
Abstract
Background:
Volunteer firefighters face elevated cancer risks from exposure to combustion by-products, exacerbated by limited decontamination resources, especially in rural departments. This proof-of-concept study assessed the feasibility and preliminary effectiveness of an online educational intervention to improve cancer prevention behaviors among Canadian English and French volunteer firefighters.
Methods:
A two-arm cluster randomized controlled trial was conducted across 23 volunteer fire departments. Departments were assigned to a 6-month online intervention (health letters, moderated chat room, and a 45-minute summary course) or a waitlist control. Firefighters completed the 20-item Firefighter Exposure to Carcinogens Scale (FECS) at baseline and 6 months, assessing intention, perceived importance, behavior, and barriers.
Findings:
A total of 115 firefighters enrolled; participant retention rates were 48.39% in the intervention group and 81.13% in the control group. The intervention group showed greater improvement in perceived importance (p = .04) and a trend toward reduced perceived barriers (p = .05). Intention scores trended positively (p = .08). Behavioral changes were not significant in the primary analysis, but when clustering was accounted for, behavior improvement reached significance (p = .01). Perceived barriers were negatively correlated with intention, importance, and behavior, with stronger correlations post-intervention.
Conclusions:
The intervention was feasible and showed potential to improve cancer prevention–related perceptions and behaviors. Recruitment challenges indicate the need for enhanced engagement strategies.
Application to Practice:
Online educational programs may support scalable cancer prevention training for volunteer fire departments, especially for rural and resource-limited settings.
Background
Firefighters face a serious risk of exposure to carcinogens from products of combustion. Modern materials burn hotter and are more toxic than older wood construction (Demers et al., 2022). Combustion releases carcinogens that can be transferred to firefighters via skin, inhalation, and ingestion causing significant risk of cancer (Sousa et al., 2022). Accordingly, the World Health Organization’s International Agency for Research on Cancer raised the cancer risk classification for occupational exposure as a firefighter from 2B classification (possibly carcinogenic) to the highest danger classification (International Agency for Research on Cancer, 2023). This classification is further reinforced by several recent studies (Laroche & L’Espérance, 2021; Sritharan et al., 2022; Stec et al., 2023; Wolffe et al., 2022). Preventing the increased risk of cancer in volunteer firefighters has raised attention as they may be more vulnerable to carcinogen exposure (Shah et al., 2024).
In Canada, there are about 89,000 volunteer firefighters, accounting for 71% of all Canadian firefighters, and 83.2% of the 3,248 fire departments are fully volunteer (Canadian Association of Fire Chiefs, 2023). The payment of volunteer firefighters varies across Canada, but they are typically paid a stipend for time spent on firefighting and training not a salary. All-volunteer departments are in smaller, more rural, and remote areas and have fewer resources, compared to career fire departments. Volunteer firefighters, while performing similar tasks to their career counterparts, typically spend less time at the fire station; respond to specific calls, and juggle full-time jobs along with their firefighting duties (Lantz et al., 2022). These challenges may make it difficult for firefighters in volunteer fire departments to conduct decontamination at the firehall, increasing the risk of bringing contaminants home and exposing their families (Harrison et al., 2018). Moreover, the absence of on-site facilities for gear decontamination and post-exposure safety measures further increases firefighters’ risk of prolonged exposure to harmful substances (Fernandez et al., 2023).
Prevention of cancers in firefighters requires significantly increasing firefighters’ understanding of preventive behavior including exposure control such as using appropriate Personal Protective Equipment (PPE) for the task, particulate blocking hoods, gear and by implementing decontamination practices (Harrison et al., 2022). It also requires education on long term effects of exposure to contaminants and appropriate monitoring for cancer (Hwang et al., 2021). Training, practice, and culture have not fully supported minimization of exposure to carcinogens at the fire scene and from contaminated gear after fires. A recent national survey of UK firefighters revealed that lack of training on fire effluents and their health risks was strongly associated with unsafe behaviors, including inadequate PPE cleaning and remaining in contaminated gear (Wolffe et al., 2022). Therefore, fire departments need timely, effective education with actionable suggestions on how to reduce exposures (Harrison et al., 2022).
Although electronic health (e-health) interventions are increasingly used across health disciplines, few peer-reviewed studies have examined their application to cancer prevention among volunteer firefighters. Educational initiatives exist through organizations such as the International Association of Fire Fighters (IAFF); however, these are not available in volunteer departments which are not unionized and have not been widely evaluated in the scientific literature. Given the wide geographic dispersion of Canadian volunteer firefighters, e-health interventions hold considerable potential due to increased accessibility and lack of geographic barriers. This study developed and evaluated the feasibility of delivering structured, behavior-focused online education, to enhance firefighters’ knowledge and cancer prevention behaviors.
This proof-of-concept study was conducted in close collaboration with the Canadian Association of Fire Chiefs (CAFC) to assess the feasibility and preliminary effectiveness of an educational intervention aimed at reducing carcinogen exposure among volunteer firefighters. The intervention was evaluated using the 20-item Firefighter Exposure and Decontamination Scale (McGrath et al., 2025), available in English and French, which assesses future behavioral intentions, perceived importance, current practices, and perceived barriers related to decontamination and exposure-reduction behaviors.
