
Abstract
Background:
Research on burnout in the medical community has extensively studied the impact of mindfulness-based interventions (MBIs), which can include meditation, outdoor retreats, in-person didactics, and/or online wellness modules. However, in addition to these MBIs lacking objective, physiological measures for wellness, there has been little to no research involving virtual reality (VR) as an MBI modality for healthcare professionals in the United States.
Methods:
A randomized controlled intervention trial was used to study the impact of VR-based guided-meditations in the form of brief paced-breathing exercises. Heart-rate variability (HRV), a biomarker for relaxation, was measured during each session. Thirty-two participants, consisting of primarily medical students, resident physicians, and registered nurses, were recruited to complete brief guided-meditations via a VR headset or a standalone mobile app in the emergency department (ED) on-call room of a large urban academic medical center.
Results:
A total of 213 guided-meditation sessions were completed over the course of 4 weeks. Self-reported ratings of anxiety improved in both VR and mobile groups post-study. However, the VR group demonstrated higher intrasession HRV progress, indicating increased state of relaxation that also correlated with the number of sessions completed. Analysis by gender revealed disparity in HRV metrics between male and female VR participants.
Conclusion/Application to Practice:
VR-based guided meditations prove to be a feasible and accessible MBI that does not require extensive time commitment for healthcare workers. VR may be a more effective meditation platform compared with standalone mobile meditation apps, especially when used on a routine basis.
Keywords
Background
In light of the extensive research on burnout among healthcare professionals, wellness in the workplace has become a top concern of hospitals and medical schools. Mindfulness-based interventions (MBIs) are one of the common tools used in the medical community to promote wellness in the workplace. Broadly speaking, mindfulness is a practice in which individuals immerse themselves in the present moment (Kabat-Zinn, 2003). Various physical and psychological benefits have been associated with MBIs such as improvements in blood pressure, heart rate, anxiety, and depression symptoms (Marino et al., 2021). One common way to practice mindfulness is through guided-breathing exercises that are facilitated in-person by a trained professional or via commercially available mobile apps (Schultchen et al., 2021; Zhang et al., 2021).
In medical education, MBIs have been used as a means to improve student well-being, but well-designed studies conducted in the United States remain sparse. In a 2021 Cochrane Systematic Review by Sekhar et al., only 10 MBI studies that focus on medical students and junior doctors met the authors’ eligibility criteria (Sekhar et al., 2021). Of these 10 randomized controlled studies, only 4 were conducted in the United States, and only 1 involved a smartphone-enabled digital app as part of the intervention. Most of the MBI modalities were in the form of in-person didactics, online computer modules, outdoor retreats, group meditations, and self-directed meditations at home. Study durations ranged from 1 week to 2.5 months. Seven studies required weekly attendance of 1 to 2 hour in-person classes. The remaining studies required participation in the intervention for at least 10 to 20 minutes daily. All of the studies used validated scales to measure self-reported impact on the participants’ general well-being. None used objective measures (e.g., blood pressure, heart rate, skin conductance, etc.) to assess the participants’ physiological response to the interventions.
To date, there has been no study that explored virtual reality (VR) as an MBI, while incorporating heart rate variability (HRV) as a biomarker for relaxation among medical students, trainees, and healthcare professionals in the United States. An increasingly popular technology, VR typically involves wearing a headset to immerse the user in a 360-degree digital rendering of a chosen environment. VR has been applied in various settings in healthcare including surgical training, chronic pain management, and physical rehabilitation (Li et al., 2017). Often measured by commercially available wearable technology (e.g., FDA-approved AppleWatch), HRV is a biomarker that can be used to quantify states of relaxation and stress (Nakao, 2019). A systematic review on occupational stress and heart rate variability has shown that occupational stress is associated with decreased HRV and reduced activity of the parasympathetic nervous system (Järvelin-Pasanen et al., 2018). In the review, 10 studies met eligibility criteria and of these, 3 studies examined the impact of occupational stress on HRV of healthcare workers in particular (Borchini et al., 2015; Hernández-Gaytan et al., 2013; Uusitalo et al., 2011). However, they were conducted outside of the United States and were not collected in the context of an MBI.
With VR as an MBI modality and HRV as an objective measurement of relaxation, this study aimed to examine the impact of brief guided meditations in the form of paced-breathing exercises on the well-being of medical students and healthcare staff in the emergency department (ED).
