
Abstract
Background:
Returning to work (RTW) is a crucial aspect of recovery for patients with breast cancer (BC), which indicates restored normalcy, financial stability, functional abilities, and an improved quality of life. However, associated factors related to not RTW among patients with BC remain unclear. In this study, we examined associated factors of not RTW among patients with BC.
Methods:
A cross-sectional study and convenience sampling were conducted in two hospitals in Indonesia to recruit eligible participants. Factors related to not RTW were collected and included symptoms of distress, loneliness, anxiety/depression, perceived social support, and frailty. A logistic regression model was performed to explore associated factors of not RTW.
Findings:
In total, 250 patients with BC were included in this study, and 148 of them experienced not RTW. Anxiety, loneliness, frailty, and social support emerged as significant factors associated with not RTW. BC patients who had a higher anxiety level (odds ratio [OR]: 5.30; 95% confidence interval [CI] [2.16, 12.98]), had high loneliness (OR: 3.15, 95% CI [1.29, 7.67]), or were frail (OR: 2.53; 95% CI [1.07, 5.98]) had a higher risk of not RTW. BC patients with lower social support (OR: 5.65; 95% CI [1.81, 17.63]) had a higher risk of not RTW.
Conclusion/Applications to Practice:
Occupational health professionals can offer early counseling, health education, and support strategies to patients with BC, assisting their preparations in terms of both physical and psychological functions for successfully RTW.
Background
Breast cancer (BC) is a prevalent cancer and the leading cause of death among the female population globally (Sung et al., 2021). According to data from the United States Census Bureau from 1975 to 2007, approximately 70.0% of women were diagnosed as having BC among working-age adults under 64 years of age, making this a significant concern for the workforce (De Moor et al., 2013). A recent review article also reports a significant increase in breast cancer incidence among young women (20–49 years; Xu et al., 2024). Previous studies revealed that patients with BC experienced challenges in returning to work (RTW) after cancer treatment (Hou et al., 2021). In addition, patients with BC have a 1.42-fold higher risk of unemployment than the general population (Choi & Lee, 2023). On average, non-RTW rates within 1 year after a BC diagnosis range from 5.0% to 58.0% (Islam et al., 2014). Return to work symbolizes recovery and healing, allowing BC patients to regain a sense of normalcy (Hou et al., 2021; Sheppard et al., 2019). Patients can rebuild social relationships, increase their self-esteem, and maintain financial stability during and after cancer treatment (Ferlay et al., 2015; Hauglann et al., 2012). Those who are incapable of RTW may experience adverse psychological impacts, including anxiety, and reduced motivation and life expectancy (Nachreiner et al., 2012). Moreover, those who do not work may be more vulnerable to financial hardships (Meernik et al., 2021). Thus, the assessment and facilitation of RTW among BC patients represent critical concerns in cancer care.
Return to work is defined as a person’s return to their job full-time, resuming the same hours and work responsibilities as they had prior to their sickness-related absence (Ersel et al., 2022). Previous studies measured RTW through work ability, using a single question “How many points would you give your current work ability” scored on scale from 0 to 10 (Tay et al., 2024), or by simply asking “Are you currently working?” with a “yes” or “no” response (Magnavita et al., 2024). However, those studies primarily focused on the work status of patients with BC rather than them successfully RTW. Since RTW early is associated with improved survival rates (Yang et al., 2021), investigating successfully RTW, which includes returning to a full-time job and resuming the same hours and work responsibilities 6 months after a cancer diagnosis or treatment, is critical for patients with BC. Identifying potential facilitators or barriers to RTW early may enable implementation of more appropriate and timely interventions, thereby supporting patients with BC in early and successfully RTW.
Various risk factors related to RTW comprise unmodifiable factors including age, marital status, educational level, cancer stage, and disease duration (Bjørkedal et al., 2023; Su et al., 2018) and modifiable factors such as fatigue, pain, anxiety, and depression (Bjørkedal et al., 2023; Carlsen et al., 2013; Ersel et al., 2022). Recent studies found that loneliness and frailty are critical factors that contribute to negative consequences in cancer patients (Çamlıca & Koç, 2024; M. Su et al., 2022). Loneliness was correlated with job loss and was a predictor of unemployment in a working-age adult population (Morrish & Medina-Lara, 2021; Morrish et al., 2022). Loneliness can lead to a reduced sense of connection with coworkers and a lack of social interactions. Additionally, frailty contributes to unemployment, as women with frailty reported a low ability to work and struggled with the physical demands of job responsibilities (Palmer et al., 2017). However, these issues related to RTW have not been examined in BC patients.
