
Abstract
Background:
Clinician well-being is crucial to the healthcare system, particularly during the COVID-19 pandemic, which intensified psychological distress among clinicians. This study examines well-being disparities between rural and urban clinicians using the NIOSH Worker Well-Being Questionnaire (WellBQ).
Methods:
A cross-sectional survey was conducted with 222 clinicians from one urban and three rural hospitals in North Carolina between September and December 2022. The WellBQ assessed well-being across five domains. Data analysis identified concerning thresholds based on positive and negative responses, with discrepancies resolved through independent reviews and focus group validation.
Findings:
In the work evaluation and experience domain, rural hospitals reported concerns with time paucity and work overload, while urban hospitals focused on work-related fatigue and job engagement. Rural hospitals noted issues with job benefits, health programs, and schedule flexibility, whereas urban hospitals emphasized the lack of supportive work culture and management trust. Both settings reported concerns in the physical environment and safety climate domain, including sexual harassment, physical violence, and bullying. Health status concerns in rural hospitals included overall stress and poor mental health, while urban hospitals highlighted chronic health conditions and risky drinking.
Conclusion:
This study identified significant well-being disparities between rural and urban clinicians, with urban hospitals showing higher concerning thresholds. Future research should refine these thresholds, explore workplace violence causes, and assess long-term impacts on clinician well-being.
Applications to Practice:
This study reveals significant well-being disparities between rural and urban clinicians, emphasizing the need for tailored occupational health interventions.
Background
One of the largest and fastest-growing industries in the United States (U.S.) is healthcare, employing 22 million workers, which accounts for 14% of all U.S. workers (Laughlin et al., 2021; U.S. Bureau of Labor Statistics, 2024). Among them, 9.8 million workers are clinicians, specifically nurses and physicians, who were at the forefront of the COVID-19 pandemic (Kirzinger et al., 2021; Laughlin et al., 2021). Clinician well-being refers to the psychological and emotional health of healthcare providers, characterized by positive professional fulfillment and personal satisfaction derived from meaningful work, effective work-life integration, and a supportive organizational culture (National Academy of Medicine, 2017). However, psychological distress, including burnout, depression, post-traumatic stress disorder (PTSD), and moral distress, is prevalent among clinicians and poses a significant threat to their overall well-being (Guttormson et al., 2022; Mealer, 2020). Generally, the rates of these forms of psychological distress are higher in clinicians compared to the general worker population, further compromising their well-being (Dall’Ora et al., 2020; d’Ettorre et al., 2021; Epstein et al., 2019; National Academies of Sciences, Engineering, and Medicine; National Academy of Medicine; Committee on Systems Approaches to Improve Patient Care by Supporting Clinician Well-Being, 2019). During the pandemic, the prevalence of psychological distress among clinicians worsened markedly (Aiken et al., 2023; Durmuş, 2023; Townsley et al., 2023). This escalating psychological distress was reflected in the 2022 National Nursing Workforce Survey, where more than 60% of the 216,832 participating nurses reported an increase in their workload, and 46.2% of them reported feeling burned out at least a few times a week because of the pandemic (Smiley et al., 2023). Similarly, a study by Shanafelt et al. (2022) found that a 2021 survey of 2,440 physicians in the U.S. showed a significant rise in burnout, with 62.8% reporting symptoms compared to 38.2% in 2020. Additionally, satisfaction with work-life integration dropped from 46.1% in 2020 to 30.2% in 2021, while depression scores rose by 6.1% (Shanafelt et al., 2022). Numerous studies have also reported an increase in alcohol and substance use among healthcare professionals during the pandemic, closely linked to high levels of work-related stress, compounded by insufficient mental health services and job instability (Beiter et al., 2022; Jaguga et al., 2022; Madoz-Gúrpide et al., 2023; Myran et al., 2022).
In addition to the overall rise in psychological distress among clinicians during the pandemic, significant geographic disparities between rural and urban hospitals have exacerbated mental health challenges for rural clinicians (Harry et al., 2024; Leigh et al., 2020). Rural hospitals often face unique difficulties, such as limited access to mental health services, heavier workloads, and greater job instability compared to their urban counterparts (Asamani et al., 2015; Coughlin et al., 2019; Vaughan & Edwards, 2020). These challenges were intensified by the pandemic, as over 35% of rural hospitals experienced a more than 20% increase in average daily volume, compared to only 13% of urban hospitals (Bipartisan Policy Center, 2022; Jiang et al., 2024). Additionally, mortality rates in rural areas significantly increased in 2020, highlighting the heightened strain on rural healthcare resources, including intensive care unit (ICU) beds, personal protective equipment (PPE), and ventilators (Cuadros et al., 2021; Schou, 2021; Ullrich & Mueller, 2023; Wenninger et al., 2023). Consequently, the geographic disparities between rural and urban hospitals not only led to resource limitations and increased workloads in rural settings but also further worsened the mental health and well-being of rural clinicians (National Institute for Health Care Management [NIHCM], 2020; Slonim et al., 2020).
