
Abstract
Background:
Occupational drivers are exposed to a wide range of risk factors, including sedentary behavior and physical inactivity, which can contribute to various chronic diseases. However, exercise interventions are likely to alleviate the negative associations and reduce chronic disease risks. This systematic review aimed to inventorize research studies investigating the effects of physical activity and exercise interventions on health outcomes in occupational drivers, and to assess interventions that have demonstrated effectiveness on health outcomes in occupational drivers.
Methods:
The electronic databases “Web of Science,” “Scopus,” and “PubMed” were searched using keywords related to “occupational drivers,” “exercise,” and “health outcomes.” Studies were included if they examined the effects of physical activity and exercise among occupational drivers on the following health outcomes: pain, disability, lifestyle factors (sleep, weight, physical activity, nutrition), fatigue, stress, and cardiometabolic risk factors. The methodological quality of the studies was assessed by the Cochrane Risk of Bias tools for randomized and non-randomized studies.
Results:
Fourteen articles were included (three randomized and 11 non-randomized controlled trials). All studies were judged to have an overall risk of bias as “some concerns, low, moderate or serious.” Evidence suggests that stretching and isometric exercises have significantly improved pain, disability, and fatigue. In contrast, multicomponent lifestyle interventions have enhanced physical activity levels, cardiometabolic risk factors, anthropometrics (body mass index, weight, waist circumference), sleep, and dietary intake among occupational drivers.
Conclusion:
The available evidence indicates the potential benefits of exercise interventions and physical activity for health outcomes in occupational drivers. However, high-quality studies are needed in the future to establish stronger evidence supporting the effect of the exercise intervention.
Background
Occupational drivers have barriers to maintain a healthy lifestyle because of their exposure to a variety of risk factors, such as long, variable, and unpredictable working hours, poor air quality, and lack of healthy food options on the road (Apostolopoulos et al., 2011; Apostolopoulos et al., 2010; Caddick et al., 2017). Physical activity levels are low in drivers, with approximately 20% to 30% failing to meet the guidelines and recommendations for physical activity, which is 30 minutes of exercise on most days each week (Sendall et al., 2019). Physical activity levels are low among drivers in comparison to other industries (Murray et al., 2019; Van Uffelen et al., 2010). Furthermore, drivers also exhibit extreme sedentary behavior, accumulating an average of 13 hours per day of sedentary behavior (Sieber et al., 2014; Varela-Mato et al., 2016). This is worrisome, as evidence shows that high levels of sedentary behavior and physical inactivity are linked to an increased risk of obesity, cardiovascular disease (CVD), diabetes, cancer, obstructive sleep apnea, metabolic syndrome, stress, fatigue, and musculoskeletal discomforts (Apostolopoulos et al., 2013; Hill et al., 2015; I.-M. Lee et al., 2012; Rezende et al., 2014). It is essential to counteract this physical inactivity and sedentary behavior to prevent chronic disease development and promote health and well-being optimally (Crizzle et al., 2017; Ha et al., 2022).
Many investigations have suggested that exercise is beneficial for improving disability and musculoskeletal pain of the spine, upper and lower extremities (Jordan et al., 2017; Rodrigues et al., 2014). Additional research has shown significant improvement in anthropometric variables and reduction in cardiometabolic risk factors resulting from exercise (Battista et al., 2021; Blüher et al., 2014). The beneficial effects of regular exercise are well known for both physical and mental health, and numerous researchers have investigated the psychological benefits of exercise, focusing on many psychological components like mood, cognitive function, stress, depression, and anxiety (Mandolesi et al., 2018; Mikkelsen et al., 2017). Physical inactivity and poor dietary habits lead to poor sleep quality and insomnia, and it has been documented that those who engaged in moderate or vigorous physical activity had adequate sleep and woke up less frequently during the night (Kredlow et al., 2015; Podhorecka et al., 2017).
Exercise interventions have a wide range of beneficial effects on musculoskeletal disorders, psychological well-being, and sleep. To the researchers’ knowledge, there is limited literature on the effectiveness of physical activity and exercise interventions in occupational drivers, which is reported due to perceived barriers to exercise, such as lack of facilities, time, and interest (Turner & Reed, 2011). There is no previous comprehensive review that has evaluated the effectiveness of physical activity and exercise interventions for health outcomes in occupational drivers. Therefore, this systematic review aimed to inventorize the effects of physical activity and exercise interventions on health outcomes among occupational drivers and to assess interventions that have demonstrated effectiveness on health outcomes in occupational drivers.
Methods
This systematic review was conducted and reported according to the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (Page et al., 2021). This study was prospectively registered with PROSPERO (registration ID: CRD42023392481).
Search Strategy
A comprehensive search of the scientific literature was undertaken using key electronic databases; Web of Science, Scopus, and PubMed until November 2022. The combination of keywords and MESH terms relevant to the review consists of two key concepts derived from population and exposure, whereby the population were occupational drivers, and the exposure was “exercise or physical activity.” For this review, exercise was defined as a subset of physical activity that is planned, structured, and repetitive and is done to maintain or enhance fitness and health (Dasso, 2019). The key concepts within each component were linked with “OR,” and the keywords of population and exposure were connected with “AND.” The comprehensive list of search terms and strategies is documented in Tables (Supplemental Materials 1 and 2). Additional relevant studies were found by searching the reference lists of the included papers.