Patients with breast cancer in developing countries such as Indonesia may experience stigmatization and social discrimination due to a BC diagnosis and body image disturbance caused by breast removal (Prates et al., 2017; Thakur et al., 2022; Tisnasari et al., 2022). Additionally, treatment-related side effects such as hair loss, skin changes, nausea, and fatigue reduce the motivation of BC patients to engage in social activities (Tao et al., 2015). Those with perceived stigmatization may experience embarrassment and unkindness, and are often blamed for their condition, which further decreases the motivation of RTW (Molina et al., 2013; Ninnoni et al., 2023). Since few studies have investigated risk factors of not RTW among BC patients in developing countries, particularly in Indonesia. In this study, we examined risk factors related to not RTW among BC patients. By identifying demographic and disease characteristics, psychological factors, and frailty that contribute to not RTW, the study sought to provide a comprehensive understanding of barriers these patients face. This information will inform the development of targeted interventions to support patients with BC in RTW.
Methods
Study Design and Participants
A cross-sectional study using convenience sampling was conducted from August 1 to October 31, 2023, to recruit participants. All participants were recruited from outpatient departments of two hospitals in Indonesia during their regular follow-up visits. The inclusion criteria were: (1) female aged 20 to 60 years (as 60 years is the official retirement age), (2) having been diagnosed with BC for at least 6 months, and (3) being able to effectively communicate in Indonesian. Individuals with cognitive impairment or psychiatric disorders (e.g., schizophrenia, psychosis, or depression), as assessed by a physician and documented in medical records, were excluded to prevent potential bias in psychological assessments. Additionally, those who were unemployed prior to their BC diagnosis were also excluded from the study.
The required sample size was determined based on established parameters: a two-sided α of .05, a power of 0.80, and a small to moderate effect size of 0.18 to 0.20 between risk factors and not RTW being small to moderate (Cohen, 1988). Consequently, 250 patients with BC were needed in this study.
Measurements
Demographics and Disease Characteristics
The following demographic characteristics were included in this study: age, marital status, educational level, and number of children. Disease characteristics such as cancer stage and disease duration were also recorded.
Returning to Work (RTW)
RTW was defined as successful when a BC patient had fully resumed her work responsibilities following her cancer diagnosis and treatment (Ersel et al., 2022). In this study, RTW was defined as reengagement of a BC patient in either part-time or full-time employment for a duration exceeding 6 months. Conversely, the non-RTW group was defined as BC patients who discontinued working or abstained from RTW following their BC diagnosis and treatment.
Symptom Distress
Symptom distress was assessed using the Symptom Distress Scale (McCorkle & Young, 1978). This scale comprises 13 items, including nausea (frequency and intensity), appetite, insomnia, pain (frequency and intensity), fatigue, bowel patterns, concentration, appearance, breathing, outlook, and coughing. Scoring uses a 5-point Likert scale, ranging from 1 (indicating no distress) to 5 (signifying extreme distress). Total scores range 13 to 65 with a higher score indicating a greater level of symptom distress. The original Symptom Distress Scale demonstrated acceptable internal reliability with a value of 0.82 (McCorkle et al., 1998; McCorkle & Young, 1978). The internal reliability of the scale in this study was 0.80, indicating acceptable internal consistency.
Loneliness
Loneliness is an unpleasant emotional response as a feeling of being alone due to a lack of social relationships or a mismatch between social relationships and individual expectations (Russell et al., 1980). The Indonesian version of the UCLA Loneliness Scale with 18 items was used to assess an individual’s perceptions of loneliness experiences. Participants were asked to rate their feelings on a 4-point Likert scale comprising 1 (never), 2 (rarely), 3 (sometimes), and 4 (always), with a higher score indicating greater loneliness (Fauziyyah & Ampuni, 2018). According to the responses, total scores were divided into two groups: low loneliness (≤36 points), indicating participants who never or rarely experienced feelings of loneliness, and high loneliness (>36 points), including participants who reported they sometimes or always felt lonely. Cronbach’s alpha of the Indonesian UCLA Loneliness scale in a previous study was .87 (Fauziyyah & Ampuni, 2018), and it was .92 in the current study, indicating acceptable internal reliability.
Anxiety and Depression
Anxiety is a nervous or worried feeling about current or potential events, while depression is characterized by a diminished mood or loss of pleasure in activities (Zigmond & Snaith, 1983). In this study, the Indonesian version of the Hospital Anxiety and Depression Scale (HADS) was utilized to assess levels of anxiety and depression. The HADS comprises 14 items with seven items focused on anxiety assessment and seven items on depression. Each item is rated on a 4-point Likert scale (0 = not at all to 3 = most of the time). Total subscale scores for anxiety and depression are evaluated as low (0–7) or high (8–14) anxiety and depression (Zigmond & Snaith, 1983). The Indonesian version of the HADS demonstrated satisfactory internal reliability, with respective Cronbach’s alpha coefficients of .80 and .81 for the anxiety and depression subscales in this study.