Recognizing the severe impact of these disparities on rural clinicians’ mental health, efforts to enhance clinician well-being have been supported by various entities, including federal and private agencies (e.g., National Institute for Occupational Safety and Health [NIOSH], National Academy of Medicine [NAM], Bureau of Health Workforce [BHW]) (Health Resources & Services Administration, n.d.; NAM, 2022; NIOSH, 2023). As one approach to address clinician well-being, the NIOSH and the RAND Corporation developed the NIOSH Worker Well-Being Questionnaire (WellBQ), a comprehensive tool designed to assess worker well-being across various sectors, including healthcare (NIOSH, 2022). The WellBQ provides an integrated assessment of worker well-being by evaluating five important domains: (1) work evaluation and experience; (2) workplace policies and culture; (3) workplace physical environment and safety climate; (4) health status; and (5) home, community, and society. The strength of WellBQ lies in its comprehensive approach to defining and operationalizing worker well-being as the concept of well-being is integrative, encompassing not only one’s health but also the environmental, organizational, and psychosocial factors related to work (Chari et al., 2022; NIOSH, 2024a). The NIOSH WellBQ is based on the NIOSH worker well-being framework, which encompasses the five domains.
However, due to the NIOSH WellBQ’s recent development, there is still insufficient information to establish standards or benchmarks for metrics across diverse worker demographics (NIOSH, 2024a). While the NIOSH WellBQ is a comprehensive tool designed to measure worker well-being across various domains, its relevance and effectiveness can vary significantly depending on the specific population being studied. For example, Powers et al. (2024) applied the NIOSH WellBQ to assess well-being of 323 early childhood education workers in the U.S. In their study, they had to exclude five questions—experiencing sexual harassment at work, experiencing physical violence at work, risky drinking, tobacco use, and work-related injury—due to low variability in responses. This exclusion indicates that these questions may not be relevant to this group (Powers et al., 2024). Thus, this study aims to (1) to identify thresholds based on concerning results by conducting a comparative analysis of findings between rural and urban hospitals, and (2) using such thresholds and corresponding survey context to prioritize concerning items for improvement efforts.
Methods
Study Design: Population and Sample
The cross-sectional and non-equivalent comparison group study designs were used to compare the percentages of positive and negative responses among clinicians in four hospitals: one academic medical center and three rural hospitals in North Carolina, U.S., from September to December 2022.
The study included a diverse group of healthcare professionals. Participants were categorized into two main groups: nurses and healthcare providers. “Nurses” refers to registered nurses (RNs) and licensed practical nurses (LPNs), who are responsible for delivering direct patient care, administering medications, coordinating patient services. The term “healthcare providers” refers to both physicians and advanced practice providers, such as nurse practitioners and physician assistants. All nurses and healthcare providers working in the participating hospitals were invited for the study.
Data Collection
Our study adhered to Institutional Review Board (IRB) protocols for participant recruitment and consent acquisition. The survey was administered electronically through Qualtrics to nurses and healthcare providers working in one academic medical center and three rural hospitals in North Carolina. The survey included demographic inquiries and assessments of work system factors utilizing the 68-item NIOSH WellBQ. All data were anonymized, and a master file was established for analysis.
To validate the findings, a virtual focus group was conducted with five researchers and five clinicians. The clinicians were recruited through purposive sampling to ensure representation from individuals with demonstrated expertise in clinician well-being and management. The focus group served two primary purposes: (1) to confirm the concerning areas identified in the survey results and (2) to explore broader perspectives on well-being domains. All members of the focus group provided verbal consent to participate in the validation efforts.
Variables and Measures
The NIOSH WellBQ is a 68-item survey that assesses worker well-being across five domains: (1) work evaluation and experience (16 items); (2) workplace policies and culture (14 items); (3) workplace physical environment and safety climate (10 items); (4) health status (23 items); and (5) home, community, and society (5 items). Additionally, there are 15 optional items covering employment circumstances and worker demographics. The items are rated on various scales, ranging from a 4-point to a 7-point Likert scale. For example, some items use a 4-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree). Others utilize a 5-point Likert scale, with 1 (poor) to 5 (excellent). Additionally, some items are rated on a 7-point Likert scale, where 1 represents “never” and 7 represents “always” (every day).
Data Analysis
Data analysis was conducted in three parts. First, the collected data were stratified based on the percentages of positive and negative responses. Our analysis took into account both types of responses from the participants. Positive responses, such as “strongly agree” and “agree,” were categorized as “no-concern.” Conversely, negative responses, including “strongly disagree” and “disagree,” were categorized as “concerning.” This approach allowed us to capture variations in responses and assess both ends of the spectrum, ensuring a comprehensive analysis.
Second, we evaluated the percentage of concerning responses versus total responses based on five corresponding thresholds set at 0% to 9%, 10% to 19%, 20% to 29%, 30% to 39%, and over 40%. These ranges were chosen to divide the data into meaningful categories based on percentage intervals, with the aim of providing a clear gradient of concern. This approach was decided upon through consensus among the researchers as a reasonable way to begin the analysis and to capture varying levels of concern in a structured manner. Then, two researchers independently reviewed descriptive survey findings for each survey item and identified thresholds where results were marked as needed further attention based on the threshold met and context of the survey item. Any discrepancies in this interpretation of results were resolved by a third experienced researcher with research background in the healthcare workforce. Missing data, which ranged from 5% to 32% across 68 questions were addressed through listwise exclusion to ensure the integrity of the analysis.