Theoretical Framework
Although not specifically a Theory of Planned Behavior (TPB) study, this trial was informed by TPB, which posits that engagement in health-protective behaviors is primarily driven by behavioral intention, influenced by attitudes toward the behavior, perceived norms, and perceived behavioral control (Ajzen, 1991). In this study, TPB informed both the design of the intervention and the selection of outcomes. The online educational content was designed to strengthen attitudes by increasing the perceived importance of cancer prevention behaviors and to enhance perceived behavioral control by addressing personal and organizational barriers to exposure reduction. Consistent with TPB, intention to engage in cancer prevention behaviors was selected as the primary outcome, with perceived importance, self-reported behaviors, and perceived barriers examined as secondary outcomes reflecting key determinants of behavior change in volunteer firefighter settings.
Methods
Study Population and Setting
This study was a two-arm proof of principle cluster randomized controlled trial (C-RCT) conducted in English and French volunteer firefighter departments across Canada. Each volunteer fire department served as a cluster. For the purposes of this study, a volunteer fire department was defined as one in which all active firefighters are considered volunteer, which may include firefighters paid part-time (if the department considers these volunteer), paid honorarium, paid expenses, or no remuneration, with no full-time career firefighters, other than possibly the department’s chief officers. Seventy-two English- and French-speaking volunteer fire departments were recruited by the CAFC, which promoted the study through its website, targeted email invitations to fire chiefs of volunteer fire departments across Canada, and online recruitment posts. Interested fire chiefs completed the departmental consent process to enroll their departments in the study. This trial was approved by IWK Research Ethics Board (IWK-REB) Halifax, NS, Canada (approval #1027461), and registered at clinicaltrials.gov (NCT05745246).
Randomization
The unit of randomization, the cluster, was the volunteer fire departments which were randomized into two groups: the intervention and control. To account for regional differences in cancer prevention policies and awareness, randomization was stratified by province. All firefighters within a department were assigned to the same study arm. The fire chief of each participating department invited their members to take part in the study voluntarily by sharing a secure REDCap link through which participants could review study information, complete eligibility screening, and provide informed consent. Interested members provided electronic consent and completed an eligibility questionnaire. Eligibility criteria included being a volunteer firefighter working in an all-volunteer fire department, residing in Canada, having regular internet access, and the ability to read, write, and understand English. Firefighters in the intervention group received a 6-month online cancer prevention program, and the waitlist control group, received the same program after the 6-month trial. This design ensured equitable access to the program for all participants while allowing for a controlled evaluation of its impact.
The unit of observation was the individual firefighter, including both frontline firefighters and department leadership (e.g., chiefs, deputy chiefs, assistant chiefs), as leadership in volunteer departments often engage in frontline firefighting activities. Participants were assessed at two time points: baseline (pre-intervention), post-intervention (6 months after baseline).
Intervention
The e-health educational program consisted of three key components: 44 health letters, a problem-solving asynchronous chat room, and a 45-minute pre-recorded summary online course at the end of the intervention period. The health letters were evidence-based messages designed by the research team members to increase awareness and motivation for cancer prevention behaviors. The letters were emailed to participants twice a week over a 6-month period through our 90Second platform. The health letters included a link to an asynchronous chat room, providing a moderated discussion forum where firefighters could engage with peers and experts to discuss challenges and exchange strategies for cancer risk reduction. The pre-recorded online course provided structured educational content covering best practices for reducing carcinogen exposure, proper use of protective equipment, and recommended screening guidelines. All intervention materials were precisely translated into French using a rigorous back-translation process to ensure linguistic accuracy and conceptual equivalence across both language groups. There was no masking or blinding of participants.
Outcomes
The outcomes were measured using the 20-item Firefighter Exposure to Carcinogens Scale (FECS), available in both English and French (Supplemental File 1; McGrath et al., 2025). The FECS assesses behaviors such as PPE use, gear decontamination, hygiene practices, equipment handling, and medical screenings. The items were derived from a comprehensive review of the existing literature. Content validity was assessed by three experts: an active-duty Deputy Fire Chief, an active-duty Fire Chief, and a retired firefighter who previously served as President of the Canadian Volunteer Fire Services Association. The FECS comprises four subscales: (1) Perceived importance of the behaviors in preventing cancer; (2) Past behaviors during the previous three fires attended; (3) Future intentions to engage in these behaviors, and (4) Barriers that hinder the performance of exposure-reduction behaviors. Barrier items reflect both personal factors (e.g., lack of time, knowledge, or training) and organizational factors (e.g., lack of departmental resources or management support). Each item is scored from 0 (Strongly disagree) to 4 (Strongly agree), with higher scores indicating greater endorsement of the construct being measured. Items in the Barriers subscale are reverse-scored so that higher scores represent greater perceived barriers. For each outcome subscale, responses were summed across the 20 behaviors to produce total scores ranging from 0 to 80. All scores were analyzed as continuous variables. The FECS has undergone exploratory and confirmatory factor analyses, which supported its factorial structure and demonstrated strong internal consistency across the first three subscales (Importance, Intention, and Behavior), with high McDonald’s omega coefficients (≥0.89). Full psychometric details are reported in our previous published paper (McGrath et al., 2025). All questionnaire responses and study data were securely collected using Research Electronic Data Capture (REDCap), an online data management system, that ensured data storage met ethical and confidentiality requirements.
