
Abstract
Background:
Violence on the job has been shown to harm both physical and psychosocial health, but the results presented in existing studies might be biased because they have not considered prior indicators of such health.
Methods:
Physical violence and threats were pooled into a measure of workplace violence for 77,388 randomly sampled respondents from the working population in Denmark in 2012, 2014, and 2016. Longitudinal analyses of these survey data merged with administrative records on sick leave (exceeding 30 days, implying that the consequences of the violence were more serious) were performed. Separate analyses were conducted by sector, gender, and by gender within sectors.
Findings:
Experiencing violence increased sick leave +36% from before to after the violence relative to the general trend among other respondents that did not experience a violent event.
Conclusions/Application to Practice:
Work-related violence is a serious health issue, especially in health care, even when we meticulously took prior use of sick leave into account to obtain less biased results.
Keywords
Background
People who deliver services are at risk of experiencing aggressive behavior and/or violence while performing their job, a risk that is especially high in health care, including inpatient and outpatient health care (Pompeii et al., 2015, 2020). This could be true also in Denmark although this context has comparatively low rates of violent crimes (33 serious assaults per 100,000 citizens in Denmark; 250 per 100,000 citizens in the United States, UNODC, 2019) and work environments in Denmark are highly regulated by law including guidelines for reducing the risk of violence (all historical versions available in Retsinformation, n.d.a, n.d.b). Workplace violence is associated with a range of negative consequences such as post-traumatic stress disorder (PTSD) symptoms, higher rates of sick leave, and poorer wellbeing more broadly defined (see Lanctôt & Guay, 2014; Phillips, 2016 for reviews). For sick leave—the focus of our study—the association could also exist in Denmark although Danish sick leave policies arguably make it harder to detect such an association. This is because eligibility for sick leave benefits occurs only after 30 days of health-related absence from work, implying that only serious health-related consequences of violence on the job will manifest in the use of sick leave benefits. Friis et al. (2018) also focused on Denmark and found increased health-related absence from work in both short and long follow-up among survey respondents who experienced violence on the job in 2005/2006. We interpreted their results to imply that it was beneficial to focus on sick leave even in the highly regulated context that workplaces in Denmark are.
The existing research potentially suffers from data limitations that impair the precision of estimated consequences. Most data only allow researchers to focus on indicators of health and wellbeing after violence took place. 1 Therefore, one core source of unobserved heterogeneity—preexisting indicators of health and wellbeing, such as receiving sick leave benefits prior to the violence—is typically not controlled for. This makes workplace violent victimization a still understudied public health issue (Estrada et al., 2010).
In this study, we merged several datasets to provide knowledge on the consequences of workplace violent victimization for the use of sick leave benefits, with emphasis on work sector and gender. We used data from three waves of national surveys of working environments in Denmark, which included questions related to experiencing physical violence and violent threats while working.
Methods
In this longitudinal study, we merged survey data and Danish administrative data. The survey data came from three rounds (2012, 2014, and 2016) of “The Work Environment and Health” survey (Danish National Research Center for the Working Environment, n.d.a), which Statistics Denmark performed for The Danish National Research Center for the Working Environment. The survey questionnaire was sent to a random sample of 167,422 Danish wage earners in the age range 18 to 64 years. The response rate was 53.9%. Statistical weights were provided to ensure representativeness in terms of gender, age, and type of job. 2 As study entities, we used persons who answered the survey questions that we rely on for defining our dependent variable (see below). We focused only on people aged 18 to 62 years to avoid our follow-up period being conflated with retirement. All data were processed in line with the 2018 Danish Data Protection Act and the 2016 General Data Protection Regulation of the European Union.
As independent variable, we defined “victims of work-related violence” as people who answered in affirmative (1 = yes, 0 = no) to either or both of the following two survey questions: “Have you within the past 12 months been the victim of physical violence in your workplace?” and “Have you within the past 12 months been the victim of threats of physical violence in your workplace?.” The wording of the survey questions (in Danish) aims directly at the respondent experiencing violence him- or herself, not simply seeing it or knowing it occurred at the workplace.
As outcome variable, we measured the reception of sick leave benefits, which was recorded in a specific category in the Den Registerbaserede Evaluering Af Marginaliseringsomfanget (DREAM; the register-based evaluation of the extent of marginalization) register (Danish Agency for Labour Market and Recruitment, 2021). This register was based on information from the Danish Ministry of Employment, the Danish Ministry of Education, and the Danish Customs and Tax Administration, and documented, for each week of the year, the main type of social benefits (if any) each of the citizens of Denmark received. Eligibility for sick leave benefit is achieved following a medical report from a general practitioner and absence from work for at least 30 days, and one sick leave period cannot exceed 22 consecutive weeks (Danish Ministry of Employment, 2019). This eligibility criterion implied that we could only observe more serious health complications (periods of absence exceeding 30 days) and hence that we likely observed only the health response to more serious cases of work-related violence. With the data, we could measure each respondent’s dependence on sick leave benefits both before and after the survey was carried out, allowing us to analyze average trajectories of sick leave benefits and how these were associated with victimization. We did not have information on the exact date when each respondent completed the survey. We, therefore, defined an “interview period” as a six quarter window to cover the period of interviews and the 12-month reporting period before the interview. We excluded these interview periods from our statistical model to ensure temporal ordering. Doing so meant we had to drop some data but secured that we could distinguish between absence from work before and after the violent event.
