
Abstract
Background:
The relationship between workplace incivility and psychological distress among nurses has been well-documented in the nursing literature. Management practices to reduce the negative impact are less clear. This study aimed to examine perceived servant leadership as a moderator between workplace incivility and psychological distress among nurses in Chinese hospitals.
Methods:
This study used a cross-sectional design and was conducted between September and October 2020. We recruited 1,604 nurses from 13 Chinese hospitals across different regions in China ranging from 18 to 55 years in age (M = 28.48 years, SD = 6.53 years). Multiple linear regression was used to analyze the data.
Findings:
The results showed that workplace incivility (β = 0.40, p < .001) and perceived servant leadership (β = −0.13, p < .001), as well as their interaction (β = −0.11, p = .002), predicted nurses’ psychological distress. Perceived servant leadership moderates the relationship between workplace incivility and psychological distress.
Conclusions/Application to Practice:
Servant leaders can create an ethical work climate, display empathy and compassion, and facilitate resilience. Our findings can assist hospital management with support from occupational health providers to recruit, train, and assess nursing supervisors. Also, occupational health providers in collaboration with nursing administration can monitor incivility, psychological distress, servant leadership levels, and impact.
Background
Workplace incivility is a low-intensity deviant behavior with ambiguous intent to harm other members of the organization (Demsky et al., 2019). Such deviant behaviors nonetheless are rude and disruptive and potentially result in psychological or physical distress for victims (Geldart et al., 2018; Huang et al., 2020). If left unaddressed, this disruptive behavior may progress into a threatening situation (Collins & Rogers, 2017). Grant (2019) argued that workplace incivility is an occupational hazard that should be recognized and controlled in health care. Unfortunately, workplace incivility is a common occurrence among nurses across the world in the health care setting (Mikaelian & Stanley, 2016). For example, in a study conducted in South Korea, 91.46% of participating nurses reported to have experienced incivility during their clinical learning experiences (Kim et al., 2020). A study in China also indicated that 56.7% of nursing students experienced various degrees of uncivilized behavior (Shen et al., 2020). High prevalence of workplace incivility and even violence is also reported among nurses in other countries such as the United States (Lewis-Pierre et al., 2019), Iran (Abdollahzadeh et al., 2017; Fallahi-Khoshknab et al., 2016), Australia (Budden et al., 2017), and the United Kingdom (Birks et al., 2017). Numerous studies have shown that incivility in the health care setting not only has a destructive effect on emotional and physical health in victims but it also results in time lost from work, financial waste, and the inhibition of the educational process (Armstrong, 2018; Budden et al., 2017; Sherrod & Lewallen, 2021). Incivility can even cascade to affect patient care and financial outcomes (Eka & Chambers, 2019). Psychological distress forms a major occupational health issue in workplaces across the globe (Huang et al., 2021; Simo et al., 2018). Psychological distress refers to a state of emotional suffering typically characterized by mental symptoms such as depression and anxiety (Arvidsdotter et al., 2016). A meta-analysis of 174 studies across 63 countries revealed that the pooled prevalence of psychological distress is as high as 17.6% (Steel et al., 2014). Longitudinal data (2007–2017) from the Household, Income, and Labor Dynamics in Australia (HILDA) Survey demonstrated an increasing trend over time in the prevalence of very high psychological distress, with the prevalence of very high distress rising from 4.8% in 2007 to 7.4% in 2017 among nurses (Butterworth et al., 2020). Psychosocial workplace factors such as high job demand, low social support, shift work, job control, and job dissatisfaction have been found to lead to psychological distress (Birhanu et al., 2018; Kabito & Mekonnen, 2020). In addition, sociodemographic components such as gender, age, education level, marital status, and experience have also been found to be related to workplace psychological distress (Bariola et al., 2015; Kabito & Mekonnen, 2020). In health care organizations, other important causes that result in psychological distress include unreasonable expectations among administrators and patients, and unsafe working conditions or practice environments, changing employment relations, deficiency in technical knowledge, and so on (Liu, Yang & Zou, 2021). Despite variation in its intensity and severity, higher psychological distress increases the risk of health outcomes including mortality, the development of asthma in adulthood, and worse physical function among adults with cancer (Barry et al., 2020). In addition to health consequences, psychological distress contributes to reduced quality of health care service, resulting in low patient satisfaction and higher medical costs (Kabito & Mekonnen, 2020). Given its adverse impact on both nurses’ health and health care organizations, protective measures must be implemented to reduce or prevent psychological distress among nurses working in hospitals.
