
Abstract
Perfectionism, academic stress, worry, and rumination are associated with increased levels of anxiety and depressive symptoms in university students. However, associations between these variables have been explored separately. Using PLS-SEM, the present study explored a multivariate model in which these variables interplay to predict affective symptoms. A sample of 403 students between ages 18 and 29 years from 55 Colombian institutions of higher education participated by completing Zung depression and anxiety scales, the Multidimensional Perfectionism Scale, the Inventory of Academic Stress, the Penn State Worry Questionnaire, and the Ruminative Responses Scale. Results indicate a positive relationship between perfectionism and academic stress, and a mediation effect of worry and rumination in the relationship between academic stress and anxiety and depressive symptoms. Findings provide evidence of a novel model that precedes the design of target prevention and intervention programs pointing to reduce the risk of affective disorders and its associated negative consequences.
Introduction
Several studies involving university students report high prevalence of anxiety and depressive symptoms worldwide (Husky et al., 2020; Ibrahim et al., 2013; Islam et al., 2020). Few of these studies involve samples from Latin America (Figuera et al., 2011; Mayer et al., 2016), where anxiety and depression rates in the general population represent a major problem. A survey from the World Health Organization [WHO] established that more than 300 million people worldwide present depression, causing 8% of youth morbidity and disability rates (Auerbach et al., 2018). Also, the WHO (2021) indicated that almost 5% of students between ages 15- and 19-years old meet criteria for anxiety disorders, leading to social isolation and negative effects in their daily life functioning. Also, reports from Latin America and the Caribbean indicate that depressive disorders are the second cause of disability in women and the forth cause in men between ages 20 and 24 years (PAHO, 2018).
In Colombia, in the last National Survey of Mental Health (Ministerio de Salud, 2015) it was reported a prevalence of affective disorders in 6.7% of Colombian adults, specifying that depression is the first cause of suicide in young adults. Studies involving nonclinical samples of Colombian university students using self-reported measures found prevalence rates for depression and anxiety between 25 and 50% (Vélez et al., 2008; Caro et al., 2019; Vinaccia & Ortega, 2020) or even higher (Monterrosa-Castro et al., 2020). Accordingly, one of the main reasons for university students to attend health services is experiencing depressive and anxiety symptoms (Gallagher, 2014). A study with this population showed that between the years 2007 and 2017 diagnoses of depression and suicide increased from 43 to 56% (Lipson et al., 2019). These findings together with the context of the COVID-19 pandemic and its associated dynamics (e.g., isolation, virtual learning, health problems; WHO, 2020) and postpandemic informed consequences represents a high-risk scenario for increased levels of affective problems in this population (Son et al., 2020).
Depressive and anxiety symptoms in university students significantly affect their quality of life and their ability to adjust and cope with new situations and context demands (Olatunji et al., 2007; Othman et al., 2019). These symptoms may also lead to broader negative outcomes such as poor social development, isolation, drug use, self-injury (American College Health Association, 2016; Caro et al., 2019), suicidal ideation and suicide (Tabares et al., 2019). The identification of these negative effects has raised the interest from different fields of psychology and associated sciences to examine the variables that contribute to the emergence and maintenance of mood disorders in university students worldwide to identify early preventive programs and interventions to reduce the associated risks (Auerbach et al., 2018).
Affective problems in university students involve the manifestation of physiological, behavioral, and cognitive responses that cause discomfort and affect persons’ functioning at distinct levels (Othman et al., 2019). The Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM–5; American Psychiatric Association, 2013) states that the main symptom of depression is low mood, disguised by irritability. Anxiety includes physiological symptoms such as constant fatigue, chest pain or pressure, increased heart rate, muscle tension, weakness, trembling, agitation, sleep difficulties, among other symptoms (APA, 2013). Also, anxiety involves cognitive responses such as fear for other’s negative evaluation and losing mental sanity, leading to poor concentration and reduced memory (Chand et al., 2020).
Previous evidence points out that some university students set ambitious standards and expectations, strongly value and strive for excellence and avoid criticism, which can be associated with the presence of perfectionist traits (Mateus et al., 2021; Craddock et al., 2009). Perfectionism can be classified as adaptive or maladaptive (Rice & Ashby, 2007): the adaptive component of perfectionism is characterized by a high perception of self-efficacy and satisfaction with one’s performance. By contrast, maladaptive perfectionism informs discrepancies between the person’s standards and his or her performance, along with self-criticism, fear of being evaluated, excessive concern for mistakes and negative emotional states (Besser et al., 2004). Frost and colleagues (1990) stated that perfectionism constitutes a personality trait composed by six dimensions: (1) personal standards, defined as the tendency of the person to seek excessively high goals and high standards of self-evaluation; (2) concern over mistakes, indicating a tendency to interpret errors as failures; (3) doubts about actions, reflecting low satisfaction; (4) parental expectations, that reflect perceived high standards; (5) parental excessive criticism; and (6) high interest in organization, referring to the preference for cleanliness and order. Some of these dimensions have been linked to the presence of anxiety and depressive symptoms (Cox et al., 2009; Harris et al., 2008; O'Connor et al., 2010; Raspopovic, 2015; Shafran & Mansell, 2001).
University students who exhibit perfectionist traits are at a higher risk of experiencing academic stress due to personal high academic standards (Kim et al., 2017). Academic stress is described as a socio-environmental factor (Reddy et al., 2018) linked to the demands that the educational context imply for university students such as time management, academic requirements, evaluation pressures, financial management, required studying hours, among others (Sharp & Theiler, 2018). According to Barraza Macías, 2006, academic stress leads to the activation of three negative responses: cognitive assessment of academic demand, physiological responses, and the deployment of coping strategies. Accordingly, the first hypothesis of this study is that perfectionism will be positively and significantly associated with academic stress in the sample.
Moreover, Saravanan and Wilks (2014) found that academic stressors generate frustration as well as the perception of excessive pressure contributing to the emergence of anxiety symptoms. Similarly, Nonterah et al. (2015) indicated that academic stress is linked to frequently perceiving a negative evaluation from others increasing the risk for depressive symptoms in university students. Thereby, hypotheses 2 and 3 of this study state that academic stress will be positively associated with increased anxiety and depressive symptoms. As evidence indicates that perfectionism contribute to increased levels of academic stress, and academic stress may lead to increased anxiety and depressive symptoms, we proposed that perceived academic stressors will mediate the association between perfectionism and anxiety (hypothesis 4a), and between perfectionism and depressive symptoms (hypothesis 4b).
In addition to academic stress increasing university students’ risk for anxiety and depressive symptoms, it has been found that personal factors such as worry and rumination may also increase this risk. In the one hand, worry is defined as a response of cognitive avoidance to internal and external perceived threats. Avoidance is used to suppress emotional discomfort, but instead, it increases and maintains negative emotionality (Borkovec et al., 2004). In this regard, evidence is contradictory with some studies pointing out the association between worry and anxiety and depressive symptoms (Erickson et al., 2020; Skodzik et al., 2016), and other studies indicating no significant associations between these variables (Pimentel & Cova, 2011). Contradictory findings suggest that not all persons exhibiting worry are anxious or depressed. On the other hand, evidence supports that rumination is linked to higher levels of depressive and anxiety symptoms (Drost et al., 2014; McEvoy et al., 2013; McLaughlin & Nolen-Hoeksema, 2011; Pimentel & Cova, 2011; Wahl et al., 2019; Yilmaz, 2015). Rumination is described as uncontrollable and intrusive patterns focused on negative information (Watkins, 2008). However, it is worth noticing that not all persons who exhibit rumination present affective disorders (Alsaleh et al., 2016; Calmes & Roberts, 2007), but they are at higher risk for.
No studies exploring the mediating role of worry or rumination in the described association between academic stress and affective symptoms in university students were found. However, Lynn-Flynn et al. (2011) indicate that stressful contexts may evoke dysfunctional responses such as rumination, which in turn leads to emotional symptomatology. Similarly, Siddique et al. (2006) described that a person’s tendency to concern about future negative outcomes (worry) increases in contexts that are perceived as highly stressful, such as the academic setting. In this line, we propose that both rumination and worry may constitute a personal factor mediating the proposed association between academic stress and anxiety (hypothesis 5a and 6a) and depression (hypothesis 5b and 6b) will mediate the association between academic stress and anxiety.