Methods
Overview
This 4-week MBI was a randomized controlled intervention trial that used a 2 × 2 assortment to assign participants either to the VR or mobile group based on the time of enrollment. Participants were asked to complete brief mindfulness-based guided meditations using paced-breathing exercises. This MBI took place at the ED of an urban academic medical center in Washington, DC with an annual volume of approximately 75,000 patients. Enrolled participants, consisting primarily of medical students, resident physicians, and other healthcare ED staff, were instructed to go to a designated area in the ED on-call room to complete their guided meditations.
Participants
Recruitment was performed via emails and after-class announcements. A convenience sample of 45 medical students, resident physicians, nurses, physician assistants, and technicians were recruited in the study. However, only those who completed at least 3 sessions over the 4-week study (32/45, 71%) were included in the final analysis. To be included in the study, participants had to be at least 18 years of age and be fluent in English. Exclusion criteria included neurological disabilities such as epilepsy or stroke, sensitivity to light or motion, current pregnancy, or any injuries that would prevent them from operating a VR headset. The study protocol was approved by the Institutional Review Board. After verbal and written explanation of the study, written informed consent was obtained from all participants.
Prior to beginning the study, participants completed a pre-survey and finished a tutorial with either the mobile or VR application, under the guidance of the research coordinator. They were also briefed on the significance of HRV and how it is an objective physiological measure of relaxation. Their HRV scores would be projected on the screen after each guided-meditation session, with higher HRV scores indicating a more relaxed state of mind than lower HRV scores. Once enrolled, participants were assigned a unique study number, which would allow them to access their respective VR or mobile meditation platform, located in the ED on-call room. Participants were encouraged to complete at least two guided-meditation sessions per week for the entire 4-week study.
MBI
Developed by CoresightsTM, the VR guided-meditation platform, which is also available in mobile version, offers mindfulness-based guided meditations in the form of paced-breathing exercises that approximately last between 3 and 5 minutes. To enable VR mode, users are instructed to login into the Android-operated Samsung smartphone, which they would subsequently dock into the Samsung GearTM VR Headset. The user would then place the HRV biosensor (eVu-TPS heart rate monitor) on their index finger and wear the VR headset with the provided headphones. Mobile users are to follow similar steps without docking the smartphone into the VR headset, since they will be viewing the guided-meditation session using only the smartphone.
Both types of users can choose from 1 of 3 environments: beach, canyon, and forest. VR users can experience these environments with an immersive 360-degree view, while mobile users view them as 2-D images on the smartphone screen. Once the session is started, users will hear calming music and audio instructions that visually sync with an enlarging circle, prompting the users when to breathe in and breathe out. Figure 1 shows the study equipment (VR headset, smartphone, HRV biosensor) and user interface seen by participants during their guided meditations. When the session is over, participants get to see their “HRV score” projected on the VR/mobile screen.

Study equipment (VR headset, smartphone, HRV biosensor) and user interface seen by participants during their guided meditations.
Measured Outcomes
To measure the impact of this MBI on self-perceived well-being, we administered pre/post surveys based on the Anxiety Short Form 8a (PROMIS) on the first and last days of the study. To measure the objective impact on relaxation, HRV was collected using a biosensor integrated into the meditation platform. The primary metrics measured in both VR and Mobile groups include (a) duration of session, (b) session average HRV, and (c) intrasession HRV progress.
Mean session HRV was the average heart-rate variability score throughout an individual session. Of note, this score is based on power spectrum analysis of the low-frequency component of the heart rate variability spectrum (0.06–0.10 Hz) subsampled every 0.05 seconds during a session. Low-frequency band analysis is a common method to determine the effectiveness of breathing exercises on stress reduction (Houle & Billman, 1999). Higher HRV scores reflect a more relaxed state, while lower HRV scores indicate a less relaxed state of mind (Kirk & Axelsen, 2020).
Intrasession HRV progress is calculated by determining the percent change in HRV score during each session. To calculate this, we subtracted the average HRV score of the first half of each meditation session (i.e., initial HRV) from that of the second half (i.e., final HRV) and divided that value by the initial HRV. This was performed to capture the relative progress made by the user on their heart rate variability, after starting each guided-meditation session. Positive intrasession HRV progress values indicate an overall improvement in HRV (i.e., user is more relaxed after the session), while negative values signal an overall decline in HRV (i.e., user is less relaxed after the session).
Mann–Whitney independent sample T-test, Kendall–Tau correlation analysis, and Wilcoxon signed-rank paired T-test were used for statistical analysis.
