
Abstract
Background:
There is evidence of disparities in COVID-19 vaccine acceptance among health care providers. The purpose of this study was to examine confidence receiving and recommending COVID-19 vaccines by health care provider type and race/ethnicity.
Methods:
This mixed methods study involved a cross-sectional survey and qualitative, semi-structured interviews from March to May 2021 among a sample of physicians, advanced practice providers, nurses, and pharmacists. These workers were recruited through voluntary response sampling from an integrated health system in Southern California. The primary dependent variables were (a) confidence in vaccine safety, (b) confidence in vaccine effectiveness, and (c) intent to recommend the vaccine to others. The primary independent variables were health care provider type and race/ethnicity.
Findings:
A total of 2,948 providers completed the survey. Nurses relative to physicians were 15% less likely to perceive the COVID-19 vaccine to be safe (risk ratio [RR] = 0.85; 95% confidence interval [CI] = 0.83–0.87); 27% less likely to perceive the vaccine to prevent COVID-19 (RR = 0.73; 95% CI = 0.69–0.76); and 11% less likely to recommend the vaccine to others (RR = 0.89; 95% CI = 0.87–0.91). Hispanic/Latinx providers were 10% less likely to perceive the vaccine to prevent COVID-19 (RR = 0.90; 95% CI = 0.83–0.98) relative to White providers. Qualitative themes included: No need for vaccine; distrusting vaccine research and roll-out; caretaking barriers; uncertainty and potential to change one’s mind; framing vaccine decisions around personal beliefs.
Conclusions & Application to Practice:
Health care workplaces should consider interventions to increase COVID-19 vaccination among their workers, including education and mandatory vaccination policies.
Introduction
More than a year into the COVID-19 pandemic, COVID-19 transmission and burden remain high. COVID-19 vaccines are essential for ending the pandemic, and there are more than 50 COVID-19 vaccines in prelicensure clinical trials (Kim et al., 2021). In the United States (US), mRNA vaccines (Moderna, Pfizer/BioNTech) and non-replicating viral vector vaccines (Janssen) have been authorized for emergency use in adults and children ages 12 years or older (Poland et al., 2020). One vaccine, the Pfizer/BioNTech mRNA vaccine, is fully approved by the U.S. Food and Drug Administration (U.S. Food and Drug Administration, 2021). The U.S. government initiative Operation Warp Speed aimed to accelerate COVID-19 vaccine development and deliver 300 million vaccine doses to Americans by early 2021. However, as of July 2021, only approximately 50% of adults were fully vaccinated, while vaccine demand has rapidly declined (Centers for Disease Control and Prevention, 2021). Enthusiasm for COVID-19 vaccines has dampened due to concerns that the accelerated timeline for vaccine development could have compromised safety and effectiveness; worries about vaccine side effects; and a lack of perceived need for a vaccine (Pogue et al., 2020; Reiter et al., 2020). Surveys early in COVID-19 vaccine development found political views and concerns about low efficacy and severe adverse events were associated with intent to decline a COVID-19 vaccine (Kreps et al., 2020).
Vaccine hesitancy is of particular concern among populations that have been disproportionately affected by COVID-19 infection, disease, and death, including racial/ethnic minorities and health care workers. Prior research suggests Black/African American and Latinx individuals are less likely to receive vaccines, and this pattern has held true for COVID-19 vaccines (Ojha et al., 2015; Williams et al., 2016). While health care workers are historically among those most likely to receive vaccines, there are concerning patterns of low uptake of COVID-19 vaccine among nurses and racial/ethnic minority health care workers (Gadoth et al., 2021). A recent survey of a large academic medical center found 87% vaccine uptake among nurses, compared with 99.5% uptake among physicians (Moniz et al., 2021). This vaccination level among nurses is similar to the level observed in a national survey of nurses conducted by the American Nurses Association, in which 88% of nurses reported receiving or planning to receive a COVID-19 vaccine (American Nurses Association, 2021). While data on the overall vaccination level among nurses across all settings and education levels in the United States are limited, recent research suggest that a majority of health care workers nationally have received a COVID-19 vaccine, with lower uptake among Black, Asian, and Latinx health care workers and those working in nursing homes, home health, and outpatient settings (Grumbach et al., 2021). These gaps in health care provider vaccination are concerning given their higher potential burden of exposure to COVID-19.
