
Abstract
Background:
Decreasing emissions of the global healthcare sector will be an important tool for decreasing the magnitude of climate change. The environmental practices of nurses can have a positive environmental impact. The purpose of this study is to identify environmental practices performed by nurses while at work and home along with their associated factors.
Methods:
This study is a cross-sectional descriptive study conducted by surveying nurses from two public hospitals in Lambayeque, Peru. We utilized the Nurses’ Environmental Awareness Tool to collect information about nurses’ knowledge on environmental impacts, their risk to health, and environmental behaviors at both work and home.
Results:
Of the 106 participants who responded, the average age was 41 years, and 29 (28%) worked in surgical services. A little more than half of nurses reported appropriate energy use (51%) and recycling (53%) at work, while 94 (89%) implemented environmental biosafety. There was an observed association between age and years of employment with appropriate energy use, recycling, implementation of environmental biosafety, appropriate chemical substance use, and preventing medication waste.
Conclusion:
Nurses reported a favorable tendency toward adequate environmental practices at work and at home. However, more studies are needed to identify the factors that increase nurses’ use of these practices.
Applications to Practice:
As one of the most trusted professions, professional nurses have an opportunity to play a pivotal role in promoting environmental health and practices in both the workplace and their personal lives. This study highlights areas of potential intervention in the workplace to develop and promote appropriate environmental practices by nurses to decrease pollution by the healthcare sector.
Keywords
Introduction
The worldwide healthcare industry consumes an average of $5.3 billion of non-renewable energy per year and 13 kg of waste produced per bed per day (Cook et al., 2019). Even though major improvements in environmental practices must be part of a national policy and institutional commitment, professional nurses and other staff are likely to play important roles within healthcare settings (Collins & Demorest, 2022; Demorest et al., 2019). The healthcare sector often relies on non-renewable energy sources, which leads to an increase in greenhouse gas emissions compared with alternative renewable energies; use of green energies should be promoted, while maintaining energy conservation processes and striving to be as energy efficient as possible (Saleem et al., 2022). In one Australian study, renewables made up less than 5% of the total energy mixture of hospitals (Burch et al., 2021). Hospitals produce many types of solid, chemical, and hazardous waste materials. The relationship between clinical services and these characteristics determines a hospital’s environmental impact, and the health risks posed to employees, patients, and the general population (Collins & Demorest, 2022; Corvalan et al., 2020). However, nurses can be essential change agents within the healthcare system through the promotion of green activities that favor the planet, which is a role recognized across nursing scholarship (Cook et al., 2019; Schenk, Potter, et al., 2021; Terry et al., 2019).
Different organizations have established guidelines and suggested interventions for health professionals for providing high-quality and safe care in the context of climate change (Kangasniemi et al., 2014; World Health Organization, 2020, 2021). In hospitals, nurses engage in environmentally positive practices (Álvarez-Nieto et al., 2017) such as reducing electrical energy consumption by turning off lights and unused devices, such as monitors, pumps, and equipment (Kwakye, 2011; Topf, 2005); using running water in a reasonable way (Burg & da Silveira, 2008; Somner et al., 2008; Topf, 2005); the consumption of non-toxic purchasing products and materials that are easy to recycle and reduce waste (Melamed, 2003; Riedel, 2011); and the management of disposable medical waste (much of it plastic) in operating rooms (Conrardy et al., 2010; Kwakye, 2011; Melamed, 2003; Mostafa et al., 2009).
Developing countries have vast economic and social inequalities when compared with developed countries that affect standardized environmental practices (Lund, 2019). For example, a simple technological innovation in the design of sanitary taps in hospital operating rooms could save 3 × 106 kWh of energy in water heating costs each year (Somner et al., 2008). However, this and other positive changes require multiple influences to achieve positive change related to the sustainability of the healthcare sector. Some of these include mandates from local governments to decrease emissions (Mercer, 2019), hospital leadership ensuring that financial resources are available to decrease emissions (Burg & da Silveira, 2008; Krüger et al., 2017), and conducting quality improvement projects to identify and implement environmental sustainability within the various settings (i.e., clinical vs. foodservices) of hospitals (Burg & da Silveira, 2008; Carino et al., 2020).
