-assess for ADHD or did not clearly describe their re-assessment process (n = 7). The remaining studies utilized both diagnostic interviews (n = 8) or self-reported current ADHD symptoms (n = 7). However, in studies that used the latter method, it was often unclear whether these self-reported symptoms still met criteria for an ADHD diagnosis. This lack of clarity and consistency in reporting sample characteristics made group demographic information difficult to ascertain and compare to other studies if not explicitly stated at each timepoint.
Data Collection Methods
Self-report methods were frequently utilized for mental health outcomes, with either the participants completing measures, or their caregivers' completing measures if the diagnosis was made at an earlier stage of a longitudinal study (i.e., when they were children). Although diagnostic interviews from a trained psychologist were also common, often used to formally diagnose ADHD and to measure specific mental health conditions such as clinical depression and other mental illnesses, it was also common for the diagnosis of ADHD and SLD to be self-reported, rather than confirmed through formal diagnostic methods.
Regarding mental health outcomes, most studies utilized common, validated measures of specific mental health conditions or concerns, such as depression (e.g., Beck Depression Inventory), anxiety (e.g., Beck Anxiety Inventory II, Generalized Anxiety Disorder Scale), suicide thoughts and behaviours (e.g., Barkley Suicide Questionnaire), self-harm (e.g., Self-Injury Questionnaire, Nonsuicidal Self-Inquiry Scale), substance use or misuse (e.g., Substance Use Questionnaire), and impairment (e.g., The Impairment Rating Scale). Although most studies focused on negative outcomes, some positive variables were also explored, such as overall health (e.g., Patient Health Questionnaire), wellbeing (e.g., Psychological Well Being Scale (PWB), Extended Satisfaction with Life Scale), social support (e.g., Multidimensional Scale of Perceived Social Support), self-efficacy (e.g., Self-Efficacy Scale, Self-Advocacy Scale), and self-esteem (Rosenberg Self-Esteem Questionnaire).
Mental Health Outcomes
Through this scoping review, we aimed to better understand the mental health outcomes of young adults with ADHD and/or SLDs as they transition to adulthood whether they attend postsecondary institutions or pursue an alternate pathway.
Contributors to Positive Mental Health Outcomes
Considering the first research question regarding what contributes to positive mental health outcomes (e.g., wellbeing, flourishing, positive coping, etc.) for emerging adults with ADHD and/or SLD, few studies explicitly examined positive outcomes. The few studies that examined wellbeing or positive aspects of mental health frequently found that young adults with ADHD had lower wellbeing and adjustment (e.g., Buchanan, 2011; Strand, 2016; Weyandt et al., 2013) or quality of life (Pinho et al., 2019) than controls, but some did not find any significant differences (e.g., Wilmhurst et al., 2011). Interventions, such as coaching and mindfulness training often reduced these negative outcomes (e.g., Fields et al., 2013; Lester & Murrell, 2019), but this was not universal (e.g., Glickman, 2014).
Due to the small number of studies examining the mental health of young adults with SLDs as they transitioned to adulthood, there were few trends. Three studies examined the role of social support. One study found greater support from family than friends, but perceived social support did not correlate with positive self-concept (Hellstrom-Kinder, 2013), and the other two studies found that increased perceptions of social support was related to higher life satisfaction (Smith, 2017; Stack-Cutler et al., 2015). Having comorbid disorders resulted in lower levels of social support and life satisfaction (Stack-Cutler et al., 2015). Using coping strategies (Vaccaro et al., 2019) and perceived parental support (Rosetti, 2014) were protective factors in transitioning effectively to postsecondary institutions, but there was little attention to young adults who choose other pathways during their transition to adulthood (e.g., entering the workforce, apprenticeships, military, etc.).
More of the studies examining ADHD and SLD focused on positive mental health outcomes; one study that used a coaching intervention found improved self-determination, self-esteem, goal setting, and persistence (Richman, 2014). Two qualitative studies focused on students’ perceptions of resilience (Vaccaro et al., 2019) and coping (Zweig, 2012) during this time. Finally, one quantitative study found that increased self-advocacy and parent support was correlated with psychological wellbeing (Rosetti, 201). Overall, research examining positive mental health outcomes did not indicate what contributed to those outcomes. However, there was some evidence that interventions, internal attributes (e.g., self-advocacy), and social support (e.g., parents) contributed.
