
Abstract
Background:
Little is known about the health and well-being of U.S. correctional nurses. To protect correctional nurses, a better understanding of organizational characteristics, job stress, and well-being must be undertaken.
Method:
A cross-sectional design was used in the form of an online survey. Correctional nurses were conveniently recruited using national listservs and snowball sampling. Variables were measured with the Health & Safety Executive Management Standards Indicator Tool, Nurse Wellbeing Index, and the Perceived Stress Scale. Data were analyzed using descriptive statistics and analyses of variance.
Findings:
Two hundred seventy participants (142 registered nurses, 83 licensed practical nurses/licensed vocational nurses, and 42 advanced practice nurses) completed the survey. Job stress scored moderate (M = 16.26, SD = 7.14), and well-being levels were just below the risk for adverse events (M = 1.8, SD = 3.06). Lower scores were noted for managerial support (M = 3.13, SD = 0.35) and job demands (M = 3.56, SD = 0.92), but slightly better for job control (M = 3.57, SD = 0.77), peer support (M = 3.85, SD = 0.64), and workplace relationships (M = 3.73, SD = 0.95).
Conclusions:
Significant differences between organizational characteristics, job stress, and well-being were found across nursing licensure, workplace environments, biological sex, and employment through state or private agencies. Registered nurses working in U.S. prisons experienced the highest job stress and worse well-being.
Application to Practice:
This work is an essential next step in promoting healthy workspaces, urging the need for further research establishing the impact of organizational characteristics and job stress on nurse well-being.
Background
The United States maintains one of the largest correctional systems in the world, incarcerating more individuals per capita with approximately two million persons behind bars (Sabol et al., 2007; Sawyer & Wagner, 2022). Despite this, the number of U.S. nurses working in jails and prisons who care for this population has declined since 2006, from an estimated 3% to only 0.8% (Chafin & Biddle, 2013; LaMarre, 2006; Smiley et al., 2021). Concurrently, correctional nurses have reported experiencing job stress stemming from job demands, fear surrounding personal safety and physical threats from persons who are incarcerated, bullying from nurse colleagues and correctional officers, and conflict from the professional moral dilemmas they face (Keller et al., 2022). There is evidence of the negative impact of job stress on correctional officer health (Buden et al., 2016; Obidoa et al., 2011; Schaufeli & Peeters, 2000; Violanti, 2017), yet the health and well-being of U.S. correctional nurses remain understudied.
Promoting worker (and correctional nurse) well-being through safe and healthy work designs with reduced workplace hazards is a priority area of concern for the National Institute for Occupational Safety and Health (NIOSH, 2022). The Surgeon General has also developed a framework of five essentials to promote worker health, underscoring the impact of one’s work environment on their mental health and well-being (U.S. Department of Health and Human Services, 2022). Well-being contributes to workers’ overall quality of life, health and longevity, and supportive social relationships (Diener et al., 2017), as higher levels of well-being act as a protective factor against negative mental health outcomes (i.e., depression, anxiety) (Santini et al., 2022). Well-being is also related to job outcomes, including satisfaction, engagement, and performance (Chari et al., 2018; Harter et al., 2003). Addressing job stress is critical in this effort to promote well-being because job stress has spillover effects onto workers’ home lives and overall health (World Health Organization, 2021). Consequences of job stress include increased organizational costs related to higher turnover rates and retraining new staff (Almost et al., 2020; Chafin & Biddle, 2013), along with a decrease in the quality of care to patients (Khamisa et al., 2013).
The purpose of this study is to conduct a national survey to better understand the well-being of U.S. correctional nurses. The two related research objectives include describing a sample of correctional nurses (i.e., age, tenure in corrections, race, ethnicity, nurse licensure, biological sex) and exploring the relationship of job stress and organizational characteristics with wellbeing.
Methods
Study Design
A descriptive, cross-sectional, non-experimental study design was used to collect data on organizational characteristics, job stress, and well-being of U.S. nurses working in correctional environments. Inclusion criteria involved those 18 years old or older; advanced practice nurses (APNs), licensed practical nurses/licensed vocational nurses (LPNs/LVNs), or registered nurses (RNs); and currently employed in the United States working in a correctional facility (i.e., prison, jail, juvenile detention center, community-based correctional facility) for more than three months.
Study Population
A priori power calculations were determined using G*Power 3.0 (Faul et al., 2007). If 270 nurses participated, an acceptable power of 80% (β = 0.20) would be achieved assuming a small to medium effect size of 0.35 and α = 0.05 with well-being as the dependent variable. Therefore, the analytical sample goal was 270 participants. Post hoc power analysis revealed a large effect size (f2 = 1.849), resulting in 100% power achieved. Correctional nurses were sampled in a non-random, convenience sampling method after approval from the University of Cincinnati Institutional Review Board (IRB) was received. From July to August 2022, participants were recruited via electronic flyer from the American Correctional Nurses Association (ACNA), National Commission on Correctional Health Care (NCCHC), and through study champions with experience and access to the correctional nurse population. Because participants were asked to provide their email addresses to receive a participant payment, a National Institute of Health Certificate of Confidentiality was obtained to assure participants’ emails and data could not be compelled to be released.