The primary outcome, intention to engage in cancer prevention behaviors, was assessed using responses to the item “I would do this in the future if the resources were available” across the 20 specific health behaviors. The secondary outcomes were perceived importance, self-reported behaviors, identified barriers and the retention of firefighters in the study. Perceived importance was measured using the item, “This plays an important role in cancer prevention.” Self-reported behavior was assessed using the item, “I did this when I performed firefighting duties at the last three working fires.” Participants were also presented with a list of nine potential barriers and given space to report any additional factors that prevented them from performing the specific task. Retention was defined as the proportion of firefighters in each study arm who completed the post-intervention assessment. Retention was calculated separately for the intervention and control groups to capture differential completion patterns.
Statistical Methods
Descriptive statistics were used to summarize baseline characteristics of participants in the intervention and waitlist groups. Continuous variables were presented as means with standard errors (SE) or medians, while categorical variables were reported as frequencies and percentages. Differences between the groups at baseline, post-intervention and changes were assessed using two-sided t tests for continuous variables and chi-square tests for categorical variables. Multilevel one-way ANOVA analysis was performed to compare the changes in outcome scores between the groups. Pairwise correlation analysis was used to examine whether the outcome variables are strongly correlated with each other. Statistical significance was set at p < .05. Because this was a proof of principle trial, a per protocol analysis was used. In the per-protocol analysis, participants were analyzed according to the group to which they were assigned at baseline. Participants were excluded if they withdrew from the study during follow-up or did not provide post-intervention outcome data. Data were analyzed using Stata 16 (StataCorp, 2019).
Results