Although efforts have been made to examine the relationship between workplace incivility and employees’ psychological distress (Geldart et al., 2018; Huang et al., 2020), far less attention has been given to the mechanism under which how this association might occur. It has been shown that social ties and relationships with others are vital protective resources that can decrease or mute the effects of stress (Taylor, 2015). Social support and organizational justice have been found to buffer the effect of workplace incivility on employees’ psychological distress (Geldart et al., 2018). Support from organizations can protect health care workers from workplace violence (Zhao et al., 2015). Employees who experience higher levels of incivility reported fewer psychological health issues when they feel organizationally and emotionally supported (Miner et al., 2012). Social support can take several forms: emotional support, instrumental support, informational support, and companionship support. According to social support theory, social support can buffer individuals from the damaging effects of stress. Servant leaders can provide empathy, give employees a sense of social belonging, and encourage employees to build their confidence to handle stressful events (Greenleaf, 1970; H. Wu et al., 2020).
According to Eva et al. (2019), servant leadership is another-oriented approach to leadership manifested through one-on-one prioritizing of followers’ individual needs and interests. This leadership approach requires leaders to express overarching concern toward the well-being of followers and other larger communities. Servant leadership has six dimensions: integrity, self-sacrifice, building community, empowering people, emotional healing, and visioning (Qiu & Dooley, 2019). Servant leaders can provide emotional healing and help make employees whole, who suffer personal and professional setbacks (Spears, 1995). Furthermore, they are honest and fair, provide true information to employees, and build a just work climate in the organization (Coetzer et al., 2017). Thus, servant leadership is perceived as a form of social support from their supervisors or other leaders. In the literature, servant leadership has been demonstrated to positively impact health care workers and organizations. For example, servant leadership can contribute positively to health care workers’ job satisfaction (Jing, 2019).
While servant leadership is perceived to benefit employees and organizations, workplace incivility has been conceptualized as a chronic and low-intensity stressor that affects employees’ psychological health (Cortina, 2008). From the perspective of stress and coping theory (Lazarus & Folkman, 1984), when stressful circumstances occur, people will usually engage in the assessment of their coping abilities and resources. If they feel their resources are sufficient to cope with the stressors, the psychological consequences would be less. Servant leadership perceived by employees can serve as helping resources to lessen the effect of uncivil workplace behaviors. Based on the above theoretical reasoning and empirical investigations, we, therefore, proposed that supervisors’ servant leadership perceived by employees acts as a moderator between workplace incivility and psychological distress.
In the literature, little research has investigated the moderating role of servant leadership in the relationship between these two variables. To the best of our knowledge, no studies have examined such a moderating effect among nurses in the context of Chinese hospitals. As aforementioned, the work of a nurse has been traditionally characterized by high work demands and role ambiguity, resulting in high job stress (Cho & Steege, 2021; Falguera et al., 2021). Nurses have to deal with relentless and unprecedented demands from the patients, contributing to physical exhaustion (Braithwaite et al., 2020). This was especially true among nurses in the Chinese hospitals during the COVID-19 pandemic in which they faced tremendous mental health pressures, leading to serious psychological distress (Wu et al., 2021; Xia et al., 2021). Therefore, further investigation of such an association among nurses in Chinese hospitals was warranted. In examining the moderation effect, we expected that when nurses perceived a higher level of servant leadership displayed from their supervisors, the association between incivility from co-workers and their psychological distress would be weaker. It was also anticipated that when nurses perceived a lower level of servant leadership displayed from their supervisors, this relationship would be stronger. In another word, perceived servant leadership buffers the effect of incivility on nurses’ psychological well-being. The purpose of this study is to examine whether servant leadership moderates the impact of workplace incivility on psychological distress among Chinese nurses.
Methods
This study used a cross-sectional design and was conducted between September and October 2020. The sampling frame included 4,946 nurses who work in 13 Chinese hospitals across different areas of China. We asked the human resource managers of each hospital to distribute the online survey to their nurses through a popular Chinese social media, WeChat. Nurses working in all departments were eligible to participate by completing the online survey. Between September 27 and September 30, 2020, human resources managers sent reminder messages to nurses asking them to complete the survey. No incentives were provided to nurses to complete this survey. This study was approved by the Ethics Committee of China Women’s University. Participation was voluntary and nurses were assured of confidentiality.