Study Selection and Eligibility Criteria
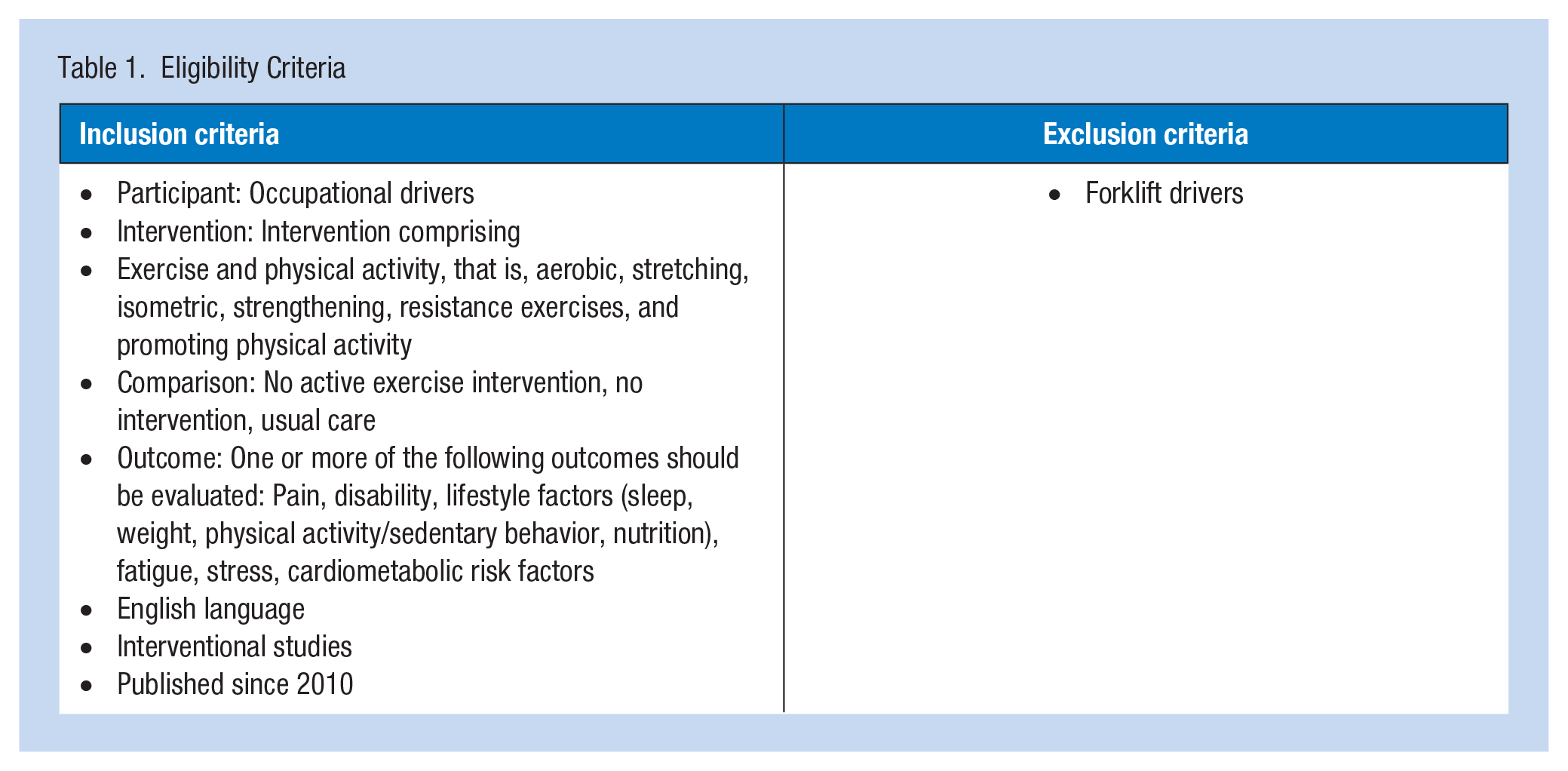
Following the literature search, results were exported into Rayan to check for duplicate studies, which were removed accordingly. The study selection process comprised three screening levels: study title, abstract, and full-text screening. The title of the study was evaluated in the first level, followed by an abstract screening in the second level. The full text of the remaining studies was then evaluated and assessed according to the eligibility criteria in the third level of the screening process (Table 1).
Eligibility Criteria
Methodological Quality Assessment
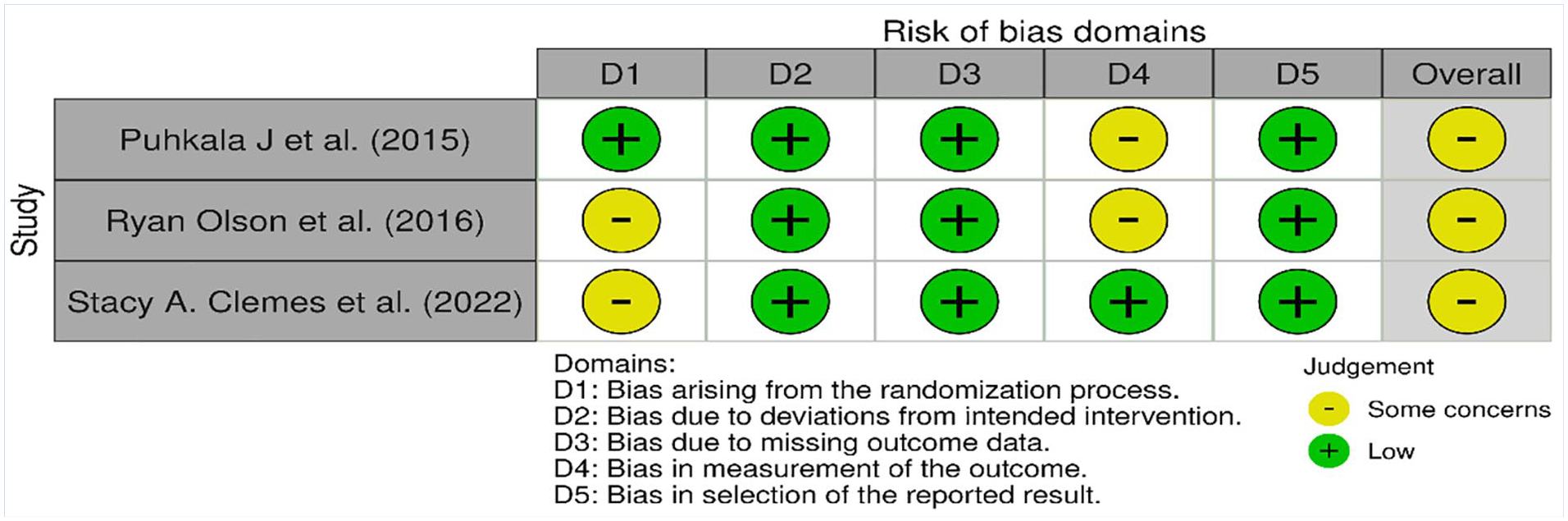
The Cochrane Risk of Bias tools for randomized and non-randomized studies were employed for methodological quality evaluation. The risk of bias for randomized studies was evaluated using the ROB-2 developed by Cochrane (Sterne et al., 2019). According to the guidelines, ROB-2 identifies five domains for bias resulting from: “the randomization process,” “deviations in the intended interventions,” “missing data on the outcomes,” “measurement of the outcomes,” and “selective reporting of the results.” Each domain’s signaling questions were answered and then the algorithm determined the overall risk of the bias according to the results for each domain as low risk, high risk, or some concerns. According to the algorithm’s evaluation, studies were rated as “low risk of bias” overall if all five domains were evaluated as “low risk of bias.” Studies with at least one domain of “some concern/high risk of bias” were overall rated as “some concern/high risk of bias.” The overall “high risk of bias” was assigned to studies with four or more domains assessed as “some concerns.”