Work sector was defined from the International Standard Classification of Occupations (International Labour Organization, 2007). We aggregated occupations into “health care workers” (doctors, nurses, and care providers), “front workers” (police, prison staff, security personnel, and teachers and pedagogues), and a residual “others” category (all other occupations, such as accountants and construction workers, in which people have a low degree of critical communication with citizens or clients). As possible confounders we included age (on January 1 of the interview year), interview year, ethnic minority background, 3 parenthood (an indicator of whether the respondents had any children), and marital status (whether respondents were married, cohabiting, or single). We obtained these variables from the linked administrative data. Because few physical assaults at the job were recorded in official police reports we could not include prior assaults and could not control for multiple victimizations.
Informed consent was obtained from all survey respondents. Statistics Denmark anonymized and de-identified the data. The use of the data for research purposes was allowed under Danish law for individuals affiliated with Danish research institutions without the need for ethical approval of individual studies (Statistics Denmark, n.d.). The present study received approval from Statistics Denmark under the auspices of data project number 703566.
Data Analysis
We describe our sample by relating it to the population of employed people in Denmark aged 18 to 62 years, and by comparing respondents who reported work-related violent victimization in the surveys and respondents who did not. Chi square tests were used to test whether respondents differed on variables by victimization status. The prevalence of work-related violent victimization—overall and by gender and sector—was estimated from the self-reports in the Work Environment and Health survey. We pooled the data from all 3 survey years. To analyze the bivariate association between victimization and sick leave, we aggregated our measure of sick leave to indicate whether (1 = yes, 0 = no) each respondent had received any sick leave benefits during each calendar quarter from eight quarters before to eight quarters after the interview period.
In multivariate analyses, to measure the strength of the association between victimization and sick leave, taking possible confounders and, importantly, prior sick leave into account, we used the weekly sick leave information to calculate the proportion of the full 2 years prior to and following the interview period that respondents received sick leave benefits. We then estimated whether the change (in percentage points) in sick leave from before to after the interview period was greater for respondents who reported violent victimization than for others. Formally, we used a difference-in-differences model, which we estimated using Ordinary Least Squares. The model belongs to the class of quasi-experimental research designs that aim to study causal relationships in settings where randomized controlled trials would be unethical or hard to implement, as in our setting (Wing et al., 2018). One major strength of this model was that it allowed us to compare the situation after the interview to before for everyone in the database, and thus took prior differences in sick leave as well as unobserved individual characteristics that were stable across time into account. The fundamental assumption of the model is that the average change in sick leave from before to after the interview period for respondents who did not report victimization mirrored what the average change would have been for respondents who reported victimization—if they had not experienced violence (the parallel trends assumption). The model could not, however, take unobserved individual traits into account if these varied over time, just as the model is fundamentally associational because we did not have experimental variation in workplace violence (Wing et al., 2018). To account for differences across gender and work sector, we also applied the model by gender and sector. All analyses were conducted in STATA 15 with a significance level of 95%.
Results
Item non-response to the survey questions that we use to measure the violence variable reduced the sample by 8,187 respondents (approximately 9.1%). The final sample included 77,388 respondents. Table 1 shows summary statistics of this final sample and compares to the population. Although survey respondents on average were older than the population (42.5 years in survey, 41.5 years in population) and a lower percentage had ethnic minority backgrounds (4.3% in survey, 5.9% in population), they resembled the population well on other key covariates (e.g., 48.7% and 49.2% women in survey and population, respectively; 10.5% worked in health care sector in both survey and population; and 14.5% and 14.4% were front workers in survey and population, respectively).