Procedures
Study data were collected and managed using REDCap (Research Electronic Data Capture) hosted at the researchers’ university (Harris et al., 2019). Participants were directed to REDCap and answered screening questions to establish eligibility. The IRB approved a waiver of signed informed consent. Participants were presented with an electronic information sheet describing study details and asking participants to continue if willing to participate. Participants were able to complete this survey online at their convenience in the setting of their choice. The first 270 participants to complete the survey received a US$25 Amazon electronic gift card code for their time and effort.
Instrument
The survey included 58 self-administered questions, taking approximately 20 min to complete. The demographic questions included age, biological sex, race, ethnicity, nursing licensure, environment type (i.e., prison, jail, juvenile detention center, community-based correctional facility), U.S. state of employment, and time spent in their correctional role (or tenure) (Agency for Health care Research and Quality, 2019; Centers for Disease Control and Prevention, 2020). The rest of the survey was comprised of the Health & Safety Executive Management Standards Indicator Tool (HSE-MS IT; Cousins et al., 2004), Nurse Wellbeing Index (WBI; Dyrbye et al., 2018), and Perceived Stress Scale (PSS-10; Cohen et al., 1983), which were used in nursing samples previously (Alharbi & Alshehry, 2019; Dyrbye et al., 2018; Gibb et al., 2010; Ravalier et al., 2020; Sathiya et al., 2016). A “prefer not to answer” option was added to each question so that participants could skip a question if it made them uncomfortable, reducing coercion for a response.
The HSE-MS IT (Cousins et al., 2004) is a five-point Likert-type scale, which assesses the five workplace characteristics of job demands (i.e., time pressures), job control (i.e., autonomy), managerial support, peer support, and workplace relationships with colleagues. Each of these was averaged to indicate how nurses perceive their workplace conditions. Item scores can range from 1 to 5, where 1 indicates a poor score and 5 is more desirable (Cousins et al., 2004; Health and Safety Executive, n.d.). The HSE-MS IT was found to have concurrent and construct validity (Marcatto et al., 2014). A satisfactory Cronbach’s α of .91 was found in this sample (Bland & Altman, 1997).
The WBI evaluates distress including depression, fatigue, burnout, anxiety, and mental/physical quality of life. Item scores can range from -2 (low risk for distress/higher well-being) to 9 (high risk for distress/lower well-being). Mean scores of distress may determine those at risk for turnover or medication error, with scores >2 considered high, placing individuals at risk of adverse outcomes associated with distress (Dyrbye et al., 2019). WBI has criterion and construct validity (Dyrbye et al., 2019) with acceptable interrater reliability (Dyrbye et al., 2011). In this sample, the Cronbach’s α was an acceptable score of .89 (Bland & Altman, 1997).
The PSS-10 questions are rated from never (0) to very often (4) to measure stress during the last month. The summative scores range from 0 (indicating low stress) to 40 (indicating high stress), and are grouped as low stress (0-13), moderate stress (14-26), or high stress (27-40; Cohen, 1988; State of New Hampshire Employee Assistance Program, n.d.). The PSS-10 has an internal consistency coefficient of 0.754, indicating satisfactory reliability (Huang et al., 2020) with concurrent and convergent validity (Mitchell et al., 2008). In this sample, Cronbach’s α was acceptable with a score of .91 (Bland & Altman, 1997).
Data Analysis
Data were cleaned, coded, and checked for outliers and missing data for each variable. Please look for the management of missing data and prefer not to answer questions by demographic characteristics in the Supplemental Material. Data were explored for patterns, trends, and distributions using JMP Pro 16 (Cary, NC) statistical software. Descriptive statistics were used to summarize sample characteristics. Variables were compared across demographic groups using analysis of variance tests, after categorizing age and tenure as nominal values. Demographic responses for certain groups that were less than five were collapsed into similar groups, and “prefer not to answer” or “don’t know” responses were removed from the analysis, that is, don’t know/not sure response for ethnicity (n = 3) was removed for analysis; other work environment (n = 1) was collapsed into prison category.
Results
Sample
A sample of 347 U.S. correctional nurses were conveniently recruited. Incomplete or nonresponse data were removed, yielding a total of 270 participants who were included in the data analysis, with a participation rate of 78%. Most of the participants were female (n = 187, 69.8%), White (n = 151, 56.8%), and not Hispanic or Latino (n = 224, 86.8%). Participants mainly worked in prisons (n = 112, 41.2%) and jails (n = 81, 30.5%). One participant (0.4%) reported working in another institution, which was federal immigration; this participant was grouped within the prison group for analysis. Most of the participants were RNs (n = 142, 53.4%), followed by LPNs/LVNs (n = 83, 31.1%) and APNs (n = 42, 15.8%). Participants were mainly employed by the state (n = 136, 52.1%) and private agencies (n = 124, 46%). One participant reported employment by “other” as the Federal Bureau of Prisons (n = 1, 0.4%); this participant was grouped as employment by the state for analysis.
