
Abstract
Background:
Healthcare organizations need to attract and retain qualified nurses, and break areas may influence nurse engagement with breaks, but this has not been studied in situ. The goal of this study was to understand nurse perception of breaks and ways building design and culture impact the frequency, duration, and location of nurse breaks.
Methods:
This was Part 1 of a two-part study. Mixed-method approaches included on-site behavior mapping, focus groups, online survey, and break room usage rates analysis.
Findings:
In this study, nurses did not take restorative breaks but focused on quick “bio” breaks in rooms nearest the central nurse station. When nurses left care floors, they preferred the cafeteria and outdoor eating spaces.
Conclusion:
Nurses’ proclivity to minimize restorative breaks remains a major organizational concern. Future studies should investigate leadership activities impacting nurses’ perception of shifts and break-taking behavior.
Application to Practice:
By optimizing the break setting and changing the cultural perspective of breaks, occupational health services and healthcare management can support nurses’ engagement in restorative activities.
Keywords
In the wake of the global pandemic and as inpatient acuity continues to climb, the need to attract and retain qualified, engaged nursing staff is mission-critical to healthcare organizations (Khan et al., 2019). Nursing work is physically, cognitively, and emotionally demanding, compounded by a perennial nursing shortage, aging nurse demographics, and high rates of turnover (Fact Sheet: Nursing Shortage, 2020). A significant portion of the interdisciplinary healthcare workforce consists of registered nurses (RN), and the loss of RNs directly impacts the quality of patient care as well as organizational operating costs and efficiencies (Halter et al., 2017). The literature provides insight as to how organizations might mitigate the effects of high job demands, including staffing ratios and patterns, “buddy” support systems, and organizational regulations that require breaks for nursing staff (Lake et al., 2020; Nejati et al., 2016). The effectiveness of rest breaks as amelioration for fatigue and improving performance is well-documented in other settings, but notably, there are no U.S. federal regulations mandating breaks for hospital nursing staff (Nejati et al., 2016; U.S. Department of Labor (1961a) 29 CFR 785.18: Rest, 1961; U.S. Department of Labor (1961b) 29 CFR 785.19: Meal, 1961). At the state level, less than half of U.S. states have laws protecting workers’ legal rights to breaks (The Joint Commission, 2012). Labor unions may also bargain with employers in good faith on subjects relating to working conditions (National Labor Relations Act, 1935), providing a means of ensuring rights to breaks. Unions may also influence legislation—for example, the California Nurses Association sponsored S.B. 1334 (authored by state senator Steven Bradford) that would guarantee enforceable breaks for public-sector workers who provide or support direct patient care in a hospital, clinic, or public health setting (California Nurses and Caregivers Applaud New Meal and Rest Break Law Signed by Governor Newsom, 2022). Nevertheless, the cultural norms around—or rather, against—taking breaks act as a major barrier to nurses fully tending to their own needs via rest breaks; for example, one qualitative study found that nurses viewed eating (not respite) as the primary purpose of breaks and further that they viewed breaks as a luxury and not a right (Landis et al., 2021).
Literature Review
Proactive “care for the caregiver” is a long-standing focus area, with increased attention due to the COVID-19 pandemic. The emotional demands of caring for others who are suffering can lead to compassion fatigue, which negatively affects both physical and mental health of nurses (Salmond et al., 2019). A systematic review of qualitative studies examining nurses’ experiences with compassion fatigue (Salmond et al., 2019) found, for example, that compassion fatigue led some nurses to call in sick or find other positions (Mackusick & Minick, 2010). One interviewed nurse reported that their work-related anxiety presented as abdominal issues and that they had sought medical care before considering that their work was making them sick, and ultimately being diagnosed with and treated for anxiety (Salmond et al., 2019; Spinelli, 2011). In their review, Salmond et al. (2019) found that some nurses experiencing compassion fatigue also experienced headaches, heaviness in the chest, aches and pain, and sleep difficulties (among other complaints), marked by the inability to refuel.