Overall Population Characteristics and Characteristics of Danish Workers in “The Work Environment and Health” Surveys Stratified by Experiencing Workplace Violence (N = 2,259,570 in Population and N = 25,796 in Surveys)
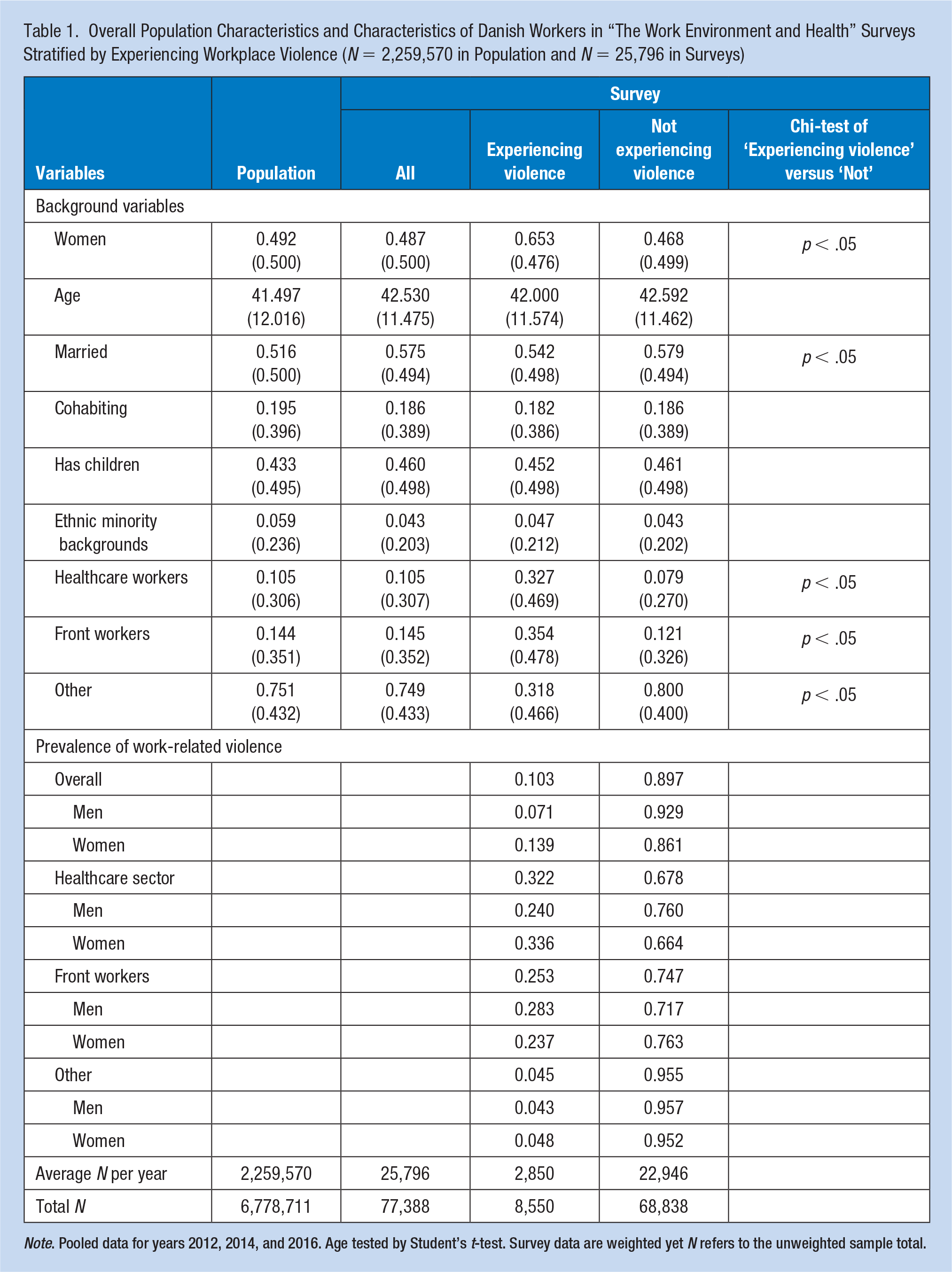
Note. Pooled data for years 2012, 2014, and 2016. Age tested by Student’s t-test. Survey data are weighted yet N refers to the unweighted sample total.
The results from additional analyses showed that among the perpetrators of the violence in our data, 93% were customers, clients, patients, or students, and the rest were predominantly colleagues. For women victims, virtually all (>97%) perpetrators were clients (for women in health care the number was as high as 99%).
Prevalence Estimates
Overall, 10.3% experienced violence on the job (5.8% physical violence, 8.7% threats, 4.0% both physical violence and threats). Results varied across sectors, with <5% in the residual “other” category experienced workplace violence; almost one in three in the health care sector (32.3%) and one in four in front work sectors (25.3%).
The prevalence was almost twice as high for women as for men (13.9% of women and 7.1% of men, p < .001). Looking at sector differences, the prevalence of violence was high for both men and women in health care and in front worker sectors, and likewise low for both men and women in the residual “other” category. For example, the estimated prevalence among women working in health care indicated that around one in three reported victimization within the preceding year; the corresponding number for men in health care was one in four. Additional analyses showed that this difference was not driven by a difference in the ratio of threats-to-physical violence, women in health care just experienced violence at a higher rate. The gender difference within front work sectors was driven by men experiencing threats more often (24.4% males, 18.2% females, p < .001); it was not driven by a difference in physical violence (18.5% males, 17.4% females, p = .145).
The results from additional analyses also showed heterogeneity across job types within the health care sector (Supplementary Table 1). Nurses and health care assistants had the highest prevalence of victimization: 28.1% for nurses and 41.5% for health care assistants. Doctors and the residual “other” categories within health care had lower prevalence, 21.4% and 10.8%, respectively. Within the health care sector, differences in which job types women and men employed did not explain the full difference in exposure: among doctors (women 26.3%, men 16.1%, p < .01), health care assistants (women 42.1%, men 36.2%, p < .05), and the residual “other” category (women 12.0%, men 6.7%, p < .01), the prevalence was higher for women. For nurses, however, the gender differential was reversed, and 36.0% of male nurses experienced violence versus 27.7% for female nurses (p < .05).