Finally, to validate the findings, a virtual focus group was conducted in October 2023 with 10 participants, comprising five researchers and five clinicians. The clinicians were selected based on their expertise in clinician well-being. During the 90-min session, results were presented in the order of the survey domains, starting with items from the first domain and proceeding sequentially. Participants were asked to review the previously agreed thresholds established by three researchers and provide feedback to confirm whether the thresholds were appropriate. Open-ended questions and discussions were encouraged to clarify the results, allowing participants to provide interpretations and key insights that informed the discussion section of the manuscript. Notes were collected by two researchers during the session, as discussions were not recorded. These notes were later used to generate key insights for the discussion of results.
Results
Our study had a response rate of about 22% (222 clinicians) across hospitals with 129 from the three rural hospitals, and 93 from the urban hospital. The distribution of nurses and healthcare providers was 161 and 61, respectively. Regarding their tenure in their current positions, a significant proportion had been working for 1 to 4 years (34.2%) or more than 10 years (32.9%). The demographic information of the sample is presented in Table 1, showing that the majority of participants were female (79.3%) and Caucasian (86.4%), with over two-thirds being married (68.3%).
Sample Characteristics
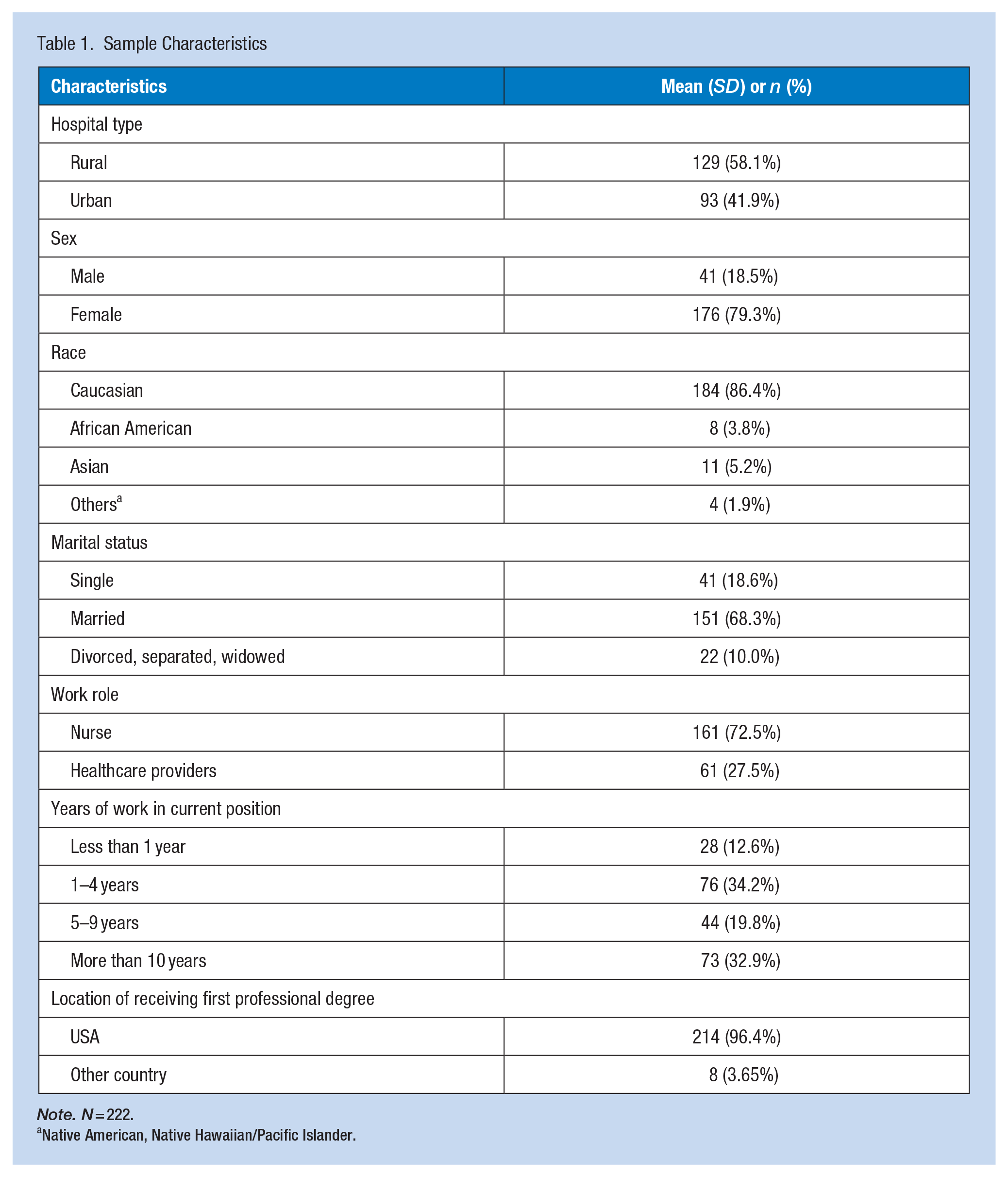
Note. N = 222.