In the present study, we propose that both contextual (academic stress) and personal variables (perfectionism, worry and rumination) contributes to explain the presence of self-reported anxiety and depressive symptoms in Colombian university students. The contribution of these variables has been previously studied separately. Using PLS-SEM, the objective of the present study is to explore a more complex model in which these variables interplay and behave as direct predictors and as mediating variables to predict university students anxiety and depressive symptoms (Figure 1). Hypothesized model: relationship between perfectionism and academic stress, possible effects of academic stress on affective symptoms and the mediation effect of rumination and worry in this association.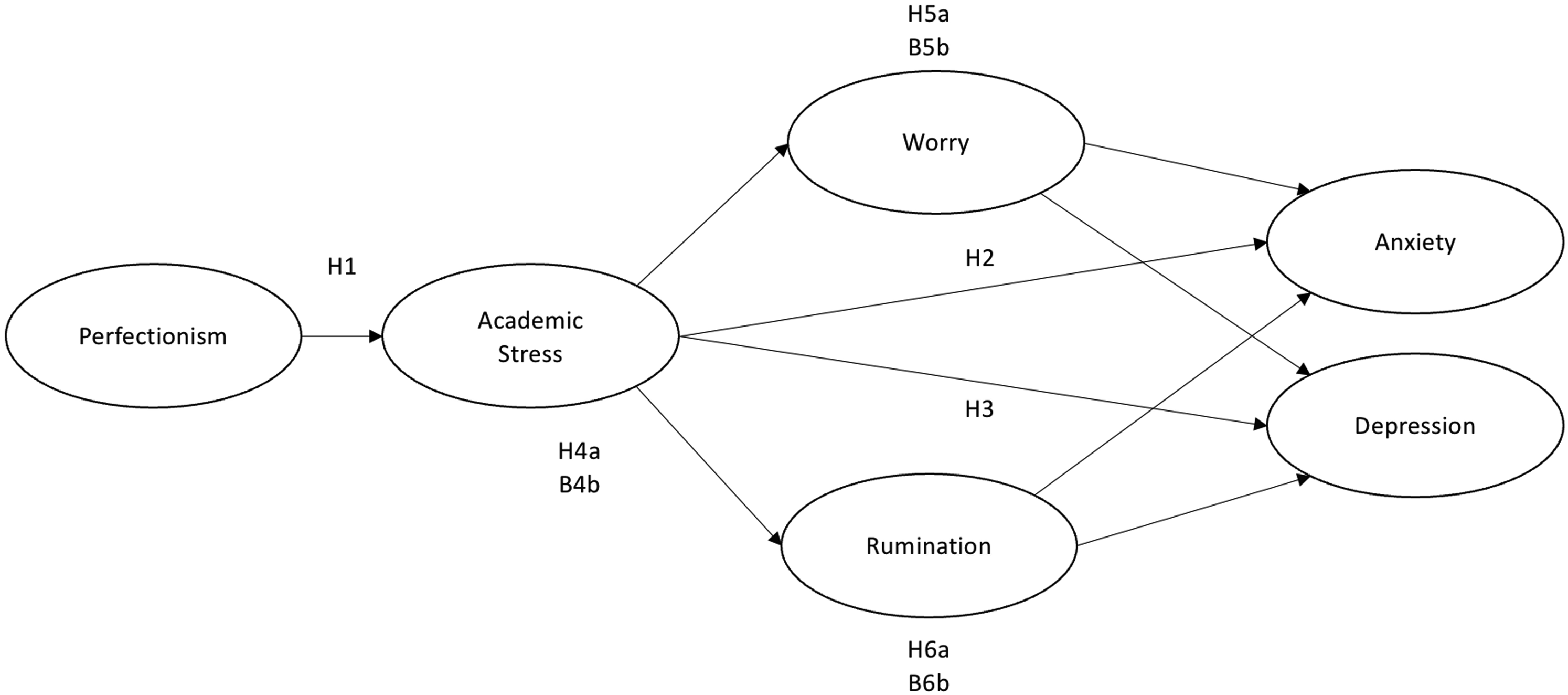
Method
Participants
The present study included 403 undergraduate university students aged between 18 and 29 years (M = 20.6; SD = 2.42; 61% women), 61% females. The sample was recruited by quota sampling where general population of university students were invited to participate through the publication of eye-catching advertisements and informative videos in social networks including Facebook, LinkedIn and Instagram, in groups where university students frequently participate (e.g., sports groups, scholarships awarded groups by the State and four music groups). The sample size was calculated a priori using G*Power 3.1.9.2 software (Lakens et al., 2018) by using one tailed test with an expected effect size of .05 and statistical power of .95 with four predictors in the model. The calculator indicated that the minimum sample size to obtain an adequate power was 218 participants.
Inclusion criteria included being an adult and belonging to an official or private university in Colombia. Exclusion criteria included being a postgraduate student and being 17 years old or younger. Responses from 425 participants were obtained, of which 22 were excluded: 5 participants were outside Colombia, 5 did not consent their participation, and 12 did not complete all the instruments. Most of the students indicated being classified in low-income socioeconomic status (75%), being single (94%), without children (96%), studying during the daytime (94%) and belonging to private universities (92%). The variable termed “previous diagnosis” aimed to identify whether the students had been diagnosed psychologically or psychiatrically in the last 6 months, to which 16% of the participants answered affirmatively.
The mean score for anxiety symptoms in this sample was 46.26 (SD = .9.97, range 26–76) being scores between 20 to 44 normal, 45 to 59 mild, 60 to 74 moderate and >75 severe. For depressive symptoms the mean was 46.82 (SD = 10.90, range 24–76) in which scores <50 are classified as normal, 50 to 59 mild, 60 to 69 moderated, and >70 severe. The mean score for rumination was 12.48 (SD = 3.33, range 6–20) being 20 the highest score indicating increased levels of negative rumination. For worry, the sample mean was 34.30 (SD = 10.57, range 11–55) in which scores <32 indicate low levels, 33 to 37 moderate levels and >38 chronic levels. Academic stress scale mean was 59.73 (SD = 15.66, range 4–96) being 0 to 48 low, 49 to 60 medium, and 61 to 100 high. For perfectionism, the mean was 85.57 (SD = 23, range 4–96) being 145 the higher possible score indicating increased perfectionism.
Instruments
Zung Depression Scale (EZ-D; Zung, 1986)
The Zung scale assesses the presence of affective, physiological, and psychological responses associated with depression and is used for diagnostic and screening purposes. The scale compresses 20 items scored on a 4-point scale (1 = not at all or few times to 4 = most of the time): 10 of them affirming the presence of depressive symptoms (e.g., “I feel down-hearted and blue,” “I have crying spells or feel like it,” and “I am more irritable than usual”), and 10 items indicating its absence (e.g., “Morning is when I feel the best,” “I am hopeful about the future”) which were reversed to calculate the total score (2, 5, 6, 11, 12, 14, 16, 17, 18, 20). Higher scores represent increased levels of depressive symptoms. A previous validation of this scale with Colombian participants showed an acceptable internal consistency of .55 (Lezama & Meneses, 2012). However, for the present sample, the scale obtained good internal consistency (α = .87).