Changes made by nurses related to their environmental practices can improve environmental impact indices (Campbell-Lendrum & Corvalán, 2007; Goodman, 2015). However, in developing countries such as Peru, it is still necessary to explore nurses’ knowledge of environmental practices and the possible reasons for conducting these practices and thus be able to recommend the necessary conditions for the successful implementation and development of the environmental-friendly policies and guidelines in nursing practice. The purpose of this study was to characterize the environmental practices conducted by nurses and the enabling factors associated with these practices.
Methods
This study was a cross-sectional descriptive study of nurses’ environmental practices and enabling factors at work and home.
Population and Sample
The population consisted of 35 nurses from Hospital Provincial Docente Belen de Lambayeque (Hospital A) and 158 from Hospital Regional Docente las Mercedes (Hospital B), for a total population of 193 nurses. Hospital A and Hospital B are Levels II-1 and II-2, respectively. Complexity Level II-1 are facilities with resolution capacity that provide outpatient care, emergency care, hospitalization, obstetric center, surgical center, medicine and rehabilitation, diagnostic imaging, clinical pathology, pharmacy, chemotherapy center and blood bank, nutrition and dietetics, and sterilization center. Complexity Level II-2 includes the resolution capacity of Level II-1, as well as intensive care units and pathological anatomy. Nurses were included in the study if they had worked for more than 3 months in the operating room, general med/surg, pediatrics, gynecology, or emergency departments.
Measures
We used the Nurses’ Environmental Awareness Tool (NEAT; Schenk et al., 2015, 2016), which consists of 27 questions with the objective to measure nurses’ knowledge of environmental impacts, their risk to human health, and ecological behaviors at both work and home. Validation of NEAT for our context was done by the expert opinions of two generalist inpatient nurses with quantitative research experience and one physician epidemiologist with quantitative research experience. Kendall’s coefficient of concordance (p < .05) was used to measure the validity of the survey, and Cronbach’s alpha was used to measure reliability (α = .791). The categorization of scales was maintained: energy and water management, solid waste management, and toxic chemical management (Schenk et al., 2015). The scale of energy and water use consisted of 10 questions that were categorized as appropriate electrical energy management, appropriate water management, and the use of green vehicles. The scale of solid waste management consisted of 10 questions that were categorized as appropriate solid waste management, recycling, and environmental biosafety. The scale of toxic chemical management consisted of seven questions that were categorized as appropriate chemical management, appropriate toxic solution management, and avoiding medication waste. Scores were grouped by the response rates of never or almost never, rarely, and sometimes representing inappropriate or incorrect management and frequently and always or almost always as appropriate or correct management according to the corresponding definition.
Permission was received from the directors and managers of each hospital’s nursing departments to conduct interviews by appointment, with each appointment lasting 10 to 15 minutes. When finished, the interviewer verified that the questionnaire was complete. The study protocol was approved by the institutional review board of the Medical Faculty at the Santo Toribio de Mogrovejo University in Lima Perú. Each participant was provided with an information sheet about the study at the time of data collection. The study followed the ethical principles of the Helsinki declaration.
Statistical Analysis
Statistical analysis was performed utilizing Stata v.16.0 (StataCorp, 2019). The continuous variables of age and work years were analyzed using means with standard deviations. Categorical variables were presented as absolute and relative frequencies. Bivariate analysis used the Student’s t test and compared the continuous variable of those who met versus those who did not meet each subscale of the NEAT. Generalized linear models (GLM), Poisson distribution family with robust variance, and log link function were used to estimate prevalence ratios(PR’s). The PR compares those who met versus those who did not meet each subscale of the NEAT for the independent variables age and working time. A significance level of 5% and 95% confidence intervals were considered.