Native American, Native Hawaiian/Pacific Islander.
The results across the NIOSH WellBQ’s five domains are shown in Table 2. The results showed that urban hospitals had more concerning thresholds across all domains compared to rural hospitals, with 41 concerning thresholds identified in urban hospitals and 28 in rural hospitals, making a total of 68 thresholds. Below, we present the findings from each of the five domains, highlighting the key differences and concerns identified between urban and rural hospitals.
Negative Thresholds in Rural and Urban Hospitals According to the NIOSH WellBQ
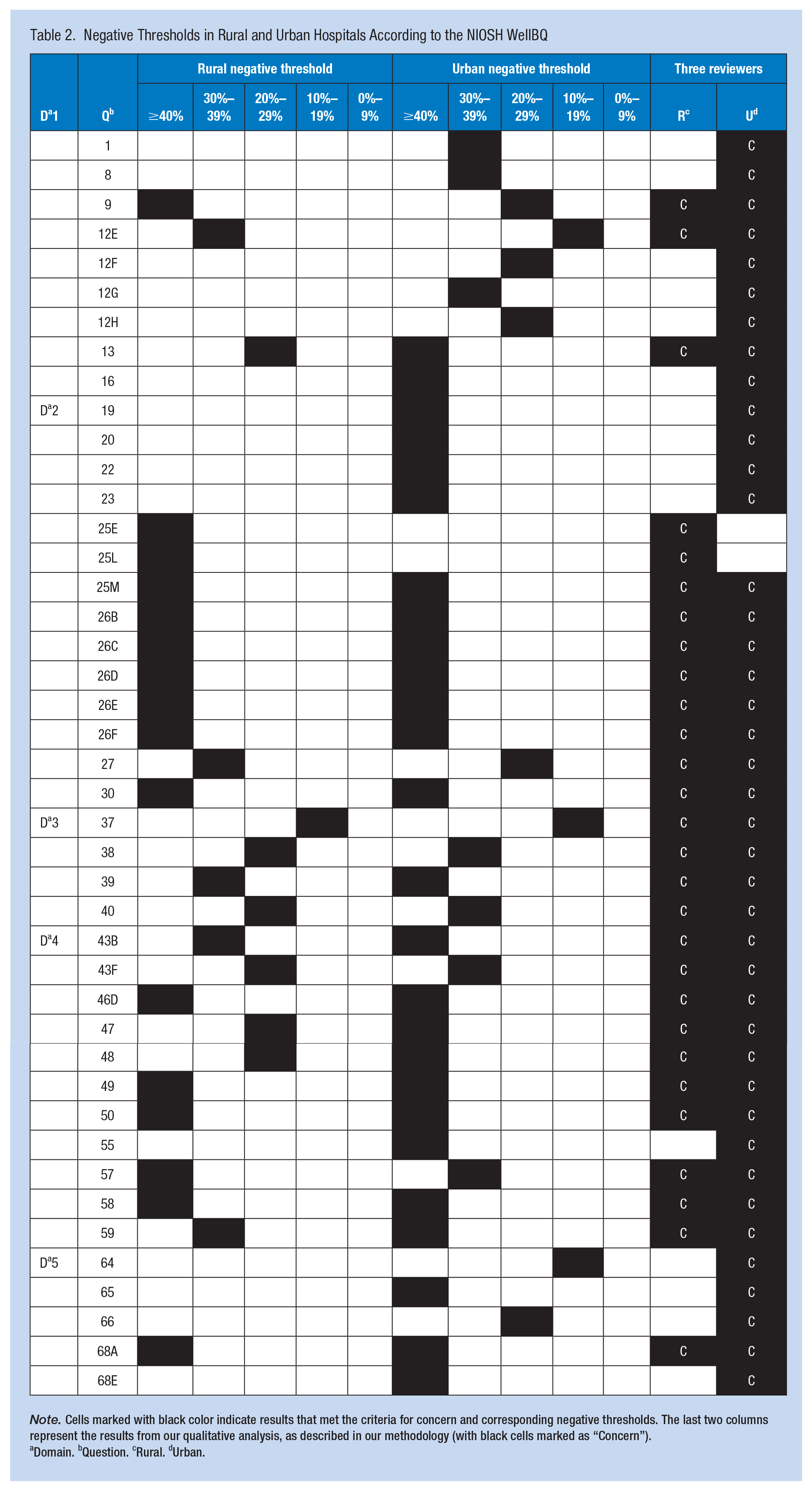
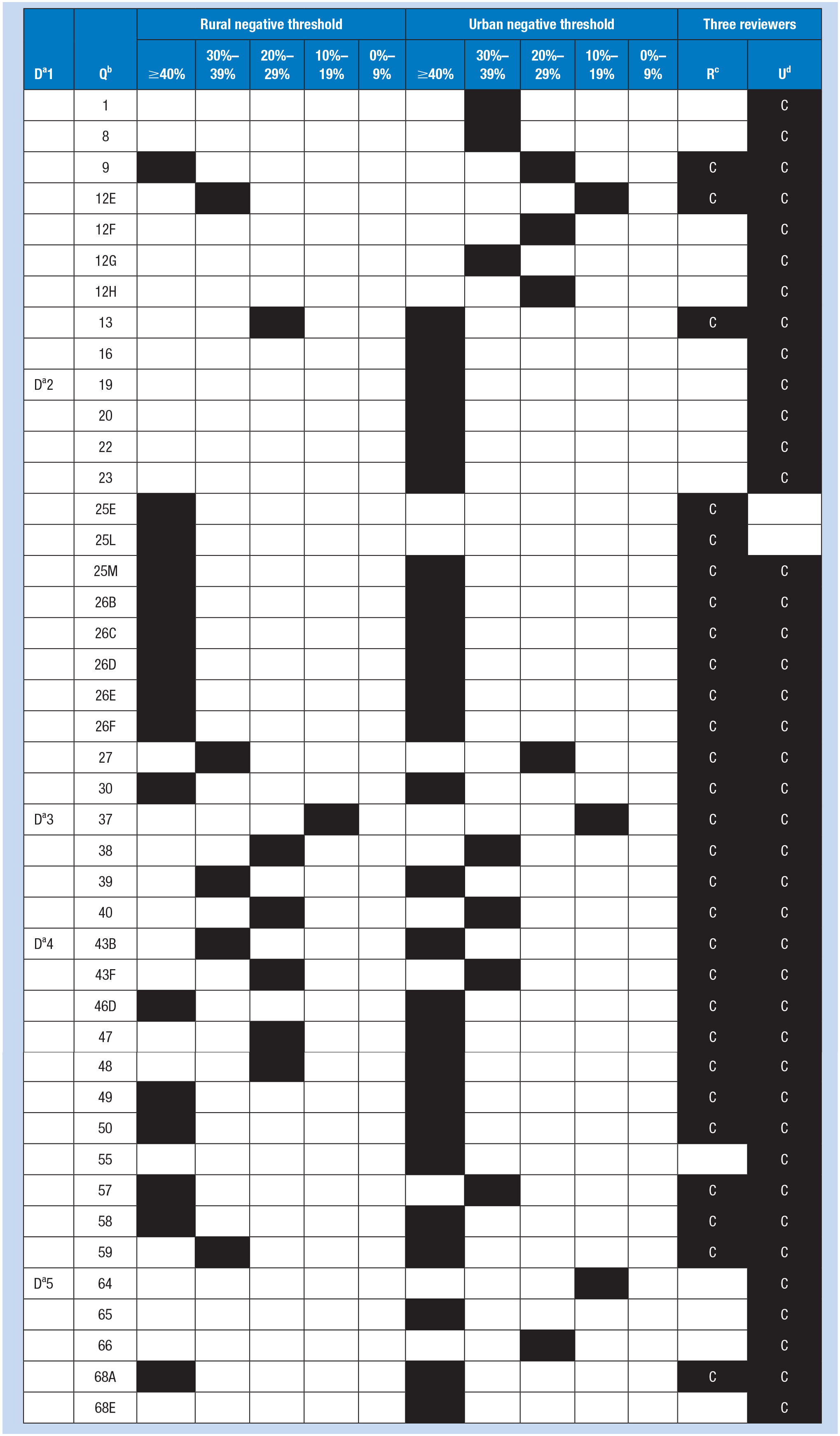
Note. Cells marked with black color indicate results that met the criteria for concern and corresponding negative thresholds. The last two columns represent the results from our qualitative analysis, as described in our methodology (with black cells marked as “Concern”).
Domain. bQuestion. cRural. dUrban.
Domain 1: Work Evaluation and Experience
This domain focuses on work evaluation and experience with a total of 16 items. Of these, three items raised concerns in the rural hospitals, while nine items raised concerns in the urban hospital. Rural participants indicated time paucity and work overload exceeding 40% thresholds, work-related negative affect (anxious) ranging from 30% to 39% thresholds, and work-related fatigue ranging from 20% to 29% thresholds. Conversely, concerning results from the urban hospital revealed work-related fatigue and job engagement exceeding 40% thresholds. For thresholds ranging from 30% to 39%, participants reported concerns about job satisfaction, job autonomy, and work-related negative affect (e.g., gloomy). Additionally, for thresholds ranging from 20% to 29%, participants identified issues with time paucity and work overload.