Zung Anxiety Scale (EZ-A; Zung, 1971)
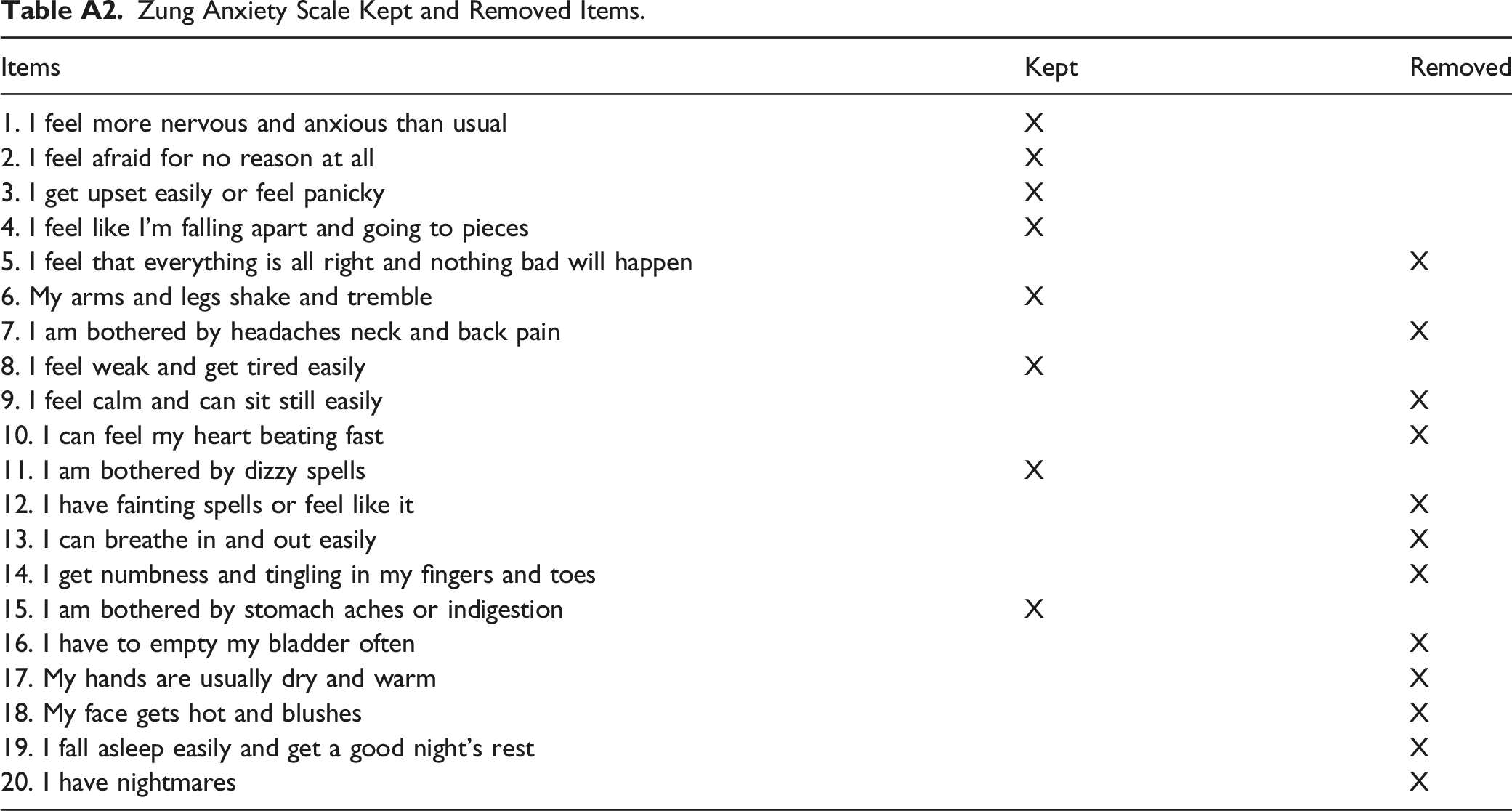
This scale evaluates anxiety symptoms during the last 30 days through 20 items: 15 for somatic complaints (e.g., “I feel more nervous and anxious than usual”, “I can feel my heart beating fast”), and 5 for cognitive symptoms (e.g., “I feel like I am falling apart and going to pieces,” “I feel that everything is all right and nothing bad will happen”). Items are answered on a 4-point scale (1 = not at all or few times to 4 = most of the time). According to the author, 5 items exploring the absence of anxiety symptoms (5, 9, 13, 17 and 19; e.g., “I can breath in and out easily,” “My hands are usually dry and warm”) were reversed to calculate the total score, indicating that higher scores represent increased anxiety symptoms. The scale was previously validated with Colombian university students obtaining an internal consistency of .77 (De la Ossa et al., 2009). For the present study, the internal consistency of the instrument was good (α = .86).
Multidimensional Perfectionism Scale (FMPS; Frost et al., 1990)
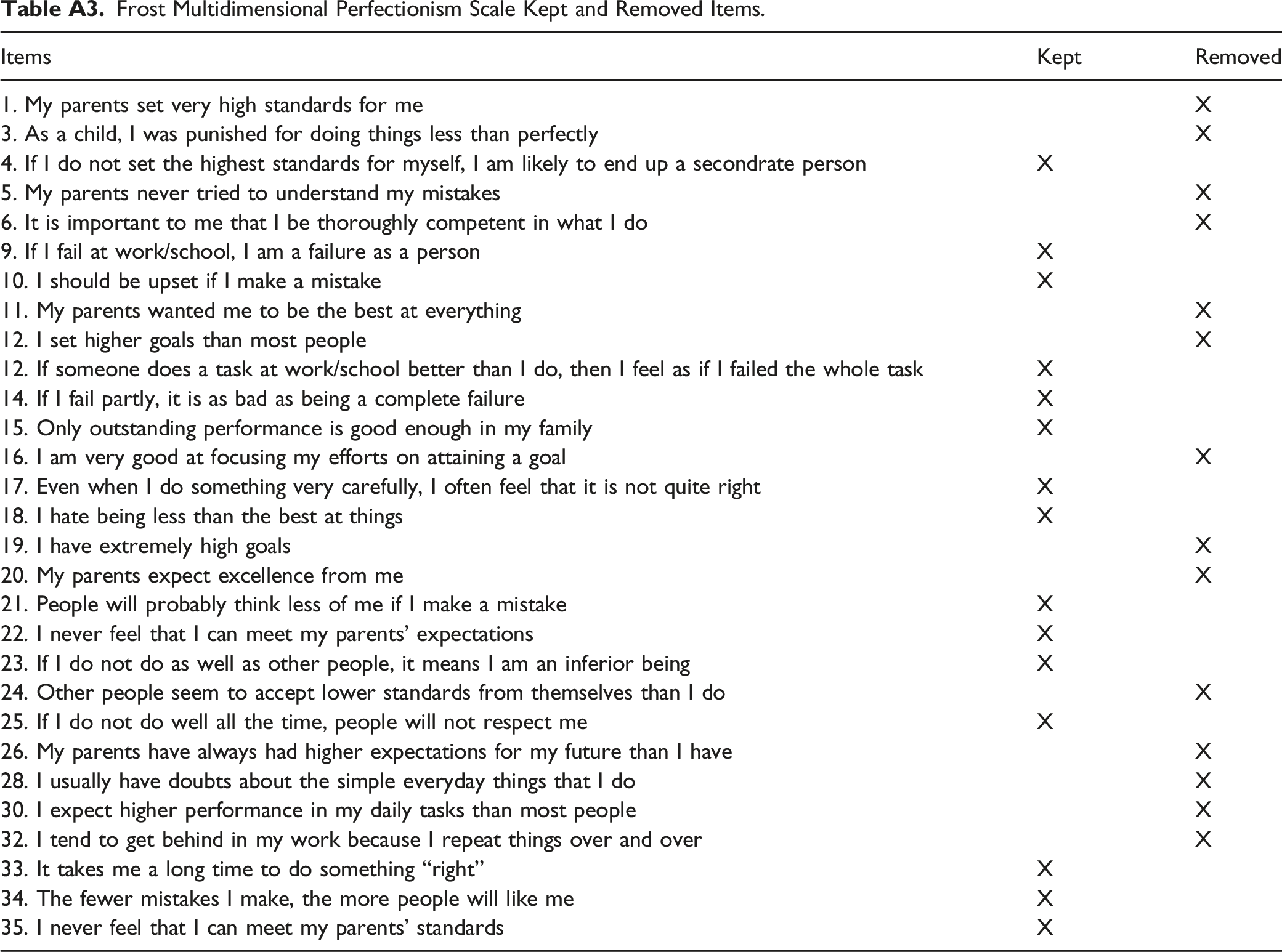
The scale assesses perfectionism from a construct composed of six dimensions through 35 items: (1) personal standards (PS, e.g., “I expect higher performance in my daily tasks than most people”); (2) concern over mistakes (CM, e.g., “I should be upset if I make a mistake”); (3) doubts about actions (DA, e.g., “If I do not as well as other people, it means I am inferior being”); (4) parental expectations (PE, e.g., “My parents set very high standards for me”); (5) parental criticism (PC, e.g., “My parents never tried to understand my mistakes”); and 6) organization (O, e.g., “I am an organized person”). Scale items are scored on a 5-point scale (1 = strongly disagree to 5 = strongly agree). The potential range of FMPS total scores is 29–145. As recommended by Frost et al. (1990), we excluded organization scale when calculating the total score for perfectionism. The validation of this scale was carried out with Mexican participants, each dimension showing appropriate internal consistency (between .76 and .86; Paredes et al., 2010). For the present study, all dimensions and the total scale, composed by the negative dimensions, showed appropriate to good internal consistency (PE = .91, DA = .76, PE = .81, PE = .71, CM = .76, and overall scale = .91).