Results
A total of 45 participants enrolled but only 32 participants (71%), who completed at least 3 sessions, were included in the final analysis. Demographic breakdown of the participants consists of 27 medical students, 2 resident physicians, 1 physician assistant, and 2 registered nurses (Supplemental A).
A total of 213 sessions were completed, of which 117 (55%) were VR sessions and 96 were mobile sessions (45%). On average, VR users (n = 16) completed 7 sessions, while mobile users (n = 16) completed 6 sessions, over the course of 4 weeks (p = .213).
VR Versus Mobile
Mobile sessions lasted 192 seconds versus 200 seconds for VR sessions (p = .134). Session average HRV also did not differ significantly in either group (mobile: 76 vs. VR: 73, p = .229). However, intrasession HRV progress was larger in the VR group than in the mobile group (2.8% vs. −0.24%, p < .001; Figure 2).
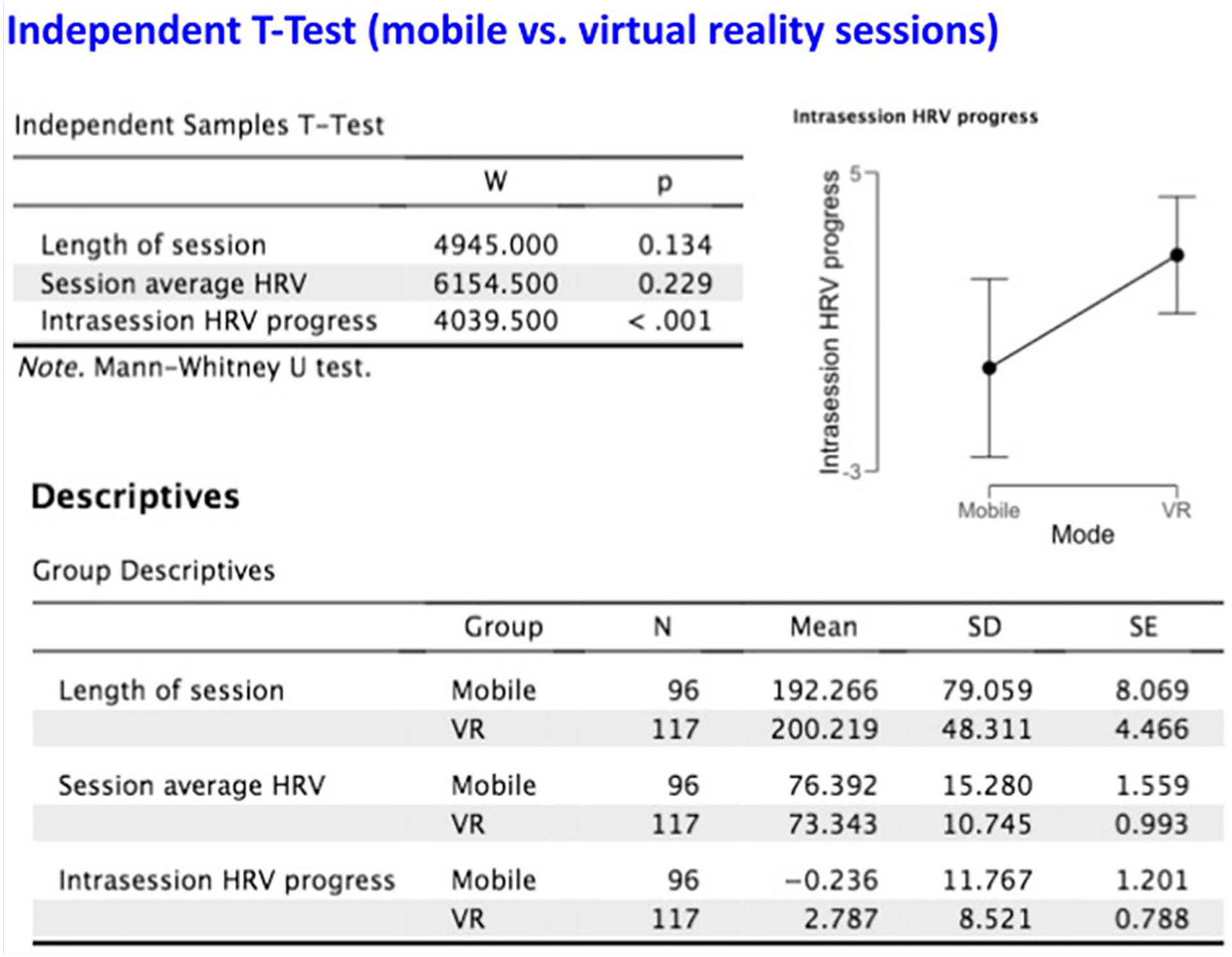
Descriptive statistics for mobile versus VR sessions.