Domain 2: Workplace Policies and Culture
This domain concentrates on workplace policies and cultures with a total of 14 items. In this domain, 10 items prompted concerns in rural work settings, while 12 items raised concerns in the urban hospital. Concerning results from rural work settings, participants highlighted issues including availability of job benefits (paid paternity leave, transit options, on-site medical care), availability of health programs (on-site fitness center, activity hubs, smoking cessation programs, alcohol/substance programs, stress management programs), and workplace/schedule flexibility. For thresholds ranging from 30% to 39%, participants expressed concerns about work to non-work conflict (interference of job with one’s personal life). In contrast, among participants in the urban hospital, exceeding 40% thresholds were observed in items including: supportive work culture, management trust, health culture at work, availability of job benefits (on-site medical care), availability of health programs (on-site fitness center, activity hubs, smoking cessation programs, alcohol/substance programs, stress management programs), workplace/schedule flexibility. For thresholds ranging from 20% to 29%, participants identified issues with work to non-work conflict (interference of job with one’s personal life).
Domain 3: Workplace Physical Environment and Safety Climate
This domain addresses the workplace physical environment and safety climate with a total of 10 items. Concerns were raised for the same items, totaling four, in both rural and urban hospitals, with slightly different threshold distributions. In the rural hospitals, thresholds of 10% to 19% were noted for work-related sexual harassment, 20% to 29% for work-related physical violence, and 30% to 39% for work-related bullying. Similarly, in the urban hospital, thresholds of 10% to 19% were observed for work-related sexual harassment, 30% to 39% for work-related physical violence, and exceeding 40% for work-related bullying.
Domain 4: Health Status
This domain pertains to health status with a total of 23 items. In the rural hospital, there were concerns raised for 10 items, whereas in the urban hospital, there were 11 items. These concerns were distributed across thresholds exceeding 40% or falling within the range of 30% to 39%. In the rural hospitals, items exceeding 40% included overall stress (work), poor mental health, sleep hours, and feeling sleepy at work. Items within the 30% to 39% threshold included chronic health conditions such as musculoskeletal disorders and depression, as well as limitations in cognitive functioning. Similarly, in the urban hospital, items exceeding 40% encompassed chronic health conditions, overall work-related stress, poor mental health, risky drinking, feeling sleepy at work, and limitations in cognitive functioning. Items within the 30% to 39% threshold included sleep hours.
Domain 5: Home, Community, and Society
This domain focuses on home, community, and society with a total of five items. Concerns were raised about one item in the rural hospitals, while the urban hospital exhibited concerns regarding five items. In the rural hospitals, the item exceeding the 40% threshold was activities outside of work, specifically voluntary or charitable activities. Conversely, in the urban hospital, items exceeding the 40% threshold included financial insecurity and activities outside of work, such as voluntary or charitable activities and training/education courses. Additionally, the item of life satisfaction fell within the 10% to 19% threshold in the urban hospital.
Discussion
In this study, we implemented a three-part methodology for data analysis aimed at identifying concerning well-being items among clinicians in rural and urban hospitals. This approach involved establishing marked thresholds, independent review and resolution of discrepancies by research team members, and validation through focus groups. The results showed that urban hospitals had more concerning thresholds across each domain compared to rural hospitals, with 41 concerning thresholds in urban hospitals versus 28 in rural hospitals, totaling 68 items.
These findings are consistent with previous research. For instance, a study of 382 nurse residents found significant differences in job stress and satisfaction between rural and urban nurses, with rural nurses reporting higher job satisfaction (85.7 vs. 81.2, p = .03) and lower job stress (43.0 vs. 47.6, p = .002; Bratt et al., 2014). Similarly, Yasin et al. (2020) identified differences in job satisfaction related to benefits and job security between rural and urban nurses, which may influence stress levels. Urban healthcare settings, characterized by greater patient volume and resource demands, often lead to increased stress and burnout among nurses (National Center for Health Workforce Analysis, 2024). Furthermore, studies on physicians indicate that those in large cities experience higher job demand and exhaustion with reduced job control, compared to those in smaller towns (Saijo et al., 2013). Additionally, rural physicians report lower rates of burnout (39% vs. 49%, p = .04) and chaotic work environments (40% vs. 52%, p = .01) compared to their urban counterparts (Harry et al., 2024). Given the identified concerns across the domains, targeted interventions are necessary to address the specific challenges faced by clinicians in both urban and rural hospitals. In urban settings, strategies should focus on mitigating work-related fatigue, enhancing job satisfaction and autonomy, and addressing health risks like chronic conditions and risky behaviors. For rural hospitals, interventions should aim to alleviate time constraints, reduce work overload, and improve access to mental health support and workplace flexibility. Tailored approaches will help improve overall well-being and job satisfaction for clinicians in these distinct environments.