Demographic information included nurses’ age (<20 years, 20–44 years, 45–30 years, 30–40 years, 40–50 years, >50 years), gender (male or female), monthly income (Chinese Yuan: <2,000, 2,000–4,000, 4,000–6,000, 6,000–8,000, 8,000–10,000, >10,000), education level (high/vocational school diploma, associate degree, bachelor’s degree, master’s or above), years at current job (less than 6 months, 6 months–2 years, 2–4 years, 4–6 years, more than 6 years), marital status (not married, married, or unidentified), and level of hospital (tertiary, secondary, and primary hospitals). Demographic variables such as age (in years), gender (male/female), and monthly income (Chinese Yuan) were used as control variables in this study. These variables were found to predict psychological distress in previous research sampling Chinese participants (Wang et al., 2010).
Workplace incivility was measured using back-translated version of the Workplace Incivility Scale (WIS; Cortina et al., 2001). WIS is a seven-item self-report instrument. Nurses were asked to indicate the frequency their supervisors or co-workers in their current job displayed uncivil behavior to them. Items were presented on a 5-point Likert-type scale ranging from 1 (never) to 5 (very frequent). An example item was as follows: “In the last year, how often did my supervisor or co-workers put you down or was condescending to you?” The internal consistency was good with Cronbach’s alpha of .91 in the current study.
Perceived servant leadership was evaluated with Qiu and Dooley’s (2019) 24-item servant leadership scale. We used this scale because it was developed in China and validated as a psychometrically sound and valid instrument to measure servant leadership in the context of the Chinese culture. Participants were asked to rate their immediate supervisors’ leadership behavior on a 5-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). Two sample items included “My immediate supervisor cares about my personal well-being” and “My immediate supervisor does everything he or she can to serve us.” Cronbach’s alpha of this scale was .86 in the current study.
Psychological distress was assessed with a self-reported K6 screening scale developed by Kessler et al. (2010). Participating nurses responded to the six statements such as “how often do you feel restless or fidgety” by rating on a scale of 1 (never) to 5 (very often). The reliability was .90 in this study.
SPSS Version 21 was used to conduct descriptive statistics (M and SD), Cronbach’s alpha, and Pearson’s zero-order correlation. Multiple linear regression was used to analyze the data. We utilized Hayes’ macro-PROCESS Version 3.5 to examine the moderating effect of perceived servant leadership between workplace incivility and psychological distress. Model 1 of the macro-PROCESS was adopted (Hayes, 2017). The predictor variable was workplace incivility, and psychological distress was the outcome variable, whereas perceived servant leadership was the moderator.
Results
A total of 1,604 participants provided valid data, yielding a response rate of 32.4%. The sample characteristics are presented in Table 1. The participant’s ages ranged from 18 to 55 years (M = 28.48 years, SD = 6.53 years). Most of the nurses were between 20 and 30 years of age (725, 45.2%) followed by those aged 30 to 40 years (489, 30.5%). A total of 1,453 (90.5%) were women. The majority of participating nurses earned less than 6,000 Chinese Yuan per month (this is equivalent to US$950). Only 130 nurses (8.1%) had a monthly salary of more than 10,000 Chinese Yuan (about US$1,600). In terms of education level, 638 (39.8%) had a high (vocational) school diploma whereas 492 (30.7%) possessed an associate degree. Most of them were married (1,116, 69.6%). Regarding work tenure at current job, a total of 509 (31.7%) nurses were working in their current position for only 6 months to 2 years whereas only 332 (20.7%) of the nurses had been at the same position for more than 6 years. The number of participants from tertiary, secondary, and primary hospitals was 823 (51.3%), 534 (33.3%), and 247 (15.4%), respectively. The number of beds in these hospitals ranged from 267 to 1,743. The number of nurses from each hospital also varied ranging from 314 to 2,565 per hospital.
