
Abstract
Few studies have addressed the application of violence risk assessment for individuals transitioning from youth to adulthood. For 202 young adults released from Dutch juvenile justice institutions this study investigated the predictive validity and potential disparities in impact of juvenile risk assessment tools (i.e., SAVRY [Structured Assessment of Violence Risk in Youth], and SAPROF-YV [Structured Assessment of Protective Factors for violence risk-Youth Version]), and comparable adult risk assessment tools (i.e., HCR-20V3 [Historical Clinical Risk management-20 Version 3], and SAPROF [Structured Assessment of Protective Factors for violence risk]). Assessments with juvenile and adult risk assessment tools yielded similar predictive validity for violent and non-violent recidivism. Risk and protective factors related to treatability, parents, community participation, resilience, and personality showed individual predictive validity. These findings offer flexibility when applying risk assessment in clinical practice. The choice between youth and adult assessment tools should be made considering the individual’s developmental stage.
Keywords
The Validity of Violence Risk Assessment in Young Adults
In most Western countries, the transition between juvenile and adult criminal law is set at 18 years (Loeber et al., 2016; Pruin & Dünkel, 2015). This implies that from the age of 18 a person is responsible for his or her own behavior as an adult. However, the transition into adulthood does not take place overnight and the arbitrary cut-off of 18 appears artificial. Previous studies have demonstrated that the brain (i.e., prefrontal cortex) continues to develop (i.e., development of the prefrontal cortex and axonal myelination) up to the age of 25, and possibly even beyond (e.g., Benes, 1998; Diamond, 2002). As a person matures, neuropsychological functions gradually develop (e.g., empathy, and self-control). For instance, self-control is often underdeveloped in children which results in impulsivity, such as rule breaking or criminal behavior (e.g., Moffitt, 2006). During adolescence a gradual shift occurs from external self-control (i.e., externally controlled by parent, teacher) to internal self-control. However, this is not to say that self-control is suddenly fully developed when someone turns 18 (e.g., Steinberg et al., 2009).
Hand in hand with brain development, an important process takes place in which a large proportion of adolescent offenders gradually desist from criminal behavior. Research has shown that the prevalence of offending increases from late childhood, peaks around the age of 18, and then declines (Age crime curve, Farrington, 1986; Piquero et al., 2007). Young adults transitioning from adolescence to adulthood show the highest official arrest numbers when compared to younger adolescents and older adults (Blumstein et al., 1986; Perker & Chester, 2017). A large proportion of juvenile offenders (40–60%) desist from criminal behavior during the development from adolescence into adulthood. However, in a small group of individuals criminal behavior continues and may even increase in severity (e.g., Moffitt, 2006; 2017). These offenders are known as persisters (i.e., their criminal career extends into adulthood). The speed at which juveniles become responsible adults and exhibit self-control differs from one person to another (Loeber et al., 2016). Several studies have suggested that immature neuropsychological functions, such as underdeveloped executive functioning involved in emotion regulation, influence the persistence of antisocial behavior into adulthood (de Kogel, 2008).
Individuals in this transitional period from adolescence to adulthood (18 – 25 years) are generally known as young adults (also referred to as Transition Age Youth or Emerging Adults). There are different views on the precise definition of young adulthood. Arnett (2007) suggests that young adulthood is a distinct life phase with specific characteristics such as an exploratory identity, self-centeredness, optimism, and growth in autonomy. According to another perspective, young adulthood is not a separate life stage, but adolescent development extends longer than was previously believed and the upper limit of adolescence should be adjusted upward (Loeber & Farrington, 2012). In any case, both definitions indicate that it cannot simply be assumed that young adults have reached adulthood by the age of 18.
The perception of young adulthood is increasingly reflected in the way young adults are handled within the criminal justice system. Young adults within the criminal justice system are increasingly regarded as psychologically and socially developing individuals. As a result, in almost all European countries, offenders turning 18 during youth imprisonment are allowed to remain in juvenile facilities until their early 20s (Pruin & Dünkel, 2015). Furthermore, in many countries young adult offenders are treated differently from either older or younger offenders. For example, many countries provide special measures with a greater emphasis on resocialization. Some countries even apply a specific flexible law system for young adults. In the Netherlands, the Adolescent Criminal Law 1 allows for the application of juvenile criminal law for defendants between 18 years of age and 23 years of age, based on their developmental stage or circumstances. Since the adoption of the Adolescent Criminal Law in 2014, the application of juvenile criminal law to young adult offenders has increased rapidly (Liefaard & Rap, 2018; van der Laan et al., 2016). As a result of this and the before mentioned prolonged stay in juvenile facilities, young adults are well represented in juvenile correctional facilities (Verweij et al., 2021). Currently, in juvenile justice institutions in the Netherlands over 70 percent of the population is 18 or older. A similar situation appears to be present in many other juvenile justice settings across Europe (Pruin & Dünkel, 2015). From a developmental perspective, it can be applauded that juvenile interventions are increasingly imposed on young adults. Yet this also raises the question of whether youth interventions and youth assessment tools applied in juvenile facilities are suitable for this older population. The reality in juvenile justice institutions is often that juvenile risk assessment tools are being applied for the entire population. This results in a situation in which juvenile risk assessment tools are frequently being used for the assessment of young adult offenders.
The general purpose of risk assessment is to determine the level of risk each justice involved individual poses towards (violent) reoffending and, based on the assessed risk level and the associated risk or protective factors, to make objective and informed decisions about the intensity and nature of interventions needed to reduce the risk of reoffending. Several tools have been developed for the assessment of (violence) risk level in youth or adult offenders. The Structured Assessment of Violence Risk in Youth (SAVRY; Borum et al., 2006) is a frequently used tool for the assessment of violence risk in young offenders between 12 and 18 years. The Structured Assessment of Protective Factors for violence risk – Youth Version (SAPROF-YV; de Vries Robbé et al., 2015) has been developed as a comprehensive assessment of protective factors that should be used in conjunction to (mainly) risk-oriented assessment tools, such as the SAVRY. Together these tools are being used in Dutch juvenile justice institutions. Two similar tools for the assessment of risk and protective factors for adults of 18 years and older are the Historical Clinical Risk management – 20 Version 3 (HCR-20V3; Douglas et al., 2013) and the Structured Assessment of Protective Factors for violence risk (SAPROF; de Vogel et al., 2012).
The impact of several risk and protective factors in risk assessment tools tends to vary between different developmental periods. For example, the strong susceptibility to peer influence and antisocial peers during puberty, decreases during adolescence and seems to disappear for many people during young adulthood (Monahan et al., 2009). In contrast, the impact of individual factors and important life changes like marriage or finding stable employment increases during young adulthood (e.g., Horney et al., 2012; Loeber et al., 2013). In addition, Spruit et al. (2017) compared the relative importance of several risk factors in different adult age groups and found that problems with education and peers were mostly associated with recidivism in young adults (18–25 years) while problems with alcohol and drugs were the most important predictors for recidivism in older age groups (26–30 years, 31–40 years, and 41 years and older).