Tenure in the correctional environment ranged from five months to 27 years, and the average was 8.5 years. Ages ranged from 24 to 75, with an average age of 40.5 years old. Nearly all U.S. states had at least one respondent, except for the states of Arkansas, North Dakota, and South Dakota. Colorado had the largest response rate (n = 17, 6.3%), followed by California (n = 15, 5.6%). Regions were grouped overall as the Midwest region, Northeast region, South region, and West region (U.S. Census Bureau, n.d.), to pinpoint trends of those working in certain areas. Most responses were from the South region (n = 85, 31.7%). For detailed socio-demographic information, please refer to Table 1.
Socio-Demographic Characteristics of a Sample of U.S. Correctional Nurses (N = 270)
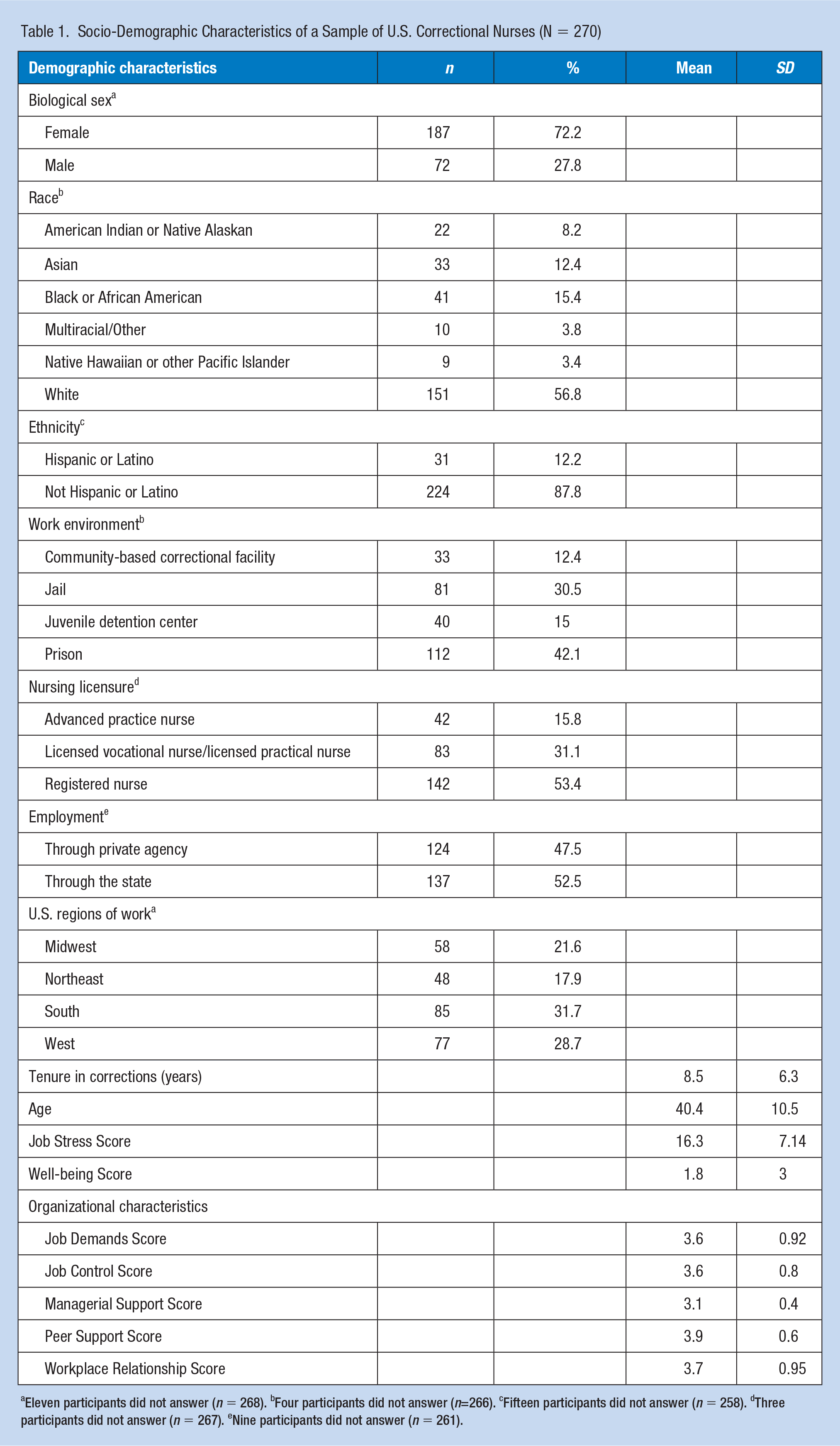
Eleven participants did not answer (n = 268). bFour participants did not answer (n=266). cFifteen participants did not answer (n = 258). dThree participants did not answer (n = 267). eNine participants did not answer (n = 261).