Association Between Victimization and Sick Leave
Figure 1 shows average trajectories of sick leave by quarter before and after the interview period and by work-related violent victimization. After the interview period, a substantial difference arose between those who reported victimization (around 3.7%) and those who reported no victimization (around 2.3%). Victims thus had around 1.4 percentage points higher average sick leave (p < .001), which in relative terms corresponded to 65% higher rate of sick leave.
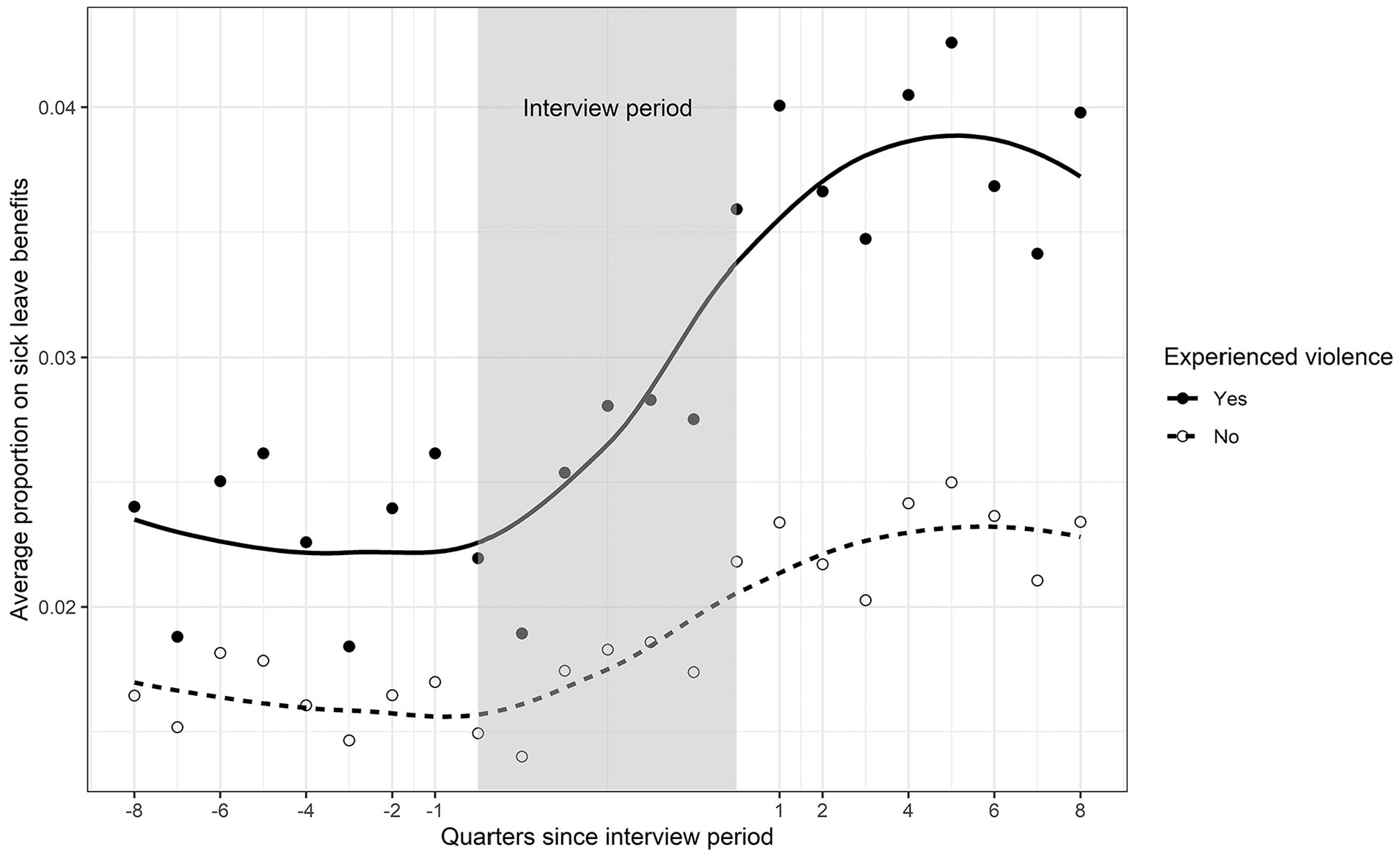
Proportion on sick leave benefits by quarter and by experiencing violence.
Prior to victimization, we also observed a difference in sick leave (Figure 1). Here, sick leave was higher among respondents who would at a later point become victimized (around 2.3% for victims, around 1.7% for controls; which in relative terms corresponded to 35% higher rate of sick leave even prior to the violence). 4 Supplementary Figure 2, which shows comparable results by gender and sector, documents differences in the average trajectories of sick leave across these characteristics. Across the sectors, women generally had higher levels of sick leave than men (e.g., >2.0% and <2.0% for women and men, respectively, in front work) but also seemed to respond more to the violence (postviolence level of sick leave for women in health care was as high as 6% within one quarter whereas the comparable number for men in health care was just above 3%).