Along with compassion fatigue, chronic occupational fatigue can negatively impact nurses’ health. Stress levels and other psychosocial factors have been linked with higher levels of chronic occupational fatigue (Rahman et al., 2016), and both general fatigue and chronic occupational fatigue have been associated with greater odds of developing pain and work-related musculoskeletal disorders (Ibrahim et al., 2019; Younan et al., 2019).
Some organizational-level recommendations for preventing and mitigating chronic fatigue and increasing job satisfaction include providing education programs for coping, relaxation, and sparing time for self; a supportive work environment that is compassionate and caring for nurses as well as for patients; allowing for schedule or assignment changes to relieve a stressed nurse; and encouraging formal and informal breaks (Salmond et al., 2019; Yılmaz & Üstün, 2018).
The physical environment of the rest break area has been shown to influence nurse engagement in breaks and their overall job satisfaction (Happell, Dwyer, et al., 2013; Nejati et al., 2016). While the hypothesized and apparently positive effect of breaks is such that more than 90 papers have been published since 1990, the moderating factors remain poorly understood (Wendsche et al., 2017). Fortunately, we are gaining an understanding of what makes for a “restorative break.” In a 2016 questionnaire-based study on breaks with nurse members of the Academy of Medical-Surgical Nurses (n = 893), Nejati and colleagues (Nejati et al., 2016) found that 10.3% of the variance in reported total break minutes per shift (M = 35 minutes, SD = 16.1 minutes) was related to environmental qualities of break spaces, such as proximity to non-meal break space, outdoor break space, and satisfaction with break areas (p ≤ .05).
In this same study, the participants reported an average of 27.7 minutes for meal breaks (SD 10.9) and an average of 7.1 minutes for non-meal breaks (SD 6.6). Notably, more than 50% of participants reported that their only breaks were meal-related. In addition, 25.9% of the variance in nurse satisfaction with indoor break areas was related to amenities such as equipment, appliances, and furniture (15.5%); environmental features such as plants, artworks, windows, and access to outdoor spaces (7%); and views to specific outdoor elements such as buildings or landscapes (3.4%, p ≤ .05). Nejati and colleagues’ work (Nejati et al., 2016) is the first of its kind to examine the relationship between break area design and perceived break time and satisfaction. However, it remains unknown if this correlation persists in situ, nor is it known whether nurse break behavior or perception, and therefore engagement, will change given the built environment “optimization.”
This is the groundwork for this timely case study of nursing behavior during nurse breaks; for in the COVID-19 era, healthcare systems are creating spaces specifically designed to help nursing staff relax and recharge during shifts (Bean, 2020). Findings from this study will inform hospital administration, including the occupational health service, and design teams to create opportunities and spaces for nurse breaks that positively influence nursing engagement and satisfaction, reduce turnover, and improve the overall quality of care.
Methods
The research team followed a mixed-methods approach for this 2-year, two-part longitudinal study. The overall goal was to identify cultural and environmental qualities impacting nurse engagement and satisfaction with restorative breaks. Part 1 (reported here) was to understand nurses’ perceptions of breaks and identify how, when, and where nurses took breaks. In addition, Part 1 sought to test whether a break room’s furniture and amenities affected its use by nurses. Institutional review board approval was secured before data collection began. Findings from the full study will inform future research investigating the impact of the critical affordances identified.
Nurses completed an online survey based on Nejati and colleagues’ study (Nejati et al., 2016) which focused on restorative design features for hospital staff break areas. Participants for the focus group and online survey were recruited via a flyer and recruitment presentation by the research investigators. Behavior mapping was conducted for 5 consecutive days at typical break times identified by nurse managers (these times were): 9:00 am, 1:00 pm, 4:30 pm, and 12:00 am. For location and behavior mapping, the nursing role was identified by scrub color; no other identifying information was obtained. Because behavior mapping data were completely anonymous, the exact nurse shift start times and lengths could not be determined or otherwise matched to the behavior mapping. A prescribed route was followed from the main floor of the medical tower to the upper Floors 4 and 5 (Zeisel, 2006). An online behavior mapping tool (https://bmapit.com) allowed the study team to conduct location and behavior observations inconspicuously, resulting in heat maps identifying the usage of break areas over time. Break room usage was also analyzed from de-identified card reader access for the break rooms on Floors 4 and 5.