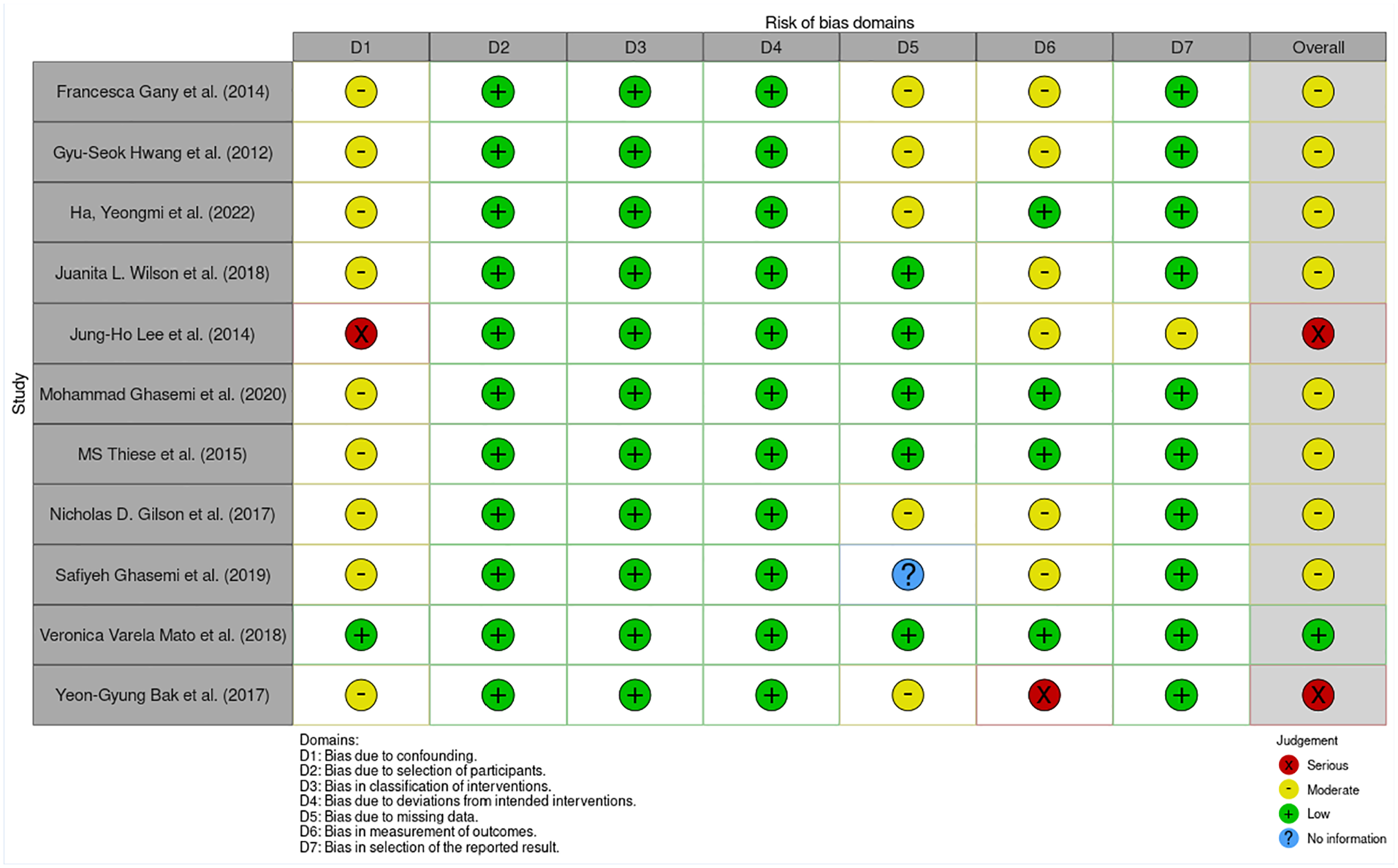
Cochrane Collaboration’s ROBINS-I tool was used to assess the risk of bias for non-randomized studies of intervention (NRSI) (Sterne et al., 2016). According to the guidelines, the ROBINS-I tool identifies seven domains for bias: “confounding factors,” “participant selection,” “intervention measurement,” “deviations in the intended interventions,” “missing data,” “measurement of the outcomes,” and “selective reporting of results.” Each domain’s signaling questions were answered, and the overall risk of the bias was estimated according to the results for each domain as low, moderate, serious, or critical. Studies were rated overall as low, moderate, or serious risk of bias according to the algorithm’s evaluation guidelines.
The methodological quality assessment of inclusive studies was performed independently by the two authors (AZ and TM). The results extracted by both authors were compared and verified for accuracy. Any disagreements/conflicts were resolved by cross-checking and discussion.
Data Extraction and Synthesis
After finalizing the study selection, standardized Excel spreadsheets were used to inventorize data from the included studies. The study characteristics extracted from the reviewed studies include author information, year of publication, study design, participant characteristics, intervention characteristics, outcome measures, results, and conclusion. The characteristics of the included studies are summarized in Table 2 and Supplemental Material 5.