Figure 2 shows the estimates of the association between trajectories of sick leave and work-related violent victimization overall as well as by gender and sector. Because the model focused on differences in average individual change between respondents who experienced violence and respondents who did not, estimates reported in Figure 2 considered both pre-existing differences in sick leave, the upward trend in sick leave over the data period (see Note 4), and the impact of confounders (including time-stable individual confounders that were unobserved in the data). Supplementary Table 2 reports parameter estimates.
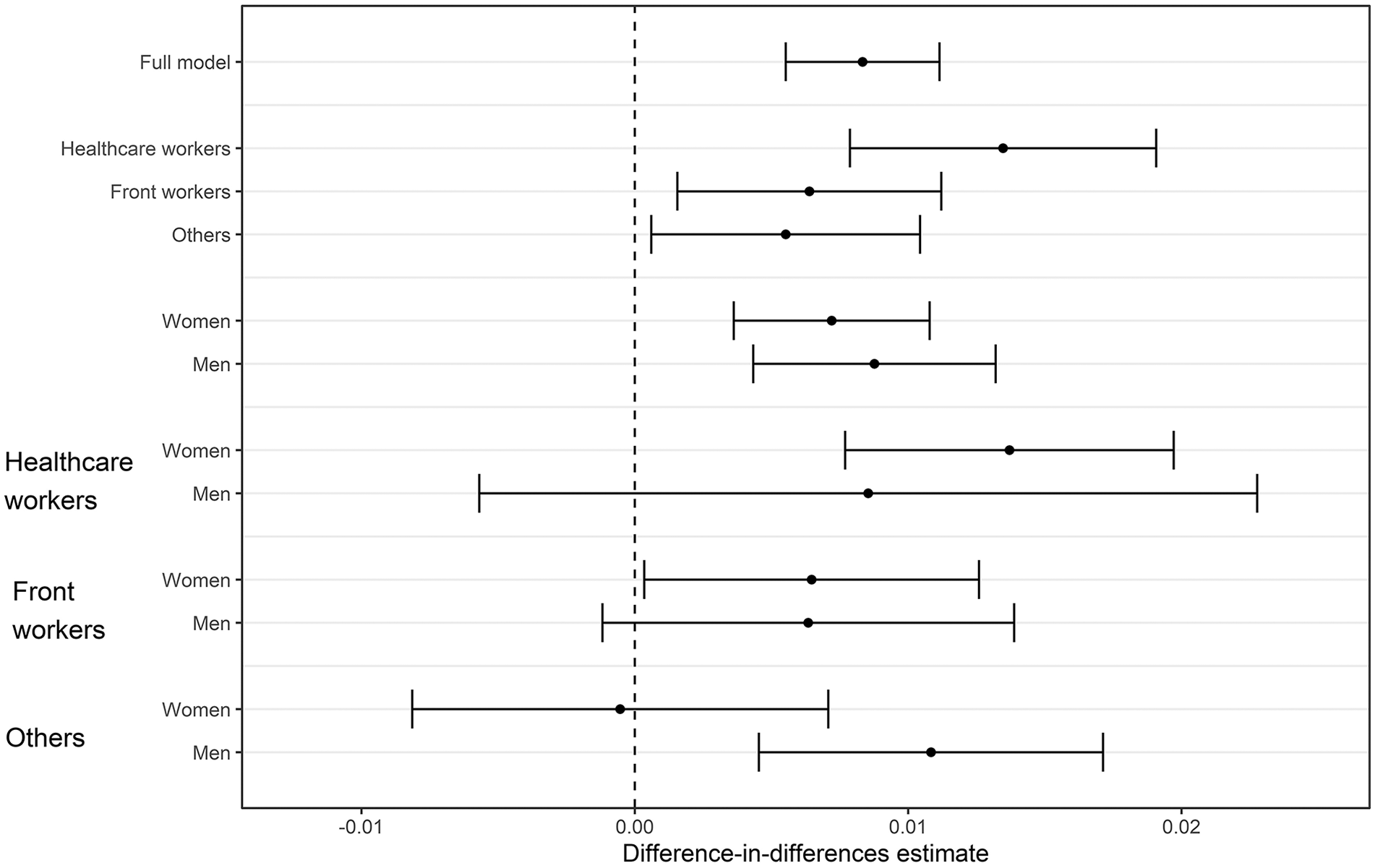
Association (in percentage points) between experiencing violence and proportion of weeks on sick leave benefits. Results from difference-in-differences models.
The association between victimization and sick leave that we estimated using this model was both statistically and substantially important, and from before to after the violence, the point estimates suggested that sick leave increased by 0.8 percentage points (p < .001) more for victims than it did for the control group (control group increased by 0.7 percentage points, p < .001). Taking the difference in sick leave prior to violence into account, this increase corresponded to a relative increase of 36% (which may be compared with 65% in the model that did not take pre-existing differences into account, mentioned above). Taking pre-existing differences into account was thus important.