Nurses engaged in on-site focus groups using user-centered design thinking techniques to gather nurse perceptions regarding engagement and satisfaction with breaks and break areas (Lorusso et al., 2021). Design thinking is a collaborative method that is human-centered, empathetic, and focused on the people at the center of a core issue. Qualitative research approaches which incorporate important aspects of the human-centered design include ethnographic interviews, observations, and behavioral mapping (Lorusso et al., 2021).
Setting
This study was conducted within a single medical tower on two architecturally identical medical-surgical inpatient units (Floor 4 and Floor 5) in Northeast Florida. The investigated break areas included meal-break and lounge-break rooms on Floors 4 and 5 as well as other areas within the medical tower that could be used during a break including the cafeteria, open lounges, open air courtyards, balconies, and a fitness area. The location and proximity of the meal-break and lounge-break rooms in relation to the central nurse station and view of the outdoor environment are identical on Floors 4 and 5 and are constant variables (Figure 1). While the relative location and proximity of the meal-break and lounge-break rooms to the central nurse station were constant between floors, furniture and amenities within the break areas varied between floors (Figures 1 and 2). The windowless meal-break rooms are 20 feet from each central nurse station and include a refrigerator, microwave, TV, and table and chairs (Figure 1).
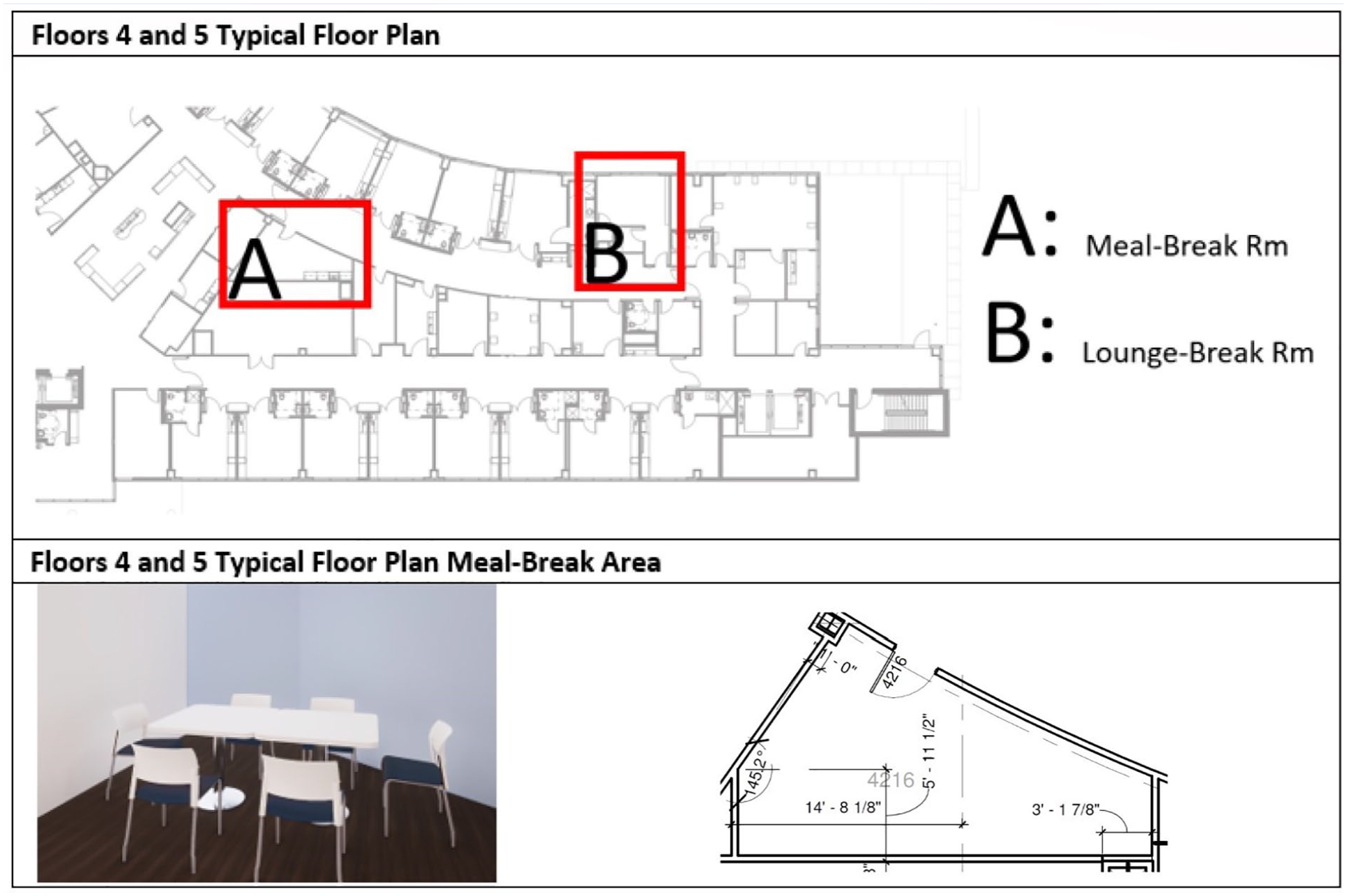
Top Pane: Typical Floor Plans Showing Relative Positions of Meal-Break and Lounge-Break Rooms. Bottom Pane: Meal-Break Room Layout.
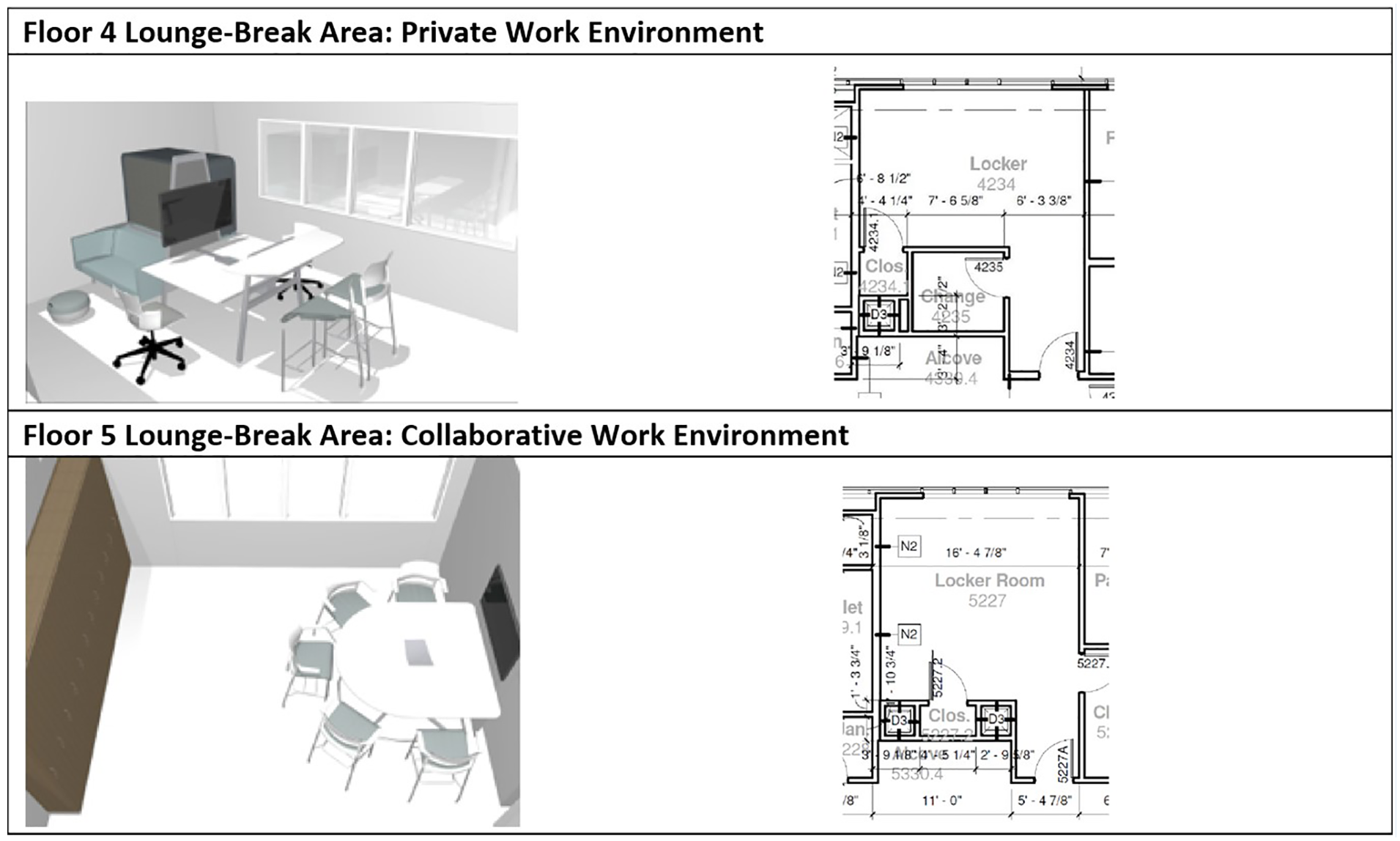
Work Environments Within Lounge-Break Area.
The lounge-break rooms are along the same path as the meal-break rooms and are at the far end of the ward, approximately 90 feet from the central nurse area, with a view to the outside, lockers, changing areas, and additional furniture amenities (Figure 2). The furniture amenities within the lounge-break rooms differ by floor. Floor 4 provides a private work environment with a couch and enclosed, visually semi-private seating arrangement (Figure 2), and Floor 5 provides a collaborative work environment with a single, semi-circular, bar-height table and chairs with a TV (Figure 2).
Results
Sample