Results
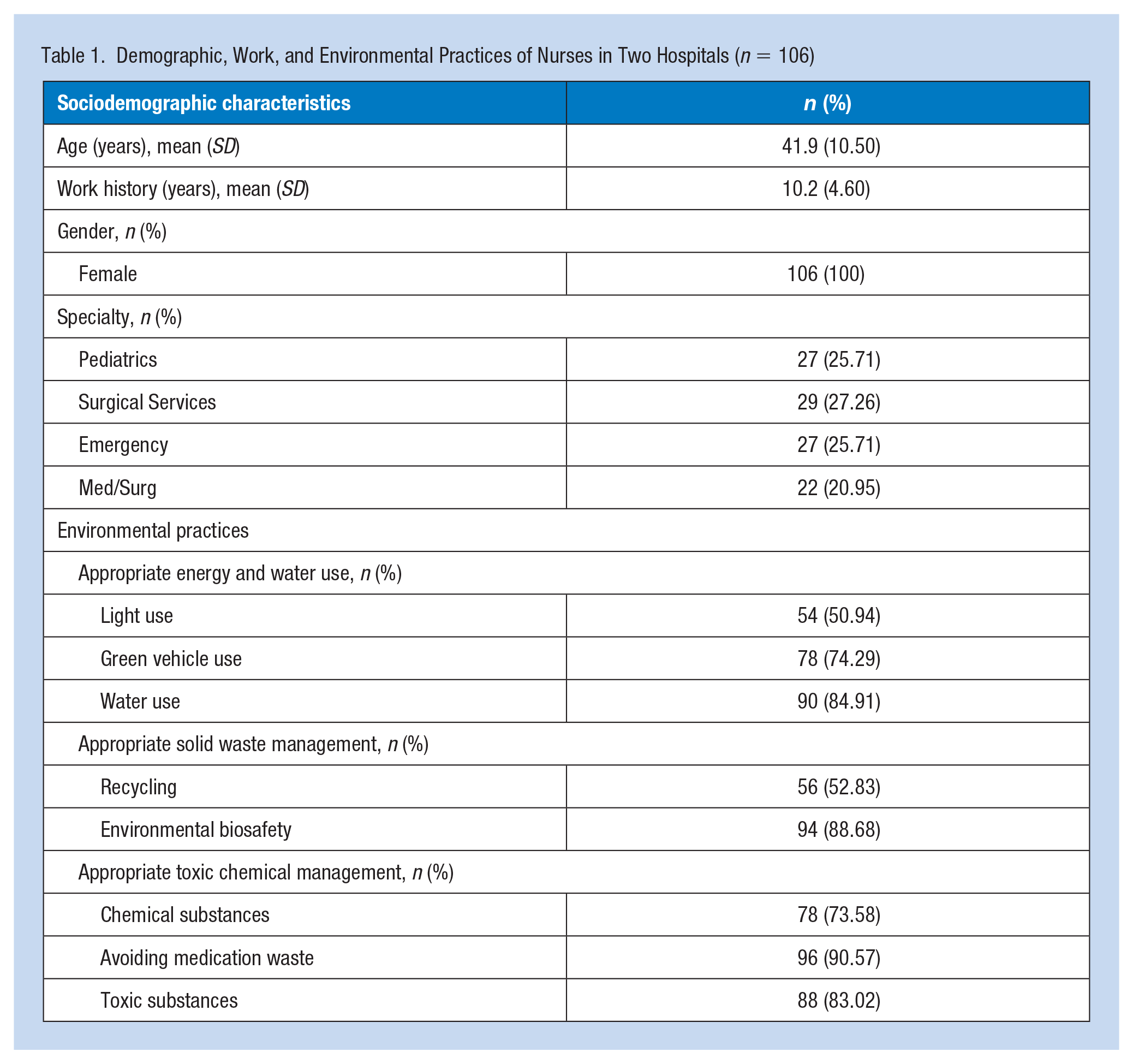
The final sample size consisted of 21 nurses from Hospital A and 85 nurses from Hospital B for a total sample size of 106 nurses. Nurses were recruited using a convenience sampling method, with a response rate of 88.4% nurses. A total of 106 nurses were included in this study, and all were female. The average age of nurses who participated in this study was 41.89 years (SD = ±10.50), and the majority worked in surgical services (25.71%). Approximately half of nurses reported appropriately using lights (i.e., turning off lights and utilization of natural light when possible; 0.94%) and recycling (52.83%). Most nurses reported appropriate environmental safety practices (88.68%; Table 1).
Demographic, Work, and Environmental Practices of Nurses in Two Hospitals (n = 106)
The Student’s t test showed that there was a tendency to have appropriate environmental practices for nurses who were older in age and had more years of services. Nurses with more years of service were observed to have statistically significant increase in appropriate light and water use, environmental biosafety, and avoiding medication waste with respect to those who did not have appropriate environmental practices, and older nurses had an adequate application of environmental biosafety, avoidance of medication waste, and adequate handling of toxic substances (Table 2).