In health care, the association was stronger than in the other sectors (+1.3 percentage points [p < .001] from pre-exposure baseline of 1.5 % in health care vs. +0.6 percentage points [p < .05], baseline 1.2% among front workers; confidence intervals overlapped, however). The association did not differ across gender (females +0.7 percentage points [p < .001], baseline 2.4% vs. males +0.9 percentage points [p < .001], baseline 1.7%). Yet breaking down results by gender and sector simultaneously documented important differences: For women, almost the full association between sick leave and victimization was driven by respondents in health care (women in general +0.7 percentage points [p < .001], women in health care sector +1.4 percentage points [p < .001], women in front work +0.6 percentage points [p < .05]). For men, we only observed a significant association in the residual “other” sector (+1.1 percentage points [p < .01], baseline 1.7%).
Table 2 provides estimates from our difference-in-differences model by job types within the health care sector. We found substantially sized and statistically significant consequences for nurses (+1.1 percentage points [p < .01] from a pre-exposure baseline of 2.0%) and health care assistants (+1.3 percentage points [p < .01]; baseline 2.0%). Estimates for doctors and the residual “other” category were far from reaching statistical significance. This finding could of course be driven by comparatively low N in these groups (at least for doctors, N = 623), but tiny point estimates (+0.6 and +0.3 percentage points) indicated that even with more data, the impact of victimization would likely be limited.
Changes in Sick Leave Attributable to Violence Among Danish Health care Workers in “The Work Environment and Health” Surveys Stratified by Job Types and Gender (N = 9,634)
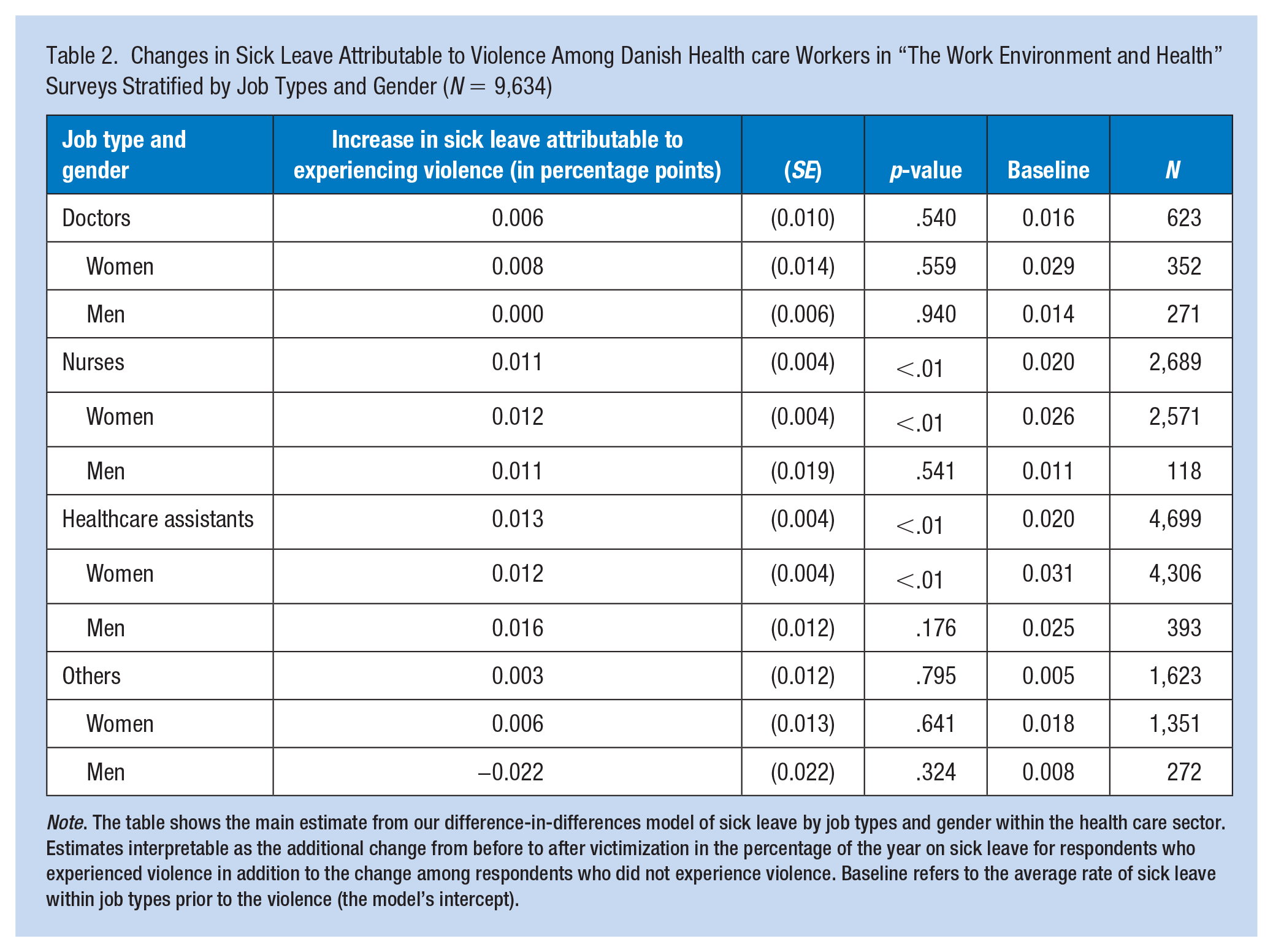
Note. The table shows the main estimate from our difference-in-differences model of sick leave by job types and gender within the health care sector. Estimates interpretable as the additional change from before to after victimization in the percentage of the year on sick leave for respondents who experienced violence in addition to the change among respondents who did not experience violence. Baseline refers to the average rate of sick leave within job types prior to the violence (the model’s intercept).