Characteristics of Studies
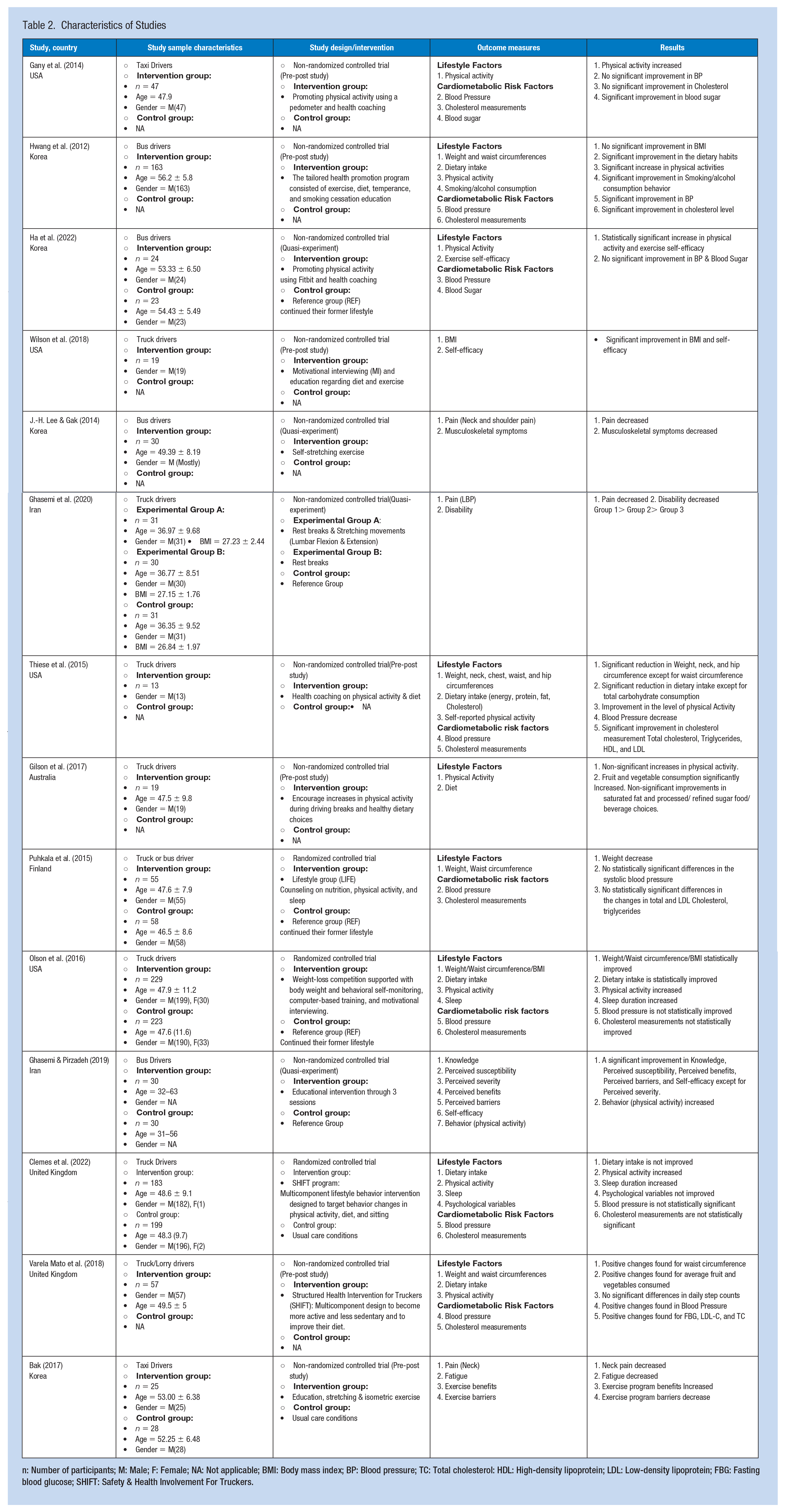
n: Number of participants; M: Male; F: Female; NA: Not applicable; BMI: Body mass index; BP: Blood pressure; TC: Total cholesterol: HDL: High-density lipoprotein; LDL: Low-density lipoprotein; FBG: Fasting blood glucose; SHIFT: Safety & Health Involvement For Truckers.
Results
Study Selection
The process of article identification and selection is documented in Figure 1. The search strategy identified 8,399 relevant studies. Of the initial 8,399 identified studies, 473 studies based on duplication and 7,731 studies by title and abstract were excluded as not being of relevance for the current review. Studies were then retrieved and assessed for eligibility against the inclusion and exclusion criteria (n = 195) by reviewing the full-text articles. Studies that did not meet the eligibility criteria (n = 181) were excluded. Finally, 14 full-text articles were included.
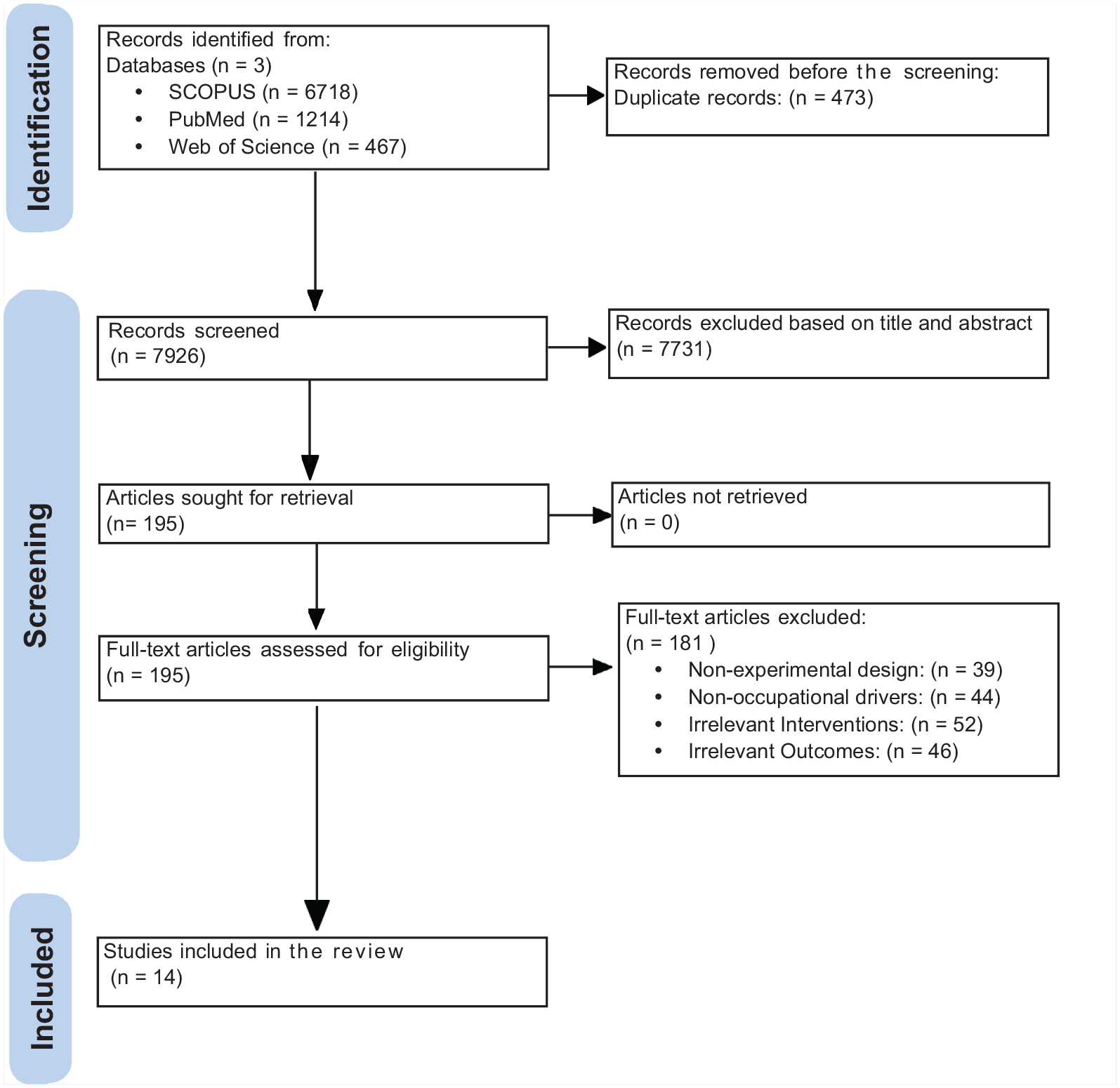
PRISMA Flowchart
Study Characteristics
The designs of the included studies are summarized in Table 2. Of the 14 studies, three were randomized controlled trials (Clemes et al., 2022; Olson et al., 2016; Puhkala et al., 2015), while the remaining 11 were non-randomized controlled trials (Bak, 2017; Gany et al., 2014; Ghasemi et al., 2020; Ghasemi & Pirzadeh, 2019; Gilson et al., 2017; Ha et al., 2022; Hwang et al., 2012; J.-H. Lee & Gak, 2014; Thiese et al., 2015; Varela Mato et al., 2018; Wilson et al., 2018). Of the 11 non-randomized controlled trials, three were quasi-experimental studies, and eight were pre-post studies.
The included studies were conducted across a wide range of nations, including Korea (n = 4) (Bak, 2017; Ha et al., 2022; Hwang et al., 2012; J.-H. Lee & Gak, 2014), the United States of America (n = 4) (Gany et al., 2014; Olson et al., 2016; Thiese et al., 2015; Wilson et al., 2018), the United Kingdom (n = 2) (Clemes et al., 2022; Varela Mato et al., 2018), Iran (n = 2) (Ghasemi et al., 2020; Ghasemi & Pirzadeh, 2019), Australia (n = 1) (Gilson et al., 2017), and Finland (n = 1) (Puhkala et al., 2015). The included studies covered three different types of occupational transportation, including truck drivers in seven studies (Clemes et al., 2022; Ghasemi et al., 2020; Gilson et al., 2017; Olson et al., 2016; Thiese et al., 2015; Varela Mato et al., 2018; Wilson et al., 2018), bus drivers in four studies (Ghasemi & Pirzadeh, 2019; Hwang et al., 2012; J.-H. Lee & Gak, 2014; Ha et al., 2022), taxi drivers in two studies (Bak, 2017; Gany et al., 2014), and one study that combined both truck and bus drivers (Puhkala et al., 2015).
The studies included in the review indicate a considerable range of sample sizes. In total, 1,547 drivers participated across the 14 studies, with a minimum of 13 (Thiese et al., 2015) and a maximum of 452 drivers (Olson et al., 2016). Thirteen studies included information on sex distribution. Ten studies included all males as participants, while three included both males and females, with males being the predominant gender (Clemes et al., 2022; J.-H. Lee & Gak, 2014; Olson et al., 2016). Only one study did not report the gender distribution (Ghasemi & Pirzadeh, 2019). All 14 studies reported the age of the participants, which ranges from 26 to 69 years, having a maximum fall between 40 and 50 years. Eleven studies reported anthropometrics of the participants in which a majority of participants fall within the overweight and obese category.