Characteristics of Chinese Registered Nurses (N = 1,604)
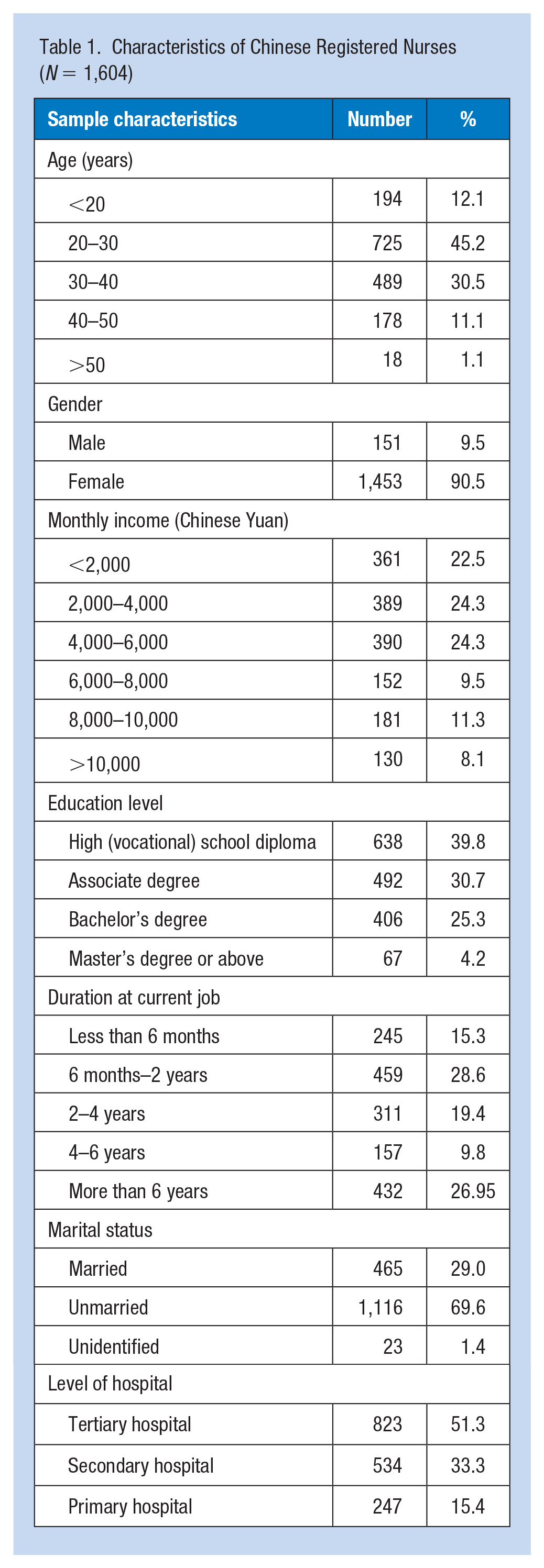
Table 2 provides the correlation coefficients for workplace incivility, perceived servant leadership, psychological distress as well as the control variables of age, gender, and income. Workplace incivility was associated with perceived servant leadership (r = −.18, p < .01) and psychological distress (r = .42, p < .01). Perceived servant leadership and psychological distress were also negatively correlated with each other (r = −.18, p < .01). The control variables were not associated with workplace incivility, perceived servant leadership, nor psychological distress.
Mean and Standard Deviation and Correlation Coefficient of Workplace Incivility, Perceived Servant Leadership, and Psychological Distress as Well as Their Correlations
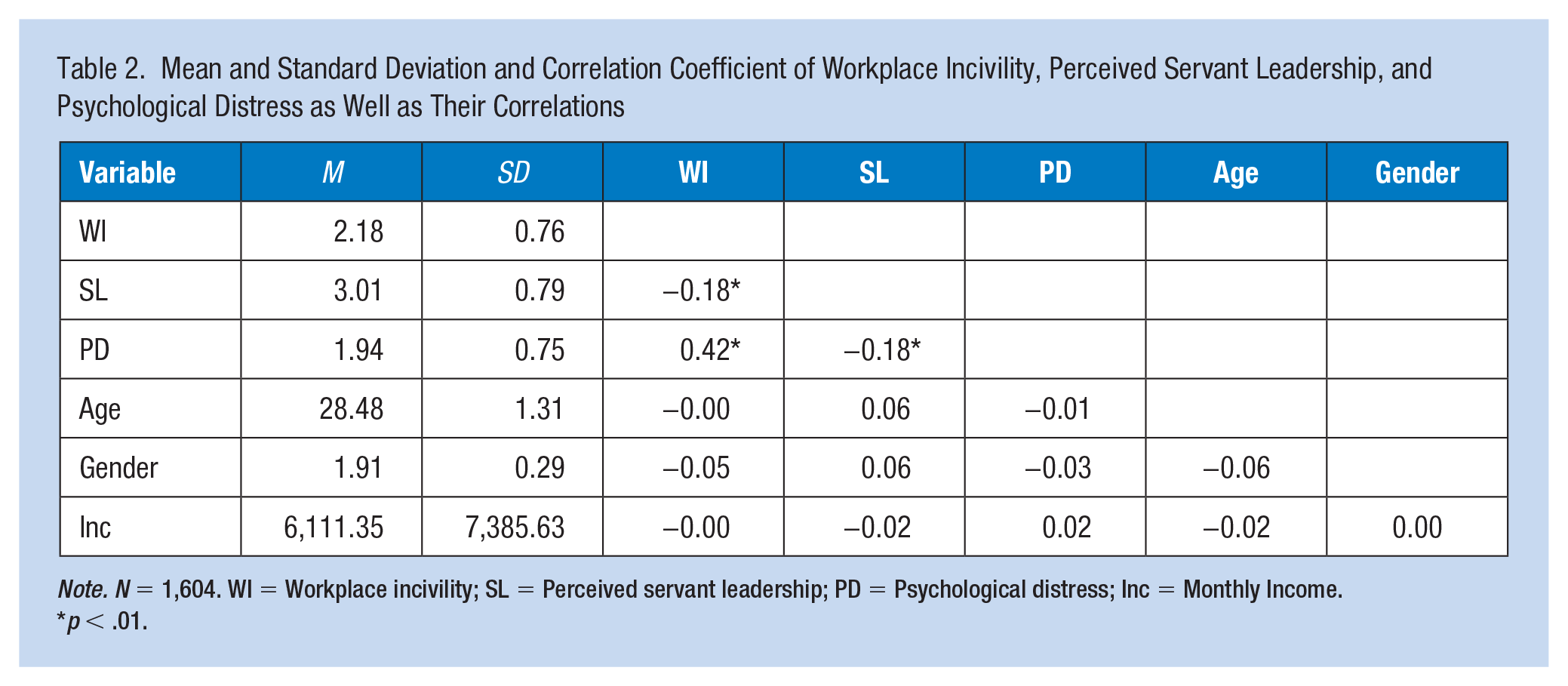
Note. N = 1,604. WI = Workplace incivility; SL = Perceived servant leadership; PD = Psychological distress; Inc = Monthly Income.
p < .01.
Before performing multiple linear regression to examine the moderation effect, we first tested the construct validity of three variables using confirmatory factor analysis (CFA). Results showed that factor loading of each item on each variable was greater than 0.50, average variance extracted (AVE) was also greater than 0.50, and composite reliability (CR) > .70. Therefore, three variables all had a good convergent validity. Furthermore, the root mean square error of approximation (RMSEA), comparative fit index (CFI), Tucker–Lewis index (TLI), and standardized root mean residual (SRMR) were calculated to test the measurement model fit. The results showed that these fit indices were good (χ2 = 3,314.230, df = 626, RMSEA = 0.052, CFI = 0.963, TLI = 0.951, SRMR = 0.047), indicating an achievement of discriminant validity. Table 3 presented the results of regression analyses examining perceived servant leadership as a moderator of the relationship between workplace incivility and psychological distress, R2 = .20, F(6, 1597) = 67.54, p < .001. It was revealed that workplace incivility (β = 0.40, p < .001), perceived servant leadership (β = −0.13, p < .001), and their interaction (β = −0.11, p = .002) were significantly related to psychological distress.