As different risk and protective factors are important for distinct age groups, juvenile risk assessment tools (generally developed for youth between 12 and 18 years of age) and adult risk assessment tools (generally developed for individuals of 18 years of age and older) show significant differences. Aspects of family environment, especially those related to parent-child relations, parental supervision or parenting skills, as well as aspects of the learning environment, especially bonding and behavior at school, are important components of juvenile risk assessment tools. Adult risk assessment tools are more focused on components such as social embedding, work and finances, symptoms of major mental illness (e.g., psychosis, bipolar disorder), and the degree of independent functioning. Both juvenile and adult risk assessment tools focus on the association between certain mental disorders and offending, however, different disorders are mainly addressed. Child and adolescent mental disorders, such as disruptive behavior disorders and attention deficit-hyperactivity disorder (ADHD), and symptoms of these disorders are frequently occurring risk factors in juvenile risk assessment. Features of personality disorders, especially psychopathic personality disorder, is a frequent cited component in adult risk assessment tools, as the association between psychopathy and adult offending has been well established (DeMatteo & Olver, 2022; Hemphill et al., 2014; Leistico et al., 2008). Maturity level has a central role in juvenile risk assessment tools, whereas personality-related factors are well-represented in risk assessment tools for adults (Borum et al., 2021; Borum & Verhaagen, 2006).
While there has been a substantial amount of research on risk assessment in juvenile as well as adult offenders, the international understanding of the application and predictive validity of risk assessment specifically for the young adult population, is surprisingly limited. Most studies on risk assessment still employ the arbitrary cut-off point of 18 years. Only a few have examined the predictive validity of different risk assessment instruments in a group of young adult offenders (de Vries Robbé et al., 2020; Spanjaard et al., 2016; Spruit et al., 2017; Vincent et al., 2019). However, these studies either used risk assessment tools developed for youth or adults, or compared youth tools in juvenile samples with adult tools in adult samples. To our knowledge, there have been no studies comparing the effectiveness of risk assessment instruments developed for youth to instruments developed for adults in the same sample of young adult offenders. The lack of empirical knowledge regarding risk assessment with young adults leads to confusion among practitioners regarding best practice. From a clinical and scientific perspective, there is need for a thorough understanding and empirical validation of risk assessment specifically for young adults (Loeber & Farrington, 2012; Vincent et al., 2019).
In a previous study (Kleeven et al., 2022), we investigated age related differences in the predictive validity of two widely used juvenile risk assessment tools (i.e., SAVRY and SAPROF-YV). The current study aims to investigate the predictive validity for recidivism (general, violent, and non-violent) of various risk assessment tools designed for different ages in a sample of young adult offenders with a history of violent behavior. More specifically, this study investigates the predictive validity of juvenile risk assessment tools that are currently being used in Dutch juvenile justice institutions (SAVRY and SAPROF-YV), and compares their predictive validity with comparable adult risk assessment tools (i.e., HCR-20V3; Douglas et al., 2013, and SAPROF; de Vogel et al., 2012). In addition, the predictive validities of individual risk and protective factors in these tools are investigated, in order to gain better understanding regarding the value of specific factors during young adulthood. Based on previous findings with the tools for juveniles and adults, we expect to find at least moderate predictive validity (i.e., Area Under the Curve [AUC] ≥ 0.64; Rice & Harris, 2005) for all instruments. In addition, the risk and protective factors with the largest predictive value for young adults are expected to be related to motivational/individual aspects.
Method
Setting
The present study is part of a national study examining violence risk assessment in Dutch juvenile justice institutions (see Appendix A for a data transparency statement). Under the Dutch criminal law juvenile offenders between 12 and 18 years can be sentenced for youth detention, a mandatory treatment order (so called PIJ order), or an alternative sentence (e.g., community service,van der Laan, 2006). Application of juvenile or adult criminal law has been available since 2014 for young adult offenders between 18 and 23 years of age (van der Laan et al., 2016). Youth detention and a mandatory treatment order for those sentenced under juvenile law are carried out in a juvenile justice institution. In these institutions youths or young adults can also remain in pre-trial custody. Detention can be imposed for a maximum duration of 1 year for youth from 12 to 15 years, and two years for youth or young adults from 16 years and upwards. While under the mandatory treatment order serious offenders are sentenced with compulsory treatment for two to 6 years, depending on the severity of the offense and the individual’s psychopathology. In all juvenile justice institutions risk assessment is performed periodically with the SAVRY, often in combination with the SAPROF-YV. Violence risk is first assessed after approximately six to 8 months of treatment, and subsequently updated every 6 months. A recent SAVRY assessment was required for the approval of leaves of all offenders residing in juvenile justice institutions. Among all juveniles and young adults in juvenile justice institutions in the Netherlands, overall recidivism within 2 years is 57% (Verweij et al., 2021). In a previous study amongst young offenders discharged from juvenile justice institutions, it was shown that recidivism rates for young adults were significantly higher than for juveniles (Kleeven et al., 2022).
Subjects
Sample Characteristics.
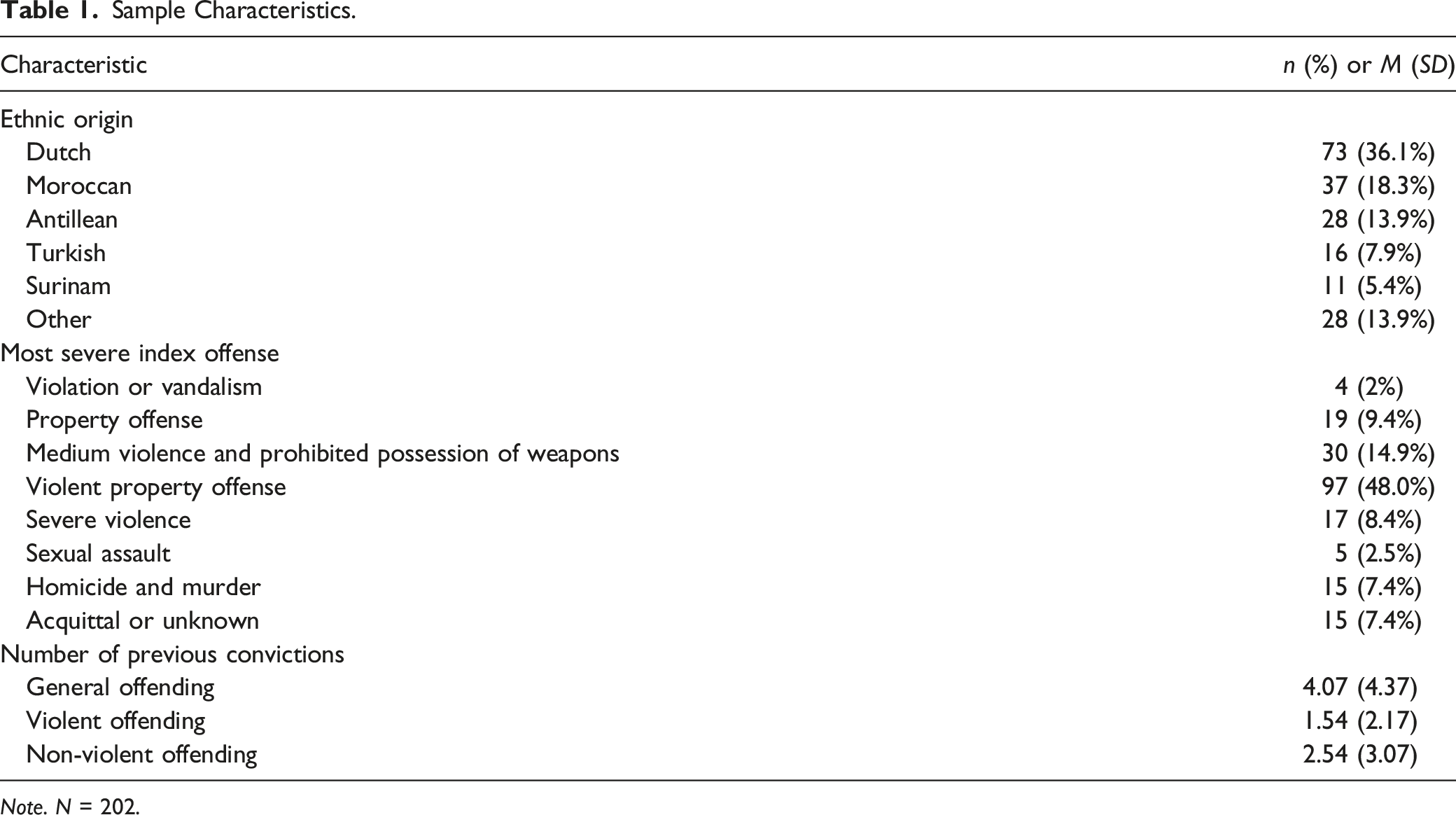
Note. N = 202.