Only five studies reported sample ethnicity, including a majority of Caucasian participants, while nine did not report the participants’ race. Seven studies reported the marital status of the participants, most of whom were married, while seven did not report the marital status of the participants. Seven studies described participants’ education levels with an overall trend toward most participants having a secondary/high school level of education.
Risk of Bias
All the studies were judged to have an overall risk of bias as “some concerns, low, moderate or serious.” The three RCTs showed “some concerns risk of bias” because of bias in the domains of the “randomization process,” and “measurement of the outcomes.” For non-randomized studies, the overall risk of bias was “low, moderate or serious,” with eight studies showing a “moderate risk of bias,” two studies showing a “serious risk of bias,” and one study showing a “low risk of bias.” There was a “low risk of bias” in the domains of “selection of participants,” “interventions measurement,” and “deviations in the intended interventions,” while “moderate risk of bias” was common in the domain of “confounding factors.” Robvis R package software was used to generate “traffic light” and “summary” plots of the included papers, which are shown in Figures 2, 3, and Online Supplement Material (Supplementary Materials 3 and 4).
Risk of Bias Assessment for RCTs
Risk of Bias Assessment for Non-RCTs
Intervention Types, Delivery Method, and Dosage
Types of Interventions
Different types of intervention were utilized to improve the various health outcomes of occupational drivers. These interventions can be classified into three main categories: stretching exercises, promoting physical activity, and multicomponent intervention, such as a combination of physical activity, diet, and lifestyle behavior changes. Studies employing stretching exercises interventions included stretching movements of the neck (J.-H. Lee & Gak, 2014), lumbar, and abdominal muscles in combination with rest breaks (Ghasemi et al., 2020), stretching and isometric exercise of neck muscles with education on the exercise of the whole body (Bak, 2017). These studies reported consistent improvements in pain, MSD symptoms, disability, and fatigue. Studies that focused on promoting physical activity as an intervention included using Fitbit (Ha et al., 2022), pedometer step counter (Gany et al., 2014) with health coaching, and educational intervention on physical activity (Ghasemi & Pirzadeh, 2019). Significant improvements in physical activity levels were noted, while no significant difference changes were observed in cardiometabolic risk factors, that is, blood pressure and cholesterol level, with interventions focusing on promoting physical activity. Studies that implemented multicomponent interventions reported comprehensive improvements across various health outcomes, including anthropometrics, physical activity levels, dietary intake, sleep, cholesterol levels, and blood pressure (Clemes et al., 2022; Gilson et al., 2017; Hwang et al., 2012; Olson et al., 2016; Puhkala et al., 2015; Thiese et al., 2015; Varela Mato et al., 2018; Wilson et al., 2018).