Organizational Characteristics
Most desirable scores for organizational characteristics would be a 5 on the continuum from 1 to 5. Results among participants included job demands (M = 3.56, SD = 0.92), job control (M = 3.57, SD = 0.77), manager support (M = 3.13, SD = 0.35), peer support (M = 3.85, SD = 0.64), and workplace relationships (M = 3.73, SD = 0.95).
Job Demands
Job demands significantly varied by groups of nursing licensure, work environment, biological sex, age, and tenure. RNs had significantly lower scores (M = 3.2, SD = 0.9) than APNs (M = 3.79, SD = 0.9), and LPNs/LVNs (M = 4.07, SD = 0.7), p < .0001. Those who worked in prisons (M = 3.17, SD = .8) had significantly lower scores than those who worked in community-based correctional facilities (M = 4, SD = .8), juvenile detention centers (M = 4.34, SD = .4), and jails (M = 3.55, SD = 1.0), p < .0001. Females (M = 3.44, SD = .9) had significantly lower scores than males (M = 3.8, SD = .9), p = .0016. Those aged between 50 and 59 (M = 2.96, SD = 0.83) had significantly lower scores than those aged between 40 and 49 (M = 3.45, SD = 0.88), 30-39 (M = 3.86, 0.89), and 18-29 (M = 3.96, 0.72), p < .0001. Those with working tenure over 10 years (M = 3.32, SD = 0.91), had significantly lower scores than those with correctional experience between 0-2 years (M = 4, SD = 0.69) and 3-5 years (M = 3.7, SD = 0.95), p < .0001. Job demand scores did not significantly differ by region or employment by private and state agencies.
Job Control
Job control significantly varied by nursing licensure, work environment, biological sex, and age. RNs had significantly lower job control scores (M = 3.3, SD = 0.7), compared with APNs (M = 4, SD = 0.7) and LPNs/LVNs (M = 3.8, SD = 0.6), p < .0001. Those working in prisons (M = 3.3, SD = .7) had significantly lower scores than those in juvenile detention centers (M = 4.2, SD = .5), community-based correctional facilities (M = 3.8, SD = .7), and jails (M = 3.7, SD = .8), p < .0001. Females (M = 3.5, SD = .8) had significantly worse scores than males (M = 3.7, SD = .8), p = .0287. Those aged older than 60 years (M = 3.06, SD = .67) had significantly lower scores than those aged 30-39 (M = 3.82, SD = .76), 18-29 (M = 3.59, SD = .69), and 40-40 (M = 3.53, SD = .67), p = .0001. There was no statistical evidence for significant differences by tenure, or employment by state or private agencies. Lowest scores for job control were found in the South region (M = 3.5, SD = .8), but these were not significant across groups, p = .5.
Managerial Support
Managerial support did not significantly differ by biological sex, nursing licensure, working environment, region, employment by state or private agency, age, or tenure.
Peer Support
Peer support significantly varied by nursing licensure and work environment. RNs had significantly lower scores of peer support (M = 3.7, SD = 0.7), compared with APNS (M = 3.9, SD = 0.6) and LPNs/LVNs (M = 4.05, SD = 0.48), p = .0003. Those who worked in prisons (M = 3.7, SD = .7) had significantly lower scores than those in juvenile detention centers (M = 4, SD = .4), community-based correctional facilities (M = 4, SD = .5), and jails (M = 3.9, SD = .7), p = .0006. Peer support scores did not significantly differ by biological sex, region, employment by state and private agency, age, or tenure.
Workplace Relationships
Workplace relationship scores were significantly different across nursing licensure, work environment, biological sex, employment by state and private agency, age, and tenure. RNs had significantly lower scores (M = 3.4, SD = 1) than LPNs/LVNs (M = 4.1, SD = 0.6), and APNs (M = 3.9, SD = 0.9), p < .0001. Those who worked in prisons had significantly worse scores (M = 3.3, SD = 0.9), than those in community-based correctional facilities (M = 4.3, SD = 0.5), juvenile detention centers (M = 4.5, SD = 0.3), and jails (M = 3.87, SD = 0.9), p < .0001. Females had significantly lower scores (M = 3.6, SD = 0.9) than males (M = 3.9, SD = 0.9), p < .0001. Scores were also significantly lower for those employed by the state (M = 3.6, SD = 1.0), than those in private agency (M = 3.9, SD = 0.9), p = .03. Those aged between 50 and 59 (M = 3.17, SD = 0.97) had significantly lower scores than those aged 18 to 29 (M = 4.2, SD = 0.57) and 30 to 39 (M = 3.92, SD = 0.95), p < .0001. Those with correctional work experience between 0 and 2 years (M = 4.13, SD = 0.72) had significantly better scores than those who worked between 6 and 9 years (M = 3.55, SD = 0.98) and those who worked over 10 years in corrections (M = 3.55, SD = 0.97), p = .0013. Workplace relationship scores did not significantly vary by region. Table 2 includes all mean organizational characteristics scores across demographics.