A total of 23 volunteer fire departments successfully recruited volunteer firefighters for this cluster-randomized study. One hundred and fifteen English and French volunteer firefighters were recruited at baseline. As shown in Table 1, the baseline characteristics of participants were similar across the intervention and control groups, indicating an effective randomization process. There were 62 participants in the intervention and 53 in the control group. As expected, the sample was predominantly male in both groups (80.65% vs. 81.13%, p = .95), with a mean age in the mid-30s (32.37 years vs. 35.28 years, p = .39). Most participants had occupational or technical vocational training and were employed full-time in addition to their firefighting duties. However, there were more fire chiefs in the intervention than in the control group (25.81% vs. 5.66%, p < .01). Although the groups differed slightly in location settings, most participants were from rural areas, and the difference was not statistically significant. The retention rate differed notably between groups. In the intervention group, 30 of the 62 firefighters completed the post-intervention assessment, resulting in a retention rate of 48.39%. In contrast, 43 of the 53 firefighters in the control group were retained, yielding a retention rate of 81.13%. Post-intervention outcome scores for intention, importance, behavior, and barriers were compared between the intervention and control groups (Table 2). While the intervention group had higher mean scores for intention, importance, and behavior, the differences were not statistically significant (p > .05). However, the intervention group reported lower barrier scores compared to the control group, suggesting fewer perceived barriers, with a trend toward significance (p = .06).
The Baseline Characteristics of the Participants in the Intervention and Control Groups
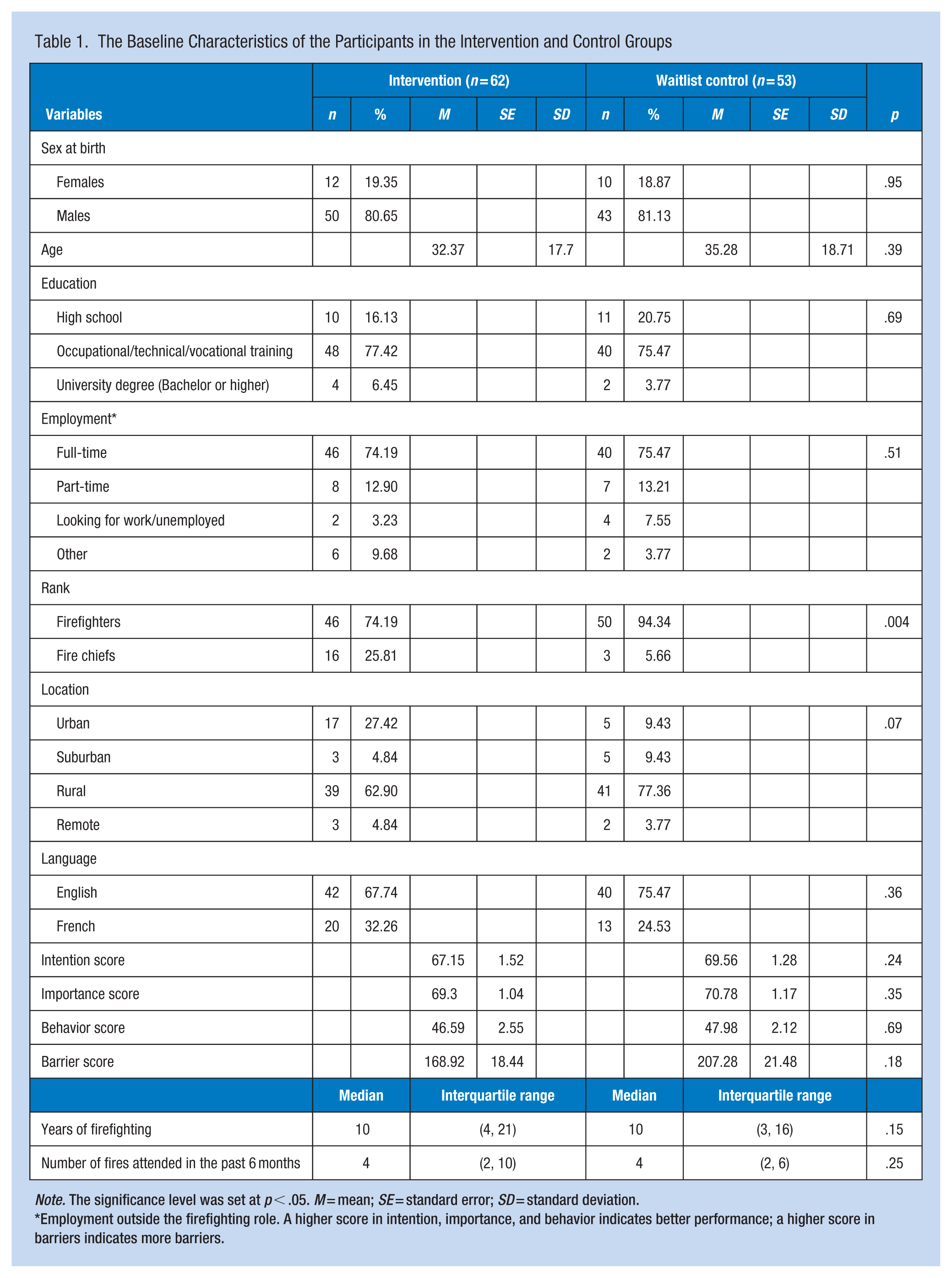
Note. The significance level was set at p < .05. M = mean; SE = standard error; SD = standard deviation.
Employment outside the firefighting role. A higher score in intention, importance, and behavior indicates better performance; a higher score in barriers indicates more barriers.
Post-Intervention Outcomes and Changes in Intention, Importance, Behavior, and Barrier Scores for Intervention and Control Groups
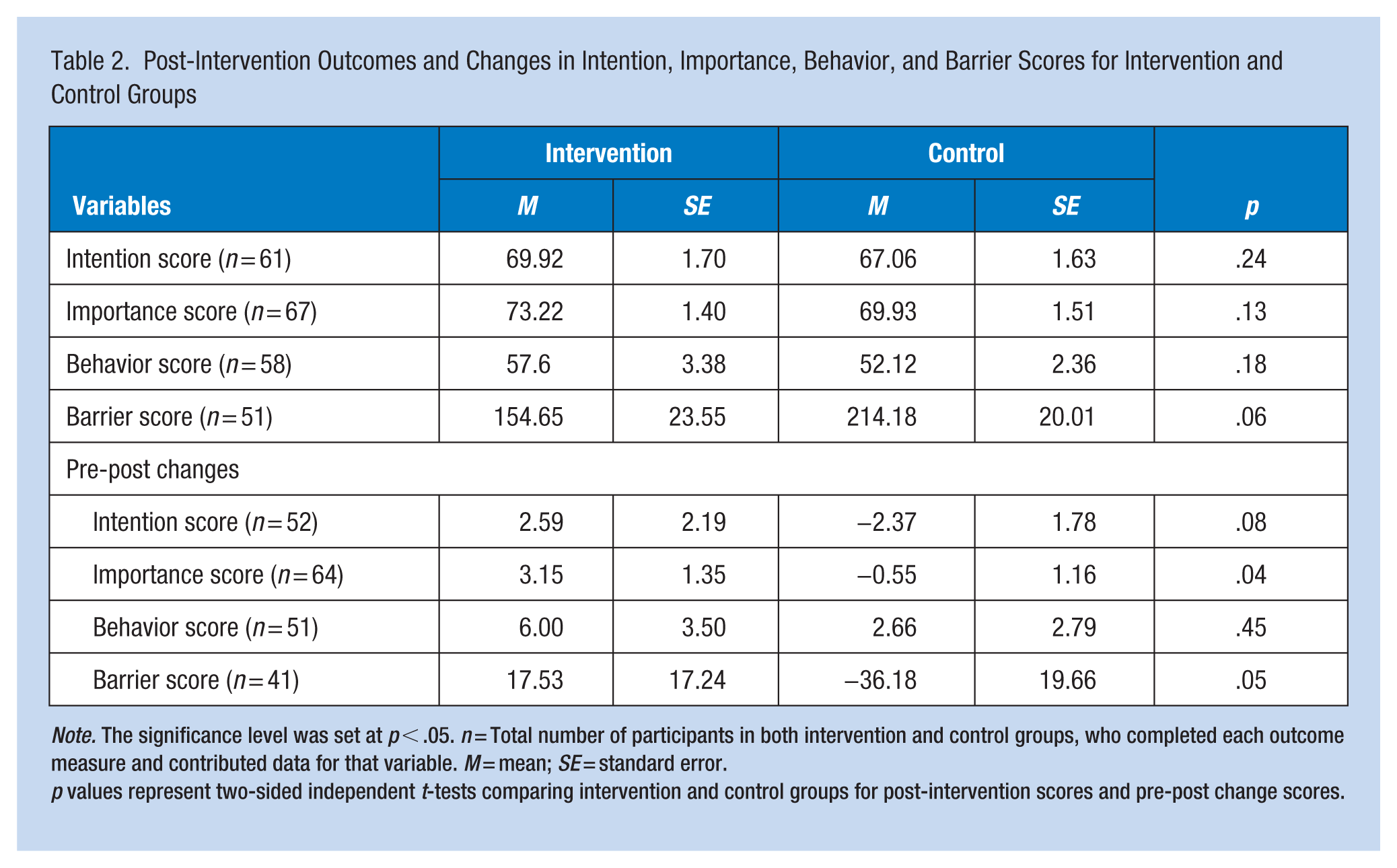
Note. The significance level was set at p < .05. n = Total number of participants in both intervention and control groups, who completed each outcome measure and contributed data for that variable. M = mean; SE = standard error.