Methods of Intervention Delivery
Methods of exercise intervention delivery and motivation for increasing physical activity included health promotion sessions, motivational interviewing, face-to-face meetings, physical therapist visits, follow-up calls, and text/photo messages on diet, physical activity, sedentary behavior, alcohol consumption, tobacco use, sleep, stress, and disease prevention. There was no linear relationship between the effectiveness of intervention and delivery methods, but it may vary with specific outcomes being measured. Stretching exercises delivered through different methods effectively reduce pain among all groups of drivers (Bak, 2017; Ghasemi et al., 2020; J.-H. Lee & Gak, 2014). Likewise, interventions aimed at promoting physical activity were administered through various methods that positively affected physical activity levels among different groups of drivers (Gany et al., 2014; Ghasemi & Pirzadeh, 2019; Ha et al., 2022).
Duration of Interventions
The systematic review covered studies with intervention durations ranging from 4 weeks to 12 months. Short-term interventions (Bak, 2017; J.-H. Lee & Gak, 2014; Wilson et al., 2018), ranging from 4 to 8 weeks, addressed specific outcomes such as pain, musculoskeletal symptoms, fatigue, and self-efficacy. Studies implementing interventions of short duration aimed to achieve immediate results and have demonstrated significant improvements in targeted outcomes. Four-week interventions emphasized motivation for increasing physical activity (Wilson et al., 2018) and self-stretching exercises (J.-H. Lee & Gak, 2014), while the one lasting for 8 weeks implemented a weekly regimen of neck muscle exercises (Bak, 2017).
Medium-term interventions (Gany et al., 2014; Ghasemi et al., 2020; Ghasemi & Pirzadeh, 2019; Gilson et al., 2017; Ha et al., 2022; Hwang et al., 2012; Olson et al., 2016; Thiese et al., 2015; Varela Mato et al., 2018), lasting from 3 to 6 months, and long-term interventions (Clemes et al., 2022; Puhkala et al., 2015), lasting 12 months, targeted a broader range of outcomes, including physical activity levels, anthropometric measures, cardiometabolic risk factors, dietary intake, disability, sleep, psychological factors, and lifestyle modification. These interventions aimed to achieve long-lasting health improvements and sustained behavior change. The review revealed inconsistent results after medium-term and long-term interventions for different variables.
Studies (Clemes et al., 2022; Gany et al., 2014; Ghasemi & Pirzadeh, 2019; Ha et al., 2022; Hwang et al., 2012; Olson et al., 2016; Thiese et al., 2015) reported positive changes in physical activity levels, anthropometric measures, dietary intake, and sleep. However, mixed responses were reported for cardiometabolic risk factors (blood pressure, cholesterol measurements, and glycemic control). Significant improvement was observed in three studies (Hwang et al., 2012; Thiese et al., 2015; Varela Mato et al., 2018), while five studies showed no effects (Clemes et al., 2022; Gany et al., 2014; Olson et al., 2016; Puhkala et al., 2015; Ha et al., 2022).
Twelve-week interventions included encouraging physical activity by increasing daily step counts (Gany et al., 2014), moderate-intensity exercise (Ha et al., 2022), decreasing weight (Thiese et al., 2015), lumbar stretching (Ghasemi et al., 2020), and cab-workout (Exercise program that can be performed during work breaks involving large muscle groups) (Varela Mato et al., 2018). Study interventions followed for 3 months (Ghasemi & Pirzadeh, 2019) and 20 weeks (Gilson et al., 2017) focused on motivation for increasing physical activity. Studies of 6 months duration focused on increasing physical activity by walking (Olson et al., 2016) and aerobic activities (Hwang et al., 2012). Studies that provided intervention for 12 months included incorporating moderate-intensity walking (Puhkala et al., 2015) and increasing physical activity by walking and cab-workout (Clemes et al., 2022).
Ten studies didn’t state clear information about the exercise setting as the interventions were mostly about increasing physical activity and exercising regularly, but only four studies advised the drivers to do their stretching and cab workout in rest breaks during their travel (Clemes et al., 2022; Ghasemi et al., 2020; Gilson et al., 2017; Varela Mato et al., 2018).
Effects of Interventions on Health Outcomes
Musculoskeletal Disorders
Three studies reported measured pain. One focused on lower back pain (Ghasemi et al., 2020), one on neck pain (Bak, 2017), and the other on neck and shoulder pain (J.-H. Lee & Gak, 2014). Low back and neck pain was improved following stretching movements, isometric exercises, and exercise education in the intervention group more than in the control group (Bak, 2017; Ghasemi et al., 2020). Moreover, another study reported improvement in neck and shoulder pain as a result of self-stretching exercises (J.-H. Lee & Gak, 2014). Significant between-group and within-group differences were observed (Bak, 2017; Ghasemi et al., 2020).
The review identified one study that measures disability, and this study showed that participants who performed stretching exercises (lumbar and abdominal) and rest breaks improved significantly more than the control group (Ghasemi et al., 2020). Significant differences between groups were seen, with no notable within-group differences identified for the variable of disability. Only one study measured musculoskeletal symptoms. Participants using stretching of the sternocleidomastoid muscle, upper trapezius, and levator scapulae muscles showed statistically significant improvement in neck and shoulder symptoms (J.-H. Lee & Gak, 2014).
Lifestyle Factors
Six studies measured anthropometric variables (BMI, weight, waist circumference). Five studies reported statistically significant reductions in anthropometric outcomes (Olson et al., 2016; Puhkala et al., 2015; Thiese et al., 2015; Varela Mato et al., 2018; Wilson et al., 2018), while one reported no significant difference (Hwang et al., 2012). Nine studies reported changes in the level or behavior of physical activity. Of these, seven studies found significant improvement in levels of physical activity (Clemes et al., 2022; Gany et al., 2014; Ghasemi & Pirzadeh, 2019; Hwang et al., 2012; Olson et al., 2016; Thiese et al., 2015; Ha et al., 2022). One study reported no significant difference (Varela Mato et al., 2018). In contrast, one study reported a non-significant increase in physical activity (Gilson et al., 2017).