Procedure
Instruments were rated retrospectively by trained researchers based on the available information in patient files at the end of treatment. The research team included 24 graduate students in Forensic or Clinical Psychology, Criminology, or related studies. All researchers received a 2-day workshop in the use of the SAVRY, SAPROF-YV, HCR-20V3 and SAPROF. In addition, during a period of 2 weeks researchers were trained in the use of the file system, coding of the risk assessment tools, and other procedures. During this period several practice cases were rated in consensus to examine whether risk assessment tools were rated as intended and the agreement between the different researchers was acceptable. Support from the principal investigator (PhD candidate) was available at all times.
Patient files consisted of reports by social workers, psychological and psychiatric reports with information on family and school context, individual characteristics, treatment plans and progress, and judicial information. Based on the available information upon release in a patient’s file, a single researcher rated the SAVRY, SAPROF-YV, HCR-20V3, and SAPROF. At the time of rating, researchers were not aware of information concerning recidivism and blind to any reports written after release from the juvenile justice institution. In addition, demographic data was obtained (i.e., sex, ethnicity, criminal history, index offense, psychopathology, treatment duration) and recidivism data was coded based on official criminal records. Interrater reliability was calculated, in order to determine the accuracy and consistency of coding the files. The files of 23 randomly selected cases were independently scored by two researchers in mixed pairs. After rating the files independently, the researchers agreed on consensus scores. The consensus scores were used in the predictive validity analysis, while the individual ratings were used only for analysis concerning interrater reliability. The Medical Ethics Committee of Amsterdam UMC University Medical Centers under the Medical Research Act issued a formal written waiver stating this research project did not require further approval from a Medical Ethics Review Committee. In addition, this research project was approved by all juvenile justice institutions in the Netherlands and the Dutch Ministry of Justice and Security.
Measures
SAVRY
The Structured Assessment of Violence Risk in Youth (SAVRY; Borum et al., 2006) is a risk assessment instrument which has been developed to determine violence risk in adolescents between the age of 12 and 18 years. In the current study, the Dutch translation of the SAVRY was used (Lodewijks et al., 2006). The SAVRY is composed of 24 risk factors in three risk domains (historical risk factors, social/contextual risk factors, and individual/clinical risk factors; see Table S1 in the supplemental material), and a protective factors domain including six protective factors. Each risk factor has a three-point rating scale with specific rating guidelines (low, moderate, or high), while each protective factor is rated dichotomously as either present or absent. The risk factors of the historical scale are rated regarding someone’s entire past, while the risk factors of the dynamic social/contextual and individual/clinical scales reflect functioning in the past 6 months, and ratings on the protective factors concern the past 12 months (Lodewijks et al., 2006). In practice the SAVRY is a Structured Professional Judgment (SPJ) tool in which scores are not added up, instead a final violence risk judgment regarding the coming months is composed based on the assessed factors combined with clinical judgment. However, for the purpose of the present study the SAVRY risk items were summed forming a SAVRY total risk score ranging from 0 to 48. The protective items of the SAVRY were summed forming a SAVRY total protection score ranging from 0 to 6. From the total sample, 23 cases showed one missing item on the SAVRY, and 1 case showed two missing items on the SAVRY. Out of all SAVRY items, 0.41% were missing. When calculating the total scores, missing values were replaced by mean values based on the remaining items for the individual. A recent systematic review on violence risk assessment in adolescents showed moderate to large levels of predictive validity, good to excellent interrater reliability, and excellent internal reliability (Cronbach’s alpha) for the SAVRY in various samples of young offenders (Koh et al., 2020). In a recent study amongst Dutch young offenders the SAVRY showed moderate to large levels of predictive validity for (violent) reoffending (Kleeven et al., 2022). In the current study, reliability analysis (Intraclass correlation coefficient [ICC], random two-way model, absolute agreement) of 23 cases showed excellent interrater reliability for the SAVRY total risk score (ICC = .82) and SAVRY protection score (ICC = .79).
SAPROF-YV
The Structured Assessment of Protective Factors for violence risk – Youth Version (SAPROF-YV; de Vries Robbé et al., 2015) is a relatively new tool for the comprehensive assessment of protective factors for violence in juveniles or young adults and can be used in conjunction with a predominantly risk-focused tool, such as the SAVRY. It consists of 16 dynamic protective factors on four domains (resilience, motivational, relational, and external items; see Table S3 in the supplemental material) that have been selected based on an extensive literature review for protective factors for violence in youth (de Vries Robbé et al., 2015). The items are rated as follows: clearly present (2), present to some extent (1), and not or hardly present (0). The possible addition of a plus (+) or minus (−) for more nuance in the scores of 0, 1, 2 results in a 7-point scale (0, 0+, 1-, 1, 1+, 2-, 2). All of the SAPROF-YV items were rated for the future context in the upcoming 6 months (i.e., post-discharge situation). Thus, the timeframe and context for which the protective factors in the SAPROF-YV are rated is different from that for the SAVRY factors. Although the SAPROF-YV is also an SPJ tool, for the purpose of this study the SAPROF-YV items were recoded into a 7 point scale (0 = 0, 0+ = 1, 1- = 2, 1 = 3, 1+ = 4, 2- = 5, 2 = 6), and summed forming a total score ranging from 0 to 96. The item Medication was rated ‘not applicable’ for 86.6% of the sample and was therefore excluded from the analyses. Of all other SAPROF-YV items 0.43% were missing. Of all cases in the current study, 10 cases showed one missing item on the SAPROF-YV, while 2 cases showed two missing items. When calculating the total scores, missing values were replaced by mean scores on the remaining items for the individual. In a recent meta-analysis it was found that the SAPROF-YV showed good interrater reliability (mean ICC = .80) and moderate-to-good validity in the prediction of the non-recidivism. Furthermore, the SAPROF-YV demonstrated incremental predictive validity when used in conjunction with a risk-oriented assessment tool (Burghart et al., 2023). In the current study, reliability analysis (ICC, random two-way model, absolute agreement) of 23 cases showed excellent interrater reliability for the SAPROF-YV total score (ICC = .79).
HCR-20V3
The Historical Clinical Risk management – 20 Version 3 HCR-20V3; Douglas et al., 2013) is a widely used SPJ violence risk assessment tool for adults containing 20 risk factors on three different scales: historical, clinical, and risk management (see Table S2 in the supplemental material). The historical scale contains 10 static risk factors. The clinical scale contains 5 dynamic risk factors that are rated on the basis of the past 6 months. The risk management scale is assessed for the near future (coming six to 12 months). All risk factors in the HCR-20V3 are rated on a three-point scale: absent (0), partly present (1), or clearly present (2). For the purpose of this study HCR-20V3 items were summed forming a total score ranging from 0 to 40. Out of all HCR-20V3 items, 0.72% were missing. From the total sample, 21 cases showed one missing item on the HCR-20V3, and 4 cases showed two missing values. When calculating the total scores, missing values were replaced by mean values based on the remaining items for the individual. In an annotated bibliography, including over 20 studies with the HCR-20V3, good to excellent interrater reliability (ICC’s from .64 to .94) and AUC values between .61 and 83 in different samples were found (Douglas et al., 2002–2016). In the current study, reliability analysis (ICC, random two-way model, absolute agreement) of 23 cases showed excellent interrater reliability for the HCR-20V3 total score (ICC = .87).