To determine whether ordinal session number (e.g., 1st session, 2nd session, etc.) was associated with our variables of interest, we conducted a Kendall–Tau correlation analysis. When examining all 213 sessions performed in both VR and mobile groups, we found a weak positive correlation (0.157, p < .01) between ordinal session number and intrasession HRV progress (Supplemental B). Ordinal session number interestingly showed a weak negative correlation to length of session (−0.187, p < .001).
When examining VR-only sessions (n = 117), there was a moderate negative correlation between ordinal session number and length of session (−0.220, p < .001). A weak positive correlation between ordinal session number and intrasession HRV progress was noted (0.180, p < .0001). When examining the mobile only group (n = 96), only length of session was associated with ordinal session number (−0.164, p < .05; Figure 3).
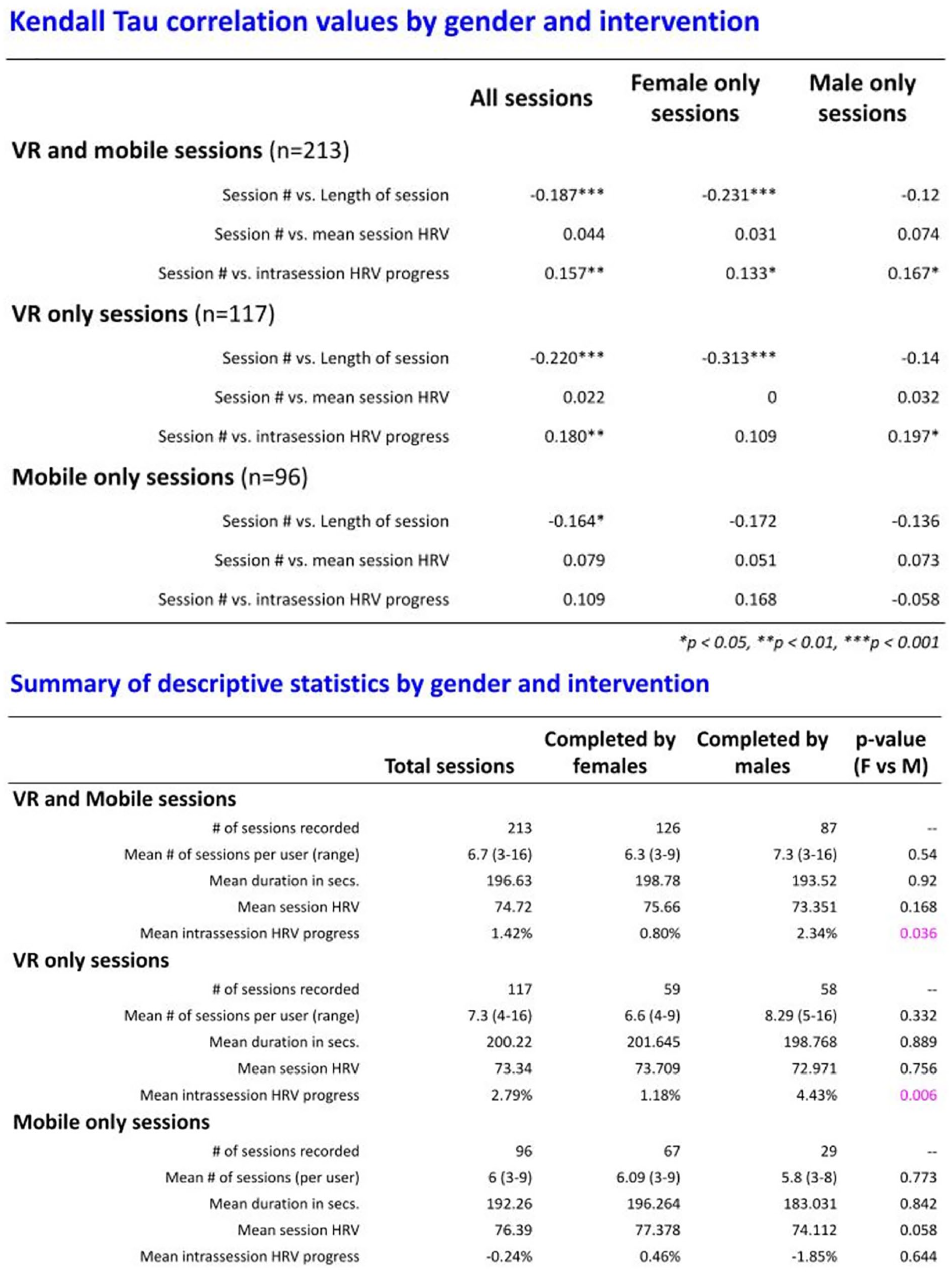
Top: Kendall–Tau correlation values subgrouped by gender and intervention type. Bottom: descriptive statistics subgrouped by gender and intervention type.