Inventory of Academic Stress (SISCO-V2; Barraza, 2007)
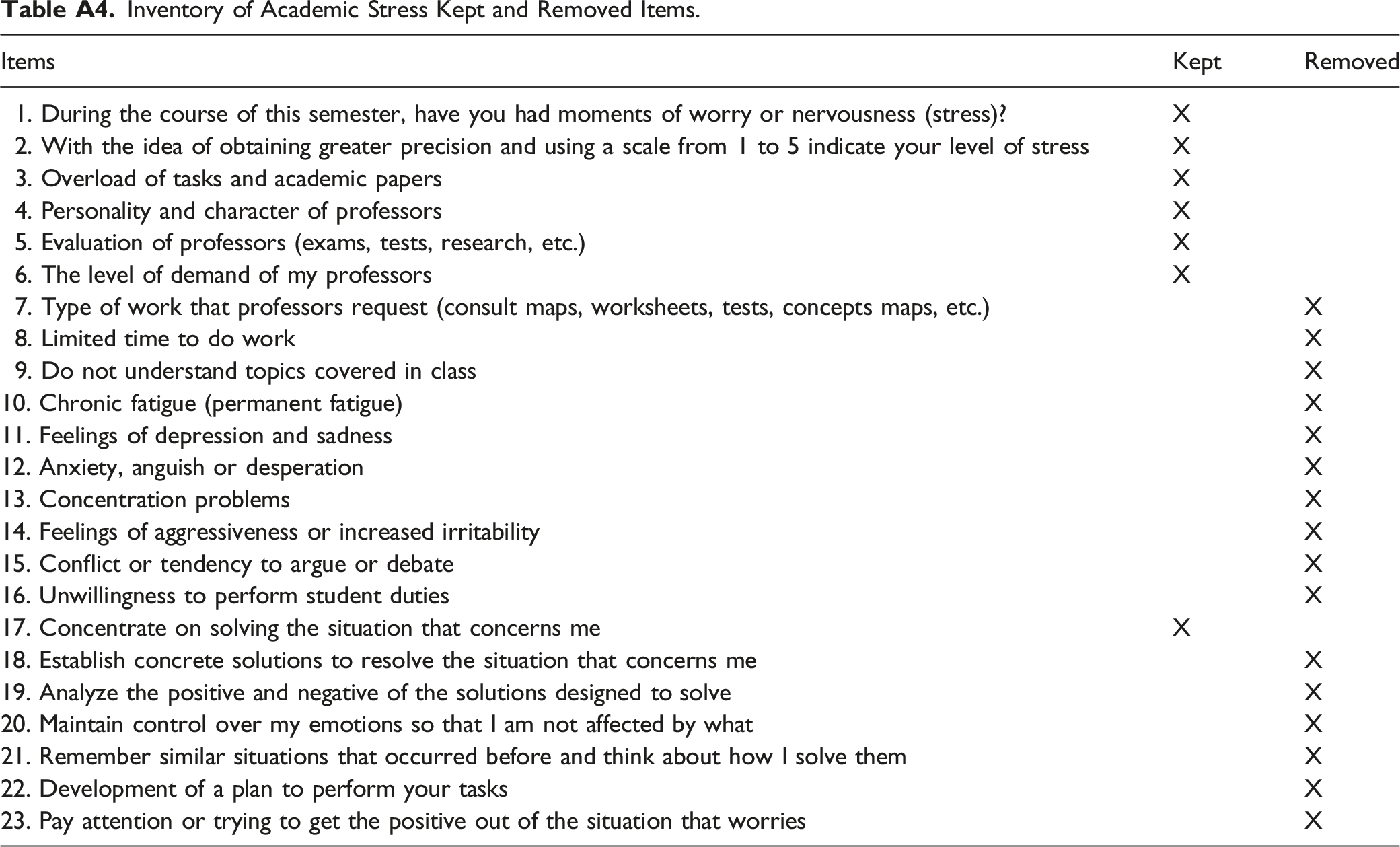
This inventory is composed by 23 items which asses three dimensions of academic stress: stressor stimuli to assess stressful demands from the environment (7 items, e.g., “I feel overloaded by teacher evaluations, essays, homework,” “Limited time to do homework ”), symptoms in terms of responses frequency and intensity (7 items, e.g., “I feel sleep problems,” “I have memory problems”) and coping strategies (7 items, e.g., “I make a plan and take actions,” “I avoid the situation”). Items are responded on a 6-point scale (never = 0 to always = 5) indicating that higher scores represented increased levels of academic stress in the sample. This inventory has been previously validated with Colombian university students with appropriate internal consistency (α = .90) (Salavarrieta et al., 2010), similar to the one obtained for the present study (α = .85).
Penn State Worry Questionnaire (PSWQ; Ruiz et al., 2018)
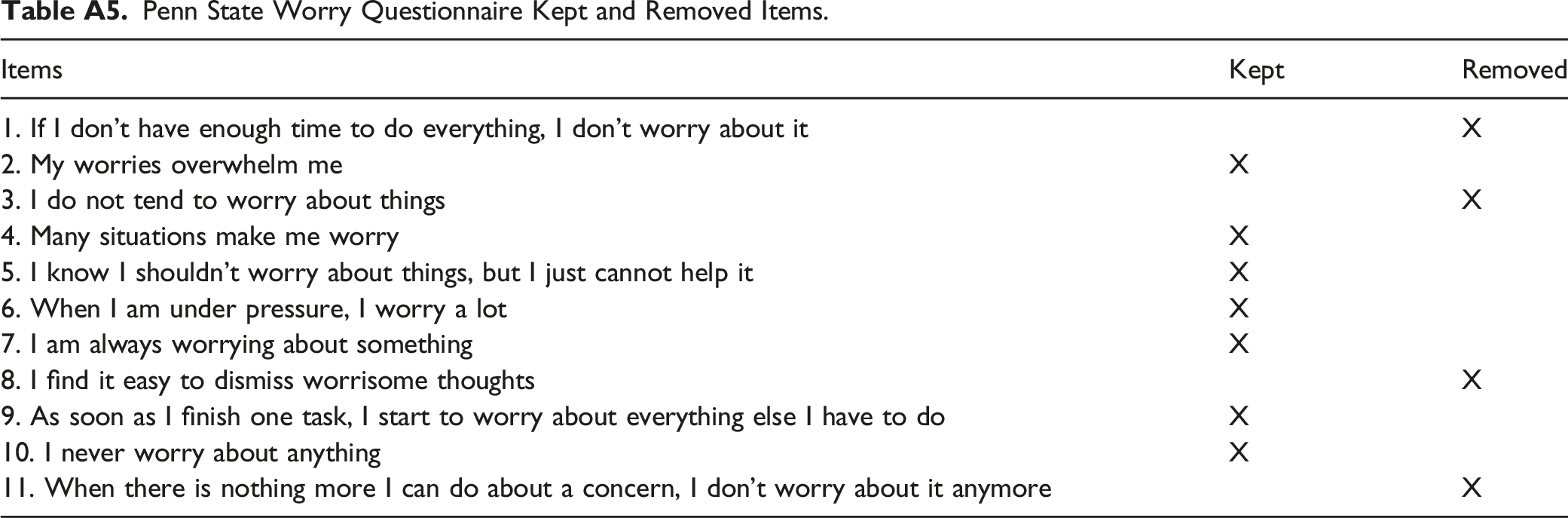
This questionnaire assesses general tendency to worry. The abbreviated version has 11 items (e.g., “many situations make worry,” “when I am under pressure, I worry a lot”) answered in a 5-point Likert scale (1 = not at all typical of me to 5 = very typical of me). Four items must be reversed to calculate the global score (1, 3, 8 and 11) (e.g., “I never worry about anything”). Higher scores on this dimension implied increased levels of worry. This questionnaire was validated by Ruiz et al. (2018) with Colombian participants, with an internal consistency of .95, similar to the one obtained for the present study (α = .91).