Six studies reported dietary intake, with five showing significant improvements in dietary behavior (Gilson et al., 2017; Hwang et al., 2012; Olson et al., 2016; Thiese et al., 2015; Varela Mato et al., 2018), while one reported changes as not statistically significant (Clemes et al., 2022). Among the studies reporting improved dietary habits, one study reported a significant reduction in total daily calories, total fat, and saturated fat consumption, except total carbohydrates, after health coaching on diet and physical activity intervention (Thiese et al., 2015). In contrast, another study reported that fruit and vegetable consumption were significantly increased, with no improvement in dietary intake of other food items (Gilson et al., 2017).
Sleep was used as an outcome measure in two studies. Sleep duration was increased on non-working days and decreased on working days in both groups, that is, “Structured Health Intervention For Truckers (SHIFT)” and the control group (Clemes et al., 2022). An increase from 7.82 to 8.04 hours in sleep time was observed in the SHIFT intervention group in comparison to the control group (7.77–7.75 hours), which shows an average between-group difference of approximately 15 minutes per night (Olson et al., 2016). One study measured smoking and alcohol consumption habits. The number of participants in the smoking group decreased from 52.1% to 39.3%, so there were significant differences in smoking behavior before and after a tailored health promotion program. Overall, the results showed a statistically significant difference in the frequency of alcohol consumption habits; however, no significant differences were found in the amount of alcohol consumption (Hwang et al., 2012).
Cardiometabolic Risk Factors
Eight studies reported blood pressure as an outcome measure. Three of them found improvements in systolic and diastolic blood pressure (Hwang et al., 2012; Thiese et al., 2015; Varela Mato et al., 2018), while one study showed improvement in only diastolic blood pressure (Puhkala et al., 2015) after an intervention. However, four of these studies did not report any significant changes in blood pressure (Clemes et al., 2022; Gany et al., 2014; Olson et al., 2016; Ha et al., 2022).
Seven studies reported cholesterol measurement (total cholesterol [mg/dL], triglycerides [mg/dL], HDL-cholesterol [mg/dL], LDL-cholesterol [mg/dL]) as an outcome measure. Of these, three studies reported significant changes in cholesterol measurement (Hwang et al., 2012; Thiese et al., 2015; Varela Mato et al., 2018), while four of them did not report any significant changes in cholesterol measurement post-intervention (Clemes et al., 2022; Gany et al., 2014; Olson et al., 2016; Puhkala et al., 2015). Two research studies examined glycemic control as an outcome measure. Neither study found any significant difference in blood sugar levels with the mHealth program and the mHealth financial incentives program (Gany et al., 2014; Ha et al., 2022).
Fatigue
One study addressed the issue of fatigue using a neck exercise program as an intervention consisting of stretching movements, isometric exercises, and exercise education. Statistically, significant improvements were noted in the fatigue of the participants (Bak, 2017).
Psychosocial Measures
Only one study reported psychosocial variables as an outcome measure, and no significant improvements were noted in the participants’ work-related psychosocial variables or mental well-being after intervention, that is, SHIFT program (Clemes et al., 2022).
Exercise Metrics
Two studies presented exercise self-efficacy as an outcome measure, and both indicated a statistically significant difference with the mHealth program and educational physical activity intervention (Ghasemi & Pirzadeh, 2019; Ha et al., 2022). Two studies reported exercise perceived benefits and barriers as an outcome measure, and both studies showed statistically significant differences with the neck exercise program and educational physical activity interventions (Bak, 2017; Ghasemi & Pirzadeh, 2019). One study listed exercise knowledge, perceived severity, and susceptibility as outcome measures and found statistically significant differences with educational physical activity intervention (Ghasemi & Pirzadeh, 2019).
In summary, exercise intervention produced beneficial effects on different health outcomes, including pain, disability, lifestyle factors, fatigue, and cardiometabolic risk factors. Exercise intervention involving stretching movements and isometric exercises demonstrated significant improvements in pain, disability, fatigue, and musculoskeletal symptoms (Bak, 2017; Ghasemi et al., 2020; J.-H. Lee & Gak, 2014). Exercise intervention focusing on promoting physical activity using wearable activity devices significantly increases physical activity levels and exercise self-efficacy (Gany et al., 2014; Ghasemi & Pirzadeh, 2019; Ha et al., 2022). However, multicomponent lifestyle behavior intervention consisting of exercise and diet intake modification significantly improved the level of physical activity, cardiometabolic risk factors, anthropometrics, and dietary intake.
Discussion
This systematic review aimed to critically review the research studies investigating the effects of physical activity and exercise interventions on improving health outcomes in occupational drivers. The systematic review identified 14 intervention studies, of which 11 were non-randomized controlled trials. The studies encompassed diverse populations from different countries, focusing on occupational transportation such as truck, bus, and taxi drivers. These studies involved exercise interventions that varied widely in terms of duration, dosage, frequency, intensity, delivery methods, and exercise settings. Intervention primarily included stretching exercises, isometric exercises, resistance exercises, physical activity promotion, health coaching, and lifestyle modification. These interventions were delivered through different methods, including health promotion sessions, motivational interviewing, meetings, messages, and technology-based tools.
The review found that the interventions led to positive changes across different health outcomes, including improvements in pain, disability, musculoskeletal symptoms, fatigue, anthropometric measures, physical activity levels, dietary behavior, sleep, and exercise metrics. There were mixed results regarding the impact of exercise on cardiometabolic risk factors such as blood pressure and cholesterol levels. However, no significant changes were reported in glycemic control and psychosocial measures.
Demographic findings showed that occupational drivers have a high BMI, falling within the overweight and obese categories (Clemes et al., 2022; Gany et al., 2014; Ghasemi et al., 2020; Gilson et al., 2017; Hwang et al., 2012; J.-H. Lee & Gak, 2014; Olson et al., 2016; Puhkala et al., 2015; Thiese et al., 2015; Varela Mato et al., 2018; Wilson et al., 2018). The findings about anthropometrics variables are consistent with the results of previous studies among professional drivers and other sedentary workers, showing a high frequency of obesity (Rosso et al., 2015; Zubery et al., 2021). Risk factors, including sedentary behavior, physical inactivity, and poor dietary choices, lead to high BMI associated with adverse health consequences such as the increased risk of cardiovascular disease, diabetes, and musculoskeletal disorders (Gany et al., 2014; Hwang et al., 2012; Varela Mato et al., 2018). So, it is essential to consider these factors when developing interventions by encouraging drivers to adopt healthier lifestyles.