More than 95% of nurses and more than 90% of health care assistants in our data were women. These gender distributions prohibited us from drawing firm conclusions about the role of gender within these job types, as statistical strength was low for men. Also, differences in baseline dependence on sick leave differed across gender within job types (e.g., 2.6% and 1.1% for female respective male nurses). But the clear similarity in sizes of the point estimates for men and women within job types (e.g., 1.2 and 1.1 percentage points for female respective male nurses) did seem to indicate that the overall gender difference in the consequences of exposure within the health care sector was driven not by gender but by gendered occupational structures.
Discussion
On average, 10.3% of the Danish workforce reported work-related violent victimization (measured jointly through threats of violence and actual physical violence) within a year, and 32.3% in the health care sector. These estimates are alarmingly high, but still dwarf those reported elsewhere, such as 69% reported in Nowrouzi-Kia et al. (2019) for physicians and 39% reported in Pompeii et al. (2015) for hospital nurses and physicians. The reason for this could be a lower prevalence of violence in Denmark, as mentioned. However, the reason could also relate to the relevant regulation in Denmark. Official guidelines (Retsinformation, n.d.b) stipulate how to interpret and implement the features of the law that concern work-related violence, including when and under which circumstances employees are at risk of violence and threats while performing their jobs. This is to raise employers’ awareness of such situations and circumstances. High-risk functions mentioned in the guidelines include the handling of cash or valuable goods, security and control functions, and frontline functions that require contact with clients or citizens (such as health care workers). Reasons for violence often relate to the employee needing to withhold some desired good from a person, but may also reflect the client’s more general frustration, drug or alcohol abuse, or the like (thus correspond to reasons elsewhere, Phillips, 2016).
Contrary to the United States, where health care organizations in only some states have specific violence prevention strategies and the only formal guidelines are voluntary (Phillips, 2016), employers in Denmark are required to monitor the risk and plan work functions to reduce it. All incidents of violence and how they are dealt with must be recorded and documented for future reference, and preventive measures should be evaluated following each incidence. Employers are encouraged to train personnel in how to avoid and handle situations that could escalate. The Danish National Research Center for the Working Environment offers training tools, which are free of charge. For example, the “Integrated Violence Prevention” program (authors’ translation, see The Danish National Research Center for the Working Environment, n.d.b) integrates risk assessment and potential solutions from both employers and employees, thereby ensuring that violence prevention measures are adapted to fit the specific context which the workplace constitutes. The program is structured into four stages, each supported by structured material available from the program webpage. In the first stage, a realistic implementation plan is agreed upon to secure the support of all involved actors. In the second stage, existing violence prevention strategies and efforts (including their strengths and weaknesses) are mapped to ensure that future measures build on existing resources. The third stage, named the process of problem-solving, consists of two parts. A structured seminar for everyone at the workplace aims to propose solutions to what was learnt in the first two stages. Then, a working group synthesizes the suggestions and implements tools based hereon. In the last stage of the program, tools from the process of problem-solving are evaluated and adapted to the working environment. The Integrated Violence Prevention program has been evaluated using a cluster-randomized controlled trial, which showed positive effects on violence prevention strategies and awareness on the treated workplaces (Andersen et al., 2021).
The guidelines encourage employers to take even minor violent incidents seriously, just as the guidelines require employers to seek emergency care if potentially needed. When an incidence occurs, the employer is required to offer physical as well as psychological emergency care. Immediately following an incidence, the employer is encouraged to ensure that the victim is not left alone during the first 24 hours and to arrange transportation to the victim’s home. The employer (or a trained employee) should have a meeting with the victim 1 to 3 days after the incidence to evaluate the immediate impact and potential preventive lessons to be drawn, to reduce future risks. Employers are encouraged to take the employee’s mental well-being into account when planning work functions. If the incidence leads to sick leave, the employer is encouraged to schedule meetings with the victim to facilitate return to work; one meeting after 4 weeks of absence is mandatory.
The eligibility criterion for receiving sick leave benefits in Denmark implies that we only observed more serious health complications (periods of absence exceeding 30 days) in our data and hence that we likely observed only the health response to more serious cases of violence. This was an important limitation of our study as the literature review in Lanctôt and Guay (2014) showed that most sick leave spells following violence lasted between 1 and 7 days. Relatedly, our dependent variable included sick leave for any reason, including reasons not directly linked to experiencing violence (e.g., somatic illness). But this is where our research design that took pre-to-post violence trajectories into account showed its strength: To undermine our results, other reasons for receiving sick leave benefits would have had to be strongly correlated with experiencing violence and with the timing of it, which seems unrealistic. We acknowledge that these are limitations to our study, but with this measure of sick leave, we still found substantial sick leave consequences of experiencing violence at work.