Social Support
Social support can be described as the perceived or actual instrumental and expressed support by the community, social networks, and confiding partners (Zimet et al., 1988) and was measured using the Indonesian version of the Multidimensional Scale of Perceived Social Support (MPSS). The MPSS is a 12-item scale assessing self-perceived social support from three specific sources: friends (four items), family (four items), and significant others (four items; Laksmita et al., 2020; Zimet et al., 1988). Each item is rated on a 7-point Likert-type scale from very strongly disagree (1) to very strongly agree (7), with a total score ranging 12 to 84. Social support was categorized into three categories: low, moderate, or high social support. The Indonesian version of the MPSS had acceptable reliability with Cronbach’s alpha of .85 (Laksmita et al., 2020). Cronbach’s alpha in this study was .92, indicating acceptable internal reliability.
Frailty
Frailty is characterized by loss of physical, cognitive, and/or psychosocial resources and functions, resulting in an individual’s inability to effectively handle stressors (Schuurmans et al., 2004). Frailty was assessed using the Groningen Frailty Indicator (GFI). The GFI evaluates the loss of function and resources across four domains: physical (encompassing mobility functions, multiple health problems, physical fatigue, vision, and hearing), cognitive (assessing cognitive functioning), social (evaluating emotional isolation), and psychological (addressing mood and feelings of anxiety). Responses were categorized as two levels: 1 indicating the presence of a problem or dependency and 0 indicating the absence of such problems. The total GFI score ranges 0 to 15, with a score of ≥4 points considered to indicate frailty (Bielderman et al., 2013; Steverink, 2001). The original GFI demonstrated a Cronbach’s alpha value of .73 (Bielderman et al., 2013), and the Indonesian GFI scale exhibited an acceptable level of internal reliability with Cronbach’s alpha of .70.
Data Collection
The study received approval from two institutional review boards of Taipei Medical University (approval no. N202206028) and Central General Hospital, Dr. M. Djamil Padang (approval no. LB.02.02/5.7/129/2022). All participants provided written consent after receiving a comprehensive explanation of the study objectives and their rights. All participants underwent face-to-face interviews, each lasting approximately 20 min, conducted by the principal researcher to complete questionnaire data collection. Each questionnaire was thoroughly reviewed to ensure that there were no missing data before the interview was terminated.
Data Analysis
Statistical analysis was performed using SPSS v. 22 software (IBM, Armonk, NY, USA). Results are presented as percentages for categorical data, and the mean and standard deviation (SD) for continuous variables. A Chi-squared test and independent t-test were used to examine relationships of demographics with disease characteristics, loneliness, anxiety, depression, social support, frailty, and the RTW status. To determine risk factors related to RTW in BC patients, univariable logistic regression models were used to examine the relationship between each risk factor (i.e., age, marital status, educational level, number of children, employment status, cancer stage, duration of disease, symptom distress, loneliness, anxiety/depression, social support, and frailty) and RTW. Independent variables with p ≤ .20 were selected for a further multivariate logistic analysis (Mickey & Greenland, 1989). Multivariate logistic regressions were used to identify risk factors for RTW, and results are presented as odds ratios (ORs) with 95% confidence intervals (CIs). Statistically significance was set to two-tailed p ≤ .05.
Results
Demographic and Disease Characteristics
In total, 250 women with BC who participated in this study had an average age of 47.23 ± 7.40 years with 2.46 ± 1.17 mean number of children and an average duration of disease of 35.12 ± 27.37 months (7 months to 5 years). Most women were married (80.8%), and 201 women had a senior high school, bachelor’s, master’s, or doctorate educational level (80.4%). More than half (56.4%) of the women had been diagnosed with stage III or IV BC.
RTW Status, Loneliness, Anxiety/Expression, Social Support, and Frailty
The percentage of women who did not experience RTW was 59.2%, with a mean symptom distress score of 22.67 (SD = 5.35). Nearly half (46.0%) of the women experienced a high level of loneliness, 52.4% had high anxiety, and 26.0% had high depression levels. Among non-RTW participants, approximately 27.6% reported receiving low social support and 56.8% exhibited frailty (Table 1).