Contributors to Negative Mental Health Outcomes
For the second research question, more studies examined the negative mental health outcomes of emerging adults with SLD and/or ADHD. Emerging adults with ADHD had increased negative outcomes including depression (e.g., Babinski et al., 2011, 2020), anxiety (Hinshaw et al., 2012), test anxiety (e.g., Dan & Raz, 2015), suicidality (e.g., Eddy et al., 2020), intimate partner violence (e.g., Wymbs et al., 2012, 2017), and substance abuse disorders and smoking (e.g., Elkins et al., 2020).
As there were also few studies examining the mental health of young adults with SLD alone, or combined with ADHD, as they transitioned to adulthood, there are also few themes from these studies. Having an SLD led to higher numbers of suicide attempts (Fuller-Thompson et al., 2018), depression and anxiety (e.g., MacInnes & Broman, 2013), and stress (Smith, 2017). However, one study found that having both dyslexia and ADHD during the transition to college did not result in increased depression and anxiety symptoms compared to students without either diagnosis (Nelson & Gregg, 2012). Another study found that females with ADHD and reading disabilities had worse outcomes in school and social functioning; those with only a reading disability had more internalizing symptoms and self-harm; and those with math disability alone had poorer social functioning (Rinsky, 2012).
Across the diagnoses, comorbidity was a risk factor for poorer outcomes. There was a focus on ADHD and/or SLD as a contributing factor for negative mental health outcomes, with little attention to what other factors contribute to these poor outcomes. One study found that in females with ADHD, deficits in executive functioning, specifically response inhibition, predicted self-harm and suicide attempts (Miller et al., 2012). Those who used cannabis had elevated risk for psychotic symptoms (Vitiello et al., 2017). Young adults with dyslexia found that the coping with postsecondary demands contributed to increased stress (Smith, 2017).
Differential Mental Health Outcomes
For the third research question examining differential mental health outcomes for different groups of emerging adults with SLD and/or ADHD, there was little attention to differential outcomes for groups. As noted in the study characteristics section, few studies provided enough information about race, ethnicity, sex, or gender to gain insight into differences between groups. Protective factors examined included supports that reduced negative mental health outcomes or increased positive mental health outcomes (e.g., Reed et al., 2011; Zwieg, 2012).
One study examined experiences of young parents who had ADHD, reporting that they felt more overwhelmed, less close to their children, and less happy as parents (Kroeger, 2018), speaking to some experiences of emerging adults with ADHD beyond those in postsecondary education. However, many of these studies related to emerging adults with ADHD and/or SLD were conducted using students attending postsecondary institutions (n = 34), and most studies using community samples did not indicate education levels. This hinders our understanding of outcomes, as students with ADHD are twice as likely to drop out of high school (Breselau et al., 2011). They are also less likely to go onto postsecondary education, and when they do, they are likely to go to vocational schools rather than four-year colleges (Kuriyan et al., 2013). Consequently, these results do not likely represent the experiences of individuals with ADHD. Similarly, most of the SLD and ADHD/SLD research focused on postsecondary school settings, making it difficult to determine the positive and negative mental health outcomes of those who do not continue their education but take another path during emerging adulthood.
Discussion
In this research, having ADHD was related to less positive mental health outcomes such as quality of life (e.g., Pinho et al., 2019), but protective factors, such as social support (e.g., Smith, 2017) or coping skills (e.g., Vaccaro et al., 2019), was related to better outcomes. Additionally, when studies used interventions to support students, the interventions generally improved outcomes (e.g., Fields et al., 2013) but not always (e.g., Glickman, 2014). There was a greater focus on positive mental health outcomes in the studies examining those with ADHD and SLD, using qualitative research methods to explore their resilience and coping skills. Much of the research examining positive mental health outcomes did not provide clear indications of what contributed to those outcomes. However, there was some evidence of interventions, internal attributes (e.g., self-advocacy), and social support (e.g., parents) contributing to positive mental health outcomes.