Low levels of COVID-19 vaccination among health care workers could exacerbate racial/ethnic disparities in COVID-19 outcomes and may present a problem for wider public vaccination. Health care providers play a vital role in creating confidence and trust around COVID-19 vaccines for their patients (Ylitalo et al., 2013). Although prior surveys have assessed COVID-19 vaccine intentions, uptake, and hesitancy among health care workers generally, less is known about reasons for vaccine hesitancy versus acceptance for subgroups of health care providers (e.g., nurses). There is also limited research on how health care worker COVID-19 vaccine confidence affects perspectives on patient vaccination (Meyer et al., 2021). Existing surveys of health care provider vaccination do not allow for in-depth assessment of reasons for confidence and identification of potential intervention targets. There is an urgent need for data on vaccine confidence among health care workers to inform development of interventions that support COVID-19 vaccine confidence. The purpose of this mixed methods study was to examine differences in COVID-19 vaccine perceptions and uptake by health care provider type and race/ethnicity; and to investigate whether provider type and race/ethnicity were associated with vaccine confidence and intentions to recommend the vaccine to others. We sampled health care providers practicing within Kaiser Permanente Southern California, an integrated health system in Southern California. Kaiser Permanente Southern California was offering COVID-19 vaccines to both providers and patients at the time of our survey in Spring 2021, and while all health care providers were eligible for vaccination, it was not mandatory.
Methods
This study used a mixed methods approach with quantitative and qualitative data collected in parallel. The study took place from March to May 2021 at Kaiser Permanente Southern California, an integrated health system with 15 hospitals and over 200 clinics. We conducted a one-time, web-based survey assessing COVID-19 experiences, COVID-19 vaccine perceptions and confidence, and demographic characteristics. We also conducted semi-structured qualitative interviews to explore health care provider COVID-19 vaccine perceptions. The survey was anonymous, except for those who opted to participate in an individual interview. The study was approved by the Kaiser Permanente Southern California Institutional Review Board, and all participants gave informed consent.
Health care providers were eligible to participate in the survey if they were currently practicing within Kaiser Permanente Southern California and had access to a web-enabled device to complete the survey (phone, tablet, computer). We engaged leadership in medicine, nursing, and pharmacy to email the survey opportunity to their staff. Two reminder emails were sent from clinical leadership, and they were also provided with study flyers to post at hospitals and clinics.
Survey Measures
The primary dependent variables were three binary items assessing COVID-19 vaccine confidence: (a) Do you think the COVID-19 vaccine is safe? (yes/no) (b) Do you think the COVID-19 vaccine will prevent COVID-19? (yes/no) (c) How likely are you to recommend the COVID-19 vaccine to others? (Will actively recommend or recommend when asked/Unsure or will not recommend).
The primary independent variables were self-identified provider type (physician, advanced practice provider [physician assistant or advanced practice registered nurse], nurse [registered nurse or licensed vocational nurse], pharmacist, and other) and race/ethnicity (White, Black/African American, Hispanic/Latinx, Asian, Multiracial, Other).
Demographic data collected included gender, age, history of testing positive for COVID-19, COVID-19 vaccination status, and history of high-risk medical conditions (chronic disease [cancer, chronic kidney disease, chronic obstructive pulmonary disease, heart conditions, organ transplant, sickle cell disease, Type 2 diabetes mellitus], pregnancy, obesity, smoking) potentially influencing perceptions of and confidence in COVID-19 vaccines.