Mean Organizational Characteristic Scores for a Sample of U.S. Correctional Nurses Across Demographic Characteristics
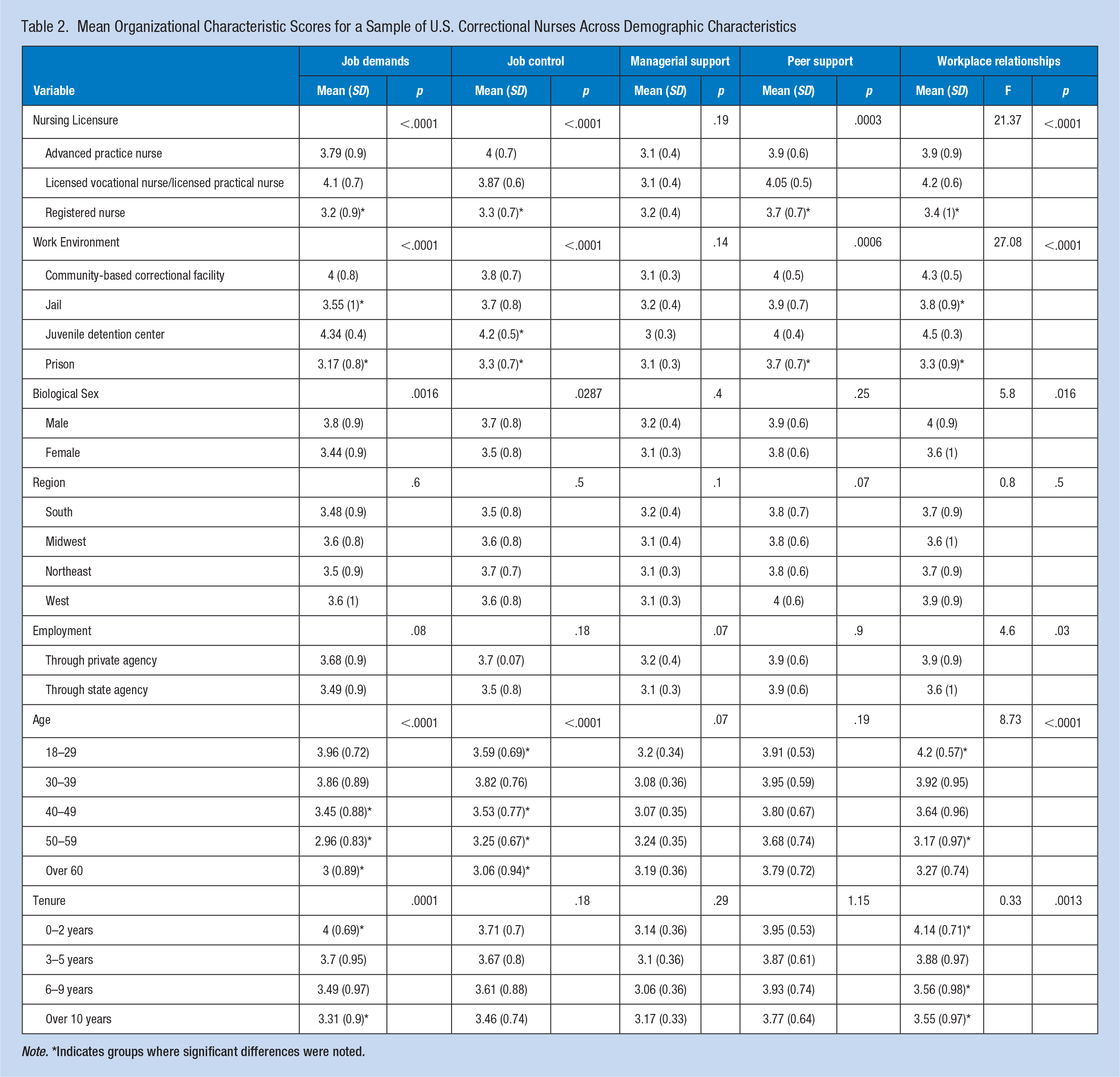
Note. *Indicates groups where significant differences were noted.