SAPROF
The Structured Assessment of Protective Factors for violence risk (SAPROF; de Vogel et al., 2012) is an SPJ tool used to identify protective factors in adults. It is intended to be used in addition to a risk-focused assessment tool, such as the HCR-20V3. This tool contains 17 protective factors (see Table S4 in the supplemental material). The first two factors in the SAPROF are static factors, while items 3 to 17 are dynamic protective factors that are rated for the near future (coming six to 12 months). The protective factors in the SAPROF are divided in three domains: internal, motivational and external items, and rated on a seven-point scale (0, 0+, 1-, 1, 1+, 2-, 2). For the purpose of this study total scores were calculated in the same way as for the SAPROF-YV, ranging from 0 to 102. The item Medication was rated ‘not applicable’ for 89.1% of the sample and was therefore excluded from the analyses. Of all other SAPROF items 1.60% were missing. From the total sample, 42 cases showed one missing item on the SAPROF, 5 cases showed two missing items, and 1 case showed three missing items. When calculating the SAPROF total scores, missing values were replaced by mean values based on the other SAPROF items for the individual. Previous studies with the SAPROF found good interrater reliability and predictive validity for violent as well as non-violent reoffending and other types of negative and positive outcomes mean ICC = .82, mean AUC = .77; see de Vries Robbé et al., 2021. In the current study, reliability analysis (ICC, random two-way model, absolute agreement) of 23 cases showed good interrater reliability for the SAPROF total score (ICC = .64).
Summary Risk Ratings
Two overall SPJ summary risk ratings (one for violent and one for non-violent criminal behavior) were composed for each individual by carefully combining, weighing and integrating the findings in all four assessment tools. As the different assessment tools in the current study were rated by one researcher, it was only possible to compose overall summary risk ratings based on all four assessment tools. These summary risk ratings were made on a five-point scale (low, low-moderate, moderate, moderate-high, or high risk) that reflected the estimated risk of violence or non-violent criminal behavior within the first 6 months after discharge. In the current study, reliability analysis (ICC, random two-way model, absolute agreement) of 23 cases showed good interrater reliability for the summary risk ratings (violence: ICC = .64, non-violent criminal behavior: ICC = .68).
Recidivism
Official recidivism data were obtained from records in the Judicial Documentation register of the Dutch Ministry of Justice. For all offenders a fixed follow-up period of 12 months post release was used. All offenses (excluding technical breaches of order) with an offense date within 12 months post release were coded as convictions for either violent offenses or non-violent offenses. General recidivism was defined as any new offense that led to official judicial conviction, violent or non-violent. Violence was defined as any (attempted) act intended to cause physical or psychological harm to others (Lodewijks et al., 2006). Young adults that committed both violent and non-violent offenses were accounted in both outcomes (i.e., violent and non-violent recidivism). To ensure that new offenses within 12 months after discharge had been processed accurately, recidivism data were retrieved over 30 months post the last release date.
Statistical Analyses
Data were analyzed using IBM SPSS statistics version 22 and the pROC package (Robin et al., 2011) in Rstudio version 3.4.2. In order to explore the overlap between the different tools Pearson’s correlations were calculated between the SAVRY, SAPROF-YV, HCR-20V3, and SAPROF (total scores). Correlations of 0.10, 0.30, and 0.50 were considered as respectively small, medium, and large in magnitude following Cohen (1992). In order to determine the predictive validity of all tools separately, Receiver Operating Characteristic (ROC) analyses were performed for general, violent, and non-violent recidivism with the total scores of the SAVRY, SAPROF-YV, HCR-20V3, and SAPROF, and the integrative summary risk ratings. AUC’s between .56 and .64 were perceived as small effect, AUC’s between .64 and .71 were perceived as medium, and AUC’s above .71 were perceived as large (Rice & Harris, 2005). The AUC’s for the SAPROF-YV, SAPROF, and protective factors of the SAVRY were reversed meaning scores were related to non-recidivism. In order to obtain the predictive value for risk and protective factors combined, multivariable logistic regression analyses were performed for general, violent, and non-violent recidivism with juvenile risk assessment tools (i.e., SAVRY total risk and SAVRY protection score; SAVRY total risk and SAPROF-YV total score) and adult risk assessment tools (i.e., HCR-20V3 and SAPROF total scores) separately. In separate analyses for general, violent, and non-violent recidivism, the SAVRY total risk scores were entered in the first step, and the SAVRY protection and SAPROF-YV total scores were entered in the second step of the analyses using different analyses for the SAVRY and SAPROF-YV protective factors. Similar multivariable logistic regression analyses were carried out with the risk assessment tools for adults, in which the HCR-20V3 total scores were entered in the first step, and the SAPROF total scores in the second step. ROC analyses were performed with the predictive values of the multivariable logistic regression analysis to obtain the area under the curve of the final prediction models. This procedure was adopted from prediction studies on key risk factors for cardiovascular disease or other medical conditions (see e.g., Schisterman et al., 2004). Through using the DeLong et al. (1988) method for comparing correlated ROC curves, obtained AUC values were compared. Finally item analyses were carried out, in order to gain better understanding regarding the value of specific risk and protective factors within the different assessment tools for young adults. ROC analyses for the SAVRY, SAPROF-YV, HCR-20V3, and SAPROF items were performed using general recidivism as outcome. For clarity, the choice was made to analyze a single outcome measure (general recidivism), since general recidivism includes both violence and non-violence, both are relevant to practitioners, and previous research has shown that the risk assessment tools used in the current study show predictive validity for violent recidivism as well as general recidivism (see for example Olver et al., 2009). In addition, it was decided not to apply corrections for multiple testing, as we expected that single items within the risk assessment tools showed small predictive validity (i.e., correcting these p-values would likely result in a situation in which all items were insignificant).
Results
Convergent Validity
Descriptive Statistics SAVRY, SAPROF-YV, HCR-20V3 and SAPROF.