Pre-/Post-Surveys
The survey administered to participants prior to and after the study was based on the PROMIS Anxiety Short Form. Both the VR and mobile group respondents reported improvement post-study with perceived anxiety in three out of the five statements (60%) (Supplemental C). Within the mobile group, respondents for “My worries overwhelm me” (p = .02) and “I feel annoyed” (p = .03) showed statistically significant improvement in self-reported ratings.
Gender Analysis
When looking collectively at both VR and mobile sessions (n = 213), sessions completed by males showed higher intrasession HRV progress compared with those of females (2.34% vs. 0.80%, p = .036; Figure 3). In our correlational analysis, we found a negative association (−0.23, p < .001) between ordinal session number and duration of session, when examining sessions completed by females but not those of males. In terms of impact on self-perceived well-being, no significant changes in self-reported ratings were observed within male or female respondents.
Within the VR group, males on average also showed higher mean intrasession HRV progress (4.43% vs. 1.18%, p = .006). In our correlational analysis, sessions completed by females showed strong negative association between ordinal session number and length of session (−0.31, p < .001).
Within the mobile group, mean intrasession HRV progress did not significantly differ between genders (−1.85% vs. 0.46%, p = .644). In our correlational analysis, no significant differences in measured outcomes were noted between sessions completed by females and males.
Discussion
Throughout the 4-week study, a total of 213 guided-meditation sessions were completed, with the majority (117/213, 55%) coming from the VR group. The average number of sessions per user (7 vs. 6) and duration of each session (200 seconds vs. 192 seconds) were both higher in the VR group compared with the mobile group, but the differences were not statistically significant. The level of participation with both mobile and VR meditation platforms was particularly encouraging given that recent research shows how MBIs aimed at medical trainees have not traditionally been successful with retention and engagement. In a 2021 systematic review of online MBIs, Yogeswaran and El Morr (2021) made note of how long-term program usage by medical students was minimal and participation typically diminished during the interventions. We believe the primary reasons for our meditation platforms successfully engaging our subjects include the (a) semi-private and convenient location to complete the guided meditations (i.e., ED on-call room), (b) on-demand availability of the VR equipment, and (c) novelty of the intervention itself for those who have never used a VR headset or HRV sensor.
Our findings demonstrated that intrasession HRV progress (i.e., % change in HRV throughout a session) was larger in the VR group compared with the mobile group (2.8% vs. −0.24%, p < .001). This suggests that overall, VR users were more successful at improving their HRV score during a guided-meditation session compared with mobile version users. VR as an MBI modality may thus be more effective at inducing a state of relaxation than a standalone meditation app on a smartphone. Second, this MBI showed that the ordinal session number is positively correlated with intrasession HRV progress for both VR and mobile groups. However, only the VR group showed statistical significance (0.180, p < .0001). This finding suggests that the more guided meditations a participant completes, the better they become at inducing a relaxed state of mind with every guided-meditation session, particularly if using a VR platform. In terms of subjective measures, overall self-reported ratings of perceived anxiety improved equally for both VR and mobile users.
One probable explanation to the disparities in HRV is the immersive 360-degree experience that may be enhancing the therapeutic effect of the guided meditation by ensuring VR users focus during the session. In contrast, because mobile users are not fully immersed in the experience, they are more likely to be subjected to additional visual stimuli in the ED on-call room, which could be distracting during a guided-meditation session.
Interestingly, when looking at all 213 VR and mobile sessions, our findings revealed that ordinal session number was negatively correlated with length of session (−0.187, p < .001). This could be due to improved familiarity with the equipment and application interface or increased rate of perceived relaxation, as more sessions are completed over the course of the study.