Demography and Disease Characteristics, Symptom Distress, Loneliness, Anxiety and Depression, Perceived Social Support, Frailty, and Return to Work (N = 250)
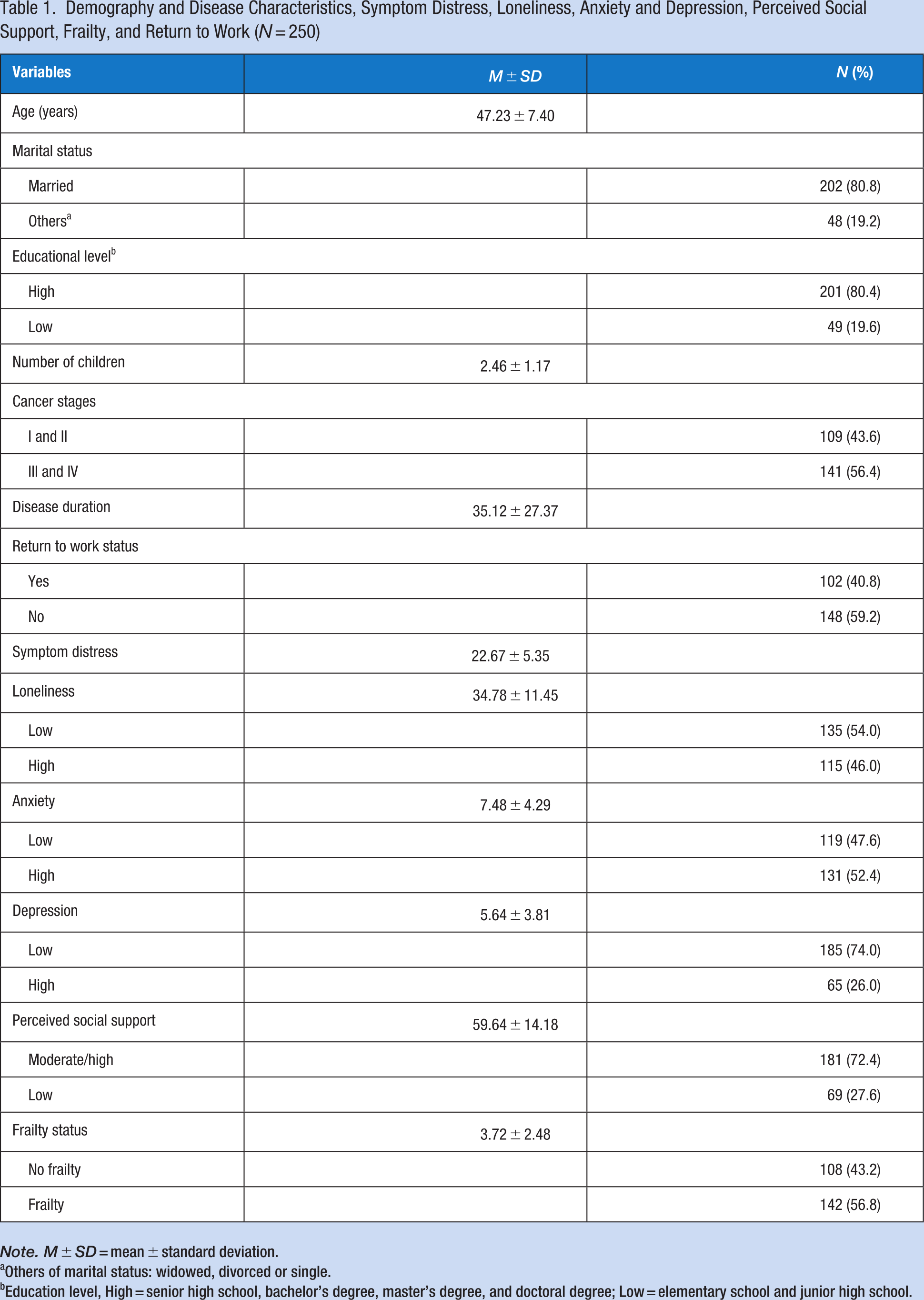
Note. M ± SD = mean ± standard deviation.
Others of marital status: widowed, divorced or single.
Education level, High = senior high school, bachelor’s degree, master’s degree, and doctoral degree; Low = elementary school and junior high school.
Correlations of Demographic and Disease Characteristics, Loneliness, Anxiety/Depression, Social Support, and Frailty With RTW
Table 2 shows that the RTW and non-RTW groups did not differ in age, marital status, number of children, or disease duration. There were significant relationships of the educational level and cancer stages with RTW (p ≤ .001). Significant correlations were found of symptom distress, loneliness, anxiety/depression, social support, and frailty with RTW among women with BC (p ≤ .001). Almost 80% of women who did not experience RTW were married, had a low educational level (27.7%), and were at the III or IV cancer stage (73.0%). Women who did not experience RTW presented a higher score for symptom distress (mean = 23.6, SD = 4.43), two-thirds (66.9%) had experienced a high level of loneliness, three-quarters (74.3%) had high anxiety, over one-third had high depression (38.5%), less than half (42.6%) perceived low social support, and 77.7% experienced frailty.