Job Stress
Total participant job stress scores ranged from 4 to 38 (with higher scores meaning higher stress), and the overall mean stress level was moderate (M = 16.26, SD = 7.1). Stress scores significantly varied by nurse licensure, work environment and age. RNs reported the highest mean scores (M = 18.79, SD = 7.1), and there was statistical evidence that RN job stress scores were significantly higher than LPNs/LVNs and APNs, p < .0001. There was evidence that those who worked in prisons had significantly higher stress scores than those in community-based correctional facilities, jails, and juvenile detention centers, p < .0001. There was also evidence that those aged between 50 and 59 (M = 19.51, SD = 7.95) had significantly different stress scores than those aged between 30 and 39 (M = 14.89, SD = 6.63), p = .0139.
Although females reported the highest mean job stress scores (M = 16.79, SD = 7.5), there was no evidence that job stress significantly differed by biological sex. Furthermore, differences in job stress were not statistically significant by region, but job stress was highest in Louisiana (M = 29.5, SD = 2.1), and lowest in Hawaii (M = 7.25, SD = 3.0) and Montana (M = 9, SD = 0.0). There was also no evidence of statistically significant difference in job stress levels between those employed by private agencies (M = 16.04, SD = 7.0) and state agencies (M = 16, SD = 7.0).
Well-Being
Well-being scores ranged from −2 to 9, with an average of 1.8 (SD = 3.1), where scores above 2 are considered at increased risk for adverse events. Scores significantly varied across groups for nursing licensure, biological sex, work environment, age, and tenure. RNs (M = 2.95, SD = 2.8) had significantly lower levels of well-being and higher distress scores than LPNs/LVNs and APNs, p < .0001. Those who worked in prisons (M = 3.5, SD = 2.6), had the lowest levels of well-being. There was evidence that distress scores of those working in prison were significantly higher than those in juvenile detention centers, community-based correctional facilities, and jails, p < .0001.
Those with a biological sex of female (M = 2.2, SD = 3.1) had significantly lower levels of wellbeing and higher distress than male scores (M = 1, SD = 2.7), p = .006. There was evidence that those aged between 50 and 59 (M = 3.3, SD = 2.59) had significantly lower levels of wellbeing with higher distress than those aged 18 to 29 (M = 0.8, SD = 2.8) and 30-39 (M = 1.01, SD = 2.92), p < .0001. There was also evidence that those who worked in corrections over 10 years had higher distress levels and worse wellbeing (M = 2.55, SD = 2.97) than those who worked in corrections between 0-2 years (M = .64, SD = 2.68), p = .0023.
While not statistically significant, well-being further varied by region with the South reporting the worst well-being levels (M = 2.2, SD = 3.0). Distress scores were highest in Louisiana (M = 6, SD = 1.41) and Missouri (M = 3.9, SD = 2.6), but lowest in Hawaii, Montana, and Nebraska (M = −2, SD = 0.0). Those who were employed by state agencies had higher risk for adverse events with WBI scores of 2.01 (SD = 3.3) compared with those employed by private agencies (M = 1.43, SD = 2.7). However, there was no evidence of significant differences found between these places of employment. Table 3 includes mean well-being and job stress scores across the demographics.