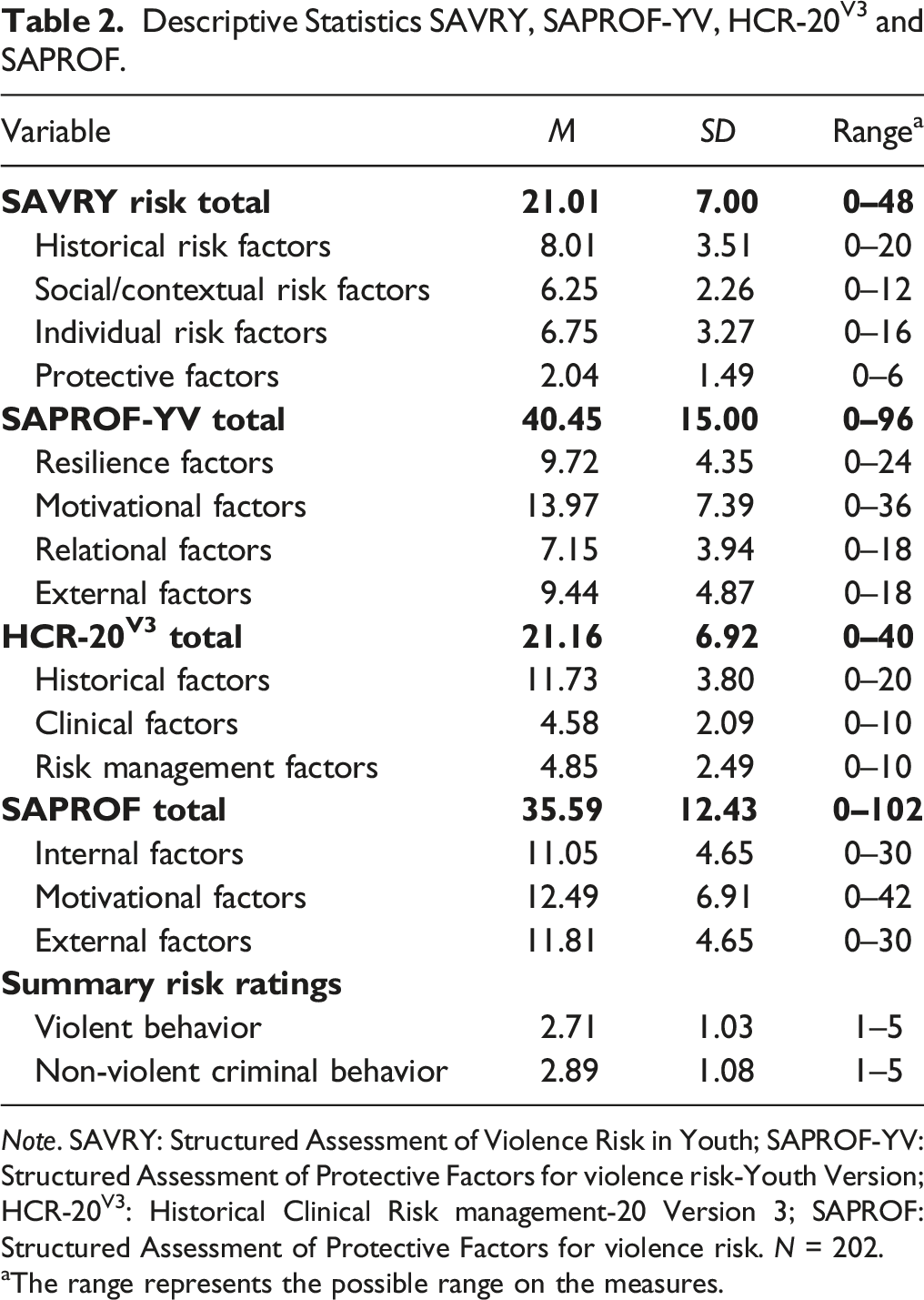
Note. SAVRY: Structured Assessment of Violence Risk in Youth; SAPROF-YV: Structured Assessment of Protective Factors for violence risk-Youth Version; HCR-20V3: Historical Clinical Risk management-20 Version 3; SAPROF: Structured Assessment of Protective Factors for violence risk. N = 202.
aThe range represents the possible range on the measures.
Correlations between SAVRY, HCR-20V3, SAPROF-YV, SAPROF, and Summary Risk Ratings.
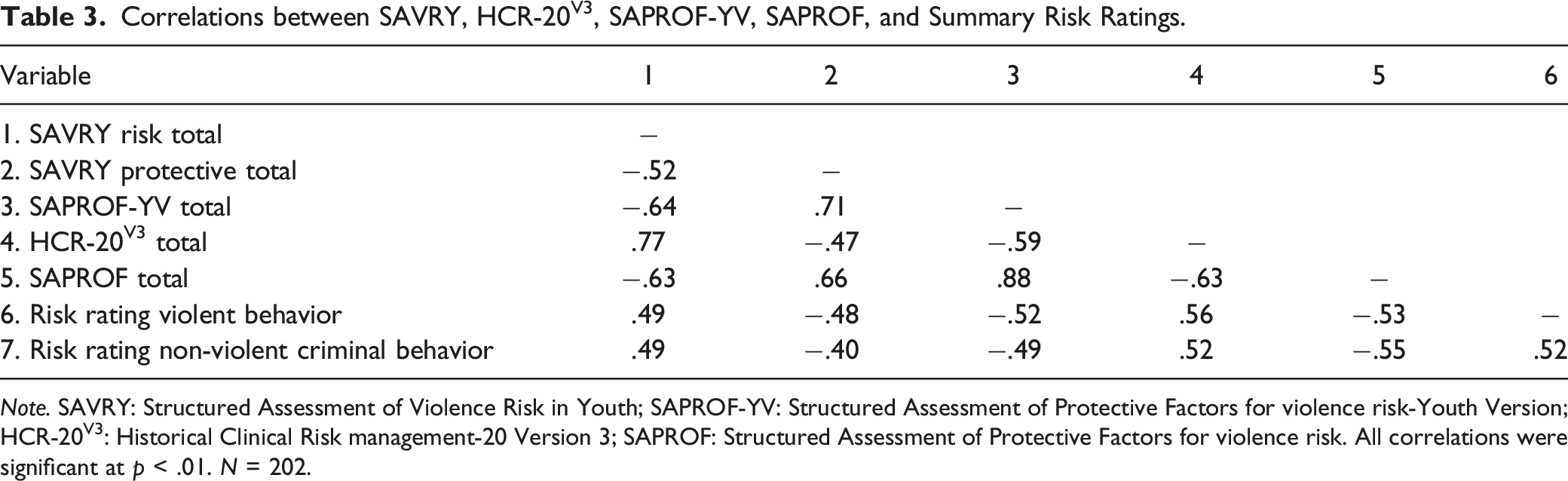
Note. SAVRY: Structured Assessment of Violence Risk in Youth; SAPROF-YV: Structured Assessment of Protective Factors for violence risk-Youth Version; HCR-20V3: Historical Clinical Risk management-20 Version 3; SAPROF: Structured Assessment of Protective Factors for violence risk. All correlations were significant at p < .01. N = 202.
Predictive Validity
AUC Values Recidivism 12 Months Follow-Up: SAVRY, SAPROF-YV, HCR-20V3, SAPROF and Summary Risk Ratings.