The Association Between Demography and Disease Characteristics, Symptom Distress, Loneliness, Anxiety and Depression, Perceived Social Support, Frailty, and Return to Work (N = 250)
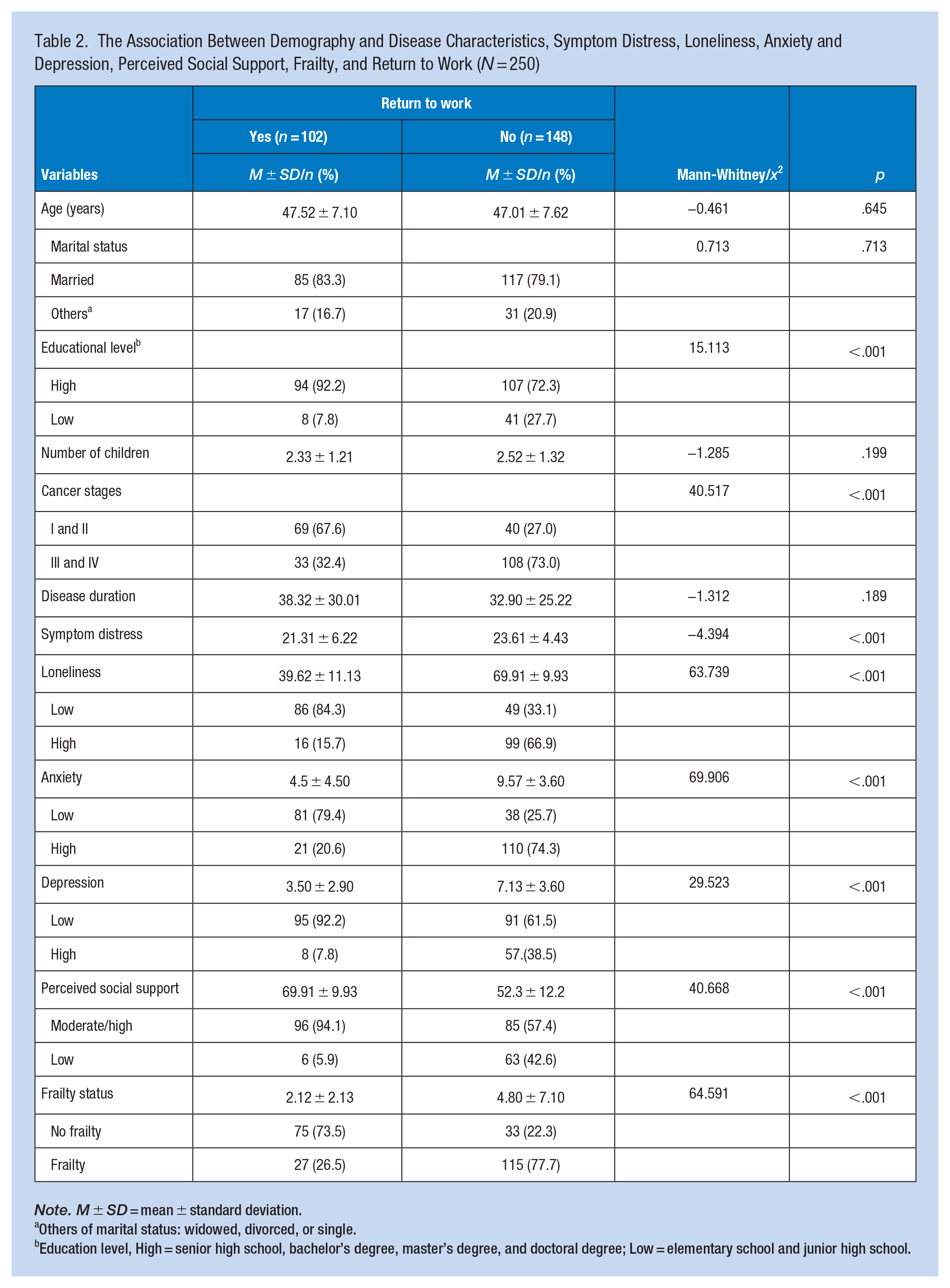
Note. M ± SD = mean ± standard deviation.
Others of marital status: widowed, divorced, or single.
Education level, High = senior high school, bachelor’s degree, master’s degree, and doctoral degree; Low = elementary school and junior high school.
Determinants of RTW
Table 3 shows that women who had a low educational level and had been diagnosed with stage III or IV cancer were more likely not to experience RTW compared to BC patients with a high educational level and in the early stages of BC. Patients with BC who had high loneliness, high anxiety and depression, were receiving low social support, and exhibited frailty were also more likely not to experience RTW (p ≤ .001).