To the best of the authors’ knowledge, there is a lack of literature on the effects of physical activity and exercise interventions on the health outcomes of drivers. Studies using Fitbit, pedometers, motivational interviewing, health coaching, and cab workouts for promoting physical activity levels effectively increased physical activity levels among all participants (Clemes et al., 2022; Gany et al., 2014; Ghasemi & Pirzadeh, 2019; Ha et al., 2022; Hwang et al., 2012; Olson et al., 2016; Thiese et al., 2015). Meaningful difference was observed in the number of steps, exercise duration, and self-efficacy in intervention groups, which suggests that these intervention strategies are beneficial for motivating occupational drivers to engage more in physical activity and adopting healthy lifestyles. These findings align with prior research studies that have demonstrated that wearable activity trackers and behavioral change strategies can significantly enhance physical activity among individuals (D’Amore et al., 2022; Ferguson et al., 2022; Lubans et al., 2009; Nuss et al., 2021; Tang et al., 2020).
Cardiometabolic risk factors (Cholesterol, blood pressure, and blood glucose) showed mixed responses to physical activity and exercise interventions, with some studies reporting significant improvements in cardiometabolic risk factors, while others did not find significant changes. Interventions such as tailored health promotion programs (Hwang et al., 2012), Structured Health Intervention for Truckers (Varela Mato et al., 2018), and health coaching on physical activity and diet (Thiese et al., 2015) reported significant improvements in cholesterol measurements. These findings show that interventions focusing on increasing physical activity and diet control can positively affect cardiometabolic risk factors. On the other hand, studies that solely focused on promoting physical activity did not achieve significant changes in cholesterol levels (Gany et al., 2014; Olson et al., 2016). These findings are consistent with earlier studies showing the effectiveness of physical activity in improving anthropometric variables and cardiometabolic risk factors in sedentary individuals (Amaro-Gahete et al., 2019; Franco et al., 2016; Kallings et al., 2009).
Findings also suggest that incorporating stretching movements, isometric exercises, rest breaks, and exercise education may reduce pain, disability, fatigue, and musculoskeletal symptoms in occupational drivers (Bak, 2017; Ghasemi et al., 2020; J.-H. Lee & Gak, 2014). These results align with previous studies revealing that musculoskeletal disorders can be decreased by improving flexibility and reducing muscle tension with exercise intervention in sedentary workers (Behm & Chaouachi, 2011; Da Costa & Vieira, 2008; Sipaviciene & Kliziene, 2020). The results of these studies suggest that these interventions can effectively reduce the morbidity and mortality ratio among occupational drivers.
Multicomponent intervention with a variety of methods positively impacted at least one outcome variable, so it is difficult to define what specific intervention component contributed to improving health outcomes. Furthermore, there were differences in the type, duration, dosage, delivery method, and outcome measures of the intervention, making it challenging to define the most effective intervention. However, the findings of these studies are consistent with earlier studies showing that workplace intervention using a variety of delivery methods has a positive impact on sedentary behavior, physical activity, and other health outcomes (An & Song, 2020; Blangsted et al., 2008; Buckingham et al., 2019; Commissaris et al., 2016; Pedersen et al., 2009; Wang & Kassavou, 2023).
The study durations varied considerably, ranging from a minimum of 4 weeks to a maximum of 12 months, but positive outcomes were reported across various durations of intervention. Short-term interventions (4–8 weeks) addressed specific issues like pain, fatigue, exercise benefits, barriers, and self-efficacy, demonstrating positive immediate effects. Long-term interventions (3–12 months) consisting of multicomponent interventions addressed multiple health outcomes such as anthropometrics and cardiometabolic risk factors. These interventions targeted long-term effects and showed positive outcomes across various health measures and sustained behavioral changes.
As stated earlier, the studies included in this review varied in intervention dosage, frequency, intensity, type, delivery method, and outcomes of interest. However, interventions characterized by consistent and structured exercise routines demonstrated beneficial outcomes by improving pain, disability, fatigue, and self-efficacy. Conversely, interventions primarily focused on motivational or educational aspects without a clear exercise regimen yielded mixed outcomes, with improvements observed in some variables like physical activity and anthropometric measures but inconsistent results in cardiometabolic risk factors. It shows that the effectiveness of an intervention is influenced not only by the frequency, duration, and intensity of exercise but also by various other factors, including the intervention type, delivery method, and outcomes of interest. These findings align with previous studies revealing that incorporating varied exercise interventions with different dosages and durations can effectively improve health outcomes (Äng et al., 2009; Foster et al., 2005; Ogilvie et al., 2007; Yuenyongchaiwat, 2016).
Conclusion
In summary, limited studies were conducted on the effectiveness of exercise interventions on health outcomes in occupational drivers. Exercise interventions and physical activity significantly improved pain, disability, musculoskeletal symptoms, fatigue, anthropometric measures, physical activity levels, dietary behavior, sleep, and exercise metrics. At the same time, mixed effects were noted on cardiometabolic risk factors such as blood pressure and cholesterol levels. This may be due to the methodological shortcomings of the studies and variability in study characteristics, demographics, interventions, and settings. Overall, the available evidence suggests that exercise interventions can significantly improve health outcomes among occupational drivers. However, future studies should consider a holistic approach with more rigorous study designs and detailed exercise protocols for stronger evidence.
Implications for Occupational Health Practice
This review highlights that the majority of occupational drivers are prone to obesity due to their job demands, which leads to a variety of chronic diseases. Therefore, occupational health practitioners should implement tailored interventions focusing on the risk factors associated with this occupational group. Common musculoskeletal issues like pain, disability, and fatigue can be alleviated by incorporating exercise into the treatment plan. Occupational health practices should encourage physical activity and lifestyle behavior changes to achieve positive effects on various health parameters, including physical activity levels, anthropometrics, cardiovascular health, and dietary habits.
Supplemental Material
sj-docx-1-whs-10.1177_21650799241291903 – Supplemental material for Effects of Physical Activity and Exercise Interventions on Health Outcomes in Occupational Drivers: A Systematic Review
Supplemental material, sj-docx-1-whs-10.1177_21650799241291903 for Effects of Physical Activity and Exercise Interventions on Health Outcomes in Occupational Drivers: A Systematic Review by Alam Zeb, Jonas Verbrugghe, An Neven, Chris Burtin, Lotte Janssens, Timo Meus and Annick Timmermans in Workplace Health & Safety
Footnotes
Author Contributions
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Higher Education Commission of Pakistan (HEC), Grant No. HEC/HRD/OSS-III/Batch-3/Belgium/2022/19745.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.