Data analysis by gender revealed that sessions completed by males showed higher intrasession HRV progress compared with females (2.34% vs. 0.80%, p = .036). When looking solely at VR sessions (n = 117), male-only sessions on average showed higher mean intrasession HRV progress compared with female-only sessions (4.43% vs. 1.18%, p = .006). Moreover, VR sessions completed by females showed strong negative association between ordinal session number and length of session (−0.31, p < .001). These findings suggest that not only did VR male users objectively display a more relaxed state of mind after their sessions compared with their female counterparts, but they were also more likely to use the VR equipment for a longer duration over the course of the study. The disparity between sessions completed by males versus females in terms of HRV progress and session duration in the VR group may be due to the increased susceptibility of females to motion sickness induced by VR, a condition referred to as “cybersickness” (Stanney et al., 2020).
There are only a few MBI studies that have used VR-based guided meditations to promote well-being in the healthcare workplace—even fewer are studies that incorporate biomarkers such as HRV to measure physiologic effects on well-being that are not self-reported. In a 2021 prospective randomized crossover trial, Weitzman et al. demonstrated a significant decrease in “emotional exhaustion” among male Otolaryngology residents compared with their female counterparts, after weekly use of VR-guided meditations over a 2-month period (Weitzman et al., 2021). While their study used the same CoresightsTM VR meditation platform as in our study, they did not incorporate HRV analysis, as a measurement of relaxation. In a preliminary study by Liu et al., VR-based guided meditations improved subjective (i.e., pain scales) and objective measures (i.e., BP and HR) of stress and chronic pain (Liu et al., 2021). However, the intervention was aimed at veterans and not medical trainees. We did find a recent MBI study using VR as a stress management tool for medical students, physicians, and allied health professionals (Soh et al., 2021). However, this study was conducted in Singapore and only collected self-reported data on perceived well-being via questionnaires, not biomarkers of stress or relaxation. Moreover, it was not clear whether the VR intervention was in the form of a guided meditation. Thus, to our knowledge, our study is the first to use VR-guided based meditations as an MBI and HRV as a biomarker of stress on medical trainees and health professionals in the United States.
This study has several strengths. First, we incorporated a control group (i.e., mobile version) to better assess the impact of VR as an MBI modality. Second, our study successfully retained at least 70% of our participants to complete at least 3 guided-meditation sessions over the course of 4 weeks at a highly dynamic and fast-paced hospital setting such as the ED. Third, we opted to use “intrasession HRV progress” instead of “mean session HRV” as a primary objective metric for relaxation. The former takes into account the relative change in HRV after being fully immersed in the guided-meditation session. Using the latter may mask the “progress” in HRV that the user would presumably have demonstrated throughout the session. Finally, in addition to the brief nature of the guided meditations (3–5 minutes), we were also able to provide a private and accessible location for our participants in the ED on-call room, where they could use our equipment whenever their schedules allowed. Moving forward, future directions can include increasing sample size, using other biomarkers for measurement of stress (e.g., skin conductance, EEG, blood pressure, etc.), facilitation of open-ended user experience interviews, and post-intervention follow-up of participants.
In summary, this brief MBI showed that VR-based guided meditations improved subjective as well as objective measures of well-being among medical trainees and healthcare professionals. VR may be a more effective meditation platform compared with standalone mobile apps, especially when used on a routine basis. More research is needed to explore potential gender bias associated with VR use.
Applications to Professional Practice
Burnout in the medical community has traditionally been addressed with time-consuming, poorly accessible, and unsustainable interventions. Our study demonstrated a brief mindfulness-based intervention (MBI) that is novel, engaging, and impactful both on subjective and objective measures of stress. Our findings revealed that virtual reality (VR)-based guided meditations show great promise as an accessible and therapeutic MBI for healthcare workers, even in fast-paced, highly dynamic occupational settings. When introducing mindfulness meditations into the workplace, virtual reality may be a more effective meditation platform compared with standalone mobile meditation apps, especially when used on a routine basis.
Supplemental Material
sj-pdf-1-whs-10.1177_21650799221123258 – Supplemental material for Should Mindfulness for Health Care Workers Go Virtual? A Mindfulness-Based Intervention Using Virtual Reality and Heart Rate Variability in the Emergency Department
Supplemental material, sj-pdf-1-whs-10.1177_21650799221123258 for Should Mindfulness for Health Care Workers Go Virtual? A Mindfulness-Based Intervention Using Virtual Reality and Heart Rate Variability in the Emergency Department by King Pascual, Amiad Fredman, Athanasios Naum, Chaitrali Patil and Neal Sikka in Workplace Health & Safety
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol was approved by the Institutional Review Board (#061728, “Effect of Paced Breathing/Virtual Reality Training on Medical Provider Stress and Wellness”).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.