The prevalence of violence varied across gender and sectors. Prevalence was almost twice as high for women as for men which mostly (but not in full) was caused by more women working in high-risk sectors such as health care. Female health care assistants had the highest prevalence (>40%). Police, security personnel, etc. had the second-highest victimization rate, whereas employees in other and more low-risk sectors (which are the sectors with by far most employees) had comparatively low exposure (results not shown but available on request from the corresponding author). The overall association between victimization and sick leave was driven by a strong association for women in health care. For men, we also detected a substantial association between experiencing violence and sick leave in the residual “other” sectors, yet this was from a very low rate of both sick leave and violence.
Implications for Occupational Health Practice
Although results from our study suggested a smaller magnitude of the association between victimization and one indicator of adverse health outcomes, our uniquely suited data and analytical setup (which controlled extensively for pre-existing health using longitudinal data) ameliorated important limitations of existing research. Still documenting a substantial association between experiencing violence on the job and sick leave bolsters the claim that workplace violence is consequential for health.
Our results direct attention to the health consequences of work-related violent victimization for women working in health care, especially nurses and health care assistants. Although men and women working in these job types suffer similar consequences of work-related violent victimization for sick leave, gendered employment patterns mean that disproportionately many women are exposed to these consequences (>90% working in these job types are women). It is important to note that even for these women in health care, the rate of sick leave in our data was not exorbitantly high. This group on average received sick leave benefits for 4.4% of the weeks during the 2-year follow-up period, which corresponds to about 4.5 out of 104 weeks or 30 out of 2 × 365 days. This number was much higher than among the controls, yet it still shows that most people who experience violence on the job manage to cope with it without long periods of absence from work—or that our dependent variable only captured the most serious cases of violence and a shorter-term response for less serious cases was not picked up by our measure. Either way, despite the low rate of sick leave, the consequences of violence still accumulate into substantial costs at the societal level: There are, after all, around 200,000 women working in health care in Denmark and one in three experience violence on the job, as our study has shown. In 2018, the Danish state paid out DKK 4,300 (~EUR 575) per week of sick leave. The sick leave-related consequences of workplace violence among women in health care therefore amount at least to DKK 417 million (~EUR 55 million) over 2 years. 5 Foregone income, productivity loss, treatment costs, and possible dynamic effects of victimization—such as long-term issues related to PTSD symptoms—should be added to this amount, implying that the total costs of violence on the job are likely immense and something that should receive far more attention not just from employers who will have to make ends meet while employees are on sick leave but also from society at large. Importantly and as was already discussed, these conclusions are based on data from Denmark, a context with a high degree of relevant regulation and the explicit training of personnel to avoid or handle situations that could escalate into threats and/or violence. The consequences of work-related violent victimization that we documented in this article could thus reasonably be lower bound estimates of what the consequences might look like in other and less regulated contexts.
Applying Research to Occupational Health Practice
The prevalence of violence while working is lower in Denmark than in other contexts but violence on the job still leads to a substantial increase in absence from work in Denmark, which is costly to society. The problem is especially pertinent in healthcare and especially for women working in healthcare. The lower prevalence of workplace violence may be caused by Denmark’s strong focus on working environments (which are regulated by law) and official guidelines for how to avoid, tackle, and follow-up on workplace violence. Guidelines come with training programs that are freely available to employers, which is likely a fruitful way to engage with employers and lower the costs associated with providing such training to employees.
Supplemental Material
sj-docx-1-whs-10.1177_21650799221096994 – Supplemental material for Taking Prior Sick Leave Patterns Into Account When Estimating Health Consequences of Violence on the Job
Supplemental material, sj-docx-1-whs-10.1177_21650799221096994 for Taking Prior Sick Leave Patterns Into Account When Estimating Health Consequences of Violence on the Job by Lars H. Andersen and Therese B. Christensen in Workplace Health & Safety
Footnotes
Conflict of Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The ROCKWOOL Foundation funded this research (grant no. 1195).
Ethical Approval
Informed consent was obtained from all respondents to the surveys. Statistics Denmark anonymizes and de-identifies the data before making it available to researchers. The use of the data for research purposes is allowed under Danish law for individuals affiliated with Danish research institutions without the need for ethical approval of individual studies (see ![]() for English versions of the relevant laws). The present study received approval from Statistics Denmark under the auspices of data project number 703566. No additional administrative permissions were required to access and use medical records or other material used in the study. All methods were carried out in accordance with relevant guidelines and regulations.
for English versions of the relevant laws). The present study received approval from Statistics Denmark under the auspices of data project number 703566. No additional administrative permissions were required to access and use medical records or other material used in the study. All methods were carried out in accordance with relevant guidelines and regulations.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.