Description of Environmental Practices by Age and Years of Service
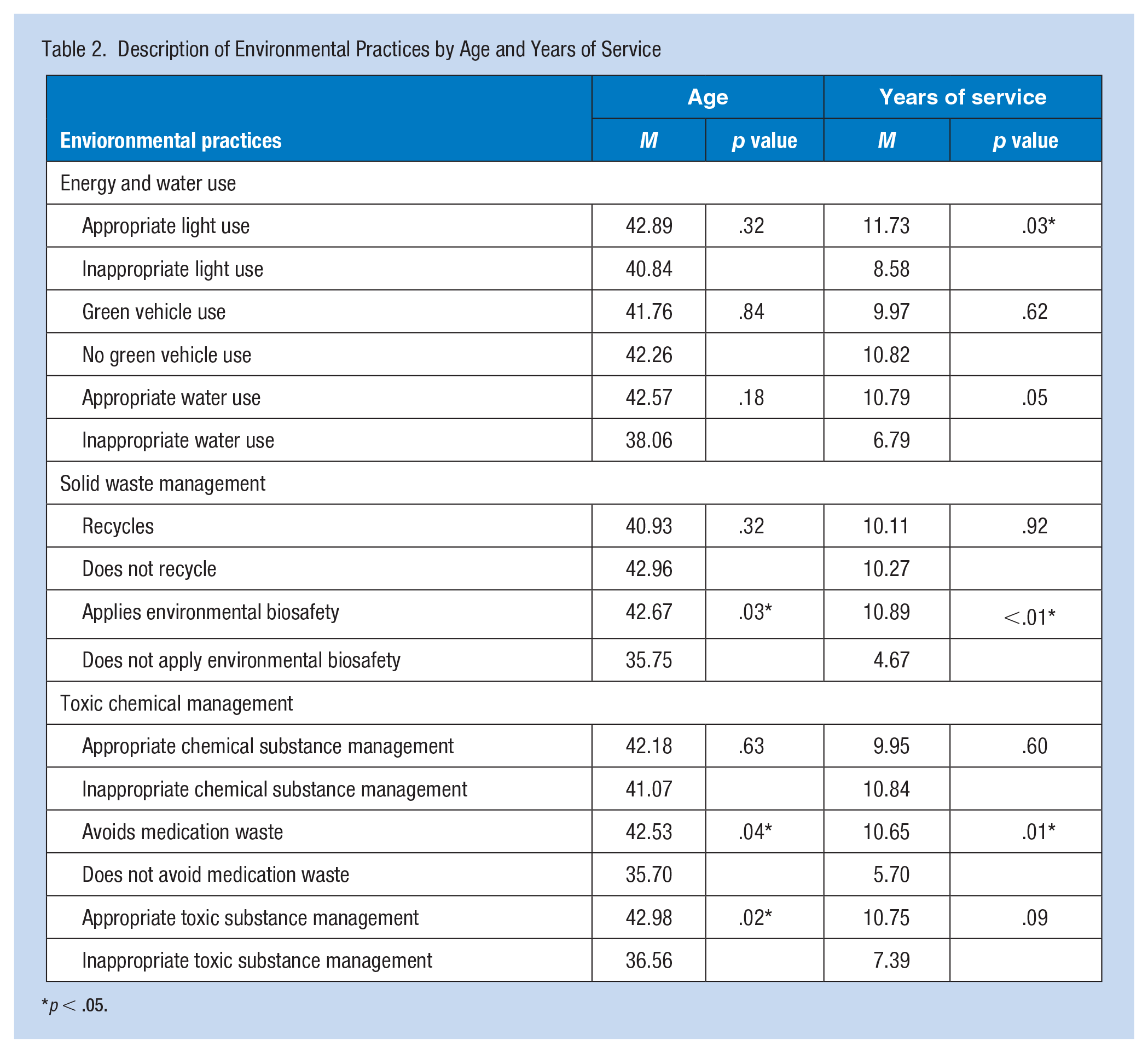
p < .05.
Regression analyses showed that for each year of increased age, the probability of applying environmental biosafety increased by 1% (PR: 1.01; 95% confidence interval [CI]: [1.00, 1.02]; p = .038) and the probability of appropriately managing toxic substances increased by 1% (PR: 1.01; 95% CI: [1.00, 1.02]; p = .021). Furthermore, for each additional year of service, the probability of adequate light use increased 3% (PR: 1.03; 95% CI: [1.03, 1.05]; p = .017), the probability of applying environmental biosafety increased 1% (PR: 1.01; 95% CI: [1.00, 1.02]; p = .003), the probability of avoiding medication waste increased 1% (PR: 1.01; 95% CI: [1.00, 1.02]; p = .011), and the probability of appropriately managing toxic substances increased 1% (PR: 1.01; 95% CI: [1.00, 1.02]; p = .043; Table 3).