Ruminative Responses Scale - Short Form (RRS-SF; Treynor et al., 2003)
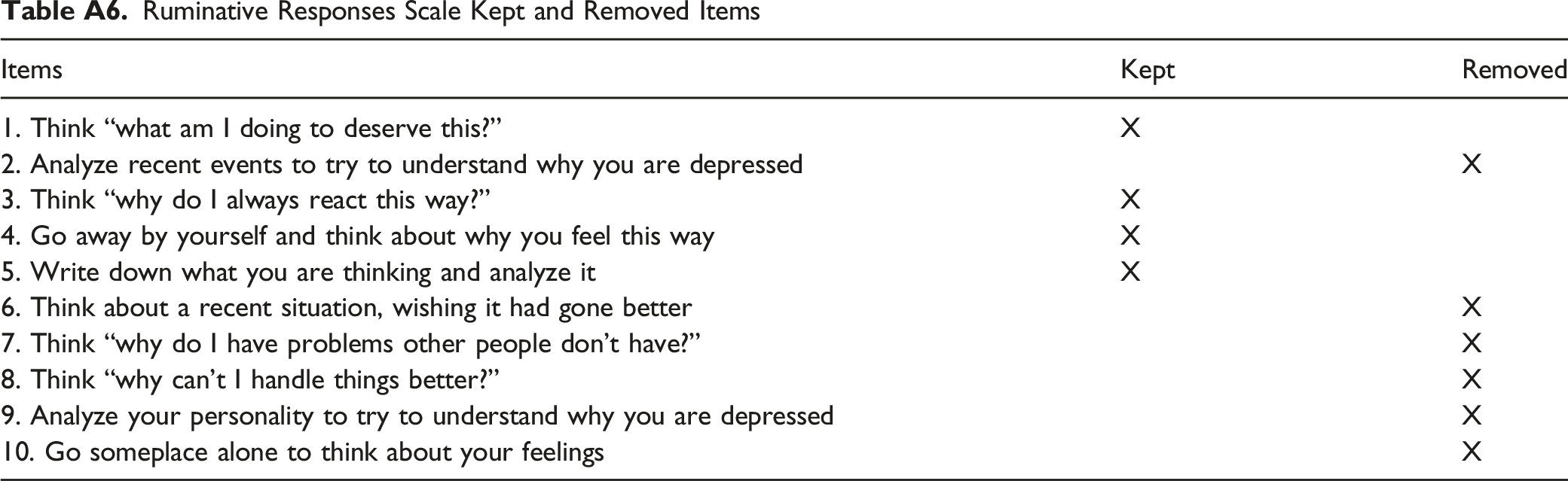
This scale has been used in previous research for the evaluation of ruminative responses in different populations. Rumination is defined as repetitive and passive self-focused thoughts on one’s negative feelings, symptoms of distress, and their causes and consequences regardless of the context that produce them. The short version contains 10 items, with five items evaluating brooding-type rumination (e.g., “think about feeling alone,” “what I am doing to deserve this?”) (Items 1, 3, 6, 7 and 8) and five evaluating reflection described as a positive type or rumination (items 2, 4, 5, 9 and 10). Items are answered in a 4-point scale (1 = almost never to 4 = almost always). For the present study, only the brooding scale was used in the analyses to assess rumination. The brooding sub-scale showed appropriate internal consistency in a previous study involving Colombian participants (α = .79; Ruiz et al., 2017). Similarly, the internal consistency for the present sample in the brooding scale was appropriate (α = .71).
When conducting PLS-SEM analyses, items in each scale were removed and others were kept (see Appendix). Keeping only items with outer loadings greater than 0.60 guarantees that the construct explains more than 50% of the indicator’s variance providing acceptable item reliability and assuming that the factor model is correct and valid.
Procedure
Instruments were digitized using Google Docs platform with prior authorization from the authors. The link to the instruments was shared in social networks for easy access and the participation was completely anonymous. The research was regulated by the ethical norms in Colombia and the American Psychology Association guidelines on human research. To comply with the code of ethics, all the participants signed the informed consent before participating. We did not provide any incentive for participation. At the end of the online application, information on how to obtain advice on mental health problems through a state toll-free phone number was provided.
Data Analysis
PLS-SEM was used to estimate the predictive capability of perfectionism, academic stress, rumination and worry in the presence of affective symptoms in a sample of university students from Colombia. PLS-SEM models involve two elements according to Hair Jr et al. (2016): a measurement model which assesses the association between items and variables (validity and reliability), and a structural model which assesses the predictive capability of the variables proposed in the model. PLS-SEM analyses for the two elements were conducted using SmartPLS 3.3.3 (Ringle & Wende, 2015). Reliability was tested using rho_A coefficient and composite reliability, convergent validity using outer loads and Average Variance Extracted (AVE), and discriminant validity using Heterotrait-Monotrait ratio of correlations method (HTMT) as proposed by Henseler et al. (2015). The structural model included the analysis of the explained variance, the effect size, the predictive effect size and the magnitude and statistical significance of the coefficients for each path proposed in Figure 1.
Results
Measurement Model Statistics
Measurement Model Statistics.
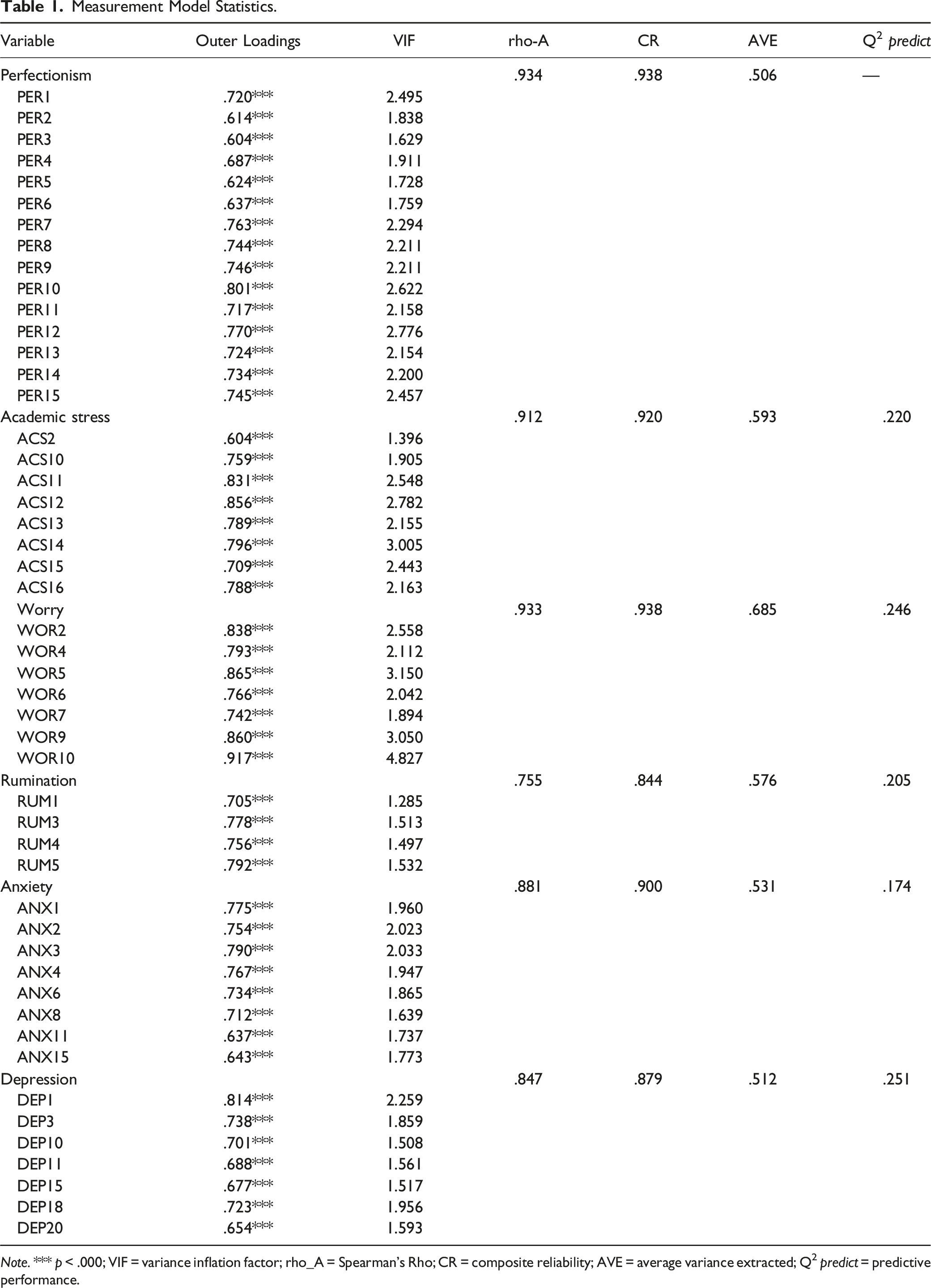
Note. *** p < .000; VIF = variance inflation factor; rho_A = Spearman’s Rho; CR = composite reliability; AVE = average variance extracted; Q2 predict = predictive performance.