At the time of the study, 374 nurses met the eligibility requirements of being employed in the medical tower for at least 3 months; of the nurses, 11.2% were male. Fifteen nurses (14 female) consented to participate in the focus group consisting of staff nurses (n = 10), nursing supervisors (n = 2), a wound care nurse (n = 1), a rapid response nurse (n = 1), and a nurse educator (n = 1). Twenty-eight (27 female) nurses participated in the anonymous online survey consisting of nurse managers (n = 3), nurse specialists (n = 2), a nurse educator (n = 1), and staff nurses (n = 22).
Staff Survey
Using a 10-point Likert-type scale (higher scores are better) to rate each lounge room in terms of how well it relieves stress and makes the respondent feel more refreshed, a Wilcoxon signed-rank test and a mixed effects regression analysis examined the within-subjects effect of each room and found a significant difference in room rating, V = 51, p = .004. The Floor 5 room was rated significantly higher than the Floor 4 room, with a mean (M) and standard deviation (SD) of M = 4.81 (SD = 2.66) and M = 3.86 (SD = 2.30), respectively (see boxplot in Figure 3).

Boxplots Comparing Lounge-Room Ratings Between Floors 4 and 5 on Their ability to Reduce Stress and Refresh.
A mixed effects regression (allowing room ratings to vary between participants) confirmed this finding, revealing a significant effect of the lounge break room in Floor 5 versus Floor 4 rating, b = 1.02, p = .007.