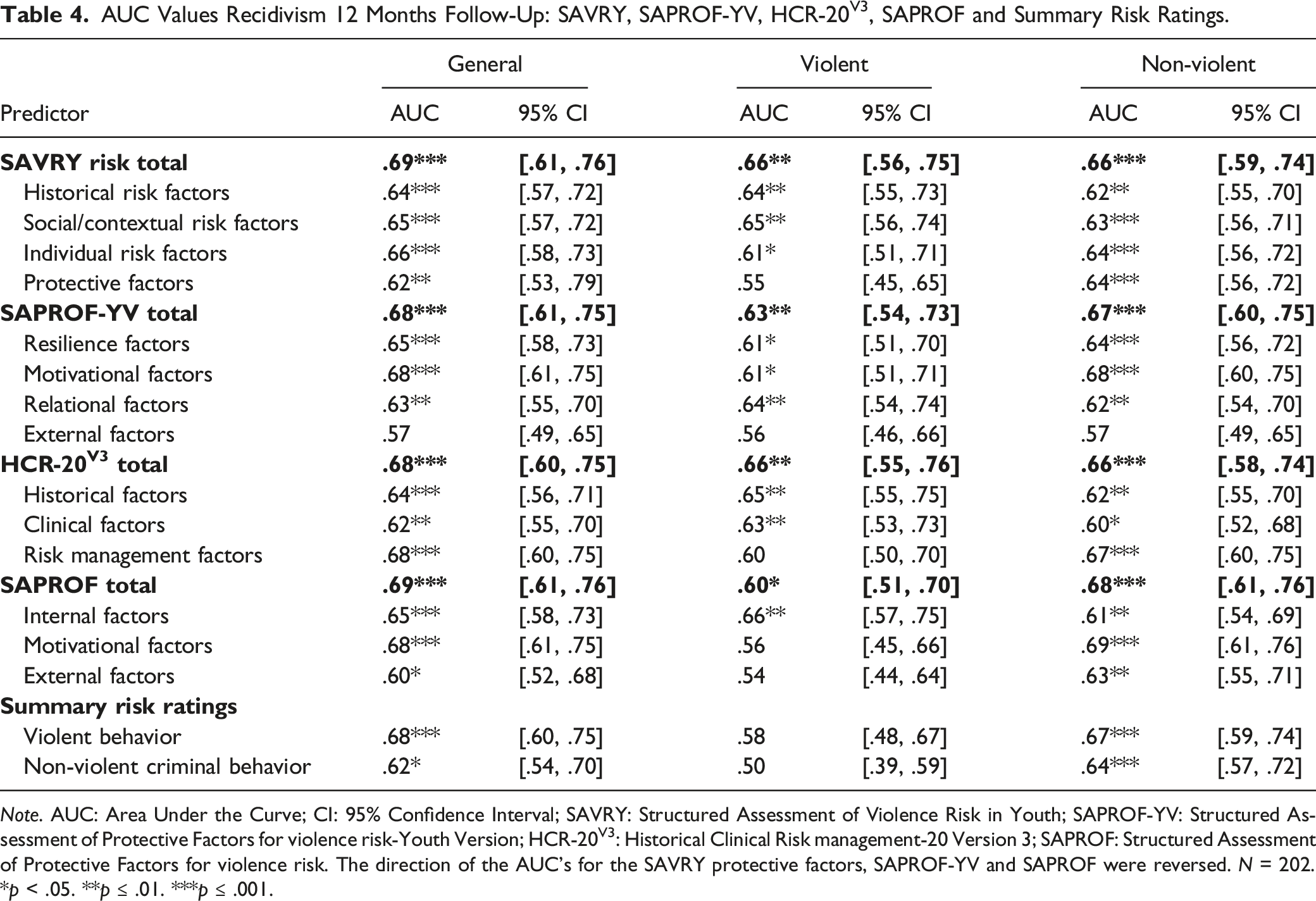
Note. AUC: Area Under the Curve; CI: 95% Confidence Interval; SAVRY: Structured Assessment of Violence Risk in Youth; SAPROF-YV: Structured Assessment of Protective Factors for violence risk-Youth Version; HCR-20V3: Historical Clinical Risk management-20 Version 3; SAPROF: Structured Assessment of Protective Factors for violence risk. The direction of the AUC’s for the SAVRY protective factors, SAPROF-YV and SAPROF were reversed. N = 202.
*p < .05. **p ≤ .01. ***p ≤ .001.
Multivariable logistic regression with the SAVRY, SAPROF-YV, HCR-20V3, and SAPROF showed that the juvenile assessment tools combined as well as the adult assessment tools combined showed significant predictive validity for general recidivism (SAVRY total risk and SAVRY protection: Χ2 = 24.09, p < .001; SAVRY total risk and SAPROF-YV total: Χ2 = 28.23, p < .001; HCR-20V3 total and SAPROF total: Χ2 = 26.08, p < .001), violent recidivism (SAVRY total risk and SAVRY protection: Χ2 = 12.13, p < .01; SAVRY total risk and SAPROF-YV total: Χ2 = 12.60, p < .01; HCR-20V3 and SAPROF: Χ2 = 10.47, p < .01), and non-violent recidivism (SAVRY total risk and SAVRY protection: Χ2 = 19.48, p < .001; SAVRY total risk and SAPROF-YV total: Χ2 = 22.35, p < .001; HCR-20V3 and SAPROF: Χ2 = 23.04, p < .001). AUC values with the predictive probabilities resulting from the logistic regression analyses with the SAVRY total risk and SAPROF-YV total scores, and HCR-20V3 and SAPROF total scores are shown in Figure 1. No significant differences were found between the combined juvenile and the combined adult risk assessment tools when assessing general, violent, and non-violent recidivism. Area Under the Curve SAVRY combined with SAPROF-YV, and HCR-20V3 combined with SAPROF.Note. AUC = Area Under the Curve; SAVRY: Structured Assessment of Violence Risk in Youth; SAPROF-YV: Structured Assessment of Protective Factors for violence risk-Youth Version; HCR-20V3: Historical Clinical Risk management-20 Version 3; SAPROF: Structured Assessment of Protective Factors for violence risk. Error bars show standard errors. N = 202.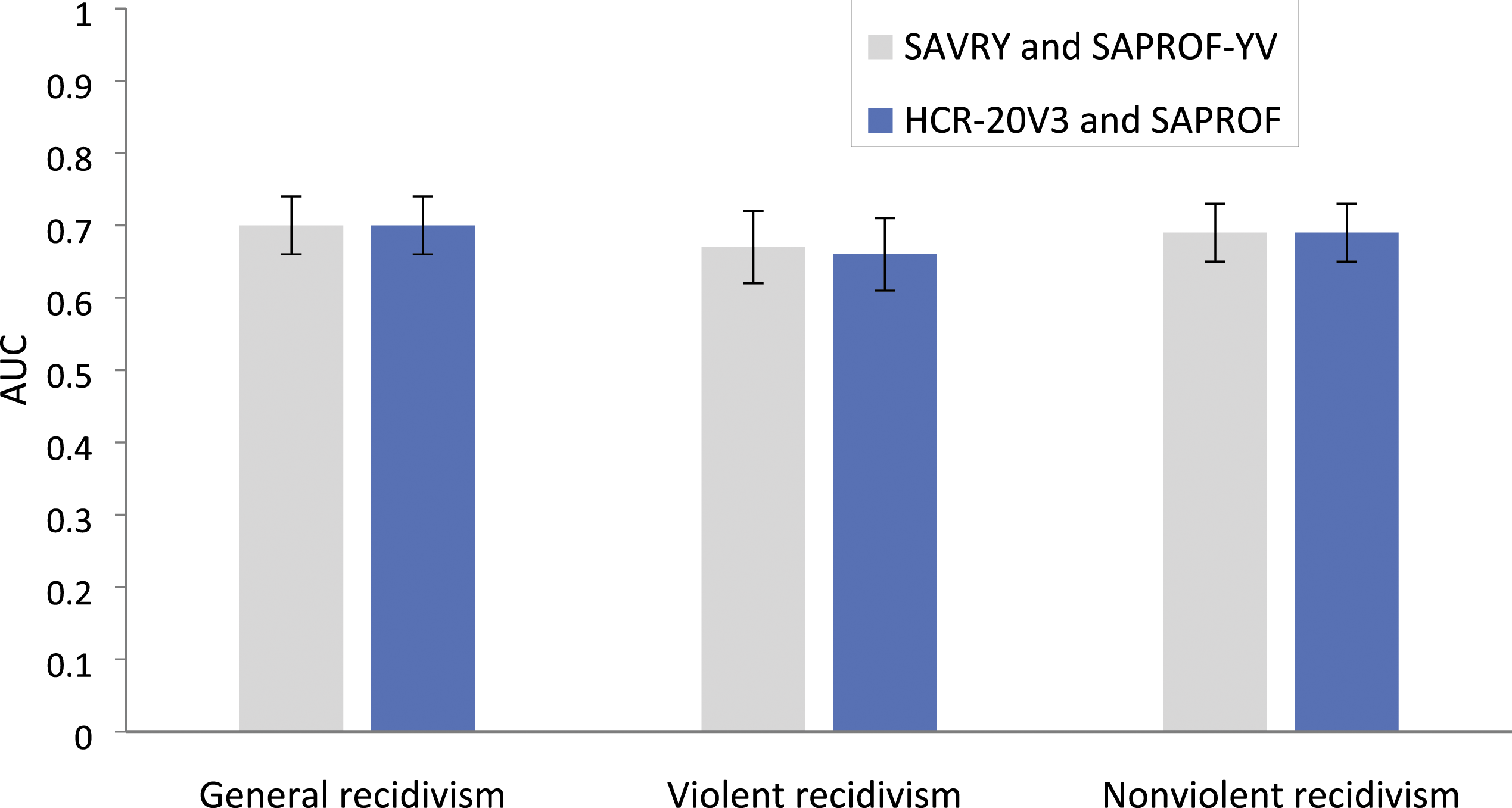
Predictive Validity Item Level
Predictive validities for general recidivism of the individual items in all four risk assessment tools are shown in the supplemental material. Significant individual predictors in the four risk assessment tools are described below.