Discriminant Validity of the Measurement Model.
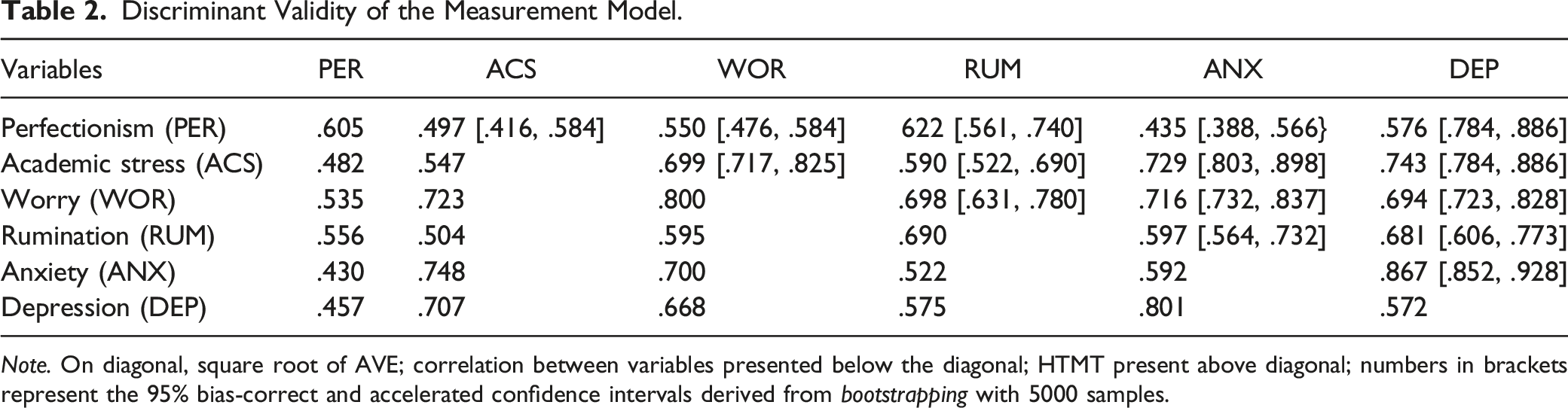
Note. On diagonal, square root of AVE; correlation between variables presented below the diagonal; HTMT present above diagonal; numbers in brackets represent the 95% bias-correct and accelerated confidence intervals derived from bootstrapping with 5000 samples.
Structural Model Statistics
Structural Model Estimates.
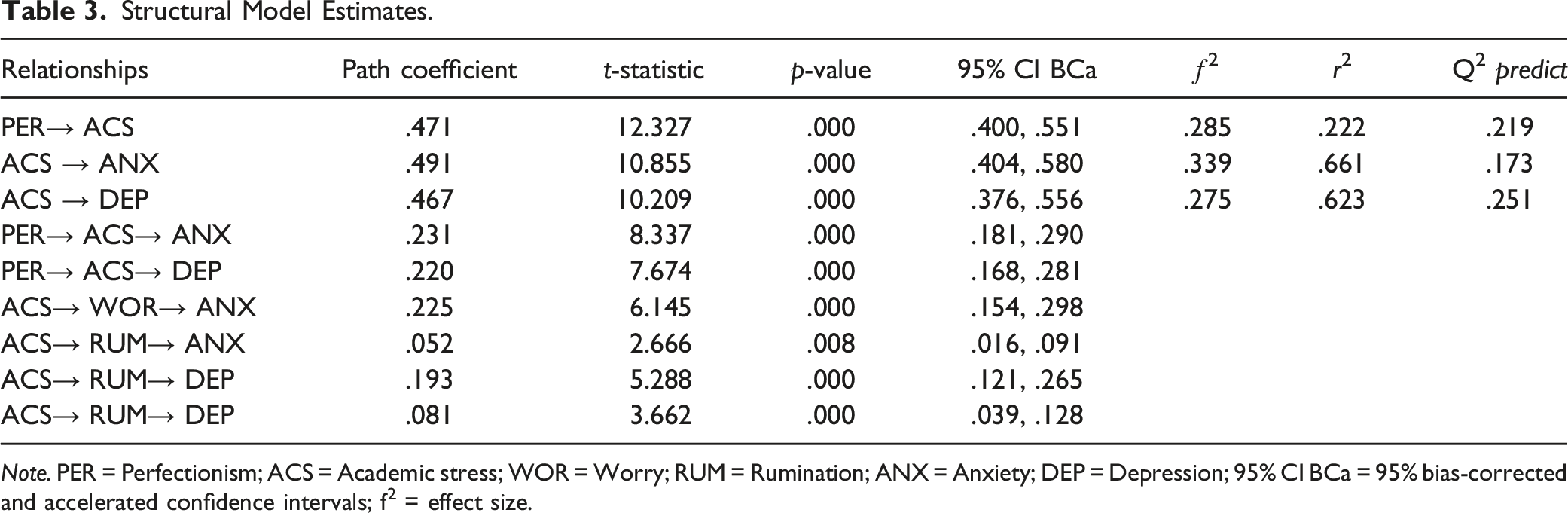
Note. PER = Perfectionism; ACS = Academic stress; WOR = Worry; RUM = Rumination; ANX = Anxiety; DEP = Depression; 95% CI BCa = 95% bias-corrected and accelerated confidence intervals; f2 = effect size.
Results in Table 3, indicates a direct, positive, and significant effect of perfectionism on academic stress (p < .01), explaining 22.2% of its variance. Likewise, positive, and significant associations were found between academic stress and anxiety (t = 10.855; p < .01) and depression (t = 10.209; p < .01). These results support hypotheses H1, H2 and H3 of the present study. The effect size was calculated according to Cohen’s criteria (2013), in which a ƒ2 >.02 is considered weak, ƒ2 >.15 moderate, and ƒ2 >.35 is strong. For the present study, the effect of perfectionism on academic stress was moderate (ƒ2 .285; p < .01), and the effects of academic stress on anxiety (ƒ2 .339; p < .01) and depression (ƒ2 .275; p < .01) were also moderate.
Results regarding mediation hypotheses in this study support an indirect and significant effect of academic stress in the association between perfectionism and anxiety (H4a; t = 8.337; p < 0,01; [.181, .290]), as well as between perfectionism and depression (H4b; t = 7.674; p < 0,01; [.168, .281]). Similarly, results corroborate the mediation effect of worry in the association between academic stress and anxiety (H5a; t = 6.145; p < 0,01; [.154, .298]), and in the association between academic stress and depression (H5b; t = 2.666; p < 0,01; [.016, .091]). The mediation effect of rumination in the association between academic stress and anxiety (H6a; t = 5.288; p < 0,01; [.121, .265]) and in the association between academic stress and depression (H6b; t = 3.662; p < 0,01; [.039, .128]), was also significant. Finally, PLS-SEM was conducted to identify the predictive relevance of the study variables. When comparing the Mean Absolute Error (MAE) with the liner regression model, as suggested by Shmueli et al. (2019) it was found that for 17 of the 34 items included in the model, minor errors were identified. This result implies that the model is plausible for predicting affective symptoms in new samples of university students.
Discussion
The present study objective was to examine a model explaining anxiety and depressive symptoms in a sample of 405 university students from Colombia using PLS-SEM analysis. The model included four variables that have been linked to the presence of affective symptoms in this population: perfectionism, academic stress, rumination, and worry. The reviewed literature denoted that most of the previous studies have explored the contribution of these variables separately or through simple mediation or moderation analysis. However, we did not identify later research exploring a model in which these variables simultaneously interact in a more complex model. The present study supports the proposed model, where the four variables simultaneously interplay predicting anxiety and depressive symptoms in Colombian university students.
The study results provided evidence of a robust model explaining the underpinning mechanisms of affective problems in this sample, where academic stress and repetitive negative thoughts -both rumination and worry-, have a significant and positive effect on depressive and anxiety symptoms in students exhibiting increased levels of perfectionist traits. All the study hypotheses were accepted, finding direct and indirect relationships between the variables. First, we found a positive and direct relationship between perfectionism and academic stress, as found in the study by Cowie et al. (2018), who proposed that perfectionist traits in students may affect the implementation of proper strategies to buffer the academic demands that higher educational context usually represents.