p values represent two-sided independent t-tests comparing intervention and control groups for post-intervention scores and pre-post change scores.
When examining the changes in scores from baseline to post-intervention, the intervention group demonstrated greater improvements across all measures (Table 2). Specifically, the increase in importance scores was significantly greater in the intervention group than in the control group (M = 3.15, SE = 1.35 vs. M = −0.55, SE = 1.16, p = .04). Additionally, barrier scores decreased more in the intervention group, indicating a reduction in perceived obstacles, with this change approaching significance (M = 17.53, SE = 17.24 vs. M = −36.18, SE = 19.66, p = .05). The increase in intention scores also showed a non-significant positive trend (M = 2.59, SE = 2.19 vs. M = −2.37, SE = 1.78, p = .08). However, the change in behavior scores was not significantly different between groups (M = 6.0, SE = 3.50 vs. M = 2.66, SE = 2.79, p = .45).
As shown in Table 3, the one-way ANOVA, which accounted for clustering by fire departments, revealed a significant improvement in behavior scores for the intervention group compared to the control group (F = 8.11, df = 1, p = .01). This suggests that the intervention effectively enhanced firefighters’ engagement in the targeted behaviors. Additionally, a trending reduction in barrier scores was observed in the intervention group (F = 3.13, df = 1, p = .08), indicating a potential reduction in perceived obstacles to behavior change. However, changes in intention (p = .83) and importance (p = .69) scores did not show significant between-group differences.
Comparison in Different Outcomes by Group
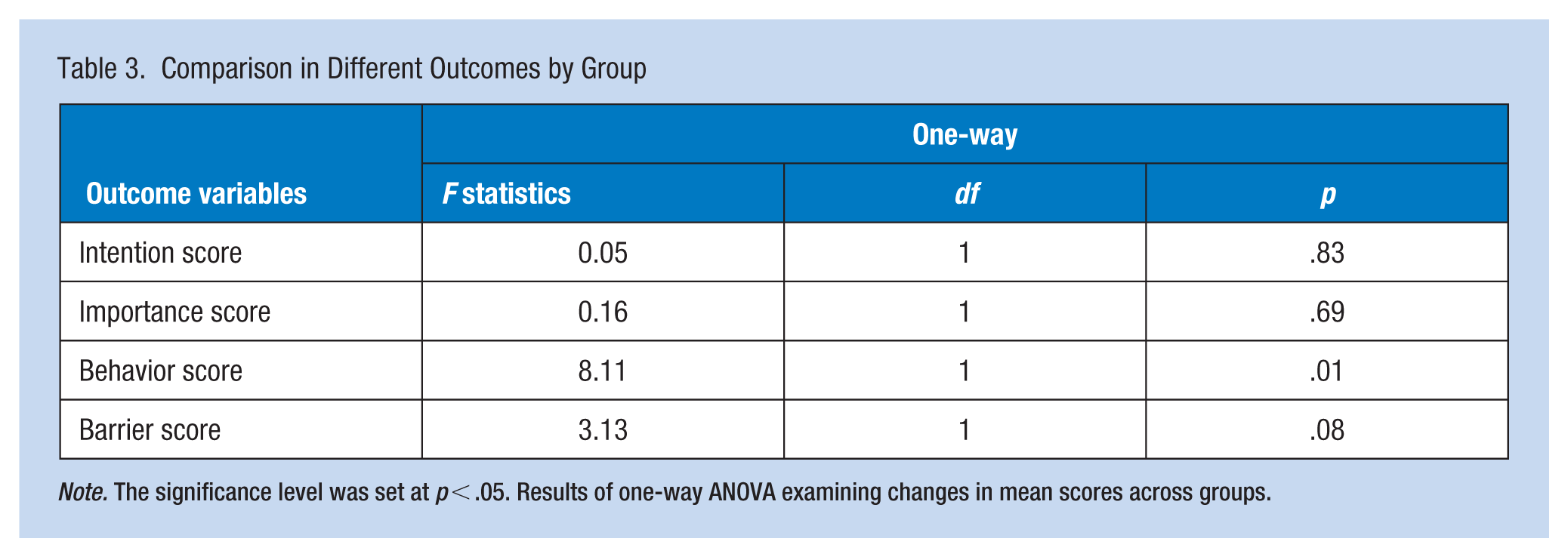
Note. The significance level was set at p < .05. Results of one-way ANOVA examining changes in mean scores across groups.