Regression Coefficients Among Variables
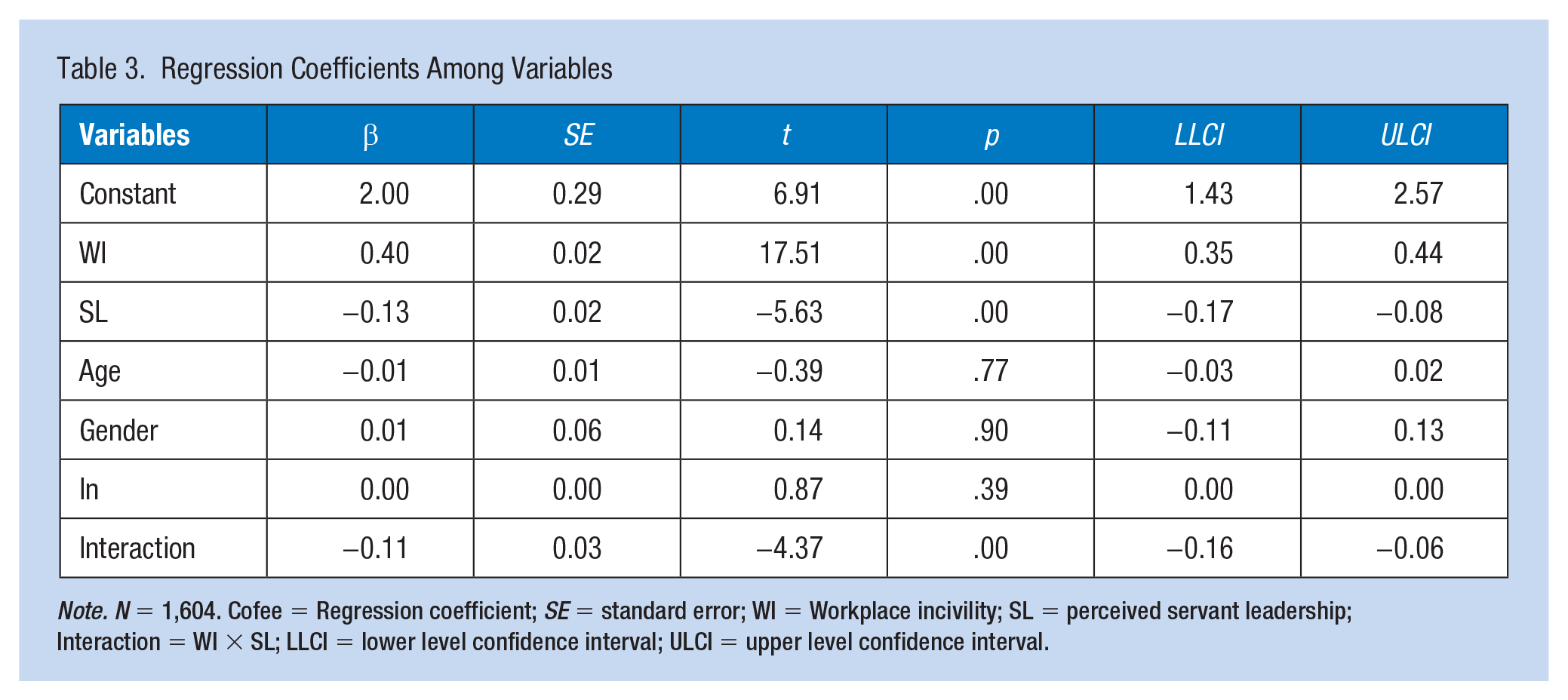
Note. N = 1,604. Cofee = Regression coefficient; SE = standard error; WI = Workplace incivility; SL = perceived servant leadership; Interaction = WI × SL; LLCI = lower level confidence interval; ULCI = upper level confidence interval.
To grasp the moderating effect of perceived servant leadership, we plotted the regression of psychological distress on workplace incivility at three scores of servant leadership (M + 1 SD, M, and M –1 SD; see Figure 1). The interactions between workplace incivility and psychological distress were all significant at low (β = 0.48, p < .001), mean (β = 0.39, p < .001), and high (β = 0.30, p < .001) levels of perceived servant leadership. Although the slopes of the three regression lines are different, psychological distress is positively related to workplace incivility for high, medium, and low levels of perceived servant leadership. The association between workplace incivility and psychological distress was strongest at low levels of perceived servant leadership, indicating that perceived servant leadership has a buffering effect.