Mean Well-being and Job Stress Scores for a Sample of U.S. Correctional Nurses Across Demographic Characteristics
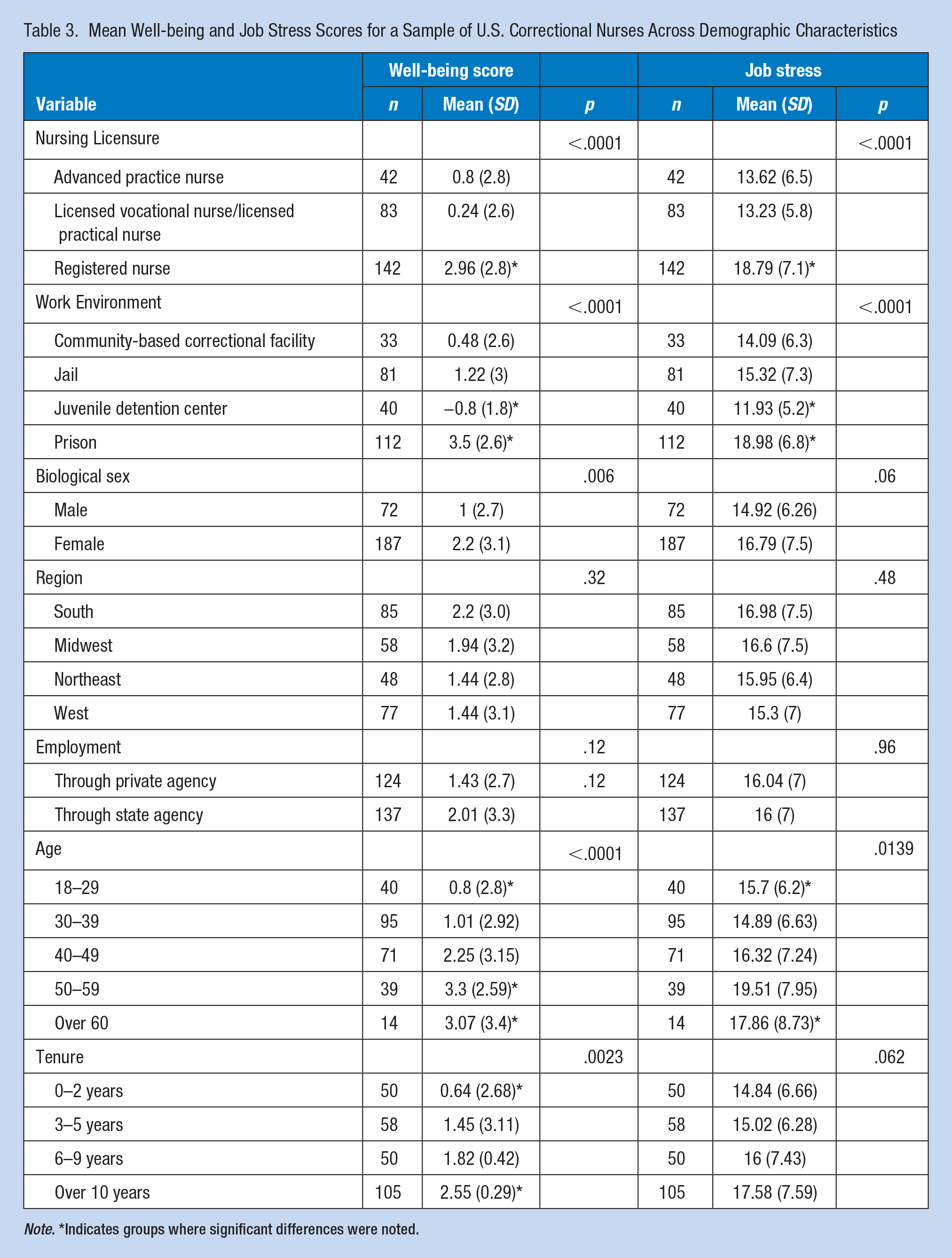
Note. *Indicates groups where significant differences were noted.
Discussion
This study described the job stress, well-being, and organizational characteristics of U.S. correctional nurses. We found moderate levels of job stress among this sample, and evidence that poorer levels of job demands, job control, managerial support, colleague support, and workplace relationships may be related to poorer well-being. Participating RNs specifically reported the highest levels of job stress across the correctional nurse types. This result aligns with other job stress literature of RNs generally, both in the United States (Jordan et al., 2016) and internationally (Alharbi & Alshehry, 2019; Lee et al., 2013), who have reported stress from the PSS-10 as moderate. Correctional RNs may experience moderate job stress due to staff shortages (Russo, 2019) and increasing mandatory and voluntary overtime hours (Caniglia, 2018).
RNs in this study also reported the worst well-being levels of all nursing licensure types (M = 2.9, SD = 2.8). This finding aligns with WBI scoring in the broader RN workforce. For instance, one study measured wellbeing before the onset of the COVID-19 pandemic with the WBI, and nurses’ scores were an average of 2.78 (Meese et al., 2021). Correctional RNs from previous research have also reported a high prevalence of short sleep duration (56.2%, six or less hours per day) and poor sleep quality (31.8%; Zhang et al., 2019). Impaired sleep has been linked to chronic illness, reduced mental health, impaired cognitive function, and lower levels of wellbeing (Steptoe et al., 2008). Thus, poor sleep may be an attributing factor to the lower levels of wellbeing found among correctional RNs in this sample.
Scores of worse well-being, or those at greater risk for adverse outcomes, included those who worked in prisons (M = 3.5, SD = 2.6) compared with other types of facilities. This result may be due to prisons housing those with more serious crimes and for a longer time, compared with those in jails who typically stay for a shorter period of time (i.e., less than a year) (International Association of Forensic Nurses, n.d.; Sawyer, 2019). Thus, the RNs working within prisons may see and interact with patients more regularly over the duration of their sentence, when compared with other nursing groups in this setting (i.e., LVNs/LPNs, APNs), increasing their risk to compassion fatigue, secondary trauma and violence (El Ghaziri et al., 2019; Munger et al., 2015; Newman et al., 2019). Prison nurses must provide care to many people at one time, because there are more people housed in prison than in jail, adding to the duration of time it takes for medication administration, contributing to high job demands (Sawyer & Wagner, 2022). Prison nurses must also manage chronic diseases that require additional treatments and monitoring (University of Southern California, 2019), and coordinate care across multiple services inside the facility. For example, emergency response and triage in prisons may involve more physically laborious activities such as carrying emergency supplies, running to other buildings/units and running upstairs.