Having ADHD and/or SLD was also associated with more negative mental health outcomes, such as increased mental illness symptomatology and decreased functioning. Some studies found increased negative outcomes (e.g., anxiety, depression, suicidality) without focusing on what contributed to those outcomes (ADHD: e.g., Hinshaw et al., 2012; SLD: e.g., MacInnes & Broman, 2013; ADHD and SLD: e.g., Nelson & Gregg, 2012). Others found that comorbidity (e.g., Biederman et al., 2014), conduct problems (e.g., Wymbs), cannabis use (Vitiello et al., 2017), or stress of postsecondary demands (Smith, 2017) were risk factors for negative outcomes.
Although the central focus of this study was on mental health outcomes for those with ADHD and/or SLD, arguably, the most important takeaways from this study focus on the current state of this literature and the opportunity that exists to grow this knowledge base and the future research that will occupy this space. One opportunity is expanding the literature, particularly for SLD and comorbid SLD/ADHD. Our search results netted a majority of articles (78%) focusing on ADHD, with only 12% and 10% focusing on those with SLD and comorbid SLD and ADHD, respectively. This distribution contrasts to the prevalence of ADHD and SLD. This speaks to a larger issue of which disorders receive research attention. Bishop (2010) found that although dyslexia and ADHD have a similar prevalence and symptom severity, there are about four times more publications on ADHD than on dyslexia, and disorders with more publications also had high levels of funding. Considering that rates of SLD are even higher when writing and math disorders are included, the limited attention to the mental health outcomes of these individuals as they transition to adulthood is concerning.
A second opportunity for future research is to increase focus on positive mental health, as opposed to focusing solely on mental illnesses and symptomatology. As indicated earlier, mental health is not about mental illnesses, but rather, is about realizing one’s potential individually and within the community (WHO, 2022). Operationalized empirically, Keyes (2002, 2007) conceptualized mental health as psychological wellbeing (e.g., autonomy, mastery, growth), emotional wellbeing (e.g., positive affect), and social wellbeing (e.g., social integration, social acceptance) rather than by experiences of mental illnesses or its symptomology. In the current review, only a small portion of the included studies focused on mental health as defined by Keyes, with a majority of studies examining the impact of ADHD and SLD on mental illness symptomology (e.g., anxiety and depression). Although the topic of the latter studies is important, an increased focus on mental health—psychological, emotional, and social wellbeing—would benefit this research area as a whole. e.g., Keyes et al. (2012) have demonstrated the utility of mental health (i.e., differences across languishing, moderate, flourishing) in predicting outcomes such as suicide and academic impairment beyond the presence or absence of a mental illness in a large sample of postsecondary students. Although the studies in this review often demonstrated the negative outcomes and difficulties emerging adults with ADHD and SLD face, Keyes and colleagues’ (2012) study highlights the necessity of also exploring how these populations can flourish.
Research Opportunities Related to ADHD and SLD Subtypes
Beyond a more targeted focus on mental health outcomes, and in addition to mental illness outcomes, there are clear opportunities to examine the role of ADHD and SLD subtypes in relation to mental health and mental illness outcomes. For example, in one of the reviewed studies, Hinshaw et al. (2012) found that participants with ADHD-C had higher rates of suicide attempts and self-injury than those with ADHD-I. Differential findings across ADHD subtypes, such as this example, suggests that researchers should identify subtypes in their study design to examine this factor. Examining those with ADHD as if they were a homogeneous group may hide useful information that could more efficiently direct specific resources to those who need it. Given the low rate of reviewed ADHD studies including subtype in their study design, this is one obvious direction for future researchers.
In a similar vein, reviewed SLD studies did not differentiate across types of SLD. These findings suggest it may be beneficial for researchers to disaggregate the SLD category to generate more specific and relevant information for those with different types of SLDs. For example, Aro and colleagues (2019) found that individuals with a math disability had higher rates of antidepressant use than those with reading disabilities. Similarly, it may also be advantageous for researchers to focus on specific SLDs, as did two articles that focused on reading/dyslexia included in this review. However, Pham and Riviere (2015) cautioned that, because approximately 80% of SLDs are reading related, there has been a focus on reading disabilities, which has limited our understanding of students with SLDs in math or writing. Future research should then be mindful to explore all types of SLDs as opposed to focusing on just reading-related SLDs.