Rapid Qualitative Assessment Procedures
We conducted semi-structured interviews with both providers who accepted or declined the COVID-19 vaccine. Participants who indicated in the survey that they would be willing to be contacted for a follow-up interview were recruited, stratified by provider type (physician, pharmacist, nurse) and by whether or not they had received a COVID-19 vaccine. We contacted 10 participants in each of these six groups (60 total), ensuring representation of a variety of provider vaccine perspectives. The interview guide was based on the Determinants of Vaccine Hesitancy matrix and included open-ended questions about COVID-19 experiences and vaccine perceptions (MacDonald et al., 2015). We conducted interviews by phone; each lasted approximately 15 to 30 minutes, was recorded, and later transcribed using transcription software. Study staff compared recordings against transcripts and corrected errors prior to analysis. A total of 32 interviews were conducted across all provider/vaccine groups (nurses = 15, pharmacists = 8, physicians = 9). Seventeen interviewees declined the vaccine.
Data Analysis
For quantitative survey data, we used chi-square tests to compare health care providers (physicians, physician assistants/nurse practitioners, pharmacists, nurses, others) by demographics, COVID-19 vaccination and vaccine confidence, and reasons for COVID-19 vaccine decisions. These analyses were repeated to compare health care providers by race/ethnicity (Hispanic/Latinx, White, Black/African American, Asian, Other). We used robust Poisson regression models to estimate relative risk of vaccine confidence outcomes, comparing (a) provider type and (b) race/ethnicity subgroups. We first estimated the association between provider type and perception of vaccine safety, perception of vaccine effectiveness, and whether providers planned to recommend the vaccine to others. Each of these vaccine confidence items was modeled as a binary dependent variable with provider type as the independent variable, adjusted for demographic items. This modeling was repeated with race/ethnicity as the independent variable. We used risk ratios (RRs) and 95% confidence intervals (CIs) as a measure of effect size. All analyses were conducted using R, version 4.0.3.
For qualitative data, we used qualitative Rapid Assessment Procedures (RAP) and thematic analysis to collect, analyze, and triangulate data (Braun & Clarke, 2006; Palinkas & Zatzick, 2019; Scrimshaw & Hurtado, 1987). Qualitative data were collected to further elucidate perspectives on COVID-19 vaccines among health care workers. Transcripts were reviewed and coded by two independent coders, using gerund coding to delineate an initial set of codes (Carmichael & Cunningham, 2017). Codes were then discussed among study investigators and stakeholder representatives from each provider group interviewed (nurses, physicians, pharmacists) to verify findings and collapse and/or further divide codes into themes. Resulting themes were then triangulated with survey data on reasons for accepting or declining the COVID-19 vaccines reported in the survey.
Results
A total of 3,164 potential participants opened the survey, 3,052 verified eligibility and consented to the survey, and 2,948 completed it. The sample comprised 45.0% physicians (n = 1,326), 40.2% nurses (n = 1,184), 8.8% pharmacists (n = 259), and 5.7% advanced practice providers (n = 169) (Table 1). The majority of respondents were female (69.6%, n= 2,051) and White (36.9%, n = 1,087) or Asian (39.1%, N = 1,153). Eight percent of respondents (n = 240) reported a history of testing positive for COVID-19 and 1.9% of the sample (n = 55) reported being pregnant. COVID-19 vaccine uptake was high among the sample, with an overall 91.3% of respondents (n = 2683) reporting receiving at least one dose of a COVID-19 vaccine.