Predictor of the Return to Work Among Patients With Breast Cancer: Logistics Regression Model
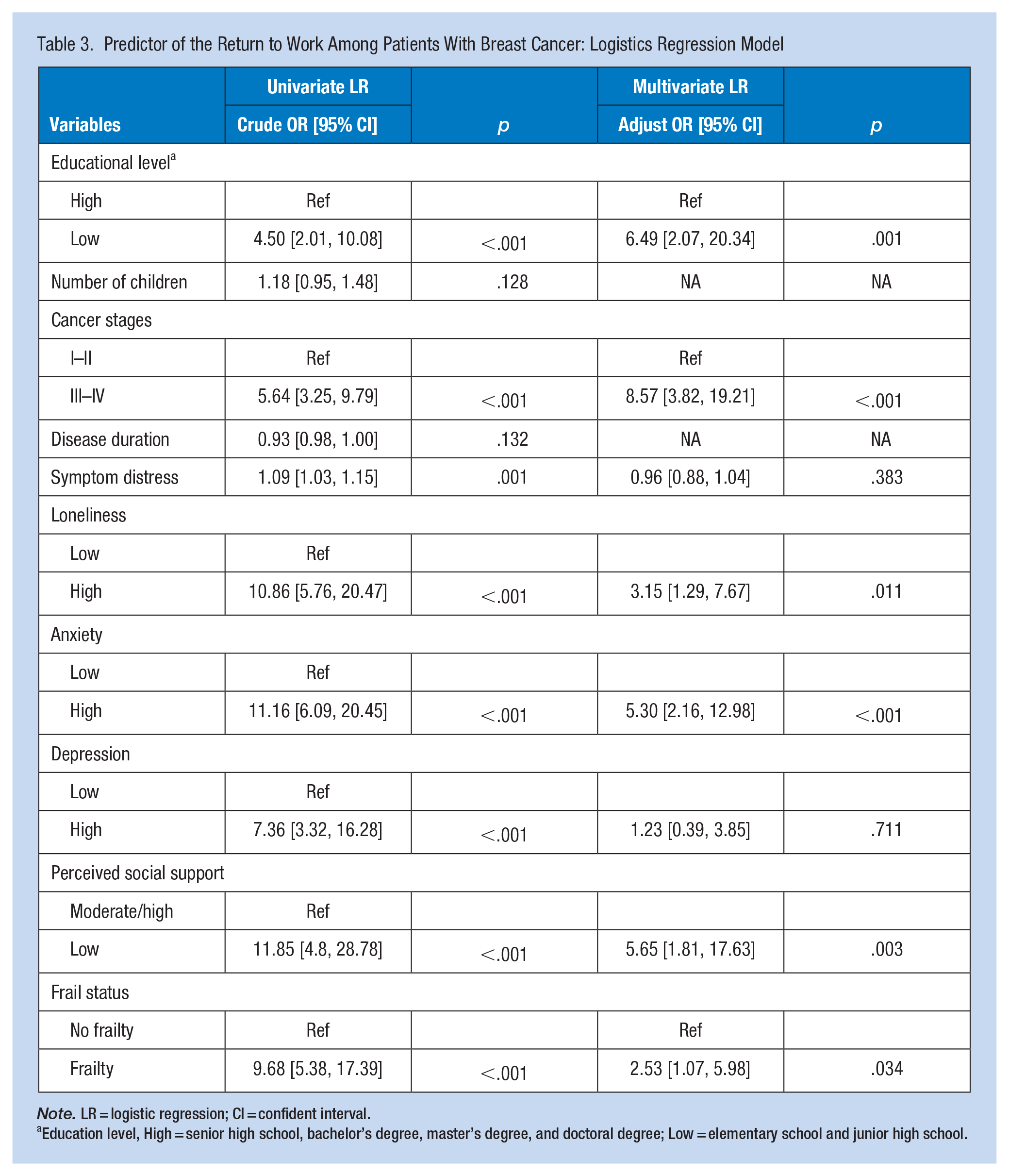
Note. LR = logistic regression; CI = confident interval.
Education level, High = senior high school, bachelor’s degree, master’s degree, and doctoral degree; Low = elementary school and junior high school.
The multivariate analysis showed that several factors were significant determinants of not RTW. Patients with BC with lower educational levels had a 6.49 (95% CI [2.07, 20.34])-fold higher probability of not RTW after their cancer diagnosis. Those diagnosed with cancer stage III or IV were at an 8.57 [3.82, 19.21]-fold higher risk of not RTW compared to those with earlier stages. Patients who perceived having low social support had a 5.65 [1.81, 17.63]-fold higher risk of not RTW compared to patients receiving high social support. Patients with BC who had high levels of anxiety had a 5.30 [2.16, 12.98]-fold higher probability of not RTW compared to patients with low anxiety levels. Patients who were experiencing a high level of loneliness had a 3.15 [1.29, 7.67]-fold higher risk of not RTW, and those exhibiting frailty had a 2.53 [1.07, 5.98]-fold higher probability of not RTW compared to their counterparts. No significant association was found between symptom distress or depression and RTW (Table 3).