Only the lounge-break rooms were rated on this item (i.e., the room’s ability to relieve stress and refresh); meal-break rooms were not rated on this item because the meal-break rooms did not differ in their configuration or amenities.
Behavior Mapping
The study team predetermined routes near all available break areas in the medical-surgical tower from the main floor through the top floor (five floors total) for consistency in observational paths. Figure 4 provides a visual representation of the behavior mapping results, presented as a heat map overlaid on a floorplan, where more green-hued colorations correspond to lower volumes of nurse presence and activity, and more red-hued colorations correspond to higher volumes of nurse presence and activity. Behavior mapping revealed that both the Floor 4 and Floor 5 lounge-break rooms were underutilized while the more traditional meal-break rooms were highly favored (Figure 4). In fact, of the 20 total observations, nurses were observed only using the meal break rooms and never the lounge break rooms. An outdoor patio on the third floor was used moderately, and the outdoor courtyard and cafeteria break areas on the first floor were highly utilized.

Heat Maps Showing Results of Behavior Mapping Observations.
Lounge-Break Room Usage Rates
Usage rate outcomes are operationalized for this analysis as the total number of visits per staff member (number of visits), the average number of minutes each staff member spent in the Lounge room during their visits (average minutes), the maximum number of minutes each staff member spent in the room (max minutes), and the total duration of hours each staff member spent in the room (total hours). The number of breaks per staff member shift was not captured for privacy reasons.
Due to the highly skewed distribution of outcome variables and overdispersion of data, a series of negative binomial regression models were used to test for differences between Floor 4 and Floor 5 in break room usage. The floor was coded as a binary indicator for Floor 5, where Floor A = 0 and Floor 5 = 1. In each regression analysis, the usage outcome was predicted by floor. The significance threshold was set at α = .05.
There were no significant differences between floors in any of the three duration outcomes (average visit duration in minutes, maximum visit duration in minutes, or total duration of all visits in hours). However, Floor 5 had a higher number of monthly visits per staff member with a mean (M) and standard deviation (SD) of 31.8 and 32.7, relative to Floor 4 (M = 19.7, SD = 36); b = .49, p = .034. Median monthly break room visits were 1 and 24, respectively. Due to the skewness of the data, medians, means, and standard deviations should be interpreted with caution and presented for illustrative purposes only. Nevertheless, the specification of a negative binomial regression model—as compared with a t test, analysis of variance, or other types of linear regression model—was specifically chosen due to its handling of this type and distribution of data.
The majority of staff members had average visits of only approximately 5.5 minutes (Table 1). In addition, the average duration for each break room user’s longest visit was just more than a half hour at 31.5 minutes overall (Table 1). Moreover, staff members appeared to take a small number of breaks in the Floor 4 and Floor 5 break rooms overall, with Mdn. = 2.6, M = 24.1, and SD = 35.2 monthly breaks per staff member.