Furthermore, we provide evidence that the relationship between perfectionism and increased levels of affective symptoms was mediated by academic stress. This is a novel finding as previous studies have shown direct associations between these variables (e.g., Cox et al., 2009; O'Connor et al., 2010; Raspopovic, 2015) but, to our knowledge, this is the first study to identify the mediating role of academic stress. This result suggests that affective symptoms will be exhibited to a greater extend in students experiencing both personal (perfectionist traits) and external factors (academic stress): the exposure to academic stress may affect the implementation of strategies to cope stressful situations (Barraza, 2007) in students prone to social isolation and negative feelings about their performance -those with increased perfectionism according to Rnic et al. (2021)-.
Moreover, this study found evidence of a double mediation, where repetitive negative thoughts also mediate the relationship between academic stress and affective symptoms. It was found that worry and rumination have a direct and positive effect on both anxiety and depressive symptoms. Later studies have also provided evidence about the contribution of worry on affective symptoms (Erickson et al., 2020; Muris et al., 2004; Skodzik et al., 2016), as well as for the contribution of rumination on these symptoms (Pimentel & Cova, 2011; Drost et al., 2014; McLaughlin & Nolen-Hoeksema, 2011; Yilmaz, 2015). However, we did not find studies exploring the mediating role of repetitive negative thoughts. In this line, our results suggest that for those university students presenting perfectionist traits who also perceive a stressful academic environment, worry and rumination represent exacerbating factors for exhibiting both anxiety and depressive symptoms.
Despite that worry and rumination are considered key components for affective disorders, previous research indicates that not all the people who exhibited them present a psychiatric diagnosis, but increases the risk for (McEvoy et al., 2013; Wahl et al., 2019). Likewise, in this study, we included measurements for depression and anxiety focused on the different levels of response (physiological, behavioral and cognitive) to guarantee we were not assessing exclusively their cognitive component in terms of worry and rumination.
Broadly, results of this study justify the need of programs pointing out to target prevention and intervention programs in order to reduce the risk of affective disorders and decreasing its prevalence in university students. Particularly, a preventive approach will focus, in an initial stage, on the identification of those students presenting increased levels of perfectionism since the beginning of their university studies or even during school years. For instance, the review by Suh et al. (2019) found evidence about the effectiveness of a cognitive-behavioral approach, principally the use of mindfulness, stress management techniques and changing biased beliefs, to reduce perfectionist traits, which can be implemented in this regard. Also, promoting the adaptive components of perfectionism in students may prevent the appearance of anxiety and depressive symptoms (Rice & Dellwo, 2002). Similarly, a preventive focus based on our findings will be identifying academic stressors, especially in those students with higher levels of perfectionism to develop coping strategies to deal with the stress of the academic context (e.g., excess of academic work, demands, competition, and evaluations).
An intervention approach will be the identification of increased levels of worry and rumination, again especially in those students exhibiting perfectionism and perceiving academic stress, who also report the presence of depressive or anxiety symptoms. This student profile, if identified promptly, will benefit of psychological -and psychiatric interventions when needed-to reduce the risk of presenting the associated negative outcomes of affective problems not only in the academic context, but also in all their contexts of interaction, such as academic dropout, poor social development, student isolation, drug use, and self-harmful behaviors (Keyes et al., 2012). For example, there is evidence that the opposite of rumination is psychological flexibility. Psychological flexibility is a more functional way of relating to negative emotions and thoughts. It would be very important to identify profiles of students with this very high rumination component and to design mental health promotion programs training psychological flexibility (Cobos-Sánchez et al., 2017).
In conclusion, this study provides a basis for students’ university services -pointing out to promote their wellbeing-to focus preventive and intervention strategies in those students at a higher risk for affective problems. These strategies must begin with the identification of those students exhibiting perfectionist traits along with increased levels of reported academic stress and a tendency to focus on negative thoughts (worry and rumination) using validated measures. Also, it is relevant to identify levels of anxiety and depression in order to identify if they can improve without professional attention (e.g., psychological or psychiatric therapy). Then, university must provide accompaniment for the students to develop functional and positive strategies to deal with stressful situations, focusing on the academic ones, and promoting psychological flexibility. Finally, students with this profile need constant monitoring to identify the correct implementation of the taught strategies.
Limitations of the present study include the use of self-reported measures since the report consists of the participants' perceptions, which can be altered by the emotional state in which they answered, or because they may manipulate information. Despite the recruitment of the participants was conducted in a systematic way and they responded as university students, it was not totally under our control. Future research must include different measurement and assessment strategies for method biasing control. Future studies may also control results for type of university (private or public) as previous studies have identified differences, for example, in academic stress levels being higher in students from public universities (Eva et al., 2015; Alshagga et al., 2015). Since results of the present study involve a nonclinical sample and depressive symptoms average fell in a normal range, they cannot be generalized to clinical samples. Studies with clinical samples involving these variables will provide specific models in the way our study variables interplay when affective disorders have been diagnosed. Additionally, this study was cross-sectional, so causality must be interpreted cautiously. Longitudinal studies will allow causality exploration between the variables, which also we recommended to include additional ones that have shown links with affective problems in university students, such as personal care habits and e-learning (Islam et al., 2020), preexisting disorders and family and social support (Woon et al., 2021).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Also, this study was regulated by the profession law of the psychologist in Colombia, and the guidelines of research with humans of the American Psychology Association.
Informed Consent
Informed consent was obtained from all individual participants included in the study, all participants signed the informed consent before answering the questionnaires, and at the end of the application the student receive information about free line to obtain professional advice about issues mental health.
Open Practices
The raw data, analysis code, and materials used in this study are not openly available but are available upon request to the corresponding author. The instruments were digitized on Google Docs platform with prior authorization from the authors. The sample was recruited through the publication of eye-catching advertisements and informative videos in different groups of social networks, popular among university students, including pages of students from official and private universities, sports groups, and scholarships awarded by the State.
Data Analysis
Using PLS-SEM, the objective of the present study is to explore a novel model in which different variables interplay to explain affective symptoms in university students. We proposed the following hypotheses in which personal and contextual variables may contribute on the emergence of affective symptoms in university students, variables that have been mostly studied separately: H1: perfectionism will be positively associated with academic stress; H2: academic stress will be positively associated with anxiety; H3: academic stress will be positively linked to depressive symptoms; H4a: academic stress will mediate the association between perfectionism and anxiety, H4b: academic stress will mediate the association between perfectionism and depressive symptoms; H5a: worry will mediate the relation between academic stress and anxiety, H5b: and rumination will mediate the association between academic stress and anxiety; H6a: rumination will mediate the association between academic stress and depression, H6b: worry will mediate the relation between academic stress and depressive symptoms.