Study results have shown that those who worked in the South had higher risk for adverse outcomes and higher job stress. Previous evidence has shown that prisons across 41 states continue to operate above their capacity (Widra, 2020), specifically in the Southern region of the United States, putting additional strain on those who work within those overcrowded systems (Jos & Tompkins, 1987; Widra, 2020). Those working in Louisiana in this study reported the highest stress, which may be attributed to the state’s higher incarceration rates when compared with the whole of the United States. Approximately 1,094 individuals are incarcerated per every 100,000 persons across the 37,100 federal and state prisons and 12,000 local county and city jails in Louisiana alone (Prison Policy Institute, n.d.).
Correctional nurses in this study perceived organizational characteristics as below desirable levels for a healthy work environment. Manager support had the worst average score comparatively (M = 3.13), followed by job demands (M = 3.56), and job control (M = 3.57). These results were similar to those found in one United Kingdom study of 40,000 employees across 39 organizations, including both health care institutions and prison and probation services, where overall averages were less than optimal for job demands (M = 3.02), job control (M = 3.42), managerial support (M = 3.47), peer support (M = 3.80), and workplace relationships (M = 3.77; Edwards et al., 2008). Despite scores in this study where workplace relationships and peer support scored relatively better than the other organizational characteristics, results underscore the room for improvement in each of these five characteristics to reduce job stress in the U.S. correctional nursing environment.
There were a few limitations to this study. First, there was some missing data from a small portion of the respondents. The researchers employed an acceptable statistical method of imputation to manage the missing data (Jadhav et al., 2019), where the lowest (or least impactful) scores for the scales of job stress, well-being, and organizational characteristics were imputed for “preferred not to answer” responses. This method minimizes the influence of data manipulation (Armijo-Olivo et al., 2009), without overestimating worse wellbeing or higher job stress. Second, the cross-sectional design limited the ability to identify cause-and-effect relationships, and the analysis was limited to the information that was collected regarding details of the facility type and health as influenced by job stress. However, establishing cause-effect relationships may be determined in future efforts along with more in-depth exploration of how specifics of each correctional organization (i.e., security level, number of incarcerated individuals), and how objective measures of health (i.e., heart rate, cortisol levels) may influence stress levels and well-being. Third, the timing of study enrollment may have had potential effects on overall findings, as participants completed the study between July and August of 2022, a time when COVID-19 pandemic was still a fluctuating and evolving global concern which may have impacted correctional nurses who were working during the onset of the pandemic.
Implications for Occupational Health Nursing Practice
This work is an essential next step in promoting healthy workplaces across diverse occupational environments and serves as a baseline for understanding the job stress and variation in the well-being levels of U.S. correctional nurses. Specifically, findings show RNs and those working in the prison setting are at higher risk for adverse events. Occupational health nurses are positioned to implement targeted interventions that promote health by mitigating the consequences of job stress and improving well-being among this population. For example, they can target stress reduction by promoting mindfulness techniques (Hillhouse et al., 2023), offering sleep promotion education (Zhang et al., 2019), and ensuring robust mental health services are accessible (Chari et al., 2018). They can consider creating cross-training programs for patient safety with other staff (i.e., correctional officers) to foster teamwork and improve workplace relationships (Shelton et al., 2020). Occupational health nurses can advocate for safe nursing ratios and hiring adequate staff to decrease pressure from job demands (Flanagan, 2006; Shelton et al., 2020). In addition, occupational health nurses can support mentorship programs between managers and nurses to enhance feelings of managerial support (Choudhry et al., 2017; Shelton et al., 2018), and positively influence health.
U.S. correctional nurses were found to have wellbeing levels just below the threshold for an increased risk for adverse events. These nurses also reported experiencing moderate job stress in their roles, with room to improve certain organizational characteristics, specifically job demands and manager support. Findings from this research underscore the need to understand how organizational characteristics and job stress interact with wellbeing in this understudied occupational group. Considering ways to reduce job stress and promote wellbeing may help to create a more sustainable nursing workforce.
Supplemental Material
sj-docx-1-whs-10.1177_21650799231207977 – Supplemental material for Unlocking Prevalence Data: Describing the Job Stress and Well-being of U.S. Correctional Nurses
Supplemental material, sj-docx-1-whs-10.1177_21650799231207977 for Unlocking Prevalence Data: Describing the Job Stress and Well-being of U.S. Correctional Nurses by Elizabeth G. Keller, Beverly M. Hittle, Samantha J. Boch, Kermit G. Davis and Gordon L. Gillespie in Workplace Health & Safety
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the International Association of Forensic Nurses (IAFN, No. 1014248) and the University of Cincinnati Education and Research Center (ERC) Pilot Research Project (PRP) Training Program. In addition, Elizabeth Keller is supported by the National Institute for Occupational Safety and Health through the University of Cincinnati Education and Research Center (No. T42OH008432) as a predoctoral trainee in occupational health nursing.
Human Subjects Review
This research was approved by the University of Cincinnati Institutional Review Board (IRB) on May 5, 2022 (ID #: 2022-0372).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.