Another concern that arose from the current review was a lack of uniformity with the diagnostic criteria used for study inclusion across the reviewed studies. In other words, inclusion criteria included diagnostic interviews with participants (e.g., Loya, 2011), diagnostic interviews in conjunction with caregiver reports (e.g., Breyer et al., 2014), self-reported diagnosis (e.g., Anastopoulos et al., 2021), or a combination of these across the reviewed studies. Consequently, the samples across studies are likely not directly comparable. Increasing consistency across inclusion criteria would improve the ability to compare findings across studies. Using a more stringent criteria, however, may have unintended consequences for reducing participation from diverse groups. e.g., a formal diagnosis of ADHD and/or SLD requires substantial financial resources to acquire from a licenced clinician. Requiring proof of a formal diagnosis may limit those who are able to participate in research studies, particularly economically-disadvantaged groups, highlighting the complexity and sometimes competing demands of rigour and inclusivity in research.
Research Opportunities Related to Participant Demographics and Sample Characteristics
One consistent observation the results pointed towards the lack of consistency in obtaining and reporting sample demographics (e.g., age, gender, and ethnicity), often manifesting as missing information, particularly in longitudinal studies. In the future, researchers conducting longitudinal studies should report age (and other demographics) for each wave of data collection. Similarly, researchers should consider reporting age-related demographics as opposed to referring readers to other places to obtain that information (e.g., other articles). These practices could allow for not only a better understanding of the sample itself but also allow researchers to make more informed comparisons across samples or intervention developers/implementers to understand boundary conditions for efficacy.
A related recommendation concerns biological sex and/or gender identity. In this case, researchers should define the term they are using, as opposed to using them interchangeably or without defining them. Doing so will allow readers to understand that (biological) sex, for example, is relevant for understanding sex-related brain differences in these populations. Similarly, as both ADHD and SLD have developmental components, it is important for researchers to report sample mean age and age range (at the very minimum), so readers have a clear understanding of the sample and how age informs the results and interpretation. The results also support researchers reporting ethnicity and race more consistently. As with age and gender/sex, many of the same points apply for collecting and detailing this information more thoroughly. In addition, understanding the ethnic makeup of the sample allows readers to understand the generalizability of the findings, particularly when many of the reviewed samples contained a majority of White participants. Consequently, researchers should continue to utilize more diverse samples to increase generalizability through more specific recruitment strategies to access populations often underrepresented in research. More importantly, using representative samples also allows researchers to better understand the experience of diverse groups, particularly those from structurally marginalized or equity deserving groups. The intersection of being in an equity deserving group and having ADHD and/or SLD will be undoubtedly different than someone without this intersection. A more comprehensive understanding of the experiences of individuals with these intersections will allow for the development of better supportive interventions or resources, for example.
A final recommendation for future research regarding sample characteristics is to expand beyond postsecondary students, as majority of the reviewed research utilized, exclusively or partially, postsecondary students. Having a majority of studies drawing from postsecondary student populations is noteworthy as only a small portion of individuals with ADHD (8% [Hechtman et al., 2016] to 30% [Kuriyan et al., 2013]) and SLD (15.5% [Sanford et al., 2011] to 21% [Cortiella & Horowitz, 2014]) attend postsecondary institutions. This focus on postsecondary students may be due to the impact of these two diagnoses has on academic success and the postsecondary experience. Although this connection is clear, a focus on postsecondary students and the postsecondary context may overshadow the impact that these two diagnoses have on daily life and experiences beyond the domain of academics (e.g., the workplace, relationships).
Conclusion
The original intent of this scoping review was to examine the research on the mental health of emerging adults with ADHD and/or SLD. Although this intent was fulfilled, few studies examined what contributes to positive mental health, limiting the conclusion that could be made and indicating the need for more future research in this realm. That said, this scoping study was fruitful, nonetheless, as important recommendations were generated through this an examination of the current state of research for this topic. For this area of research to advance, a more concerted effort is required to understand the nuanced mental health of emerging adults with ADHD and/or SLD. The benefits of the suggestions provided will not only be a better appreciation of the lived experiences of these emerging adults but also knowledge that can support ways to improve their mental health, leading to flourishing.
Supplemental Material
Supplemental Material - Mental Health in Emerging Adults With ADHD and/or Specific Learning Disabilities: A Scoping Review
Supplemental Material for Mental Health in Emerging Adults With ADHD and/or Specific Learning Disabilities: A Scoping Review by Gabrielle Wilcox, Arianna M. Gibson, Brittany L. Lindsay, Sonal Prasad, and Andrew C. H. Szeto in Emerging Adulthood
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.