As shown in Table 4, pairwise correlation analysis revealed significant negative relationships between perceived barriers and intention, importance, and behavior at both baseline and post-intervention. At baseline, barriers were moderately negatively correlated with intention (r = −.20, p < .01), importance (r = −.28, p = .01), and behavior (r = −.49, p < .01), indicating that higher perceived barriers were associated with lower motivation, perceived importance, and engagement in the behavior. These negative associations strengthened post-intervention, with barriers showing stronger correlations with intention (r = −.52, p < .01), importance (r = −.53, p < .01), and behavior (r = −.57, p < .01).
Pairwise Correlation Between Barriers and Intention, Importance, and Behavior Outcomes
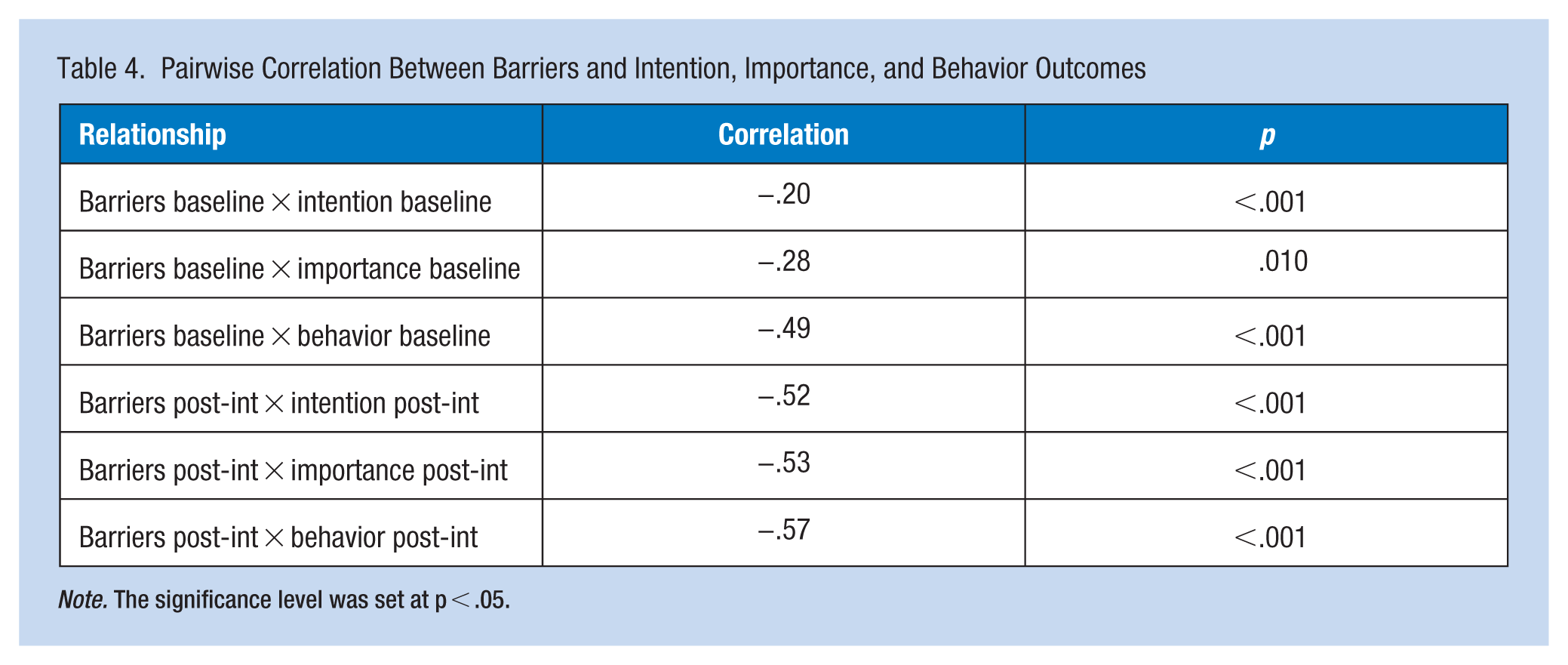
Note. The significance level was set at p < .05.
Discussion
The current proof of principle study evaluated the feasibility and preliminary effectiveness of an online educational intervention designed to enhance cancer prevention behaviors among Canadian volunteer firefighters. This cluster-randomized digital health intervention produced meaningful improvements in several cancer prevention related outcomes among volunteer firefighters. Compared with the control group, the intervention group showed significantly greater increases in perceived importance of the behaviors over the 6-month period and a significant improvement in behavior scores when accounting for clustering by fire department. The intervention also led to a notable reduction in perceived barriers, with this change approaching statistical significance, and consistent positive trends were observed for intention scores. Across both timepoints, perceived barriers were strongly and negatively correlated with intention, importance, and behavior, with these relationships becoming even stronger post-intervention, underscoring the central role of barrier reduction in behavior change.