Break Room Usage Rate Descriptive Statistics
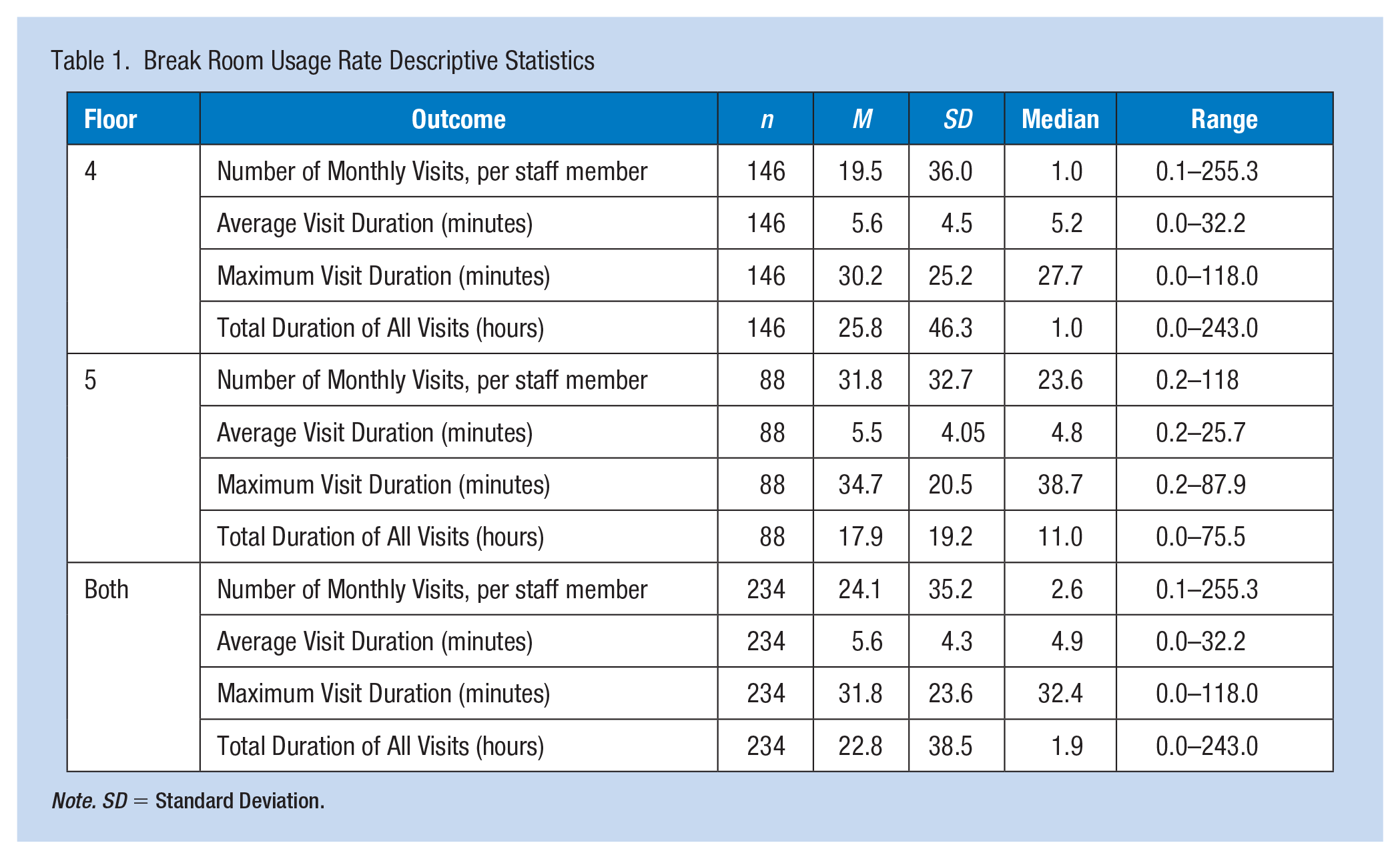
Note. SD = Standard Deviation.
Focus Groups
During a 2-hour session, 15 participating nurses were divided into three groups of five and asked to define nurse breaks and their importance. Participants also provided insights into a typical day in the life of nurses working on floors 4 and 5 and identified optimal break area design features.
Participants overwhelmingly articulated that breaks provided relief from the stress and anxiety incurred from the emotional and physical toll during shifts. In their discussion of break definition and importance, participants described two distinct types of breaks. “Restorative Breaks” were defined as those that allow staff to de-stress and re-charge by experiencing a relaxing sensory experience, uninterrupted and away from the central nurse station. “Bio-breaks” were defined as those that are quick and focus on basic needs like food, water, and toileting. Nurses confessed that due to staffing shortages and an unspoken, universally accepted cultural nuance that “nurses don’t take breaks,” they do not typically take restorative breaks but rather quick bio-breaks. Socializing with colleagues was discussed as an important way to reduce stress by building trust and strengthening team-based camaraderie. While nourishment was mentioned as a critical element of a break, nurses felt that having a space for restorative breaks was important to improve staff shortages, shift expectations, and maintain overall work–life balance.