In this study, we identified significant concerns regarding work-related sexual harassment, physical violence, and bullying among both rural and urban clinicians. These findings are consistent with existing literature, which highlights the severity of workplace violence in healthcare settings. Nurses face severe challenges, particularly in emergency settings, where Ayasreh and Hayajneh (2021) noted frequent occurrences of verbal abuse and physical assaults due to the high-stress nature of their work. Furthermore, Bambi et al. (2018) found that nurses encounter high levels of workplace incivility, lateral violence, and bullying, which severely impact their job satisfaction and mental health. Similarly, Yusoff et al. (2023) reported that violence against healthcare providers is widespread, with physicians experiencing violence rates from 14.0% to 73.0%, including significant incidents of verbal abuse and threats. Kumari et al. (2020) underscore that physicians are also vulnerable to workplace violence in high-stress areas such as emergency departments and psychiatric units, where patient-led violence is especially prevalent. These findings emphasize that workplace violence is a critical issue for both nurses and physicians, manifesting in different forms and intensities. The severity of violence across these professions highlights the urgent need for comprehensive and targeted interventions tailored to the specific forms of violence experienced by each group. Additionally, experimental studies should explore the effectiveness of targeted training programs, support systems, and policies designed to mitigate the specific types of violence prevalent in different healthcare settings. Longitudinal research is also needed to assess the long-term impacts of workplace violence on clinicians’ mental health and job satisfaction, and to identify best practices for creating safer work environments.
Our results also revealed that items related to overall work stress, poor mental health, chronic health conditions, feeling sleepy at work, and limitations in cognitive functioning exceeded thresholds of either 30% to 39% or 40% in both rural and urban hospitals. This possibly indicates how clinicians in both settings perceived their physical and mental well-being in relation to their work. Elevated work stress and poor mental health are well-documented among healthcare professionals, impacting both job satisfaction and patient safety (Azemi et al., 2022; Jun et al., 2021; Labrague et al., 2018). Chronic health conditions related to stress can further exacerbate these issues, contributing to higher rates of absenteeism and reduced work efficiency (Frey et al., 2015; Goh et al., 2015). Additionally, sleep deprivation and its effects on cognitive functioning are significant concerns, as inadequate rest impairs decision-making and performance in healthcare settings, such as medication administration errors (Bell et al., 2023; Rogers et al., 2004; Zhao et al., 2023). These findings underscore the urgent need for targeted interventions and further research to address these challenges and improve clinician well-being across various healthcare environments (Kelly et al., 2021; Shanafelt et al., 2012). For example, studies could investigate the effectiveness of tailored wellness programs, improved work conditions, and strategies to enhance sleep quality and cognitive functioning. Additionally, longitudinal research is needed to assess the long-term impacts of these stressors on clinician health and job performance. Exploring these areas will be crucial in developing comprehensive strategies to support clinician well-being and improve patient care outcomes.
Understanding these findings requires considering the demographic composition of the study participants, as it reflects the broader characteristics of the healthcare workforce. The majority of participants in this study were female and Caucasian, with over two-thirds being nurses. These demographic characteristics reflect broader national trends in the nursing workforce, where the majority are female and White/Caucasian (American Association of Colleges of Nursing, 2024; National Center for Health Workforce Analysis, 2024; Smiley et al., 2023). These findings provide valuable insights into the well-being of clinicians in rural and urban settings, contributing to a deeper understanding of workforce dynamics in healthcare environments.
Limitations
This study has several limitations. First, the use of a cross-sectional design and data collection from only one urban and three rural hospitals restricts the generalizability of the results. Second, the small sample size (n = 222), predominantly female (n = 176) and Caucasian (n = 184), limits the diversity of perspectives captured. Third, data collection occurred from September to December 2022, during a period when clinicians were still managing the heavy workloads associated with the COVID-19 pandemic. During this time, they were also subjected to multiple similar surveys assessing work-related stress and job satisfaction. The relatively lengthy nature of our survey may have further burdened these already busy healthcare professionals, potentially contributing to a low response rate. Lastly, a limitation is related to our methodology for evaluating concerning responses. We categorized the data into five threshold ranges (0%–9%, 10%–19%, 20%–29%, 30%–39%, and over 40%) to provide a gradient of concern. While this approach was considered reasonable by consensus among researchers, it may not be the most optimal way to categorize concern levels. Alternative methods or threshold ranges might better capture the nuances in clinician well-being data. Future research should consider reducing the number of survey items to better accommodate clinicians’ workloads. Additionally, studies should aim to include larger and more representative samples for a more comprehensive analysis of clinician well-being across both rural and urban settings. Longitudinal studies are also needed to uncover causal relationships among the factors influencing clinician well-being.
Implications for Occupational Health Practice
The findings of this study have significant implications for occupational and environmental health practice across various healthcare settings. First, the methodology used to identify concerning thresholds for clinician well-being underscores the need for developing specific benchmarks that can be applied by occupational health practitioners in collaboration with healthcare administrators, policymakers, and community organizations. These benchmarks can guide the early identification of distress among clinicians and facilitate timely interventions to mitigate these concerns. For example, occupational health practitioners can partner with local organizations, such as community mental health centers or professional associations (e.g., American Nurses Association [ANA], National Association for Healthcare Quality [NAHQ], United Way Partners), to enhance support systems in high-stress areas like emergency departments. In rural settings, practitioners could collaborate with telehealth providers or local non-profits to develop tailored mental health resources for clinicians in regions with limited access to care.