This shift in perceived importance reflects a meaningful cognitive change, as individuals are more likely to adopt and sustain health-protective behaviors when they recognize their relevance (Schwarzer, 2008). These findings align with established behavior-change frameworks such as the Health Action Process Approach and the TPB, which emphasize that cognitive antecedents, including perceived importance, attitudes, risk perceptions, self-efficacy, and perceived barriers play central roles in shaping motivation and the adoption of protective health behaviors (Ajzen, 1991; Schwarzer, 2002). Although perceived importance is conceptually distinct from constructs such as attitudes or perceived risk of cancer, prior occupational health research shows that a range of cognitive antecedents influence firefighters’ safety behaviors. The review by Harrison et al. (2022) shows that perceived risk serves as a cognitive antecedent to the recognized importance of safety behaviors. Firefighters perceive their risk of developing cancer as originating from a comprehensive blend of hazards inherent to their work. These direct occupational risks arise immediately from their essential duties, including exposure to carcinogens during fire entry and the extensive clean-up process known as overhaul (Anderson et al., 2017; Macy et al., 2019; Solle et al., 2021).
McDonough et al. (2015) showed that tailored wellness programs can improve health behaviors and fitness among firefighters, supporting the value of structured interventions to enhance occupational health, such as the digital intervention evaluated in the present study.
Building on these cognitive shifts, we observed a reduction in overall perceived barriers to decontamination and exposure-reduction behaviors, with this change approaching statistical significance. The FECS captures both organizational barriers (e.g., departmental resources, leadership support) and personal barriers (e.g., time constraints, physical or emotional stress). It is likely that the observed reduction in barriers primarily reflects changes in personal barriers, as the educational content addressed factors within participants’ immediate control. Nevertheless, many organizational barriers captured by the FECS require systemic action at the department level. These findings suggest that while education can shift perceptions and enhance personal motivation, broader occupational health improvements will also require structural and organizational interventions. Future studies should also compare changes among fire chiefs and firefighters, as shifts in leadership behavior may be particularly influential in driving departmental change. Aligned with this result, we also observed moderate to strong inverse correlations between overall perceived barriers and outcomes such as intention, importance, and behavior, which became stronger after the intervention. While improvements in behavior were observed, the effect sizes were modest and not statistically significant in change scores, although a significant difference was detected when clustering was accounted for. This suggests that peer or organizational dynamics within departments may play a role in reinforcing behavior change. It is possible that informal peer interactions, common exposure to risk environments, or shared cultural attitudes toward safety may have played a role in reinforcing the behavioral messages conveyed through the intervention.
Participant retention differed notably between groups, with a smaller proportion of intervention participants completing the follow-up assessment compared with those in the control group. The higher retention in the control group may reflect the lower participation demands placed on this group, as they were not actively engaged in intervention activities. In contrast, participation in the structured educational content may have contributed to burden among firefighters in the intervention group, particularly given the competing responsibilities common among volunteer firefighters, many of whom balance full-time employment, family duties, and irregular emergency response schedules. This dynamic is well-documented in the literature. Lantz and Runefors’s (2021) systematic review of non-career firefighters identified family-related challenges and work-life balance as significant reasons for attrition. Building on this, longitudinal research by Huynh et al. (2024) using a job demands and resources framework found that higher job demands among volunteer firefighters predicted greater exhaustion, which in turn was associated with lower retention over time.
While volunteer firefighters in our study showed lower retention in the intervention arm, comparable data from career fire departments remain limited. Web-based interventions have been implemented among career and wildland firefighters, demonstrating feasibility and acceptability. For example, a web-based Total Worker Health program for wildland firefighters produced significant increases in safety and health knowledge and engagement with protective behaviors, with a 38% post-intervention follow-up rate (Kuehl et al., 2023). Similarly, the NFFF Stress First Aid intervention, which included an online module for career firefighters, achieved high satisfaction among participants (Jahnke et al., 2023). Large-scale multi-module online wellness programs have also been deployed for career, on-call, and volunteer firefighters in British Columbia, reaching thousands of participants (British Columbia Municipal Safety Association, 2024). These findings indicate that digital health interventions are feasible in career departments, but comparable data on retention rates in cancer prevention focused programs are sparse. Our results underscore the ongoing challenges of engagement and retention in volunteer firefighters and highlight the need for further research on scalable interventions across both volunteer and career settings.
Recruitment of volunteer fire departments into the trial was also lower than anticipated, despite substantial outreach efforts through the Canadian Association of Fire Chiefs. The dual role of volunteers as both full-time workers and firefighters likely limited their capacity to engage with an optional, multi-month online program. This aligns with broader evidence showing that workload, occupational stress, and competing life demands are major barriers to participation in supplemental programs among volunteer firefighters (Lantz & Runefors, 2021). Cultural factors in volunteer or rural departments such as informality in training practices, limited administrative capacity, and reliance on discretionary participation may also have contributed to reduced engagement. Future e-health interventions should consider strategies such as shorter modules, flexible schedules, multi-modal delivery, and integration into mandatory or routine departmental training to enhance feasibility in volunteer settings.