Nurses identified six major themes for a restorative break environment, including technology (television with shows like HGTV and ample charging stations for laptops and phones), opportunities for nutrition (coffee, a water filling station, and healthy food options), relaxing décor (accent wall colors, serene, nature-based artwork in a space that is well-organized, uncluttered, and clean), access to nature (window with a view of nature and live plants and flowers), and ergonomic furniture that provides physical relaxation (allowing for feet to be elevated as well as massage and reclining).
Discussion
Despite the health system’s efforts to encourage restorative breaks, the lack of nurses’ engagement with restorative breaks was surprising to the study team. Nejati and colleagues’ (Nejati et al., 2016) survey-based work identified key environmental attributes that set up the basis of this study, but these did not hold when isolated from basic human needs: hydration, nutrition, and toileting. These needs should inform the basic requirements of future break rooms. Once bodily sustenance was satisfied, however, nurses demonstrated a preference for the “work-oriented” lounge setting in terms of the number of visits. Upon greater inspection, these nurses were seeking the work–like setting for team meetings, a finding that may be particular to this case study.
The culture of “no breaks” cannot be underestimated. Within this study, even accounting for half-hour breaks or longer, staff members spent small amounts of time in the break rooms. It is a mindset that threatens nurse sustainability and patient safety. Future studies should investigate leadership activities impacting nurses’ perception of shifts and break-taking behavior. Once these core issues are resolved, the restorative nature of break rooms becomes paramount, given their potential influence on break behavior. Focus groups revealed the need for staff’s sense of ownership, attention to sensorial elements, ability to connect with others or “get away” via technological means, and physical rest and comfort. Staff also reported concerns for physical safety—as evidenced by cleaning protocols and clean air exchanges—as part of a restorative break, an unsurprising result of their pandemic experience.
Limitations
Given the sensitivity surrounding break behavior, the number of breaks per nurse per shift and their location were not documented. The dose–response effect of breaks at the level of the individual nurse will not be possible without shift-level variables, and we recognize this as a necessary next step.
Recommendations for Future Research
As noted above, there are strong cultural norms that act as barriers to nurses taking breaks at all, let alone breaks solely for the purpose of rest rather than fulfilling physiological needs. Instead, nurses felt that their responsibility was to their patients first (Landis et al., 2021), preferring to retain availability and accessibility to patients when possible. Some nurses feel uncomfortable or unable to hand over duties and care of their patients so the nurse can take a break (The Joint Commission, 2012; Landis et al., 2021); thus, it is evident that both cultural and organizational shifts will be required to encourage restorative breaks. Future research should investigate the importance and effect of administrative and environmental design interventions on the restorative break, beyond the fundamentals as described. The UF Health North administration is implementing such an effort at the time of this publishing.
Conclusion
Human health and safety are dependent upon the mental and physical state of nurses globally. Attention to the restorative break is part of an ongoing effort to maintain and support this valuable resource—nursing care.
Applying Research to Occupational Health Practice
This study outlines a process for examining the location and amenities of spaces for direct care providers to take restorative breaks. A safe, biologically, and psychologically restorative space is part of the design elements of a nursing unit and allows for nursing staff to quickly reset, if only for a few minutes. It will be critical for nurse leaders to offer permission and even assign breaks when they see signs of a nurse in or headed toward a crisis. The hospital occupational health services should be part of design teams for restorative break spaces.
Footnotes
Acknowledgements
The authors thank Steelcase Health for their partnership and support; at the time of the research, Michelle Ossmann was Director of Healthcare Environments at Steelcase Health.
Author Contributions
Lesa Lorusso, Michelle Ossmann, and Linda Lawson contributed to the study design, literature review, data collection, and qualitative data analysis. Tatiana Orozco contributed to literature review and quantitative data analysis. All authors contributed to manuscript writing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human Subjects Review Details
This research was approved by the University of Florida (UF) Institutional Review Board (#UFIRB201702791).