Association Between Age and Years of Services With Environmental Practices
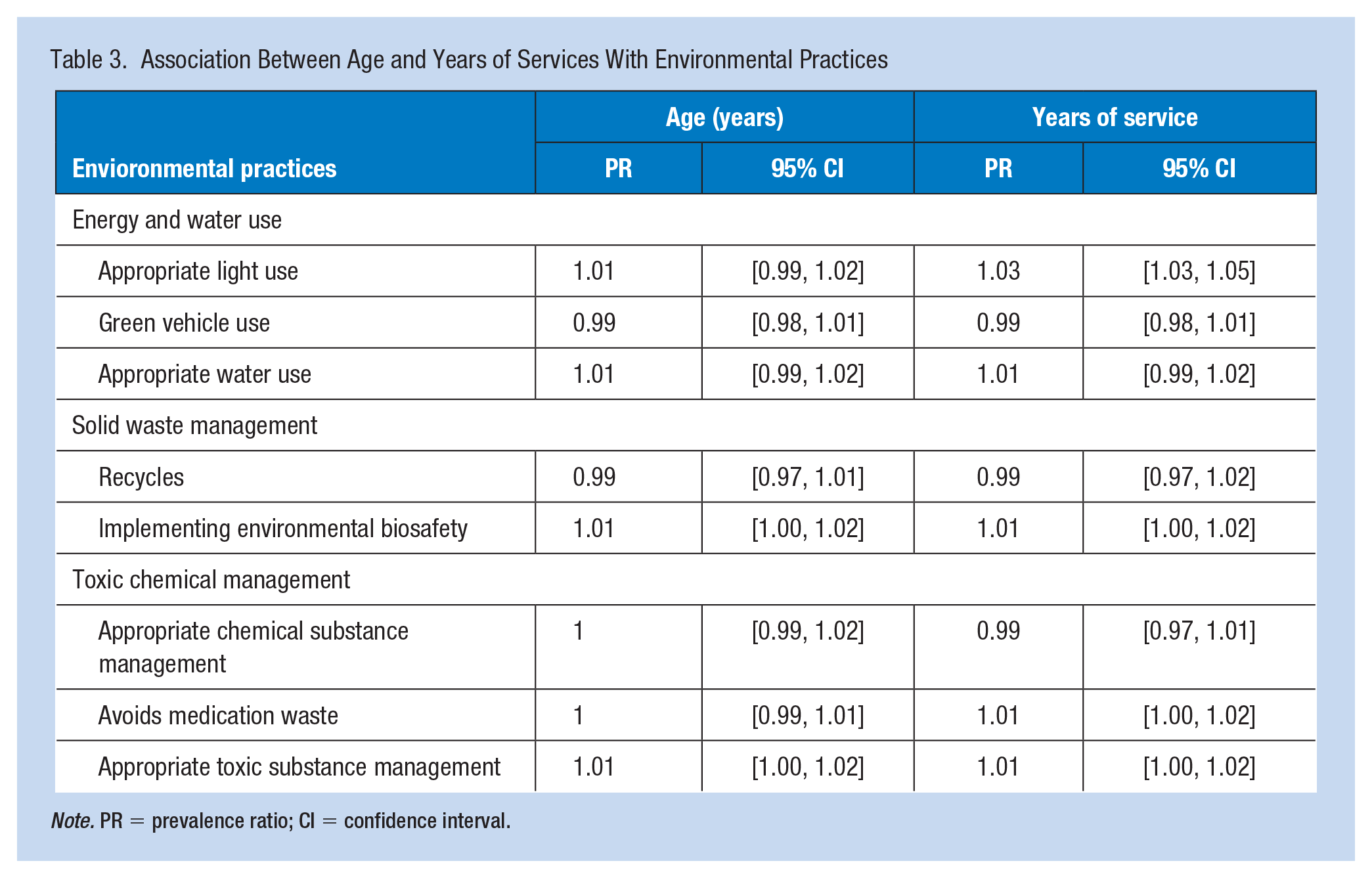
Note. PR = prevalence ratio; CI = confidence interval.