Discussion
Our findings showed that 59.2% of patients with BC did not experience RTW after their cancer treatments. Those BC patients who experienced frailty, high anxiety and loneliness, and low social support had a high probability of not RTW. The prevalence of not RTW (59.2%) was higher than previous meta-analytical findings for not RTW among BC survivors in the United States and the Netherlands at 7% to 57% (Islam et al., 2014). In Indonesian culture, BC patients may be labeled as suffering persons and experience social discrimination (Tisnasari et al., 2022). They may endure feelings of embarrassment, being treated unkindly, and being avoided and blamed (Ninnoni et al., 2023). Moreover, previous studies focused on assessing RTW as based on work ability or work limitations (Magnavita et al., 2024; Tay et al., 2024). The definition of RTW in this study was that BC patients could effectively resume their job responsibilities at least 6 months after treatment. Most cancer survivors worry about their capability of RTW due to side effects of cancer treatments and the workload (van Egmond et al., 2017), which may reduce the motivation of RTW. Since RTW represents a sense of overall well-being and is an important determinant of one’s quality of life (Hou et al., 2021; Nilsson et al., 2013; Sheppard et al., 2019), suitable strategies for assisting those patients with BC in RTW should be imperative in cancer care.
Anxiety and RTW
Our study revealed that BC patients with high anxiety levels were more likely not to experience RTW. This aligns with a previous study that found that cancer patients who were not RTW had higher levels of anxiety than patients who were RTW (Lieb et al., 2022). Anxiety in BC patients is related to cancer treatments, the possibility of cancer recurrence after treatment, and a fear of death (Baqutayan, 2012; Tiedtke et al., 2012). A feeling of anxiety may cause cancer patients to fail to start planning for their future life such as RTW (van Egmond et al., 2017). Additionally, BC patients may doubt that they will be accepted in the workplace after RTW (Tiedtke et al., 2012). Thus, early assessment and management of anxiety are important care strategies for patients with BC.
Social Support and Loneliness With RTW
Results showed that BC patients who were receiving low social support and were experiencing a high level of loneliness were more likely not to be RTW. Cancer patients who were receiving low social support during their cancer treatment experienced uncertain feelings, were less proactively self-controlled, and had negative self-esteem (Pasek et al., 2021), which might reduce their confidence and motivation for RTW. Conversely, individuals with a high level of loneliness tend to experience feelings of rejection and perceive less respect from their coworkers or supervisors, leading to social isolation and negative self-esteem (Rokach, 2014). Furthermore, the reduction in workplace connections and social interactions might decrease the motivation to continue their jobs, and thus they were not RTW (Basit & Nauman, 2022; Jung et al., 2021; Kaymaz et al., 2014). Consequently, offering sufficient social support and addressing loneliness at an early stage are crucial for BC patients. Implementing appropriate methods during the initial stages of cancer treatment, such as counseling or supportive services, to enhance social support and alleviate loneliness should be contemplated.
Frailty and RTW
Our findings indicated that patients with BC who experienced frailty were more likely not to be RTW. Similarly, a previous study reported that individuals with frailty had a higher probability of leaving their job or not RTW (Palmer et al., 2017). The pathogenesis and inflammation of cancer can cause aging-associated declines in reserves of physical and psychological functions that would increase the risk of frailty symptoms (Xue, 2011; Q. Zhang et al., 2023). Women grappling with frailty often report leaving their job, taking prolonged sick leave, and facing physical limitations (Palmer et al., 2017). Thus, frail people experience reduced physical capabilities and energy levels, and difficulties with concentration and decision-making which influence their ability to sustain employment. Since frailty is related to a poor health-related quality of life and risk of mortality among patients with cancer (M. Su et al., 2022; D. Zhang et al., 2022), early screening and preventive interventions such as suitable physical activity and nutrition supplementation to improve frailty are critical for better outcomes in BC patients.
Education and RTW
A low educational level was a significant risk factor for not RTW in patients with BC. Survivors with an educational level of junior high school or below had a higher probability of not RTW after a BC diagnosis compared to those RTW (OR: 6.49, 95% CI [2.07, 20.34]). In our study, 27.7% of survivors had a low educational level in the non-RTW group, while only 7.8% had the same level in the RTW group. Lower educational attainment may limit job opportunities, especially in roles accommodating post-cancer physical and emotional challenges, and may present socioeconomic barriers, such as inadequate access to flexible work, financial resources, and social support, further hindering RTW (Kemp et al., 2021). Moreover, a lower education is associated with lower health literacy and reduced access to information about support services, which can affect a survivor’s confidence and readiness to reenter the workforce (Föhner et al., 2024). Therefore, cancer care should include targeted management and support strategies to facilitate RTW by vulnerable individuals with a low level of education.