Out of the 24 risk factors in the SAVRY nine showed significant individual predictive validity for general recidivism (see Table S2 in the supplemental material). None of the six protective factors in the SAVRY showed significant individual predictive validity for general recidivism. Small AUC’s were found for the SAVRY items history of violence (AUC = .62, p = .003), history of non-violent offending (AUC = .63, p = .001), past supervision/intervention failures (AUC = .62, p = .004), risk taking/impulsivity (AUC = .60, p = .02), anger management problems (AUC = .60, p = .02), low empathy/remorse (AUC = .58, p = .04), and poor compliance (AUC = .61, p = .007). Medium AUC’s were found the SAVRY items poor parental management (AUC = .64, p < .001) and negative attitudes (AUC = .67, p < .001).
For the HCR-20v3, 11 out of 20 risk factors showed significant predictive validity for general recidivism (see Table S2 in the supplemental material). Small AUC’s were found for the HCR-20V3 items history of other antisocial behavior (AUC = .59, p = .45), personality disorder (AUC = .59, p = .04), violent attitudes (AUC = .62, p = .004), problems with treatment or supervision response (in the historical scale and clinical scale: both AUC = .63, ps = .001), insight (AUC = .62, p = .004), instability (AUC = .62, p = .01) problems with professional services and plans (AUC = .62, p = .004), problematic living situation (AUC = .58, p = .05), and lack of personal support (AUC = .61, p = .01). A medium AUC was found for the risk factor problems with future treatment or supervision response within the risk management scale (AUC = .66, p < .001).
For the SAPROF-YV, 11 out of 16 protective factors showed significant predictive validity for general recidivism (see Table S3 in the supplemental material). Small AUC’s were found for the SAPROF-YV items social competence (AUC = .60, p = .02), coping (AUC = .62, p = .003), self-control (AUC = .60, p = .02), future orientation (AUC = .63, p = .001), parents/guardians (AUC = .63, p = .001), peers (AUC = .60, p = .03), and pedagogical climate (AUC = .59, p = .03). Medium AUC’s were found for the SAPROF-YV items perseverance (AUC = .67, p < .001), motivation for treatment (AUC = .65, p < .001), attitude towards agreements and conditions (AUC = .68, p < .001), and school/work (AUC = .64, p = .001).
For the SAPROF adult version, eight out of 17 protective factors showed significant predictive validity for general recidivism (see Table S4 in the supplemental material). Small AUC’s were found for the SAPROF items secure attachment in childhood (AUC = .61, p = .01), empathy (AUC = .59, p = .03), coping (AUC = .63, p = .001), self-control (AUC = .60, p = .01), life goals (AUC = .63, p = .002), and social network (AUC = .59, p = .03). Medium AUC values were found for the SAPROF items motivation for treatment (AUC = .66, p < .001) and attitudes towards authority (AUC = .67, p < .001). For comparison, all analyses were repeated post-hoc without the female offenders. This yielded similar results.
Discussion
The international understanding of the application and predictive validity of risk assessment in the young adult population specifically, is surprisingly limited. The present study was the first to compare the predictive validity of several risk assessment tools designed for juveniles with tools designed for adults in a national sample of young adult offenders (18–26 years). The results of this study suggest that juvenile and adult risk assessment tools are on group level equally applicable in young adult offenders when predicting recidivism risks.
Correlations
A strong positive association was found between both risk-oriented risk assessment tools for youth and adults (SAVRY risk and HCR-20V3) and between the youth and adult tools for protective factors (SAVRY protective factors, SAPROF-YV, and SAPROF), which suggests a high degree of overlap between items in juvenile and adult assessment tools. In line with our hypothesis a negative association was found between risk and protective factors in the different tools. This suggests that risk factors measure negative aspects and protective factors measure positive aspects, yet not directly opposite characteristics, of the individual or environment.
Predictive Validity of Youth versus Adult Risk Assessment Tools
No significant differences were found between the predictive accuracy of the combined SAVRY and SAPROF-YV in relation to the combined HCR-20V3 and SAPROF adult version, suggesting that total scores on both youth and adult tools predict recidivism in young adults in a similar way. It should be noted that the current study only included data on young adult offenders. As a result, no conclusions on the relative predictive validity in relation to other age groups can directly be drawn. However, a previous study in which the current sample of young adults was included and compared to a younger group of adolescents released from Dutch juvenile justice institutions, found that the predictive validity especially of several SAPROF-YV domains was somewhat higher in younger offenders (Kleeven et al., 2022). Comparison of the present results with previous meta analyses on the performance of risk assessment confirms that the predictive validity in the current study appears somewhat lower in relation to studies that applied these tools in either adolescents or adults (see also Olver et al., 2009; Singh & Fazel, 2010; Singh et al., 2011; Viljoen et al., 2017; Yang et al., 2010). The conclusion that can be drawn from this could be that although it is possible to predict recidivism in young adults with both juvenile and adult risk assessment tools, the overall performance of these tools is somewhat diminished when compared to either younger or older offenders. Thus, in general it seems young adults are a more difficult group to assess. However, these data must be interpreted with caution as research in this specific area is still limited. Future studies are needed in which juvenile and adult risk assessment tools are compared between different age groups (e.g., adolescents, young adults, and adults).
A surprisingly low predictive validity was found for the summary risk ratings when assessing violence. It has been found that combining and interpreting risk factors in order to arrive at a summary risk rating is a task that relies heavily on professional expertise (Douglas et al., 2003). In the current study this task was performed by students with little clinical experience. The current results could reflect that these students struggled with estimating final risk levels on the basis of all risk and protective factors, their relevance to the individual case and the future context. Prospective studies are needed to further investigate the predictive validity of summary risk ratings made by professionals in clinical practice using both youth and adult tools.
Predictive Validity Item Level
Analyses at item level revealed several important risk and protective factors for the assessment of (violent) recidivism in the current sample of young adults. These risk and protective factors were mostly related to treatability (e.g., treatment compliance, motivation, and attitudes towards agreements), social network (e.g., peers, parents/guardians, lack of social support, or parental management), community participation (e.g., school/work, future orientation), and resilience or personality factors (e.g., self-control, coping, perseverance, negative/violent attitude). When examining whether these factors were equally present in both juvenile and adult risk assessment, several similarities between the SAPROF-YV and SAPROF and between the SAVRY and HCR-20V3 emerged. For example, on both the SAPROF-YV and SAPROF, the items coping, self-control, motivation for treatment, attitude towards agreements/authority, future orientation (SAPROF-YV), and life goals (SAPROF) showed individual predictive validity for recidivism. In addition, risk factors related to problems with treatment compliance on the SAVRY and HCR-20V3 showed individual predictive validity.