Discussion
We found that nurses carry out appropriate environmental practices with respect to the management of electricity, water, solid waste, and chemical and toxic substances. Age and years of service partially explains the predisposition toward having better environmental practices. The least frequently used practices were appropriate use of lights and recycling, which could indicate a knowledge deficit about appropriate light use or could also be caused by the particular conditions in each hospital that frequently prevent natural light’s ability to enter the facility. On the contrary, knowledge about recycling could be lesser due to lack of established recycling programs and/or norms. Recycling could also be less frequent due to not having environments that favor practicing recycling due to the time restraints and pressures that exist in nursing practice (Campbell-Lendrum, & Corvalán, 2007; Cook et al., 2019). It will be necessary to further explore these characteristics to determine factors that will be susceptible to interventions conducted at the systems level within hospitals and accompanied by education and economic incentives at the individual level.
Future research could also explore possible driving forces for behavior change that promotes a positive environmental impact. George et al. (2017) identified that nurses practice an essential role in multiple activities that mitigate the effect of respiratory diseases associated with climate change. One study conducted in both the United States and United Kingdom provided evidence that leadership skills and activism of nurses can promote sustainable health programming related to environmental health (Terry et al., 2019). Likewise, a study utilizing the CHANT tool with U.S. nurses found that a considerable number of nurses recognized the importance of climate change and its impact on health. However, few participants had appropriate environmental practices at work (Schenk, Cook, et al., 2021). These results highlight the importance of nursing’s role in optimization of patient care and their work environments by standardizing processes related to environmental health.
The results of this study also suggest that, while nurses who are both older and have more years of nursing experience appear to have more appropriate environmental practices, the reported characteristics of appropriate light use, recycling, application of environmental biosafety, appropriate use of chemical substances, and avoiding medication waste were not statistically significant to provide recommendations in respect to hospital management. We did not find a previous study that has reported these results, but believe that more time in services, training, and social responsibility is occurring as time goes on for nurses within hospitals. It is necessary to further explore these characteristics in future studies. Nonetheless, this study serves as one of the first analyses of environmental practices within Peruvian hospitals.
The environmental impact is dependent upon multiple factors within the clinical environment, but nursing’s role has been recognized as an essential component of promoting a positive environmental impact due to leadership characteristics and positioning at the frontline of clinical services (Cook et al., 2019). For individuals, improving specific practices related to electricity and water use could help to mitigate healthcare’s environmental impact. Nurses can positively influence the reduction of hospital waste by being informed about biohazardous waste produced while providing care, such as needles, catheters, body fluids, and so on. Validation of NEAT has been completed with Spanish-speaking populations, such as the one in this study, with a Cronbach’s alpha greater than .90 (Luque-Alcaraz et al., 2022). As such, having a baseline representation of the nurses’ environmental awareness allows for the application of teaching methods on environmental awareness to change nurses’ environmental awareness in the short term with long-term analysis following.
Limitations
The cross-sectional design of this study does not permit that causality can be inferred between the association of the included variables. The convenience sample limits the generalizability of these findings to a broader population. Likewise, nurses included in this study only worked in the inpatient setting, and it is possible that nurses working in other settings could have different environmental health practices that should be explored. The sample size of this study also inhibits our ability to adjust for potential confounders. Finally, the data collected in this study are representative of nurses who work within a single geographic region of Peru, and due to cultural and socioeconomic factors, which may be distinctly different from other regions of the country.
Conclusion
There was a favorable tendency toward appropriate environmental practices within nurses’ clinical practice in this study. There are minimal differences in the frequency of these practices with respect to nurses’ age and years of service. It is important to further explore the characteristics of nurses that could optimize environmental health practices in the workplace, propose educational programming related to institutional environmental health initiatives, and national environmental protection policies. Nursing’s role in these initiatives will be vital for providing concrete clinical guidelines for appropriate environmental practices.
Applying Research to Occupational Health Practice
Half of the nurses already adequate use of energy and recycling, and the vast majority implement environmental biosafety, appropriate use of chemical, prevention of drug waste, and use of environmental-friendly transportation. Some nurses need training to help them understand the connection between climate and health and generate environmental awareness. However, the government should implement sustainable policies in management by adhering to the Global Green Hospital Network https://noharm-global.org/issues/global/global-green-and-healthy-hospitals Initiatives should include sustainability offices or committees, carbon footprint reduction for reducing energy consumption, and/or using renewable energy. Additionally increasing recycling to minimize its generation and encourage a circular economy as well as reduction in water consumption must also be considered.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was given by the institutional review board of the Medical Faculty at the Santo Toribio de Mogrovejo University in Lima Perú.