Our findings also align with the emerging literature on digital-health interventions aimed at improving occupational cancer prevention and general health behaviors among firefighters. Cancer-Free Heroes, a tailored web- and telephone-based program promoting colorectal cancer screening, demonstrated high feasibility and acceptability among current and retired firefighters (Piñeiro et al., 2025). In an online cross-sectional study, Oh et al. (2022) found that firefighters’ awareness of occupational exposure risks and related health beliefs were associated with their likelihood of engaging in protective behaviors, suggesting that educational interventions could enhance risk recognition and reduce barriers to protective practices. Web-based Total Worker Health interventions for wildland firefighters have also reported increases in health-related knowledge and safety-related engagement (Kuehl et al., 2023). Together, these studies reinforce the potential of digital and hybrid educational programs to shift knowledge, attitudes, and behaviors across diverse firefighting contexts, while also highlighting the unique implementation challenges in volunteer departments such as those reflected in our results.
Nevertheless, the cognitive and behavioral improvements identified here indicate that e-health interventions can be effective in both career and volunteer settings, particularly when designed to be scalable, flexible, and accessible for resource-limited departments.
Strengths and Limitations
A key strength of this study is its cluster-randomized design, which accounted for departmental influences and strengthened the validity of behavioral findings. In addition, the intervention demonstrates the feasibility of delivering a scalable digital program to geographically dispersed volunteer firefighters, producing measurable improvements in cognitive and behavioral outcomes related to cancer prevention.
Limitations of the current study include the large dropout rate in the intervention group, its small sample size, and the reliance on self-reported data, which may be subject to social desirability and recall bias. In addition, because this was a proof-of-concept trial with a small sample size, we used ANOVA to enhance statistical power; however, this approach carries a risk of inflated Type I error compared with multilevel modeling. Mixed-effects modeling will be used in the full-scale trial to address this limitation. The short follow-up period also limits conclusions about long-term behavior change. Future research should involve larger samples, objective outcome measures (e.g., contamination levels on gear or skin), and follow-ups extending beyond 6 months to assess sustained impact.
Implications for Occupational Health Practice
This study highlights the value of accessible online education as a practical tool for supporting cancer-prevention practices in volunteer fire departments. Digital programs may help fire departments, especially those in rural or resource-limited settings, provide consistent guidance and reinforce safer day-to-day practices related to exposure reduction. Nonetheless, strategies are needed to improve enrollment of departments and individual firefighters in such educational programs.
Applying Research to Occupational Health Practice
Volunteer firefighters face elevated cancer risks due to repeated exposure to combustion by products, while many departments, particularly those in rural or resource limited settings, have limited access to consistent occupational health training. This proof of concept study evaluated the feasibility and preliminary effectiveness of an online educational intervention designed to support cancer prevention practices among Canadian volunteer firefighters. Findings suggest that accessible online education may help strengthen firefighters’ perceptions of the importance of cancer prevention practices and support engagement with exposure reduction behaviours. The results also highlight the role of perceived barriers, which were closely associated with firefighters’ intentions, perceptions of importance, and engagement in cancer prevention practices. Addressing these barriers may therefore be an important consideration when designing prevention focused training programs. Online educational approaches may provide a scalable method to support cancer prevention education across volunteer fire departments, although improving recruitment and engagement remains an important consideration for future implementation.
Supplemental Material
sj-docx-1-whs-10.1177_21650799261429946 – Supplemental material for A Cluster Randomized Trial of an Online Training Program on Cancer Prevention Behaviors in Volunteer Firefighters: A Proof of Principle Trial
Supplemental material, sj-docx-1-whs-10.1177_21650799261429946 for A Cluster Randomized Trial of an Online Training Program on Cancer Prevention Behaviors in Volunteer Firefighters: A Proof of Principle Trial by Maryam Akbari-Fakhrabadi, Tina Saryeddine, Ivana Irwin, JianLi Wang, Graham Pawlett, Elena Laroche, Jim Petrik, Alberto Caban-Martinez, Lily Wang and Patrick J. McGrath in Workplace Health & Safety
Footnotes
Author Contributions
Graham Pawlett died before submission of this paper. Patrick J. McGrath: Led the research project, oversaw the study design, and ensured the research objectives were met, manuscript preparation. Maryam Akbari-Fakhrabadi: Research coordinator, contributed to study design, sampling techniques, and data collection procedures, manuscript preparation. Tina Saryeddine: Supported various aspects of the study: study design, participant recruitment logistics, intersectoral communications. Ivana Irwin: Contributed specific expertise such as firefighter safety practices, manuscript preparation. JianLi Wang: Analyzed the data collected from the study, conducted statistical analyses, manuscript preparation. Graham Pawlett: Contributed specific expertise such as firefighter safety practices. Elena Laroche: Contributed to study design, and data collection procedures specifically for the French firefighter recruitment. Jim Petrik: Contributed to study design and specific expertise such as firefighter safety practices, manuscript preparation. Alberto Caban-Martinez: Study design consultant. Lily Wang: Analyzed the data collected from the study.
Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by Canadian Institutes of Health Research (CIHR) and Canadian Cancer Society (CCS).
Ethical Approval
This study received ethical approval from IWK Research Ethics Board (IWK-REB) Halifax, NS, Canada (approval # 1028192) on July 27, 2022.
Consent to Participate
All participating firefighters provided online informed consent prior to enrollment.
Artificial Intelligence
The authors declare that the content, ideas, results, discussion, and conclusions presented in this article are their sole responsibility.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.