In contrast, analyses at item level also revealed several important risk or protective factors for the current sample that were more prominent in either the juvenile assessment tools (SAVRY and SAPROF-YV) or the adult assessment tools (SAPROF and HCR-20V3). For example, while school/work in the SAPROF-YV showed significant predictive validity for recidivism, work in the SAPROF showed a predictive value at chance level, suggesting that school/education for the current sample might be more important than work. In addition, in the SAPROF-YV several relational items (i.e., parents and peers) showed individual predictive validity. It must be noted that relational factors in the SAPROF adult version are pooled together into one item (social network) that indeed also showed individual predictive validity. It appears valuable for the young adult group to be able to assess the support from different types of network members more specifically. Further, risk factors related to poor parental management showed individual predictive validity in the SAVRY, while in the HCR-20V3 no risk factors related to parental management are included. Finally, risk factors in the HCR-20V3 related to personality disorders or problems with insight showed individual predictive validity (these factors are less explicitly represented in the SAVRY).
Implications
Taken together these results could reflect that young adults are indeed still in development with characteristics represented in both juvenile and adult risk assessment tools that could be important in the prevention of future offending. As adolescence is a period of immense growth, there is also incredible diversity and heterogeneity in developmental pathways and the rate at which specific characteristics evolve. This implies that there is no simple uniform answer to the question which risk assessment is most applicable for this age group. Rather, the choice of the most appropriate assessment tool for each young adult individual should be based on his or her developmental phase and specific characteristics (e.g., degree of independence, presence of a personality disorder or other major mental disorders). Thus, given the little difference at group level, the judgment call whether to apply juvenile or adult risk assessment tools can best be evaluated at individual level.
Strengths and limitations
The current study had a number of strengths. This study was part of a national multicenter study on risk assessment in which all juvenile justice facilities in the Netherlands participated. It was the first study that directly compared the predictive accuracy of risk assessment tools developed for juveniles and adults in a sample of young adult offenders. As a result, possible differences in predictive validity between different tools could not be a function of other factors such as outcome follow-up duration or population differences, which have been known to influence differences in predictive validity. The results of this study could be of great value for clinical practice as there is much uncertainty about the best instruments to be applied.
Notwithstanding these strengths, this study should be viewed in the context of several limitations. It should be noted that in the current study instruments were scored on the basis of file information. As a result, it was impossible to retrieve additional information and behavior could not be observed in clinical practice, which could complicate the rating of some risk and protective factors. Future prospective research is recommended. However, by choosing this retrospective research method, a large number of young adults for whom recidivism data were available after release could be included within a short period of time. Recidivism data was collected based on criminal records, which reflects the crime that was noticed by law enforcement. While we believe that official reconvictions are the most reliable measures of recidivism, using official data most likely results in an underestimation of the true number of re-offenses. Future studies could attempt incorporating other measures of recidivism (e.g., self-report, police registrations) besides official reconviction data to overcome this obstacle. Further, it should be noted that in the current study all risk assessment tools for a given case were rated by the same research assistant. This was seen as the best method to prevent possible bias through different raters. Although research assistants were explicitly instructed to follow the different manuals at all times, and differences between relating items were extensively discussed during the training phase, this possibly resulted in greater similarities between ratings on juvenile versus adult tools. In addition, the current study only includes data on young adult offenders. Finally, the possibility of false positives should be acknowledged since it was decided not to correct for multiple testing in the item analyses.
Future Studies
The results of this study point to a compelling need for further research in the area of young adult risk assessment, especially for young adult offenders in relation to younger and older age groups. It appears that recidivism within this sample of young adult offenders is difficult to correctly predict. It must be noted that the young adults within the current sample represent a relatively high risk group of offenders. For instance, 21% of young adults were imposed with a mandatory inpatient treatment order, which is the most severe measure within the juvenile justice system in the Netherlands. It is unclear whether the complexity within this group or other specific characteristics of young adults significantly influence the predictive validity of risk assessment. For future studies it is advised to take the heterogeneity within these groups of offenders into account and to investigate which characteristics of young adults, their developmental stage, or brain maturation level could influence predictive validity. In addition, given that males and females mature at different rates, further work is encouraged to examine potential gender differences in the young adult population. Moreover, further work is required to establish if the current results could be translated to other samples, for example young adults within the adult correctional systems or young adults within other phases of the juvenile justice system or less restrictive interventions. Finally, for future studies in which multiple risk assessment tools are rated, it is recommended to counterbalance the order in which the tools are completed to avoid possible inter-instrumental effects.
Conclusion
Taken together, this study indicates that the use of either juvenile or adult risk assessment tools seems justified for predicting recidivism in young adults. Juvenile and adult assessment tools rely on a different set of risk and protective factors and both juvenile and adult tools seem to incorporate important factors for these transition age youth. Although the predictive validity of juvenile and adult tools is comparable, this does not imply that both tools are equally applicable for each individual in clinical practice when designing individually tailored treatment strategies. It is advised to choose assessment tools based on the clinical picture of the developmental phase and personal circumstances of the young adult. The tools best suited to the individual’s developmental stage are also expected to be the most valuable in informing treatment, designing risk management plans and monitoring progress over time. Future (prospective) studies are recommended to establish if a reduction in risk factors and increase in protective factors as measured by these tools is indeed associated with long-term desistance. It is also recommended to investigate how (brain) maturation plays a role in the effectiveness of juvenile or adult assessment tools. Additionally, studies in other young adult offender populations are needed as well (e.g., young adults in the adult correctional system or other settings such as probation or outpatient intervention and from different cultural backgrounds) to be able to generalize the current findings in order to further improve the effectiveness of risk assessment and management in this important transitional life phase.
Supplemental Material
Supplemental Material - The Validity of Violence Risk Assessment in Young Adults: A Comparative Study of Juvenile and Adult Risk Assessment Tools
Supplemental Material for The Validity of Violence Risk Assessment in Young Adults: A Comparative Study of Juvenile and Adult Risk Assessment Tools by Anneke T. H. Kleeven, Michiel de Vries Robbé, Eva A. Mulder and Arne Popma in Emerging Adulthood
Footnotes
Acknowledgements
We would like to thank all Juvenile Justice Institutions (JJI Den Hey-Acker, JJI De Hunnerberg, JJI De Hartelborgt, JJI Intermetzo Lelystad, Forensisch centrum Teylingereind, SJSJ Via Het Keerpunt, Het Poortje Jeugdinrichtingen JJI Juvaid) for participating in the current study.
Authors’ Note
This research project was conducted from the Amsterdam UMC, Vrije Universiteit Amsterdam in collaboration with the Academic Workspace Youth at Risk (AWRJ) and the Juvenile Justice Institutions in the Netherlands.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Co-author de Vries Robbé is also one of the authors of the SAPROF and the SAPROF-YV, two risk assessment tools used in the current study, which may be perceived as a conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Forensic Consortium for Adolescents (ForCA) and Ministry of Justice and Security, The Netherlands.
Transparency and Openness Statement
The raw data contained in this manuscript are not openly available due to privacy restrictions set forth by the institutional ethics board and the Dutch Ministry of Justice and Security, but can be obtained from the corresponding author following the completion of a privacy and fair use agreement. The analysis code, and materials used in this study are available upon request to the corresponding author. No aspects of the study were pre-registered.
Supplemental Material
Supplemental material for this article is available online.
Note
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.