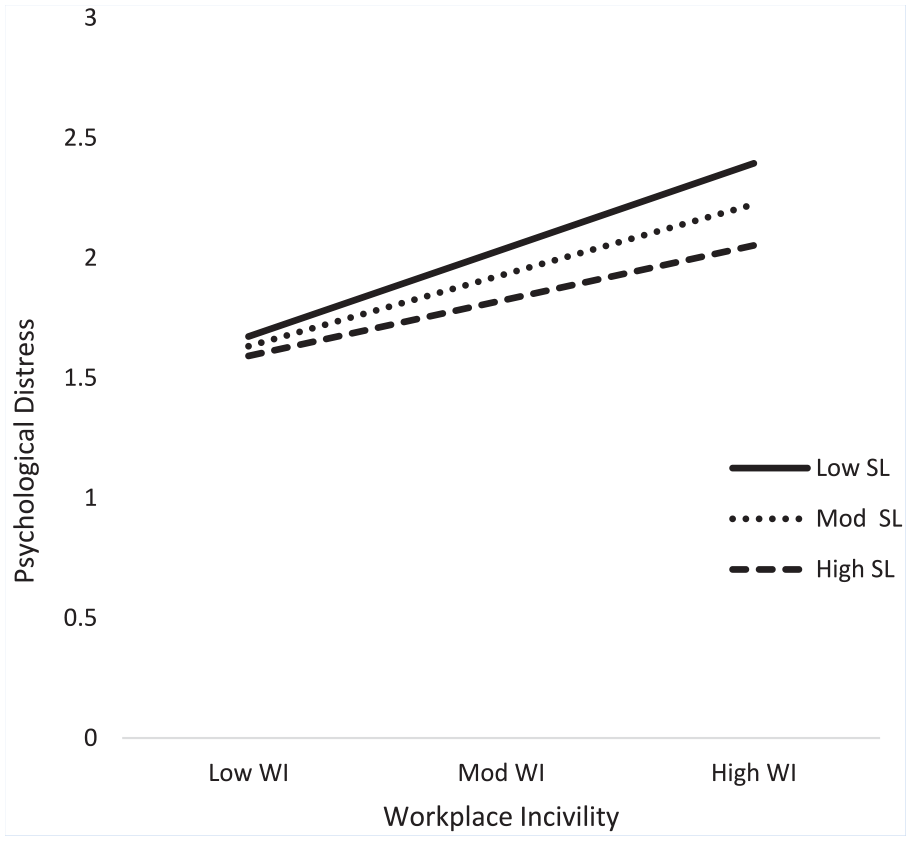
Moderating effect of perceived servant leadership.
Discussion
The current study examined the relationship between workplace incivility, perceived servant leadership, and psychological distress using a nurse sample collected in China during the COVID-19 epidemic. Although the previous study has linked workplace incivility with psychological distress, the underlying mechanism between these two variables remains unclear. No studies have examined how servant leadership moderates the relationship between workplace incivility and psychological distress among nurses in Chinese hospitals. Therefore, more studies are needed to investigate the interplay between these variables to better understand the complexities of psychological distress, as well as to plan interventions and take measures to improve nurses’ psychological health.
The relationship between workplace incivility and psychological distress was significant in the current study. These results aligned with the findings of a study by Geldart et al. (2018). Note that their study was conducted among postal workers in Canada. Several similar empirical findings have been observed signaling a detrimental effect of uncivil behaviors stemming from both co-workers and supervisors in Singapore (Lim & Lee, 2011) and Nigeria (Abubakar, 2018). The consistency of the results among these studies might signify that the deleterious impact of workplace incivility on employees’ psychological health might be universal, regardless of different cultures and industry sectors. While workplace incivility adversely affects employees’ mental well-being, support from servant leaders may serve as a cushion mitigating such a relationship. In our study, the interaction of workplace incivility and perceived servant leadership was significant in predicting nurses’ psychological distress. Prior studies have demonstrated that social support buffers the effect of employees’ job stress on their psychological well-being (Niedhammer et al., 2006). Geldart et al. (2018) even explicitly indicated the role social support plays in minimizing the effect of workplace incivility on psychological distress. The results of our study also dovetail with Miner et al.’s (2012) study that indicated emotional and organizational supports buffer the relationship between incivility and psychological well-being in the workplace. As discussed previously, emotional support is a form of social support. Servant leaders always provide emotional support to their followers whenever employees experience uncivil behaviors and disrespect from others (Spears, 1995). Our study results also showed that workplace incivility is positively related to nurses’ psychological distress, regardless of a perceived high level of servant leadership. This means that uncivil acts have a detrimental effect on their psychological health from the perspective of the nurses. Please note this study was conducted during the COVID-19 pandemic. As previously discussed, the COVID-19 significantly and adversely impacted the nurses’ psychological well-being (Wu et al., 2021; Xia et al., 2021). Most hospital nurses experience job-related stress (Liu, Aungsuroch, et al., 2021). During the COVID epidemic, this stress was even higher, resulting in health impacts such as sleeplessness, anxiety, depression, and post-traumatic stress disorder (PTSD) in some cases (Ariapooran et al., 2021; Cao et al., 2022; Xia et al., 2021). However, we argue that support from the servant leaders lessens the impact of incivility. Those who perceive a high level of servant leadership benefit most because they experience less psychological distress in the face of uncivil behaviors from supervisors and co-workers. In this sense, servant leaders in the hospitals are especially important during the COVID-19 pandemic because they are always supportive, put the nurses first, and provide emotional healing to their followers.