Symptoms Distress and RTW
Our study revealed a significant difference in average symptom distress scores between individuals RTW and those not doing so (23.61 ± 4.43 vs. 21.31 ± 6.22). However, symptom distress was not identified as a significant risk factor for RTW in the multivariate logistic regression model, suggesting that it might not directly influence the decision or ability to return to work when other factors, such as social support, loneliness, anxiety, and frailty, are considered. A follow-up study indicated that changes in overall symptom distress were significantly predicted by state anxiety, health professional support, and time since the cancer diagnosis (Liao et al., 2015). Additionally, social support is crucial in helping BC survivors manage distress (Lee & Kim, 2018). Therefore, implementing strategies such as enhancing social support to reduce symptom distress and facilitating RTW is recommended. Further research is needed to clarify these relationships.
Limitations
Some limitations should be kept in mind when interpreting the current findings. First, temporal ambiguity between these factors and non-RTW could not be confirmed due to the cross-sectional study design. Second, all study participants were recruited from only two hospitals in an urban area of Indonesia which limits the generalizability of the findings. Finally, although we investigated comprehensive risk factors for non RTW, other risk factors, such as workplace support from supervisors and colleagues (Sohn et al., 2021), and stigmas and discrimination in the workplace (Stergiou-Kita et al., 2017), were not examined in this study. Future research could be conducted to clarify the correlations of these factors (i.e., stigmas, discrimination and social supports from workplace) with non-RTW in patients with BC.
Conclusions
This study found that anxiety, loneliness, frailty, and social support were related to not RTW in patients with BC. Since RTW represents financial stability and a sign of recovery and provides a sense of normalcy for BC patients, early assessment and suitable strategies targeting improvement of anxiety, loneliness, frailty, and social support are imperative for BC patients. Since few standard mental healthcare practices are available for patients with BC in Indonesia, identifying the impacts of anxiety and loneliness on RTW highlights the need for mental health assessments and management, particularly for patients with BC in Indonesia.
Implications for Occupational Health Practice
Breast cancer is more prevalent among the middle-aged and elderly workforce, making occupational and environmental health care crucial for supporting BC patients in RTW after treatment. Occupational health practitioners should play a key role in facilitating RTW by matching suitable jobs for patients with stable clinical conditions. Additionally, occupational health nurses should provide appropriate counseling and psychological strategies to address loneliness and anxiety, as well as physical activity programs to improve frailty, aiding in adapting to RTW. Comprehensive social support, including informational, emotional, esteem, and social network resources, is essential for successful reintegration into the workplace (Zomkowski et al., 2019). Continuing education and training for occupational health nurses are necessary to empower them in delivering effective health services for these patients. Furthermore, more research is needed to develop and validate suitable interventions targeting these risk factors to ensure successfully RTW for BC patients.
Applying Research to Occupational Health Practice
This study investigated factors associated with not RTW among BC patients in Indonesia, involving 250 participants from two hospitals. Results showed that high levels of anxiety, loneliness, and frailty, and low perceived social support significantly increased the risk of not RTW. Specifically, patients with higher levels of anxiety (OR: 5.30, 95% CI [2.16, 12.98]), loneliness (OR: 3.15, 95% CI [1.29, 7.67]), and frailty (OR: 2.53, 95% CI [1.07, 5.98]) and low social support (OR: 5.65, 95% CI [1.81, 17.63]) were more likely to not experience RTW. These findings highlight the need for occupational health nursing to focus on early intervention strategies related to these risk factors for successful reintegration into the workplace by patients with BC. Occupational health nurses can implement tailored counseling, psychological support, and physical activity programs to address these risk factors and enhance preparation for RTW. Additionally, reinforcing social support networks is essential for ensuring successfully RTW.
Footnotes
Acknowledgements
We extend our gratitude to all of the breast cancer patients who participated in this study, as well as project staff. We would also like to thank Dr. M. Djamil Padang Public Hospital, Andalas University Hospital, the Faculty of Nursing at Universitas Andalas (UNAND) in Padang, Indonesia, and Taipei Medical University in Taiwan for their invaluable support.
Author Contributions
Merdawati, L conducted the cross-sectional study, analysis and interpretation of results, and draft preparation and revised the manuscript. H.C. Lin and C.H. Pan provide intellectual comments on study designs, data analysis, and data interpretation. H.C. Huang provided methodological support and data analysis, reviewed the results, and revised and approved the final version of the manuscript.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethics approval was obtained from the Ethical Committee of Central General Hospital, Dr. M. Djamil Padang (no. LB.02.02/5.7/129/2022), and Taipei Medical University Joint Institutional Review Board (no. N202206028).