Appendix
Zung Depression Scale Kept and Removed Items. Zung Anxiety Scale Kept and Removed Items. Frost Multidimensional Perfectionism Scale Kept and Removed Items. Inventory of Academic Stress Kept and Removed Items. Penn State Worry Questionnaire Kept and Removed Items. Ruminative Responses Scale Kept and Removed Items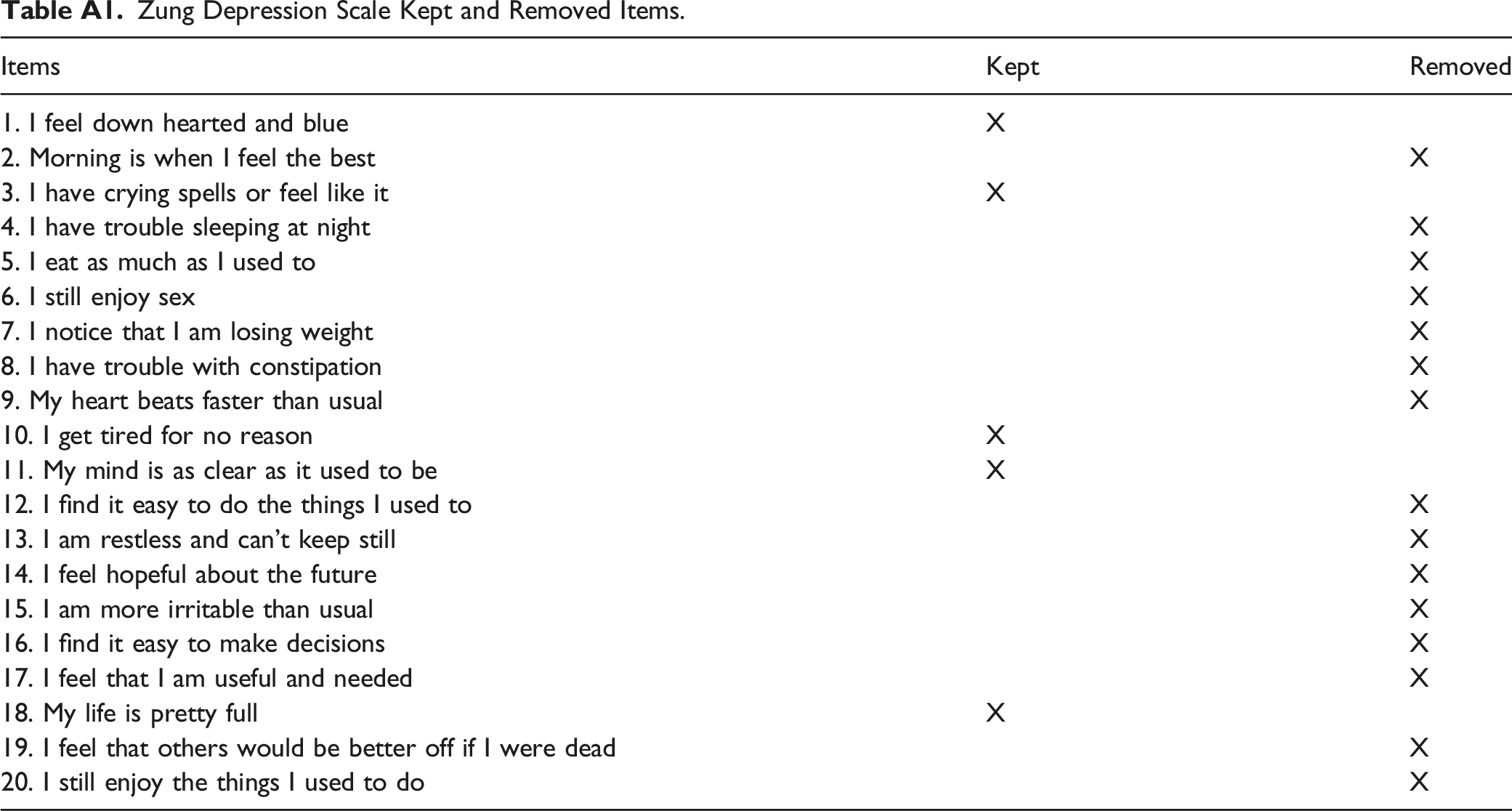
Items
Kept
Removed
1. I feel down hearted and blue
X
2. Morning is when I feel the best
X
3. I have crying spells or feel like it
X
4. I have trouble sleeping at night
X
5. I eat as much as I used to
X
6. I still enjoy sex
X
7. I notice that I am losing weight
X
8. I have trouble with constipation
X
9. My heart beats faster than usual
X
10. I get tired for no reason
X
11. My mind is as clear as it used to be
X
12. I find it easy to do the things I used to
X
13. I am restless and can’t keep still
X
14. I feel hopeful about the future
X
15. I am more irritable than usual
X
16. I find it easy to make decisions
X
17. I feel that I am useful and needed
X
18. My life is pretty full
X
19. I feel that others would be better off if I were dead
X
20. I still enjoy the things I used to do
X
Items
Kept
Removed
1. I feel more nervous and anxious than usual
X
2. I feel afraid for no reason at all
X
3. I get upset easily or feel panicky
X
4. I feel like I’m falling apart and going to pieces
X
5. I feel that everything is all right and nothing bad will happen
X
6. My arms and legs shake and tremble
X
7. I am bothered by headaches neck and back pain
X
8. I feel weak and get tired easily
X
9. I feel calm and can sit still easily
X
10. I can feel my heart beating fast
X
11. I am bothered by dizzy spells
X
12. I have fainting spells or feel like it
X
13. I can breathe in and out easily
X
14. I get numbness and tingling in my fingers and toes
X
15. I am bothered by stomach aches or indigestion
X
16. I have to empty my bladder often
X
17. My hands are usually dry and warm
X
18. My face gets hot and blushes
X
19. I fall asleep easily and get a good night’s rest
X
20. I have nightmares
X
Items
Kept
Removed
1. My parents set very high standards for me
X
3. As a child, I was punished for doing things less than perfectly
X
4. If I do not set the highest standards for myself, I am likely to end up a secondrate person
X
5. My parents never tried to understand my mistakes
X
6. It is important to me that I be thoroughly competent in what I do
X
9. If I fail at work/school, I am a failure as a person
X
10. I should be upset if I make a mistake
X
11. My parents wanted me to be the best at everything
X
12. I set higher goals than most people
X
12. If someone does a task at work/school better than I do, then I feel as if I failed the whole task
X
14. If I fail partly, it is as bad as being a complete failure
X
15. Only outstanding performance is good enough in my family
X
16. I am very good at focusing my efforts on attaining a goal
X
17. Even when I do something very carefully, I often feel that it is not quite right
X
18. I hate being less than the best at things
X
19. I have extremely high goals
X
20. My parents expect excellence from me
X
21. People will probably think less of me if I make a mistake
X
22. I never feel that I can meet my parents’ expectations
X
23. If I do not do as well as other people, it means I am an inferior being
X
24. Other people seem to accept lower standards from themselves than I do
X
25. If I do not do well all the time, people will not respect me
X
26. My parents have always had higher expectations for my future than I have
X
28. I usually have doubts about the simple everyday things that I do
X
30. I expect higher performance in my daily tasks than most people
X
32. I tend to get behind in my work because I repeat things over and over
X
33. It takes me a long time to do something “right”
X
34. The fewer mistakes I make, the more people will like me
X
35. I never feel that I can meet my parents’ standards
X
Items
Kept
Removed
1. During the course of this semester, have you had moments of worry or nervousness (stress)?
X
2. With the idea of obtaining greater precision and using a scale from 1 to 5 indicate your level of stress
X
3. Overload of tasks and academic papers
X
4. Personality and character of professors
X
5. Evaluation of professors (exams, tests, research, etc.)
X
6. The level of demand of my professors
X
7. Type of work that professors request (consult maps, worksheets, tests, concepts maps, etc.)
X
8. Limited time to do work
X
9. Do not understand topics covered in class
X
10. Chronic fatigue (permanent fatigue)
X
11. Feelings of depression and sadness
X
12. Anxiety, anguish or desperation
X
13. Concentration problems
X
14. Feelings of aggressiveness or increased irritability
X
15. Conflict or tendency to argue or debate
X
16. Unwillingness to perform student duties
X
17. Concentrate on solving the situation that concerns me
X
18. Establish concrete solutions to resolve the situation that concerns me
X
19. Analyze the positive and negative of the solutions designed to solve
X
20. Maintain control over my emotions so that I am not affected by what
X
21. Remember similar situations that occurred before and think about how I solve them
X
22. Development of a plan to perform your tasks
X
23. Pay attention or trying to get the positive out of the situation that worries
X
Items
Kept
Removed
1. If I don’t have enough time to do everything, I don’t worry about it
X
2. My worries overwhelm me
X
3. I do not tend to worry about things
X
4. Many situations make me worry
X
5. I know I shouldn’t worry about things, but I just cannot help it
X
6. When I am under pressure, I worry a lot
X
7. I am always worrying about something
X
8. I find it easy to dismiss worrisome thoughts
X
9. As soon as I finish one task, I start to worry about everything else I have to do
X
10. I never worry about anything
X
11. When there is nothing more I can do about a concern, I don’t worry about it anymore
X
Items
Kept
Removed
1. Think “what am I doing to deserve this?”
X
2. Analyze recent events to try to understand why you are depressed
X
3. Think “why do I always react this way?”
X
4. Go away by yourself and think about why you feel this way
X
5. Write down what you are thinking and analyze it
X
6. Think about a recent situation, wishing it had gone better
X
7. Think “why do I have problems other people don’t have?”
X
8. Think “why can’t I handle things better?”
X
9. Analyze your personality to try to understand why you are depressed
X
10. Go someplace alone to think about your feelings
X