Second, the findings highlight the importance of addressing workplace stressors unique to urban and rural settings, particularly in relation to job demands, mental health, and workplace violence. Occupational health practitioners should advocate for and implement targeted interventions that consider these distinct needs. For example, programs like the American Hospital Association’s (AHA, 2018) Hospitals Against Violence (HAV) Initiative provide resources to create safer work environments by promoting education, awareness, and multidisciplinary collaboration. Similarly, the Occupational Safety and Health Administration’s (OSHA, 2015) Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers outline key strategies, including hazard identification, training, and employee participation, to reduce violence risks. In high-risk environments like urban emergency departments, interventions could include de-escalation training, on-site security personnel, and the establishment of anonymous reporting systems, modeled after programs endorsed by The Joint Commission’s Workplace Violence Prevention Resources (The Joint Commission, 2022). For rural settings, where access to resources may be limited, practitioners could collaborate with telehealth services or community organizations to provide mental health support and violence prevention training remotely. Practitioners should also work with institutional leaders to equip healthcare workers with tools to recognize, report, and manage incidents of workplace violence, such as those advocated by the American Organization for Nursing Leadership (AONL) and Emergency Nurses Association (ENA) Toolkit for Mitigating Violence in the Workplace (American Organization for Nursing Leadership & Emergency Nurses Association, 2022). By leveraging these established programs and tailoring them to the specific risks faced by nurses and physicians in different environments, occupational health practitioners can improve overall safety and well-being in healthcare settings.
Finally, the study’s findings emphasize the need for comprehensive wellness programs within healthcare organizations. Occupational health practitioners should take a leadership role in designing and implementing these programs, leveraging established models such as the AMA’s Steps Forward® Well-Being Program, which provides resources to reduce burnout, promote resilience, and enhance work-life balance among healthcare professionals (American Medical Association, n.d.). For example, initiatives like structured peer-support programs, such as the Schwartz Rounds, enable clinicians to openly discuss the emotional and social challenges of their work, fostering a culture of mutual support (The Schwartz Center, n.d.). To address sleep quality and cognitive functioning, programs like Center for Work and Fatigue Research by the NIOSH can offer evidence-based strategies, including scheduling guidelines to minimize fatigue and cognitive impairments (NIOSH, 2024b). Additionally, introducing flexible scheduling and mandatory rest periods, modeled after practices in high-reliability organizations, can reduce clinician burnout and improve performance. Collaborative efforts with hospital administrators and employee wellness teams can further amplify these efforts. For instance, incorporating Employee Assistance Programs (EAPs) that provide confidential counseling and mental health services, or integrating digital wellness platforms can ensure accessibility and scalability. By addressing these areas with proven strategies and collaborative initiatives, occupational health practitioners can significantly contribute to improving clinician well-being and patient care outcomes across diverse healthcare settings.
Conclusion
This study demonstrates the effectiveness of our three-part methodology—establishing thresholds, resolving discrepancies through independent reviews, and validating findings via focus groups—in identifying concerning well-being issues among clinicians in both rural and urban hospitals. Our results show that urban hospitals present more concerning thresholds than rural hospitals, consistent with existing research on job demands and burnout disparities. The study highlights the urgent need for targeted interventions tailored to the specific challenges of these settings, especially in addressing higher job stress, lack of diversity, and workplace violence. While these findings offer valuable insights, the study’s limitations, including its cross-sectional design, small sample size, and low survey response rate—likely influenced by the COVID-19 pandemic—underscore the need for further research. Future studies should refine well-being thresholds, explore the factors contributing to workplace violence and financial insecurity, and assess the long-term effects of these stressors. Additionally, incorporating more representative and diverse samples and utilizing longitudinal designs will better illuminate and address clinician well-being. Advancing this research is essential for developing more effective support strategies and policies to enhance clinician well-being and patient care across various healthcare settings.
Applying Research to Occupational Health Practice
This study reveals significant well-being disparities between rural and urban clinicians, particularly in areas such as job stress, mental health, and workplace violence. Occupational health practitioners must recognize the contextual differences between rural and urban settings, understanding that different approaches are required for each environment. In urban settings, where higher thresholds of concern were identified, interventions might focus on mitigating job stress and addressing workplace violence. In contrast, rural settings may require strategies that enhance access to mental health resources and support systems due to their limited availability. By applying specific benchmarks to monitor clinician well-being, occupational health practitioners can implement timely, tailored interventions that reflect the unique challenges of each setting. Moreover, promoting diversity and developing comprehensive wellness programs are essential for improving clinician well-being and patient care outcomes across these diverse healthcare environments. Understanding and addressing these contextual differences is crucial for effective occupational health practice.
Footnotes
Author Contributions
NL, LM, MB, BE, and KA contributed to the conception and design of the work. All authors contributed to the analysis and interpretation of data for the work. The manuscript was drafted by NL, LM, MB, KA, BE, and JB and approved by all authors.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute for Occupational Safety and Health (NIOSH 1U19OH012303).
Ethical Approval and Consent to Participate
This study was approved by the institutional review board (#21-2592) at the University of North Carolina. Written permission to conduct the study was obtained from the administrator in each participating hospital. An informed consent procedure was used with all study participants.
Availability of Data and Materials
The datasets are available from the corresponding authors on request.