This study also supports social support theory (Vaux, 1988) and stress and coping theory (Biggs et al., 2017) by examining the moderating role of servant leadership in the field of nursing, thus adding value to both nursing and leadership literature. The study results offer additional evidence for the link between uncivil behaviors and psychological health. This study highlights the significance of incivility as a risk factor for nurses’ well-being. It was also found that the relationship between incivility from supervisors or co-workers and nurses’ psychological distress was weaker at a higher level of perceived servant leadership.
There are several limitations to the current study. First, this study used a cross-sectional design. Therefore, causal links between variables cannot be drawn from the study findings. Future research should utilize an experimental design or a longitudinal design to test causal relationships. Second, although appropriate for the current study, the data were collected from Chinese hospitals, potentially limiting the generalizability of the study results to other cultures, especially western cultures. In Chinese culture, it is important to maintain harmony in society (Cai et al., 2019; Cheung et al., 2020). Nurses tend to keep silent when they encounter uncivil behaviors at the workplace, leading to more psychological health issues (Zhan et al., 2019). It is especially so if the incivility comes from supervisors (Liu et al., 2018). Investigating the buttering effect of servant leadership in other nations or cultures is highly recommended. Limitations notwithstanding, the current study highlights the importance of servant leadership in increasing nurses’ psychological health.
Implications for Occupational Health Nursing Practice
This study has important implications for occupational health nursing practice. First, this study showed that workplace incivility is positively related to psychological distress among Chinese nurses. The more uncivil behaviors happened to nurses, the more severe their psychological health. Workplace incivility cannot be ignored in hospitals. Nursing managers should set a good example in modeling civil behaviors. Nursing supervisors need to educate their subordinates to exhibit healthy and civil behavior toward co-workers and patients, creating a safe work environment to prevent such behaviors. Second, this study also demonstrated that servant leadership makes a difference in the relation between uncivil behaviors and the victim’s well-being. Hospitals should recruit, select, and train their managers and supervisors to be servant leaders. If nurses perceive their supervisor to exhibit servant leadership behaviors, they will suffer less psychologically and mentally at the time or after they are perpetrated by uncivil behaviors.
Servant leaders can create an ethical work climate, display empathy, compassion, and facilitate resilience. Our findings can assist hospital management with support from occupational health providers to recruit, train, and assess nursing supervisors. Also, occupational health providers in collaboration with nursing administration can monitor incivility, psychological distress, servant leadership levels, and impact.
“Applying Research to Occupational Health Practice”
Psychological distress has been a major issue in the workplace and is especially prevalent among nurses across the globe. Given its adverse impact on nurses’ health (and probably many other types of employees) employers, including health care organizations, must take protective measures to reduce or prevent psychological distress among nurses working in hospitals. This study found that workplace incivility and perceived servant leadership predicted nurses’ psychological distress among nurses in Chinese hospitals. Especially, perceived servant leadership moderated the relationship between workplace incivility and psychological distress. This study highlights the importance of servant leadership in Chinese hospitals as servant leaders can create an ethical work climate, display empathy and compassion and provide emotional healing, and assist nurses to develop resilience. Occupational health providers in collaboration with nursing administration can monitor incivility, psychological distress, servant leadership levels, and impact on nurses’ health. Several organizations such as Servant Leadership Institute (Website: www.servantleadershipinstitute.com), eCornell (Website: ecornell.cornell.edu/certificates/leadership-and-strategic-management/servant-leadership), Greenleaf Academy (Website: www.greenleaf.org/greenleaf-academy) provide servant leadership training programs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by China Women’s University (No: ZKY209020208).
Ethical Approval
This study was approved by China Women’s University on July 8, 2020. ID number is EC 2020029. Permission was obtained from the sample hospitals for data collection. Participation was completely voluntary. Data confidentiality was guaranteed.
Author Biographies
Shaoping Qiu, PhD, is a postdoctoral researcher in the Department of Engineering Technology and Industrial Distribution, Texas A&M University. His research interests include organizational leadership, organizational change, stress and well-being, systematic review, and quantitative methods such as multiple regression, structural equation modeling (SEM), hierarchical linear model (HLM), item response theory, and meta-analysis.
Ruijuan Zhang, PhD, is an associate professor in School of Management, China Women’s University. Her research interests include human resource management, leadership, and gender studies.