Demographic and Background Information of Health Care Worker Survey Respondents in a Southern California Health System (N = 2,948)
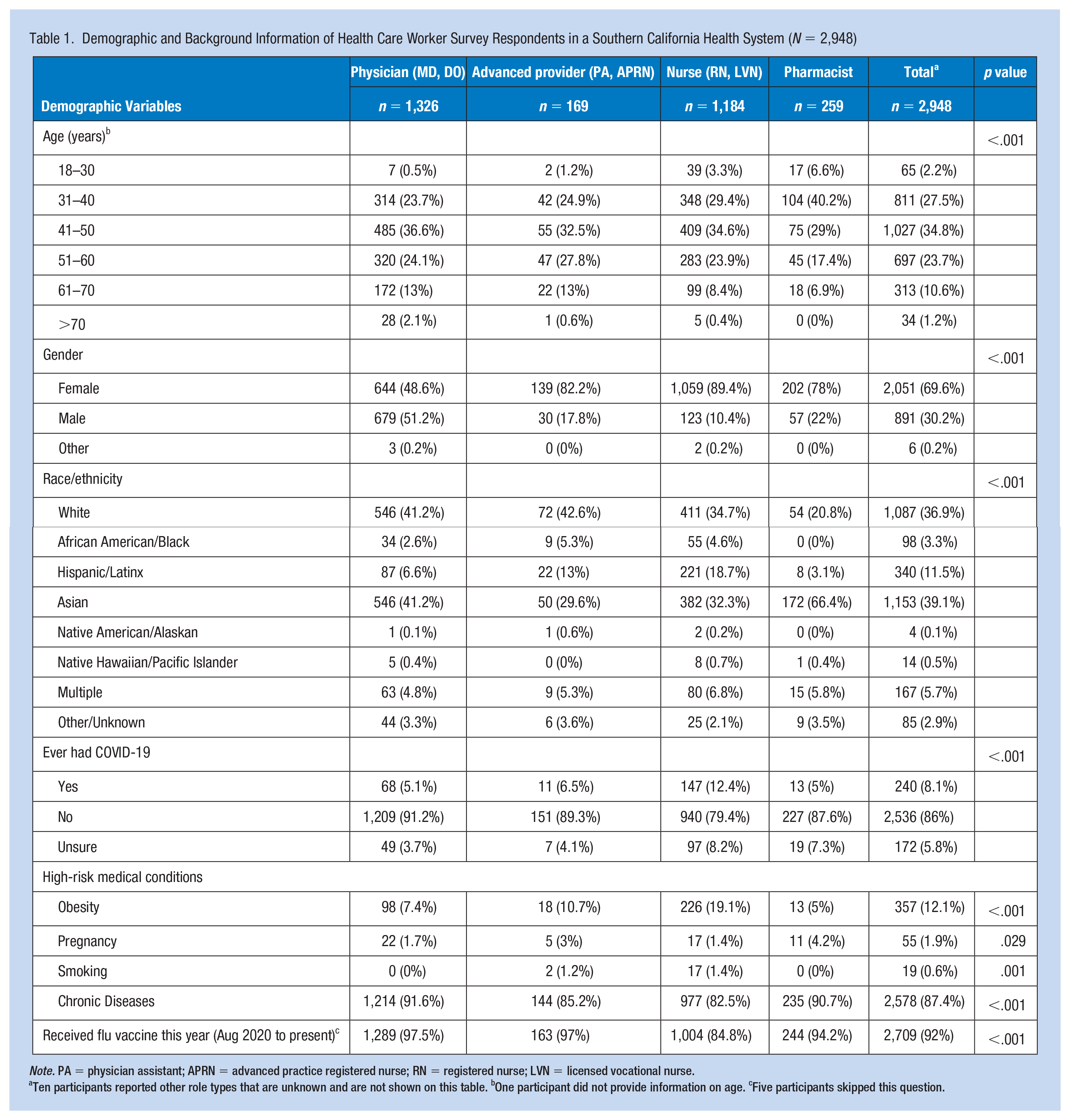
Note. PA = physician assistant; APRN = advanced practice registered nurse; RN = registered nurse; LVN = licensed vocational nurse.
Ten participants reported other role types that are unknown and are not shown on this table. bOne participant did not provide information on age. cFive participants skipped this question.
COVID-19 vaccine uptake differed by type of health care provider, with the lowest uptake reported by nurses (82.9%, n = 980) versus 98.1% (n = 1294) by physicians; 95.9% (n = 162) by advanced practice providers; and 92.3% (n = 259) reported by pharmacists (Table 2). These proportions were comparable to those of the 2020–2021 influenza vaccine uptake reported in our study. Notably, nurses also had the highest percentage with a prior positive COVID-19 test (12.4% of nurses versus 5.1% of physicians, 6.5% of advanced practice providers, and 5% of pharmacists) and reported lower vaccine confidence across all three outcomes.
COVID-19 Vaccine Perspectives Among Health Care Workers in a Southern California Health System Who Responded to a Survey of COVID-19 Vaccine Confidence Between March and May 2021
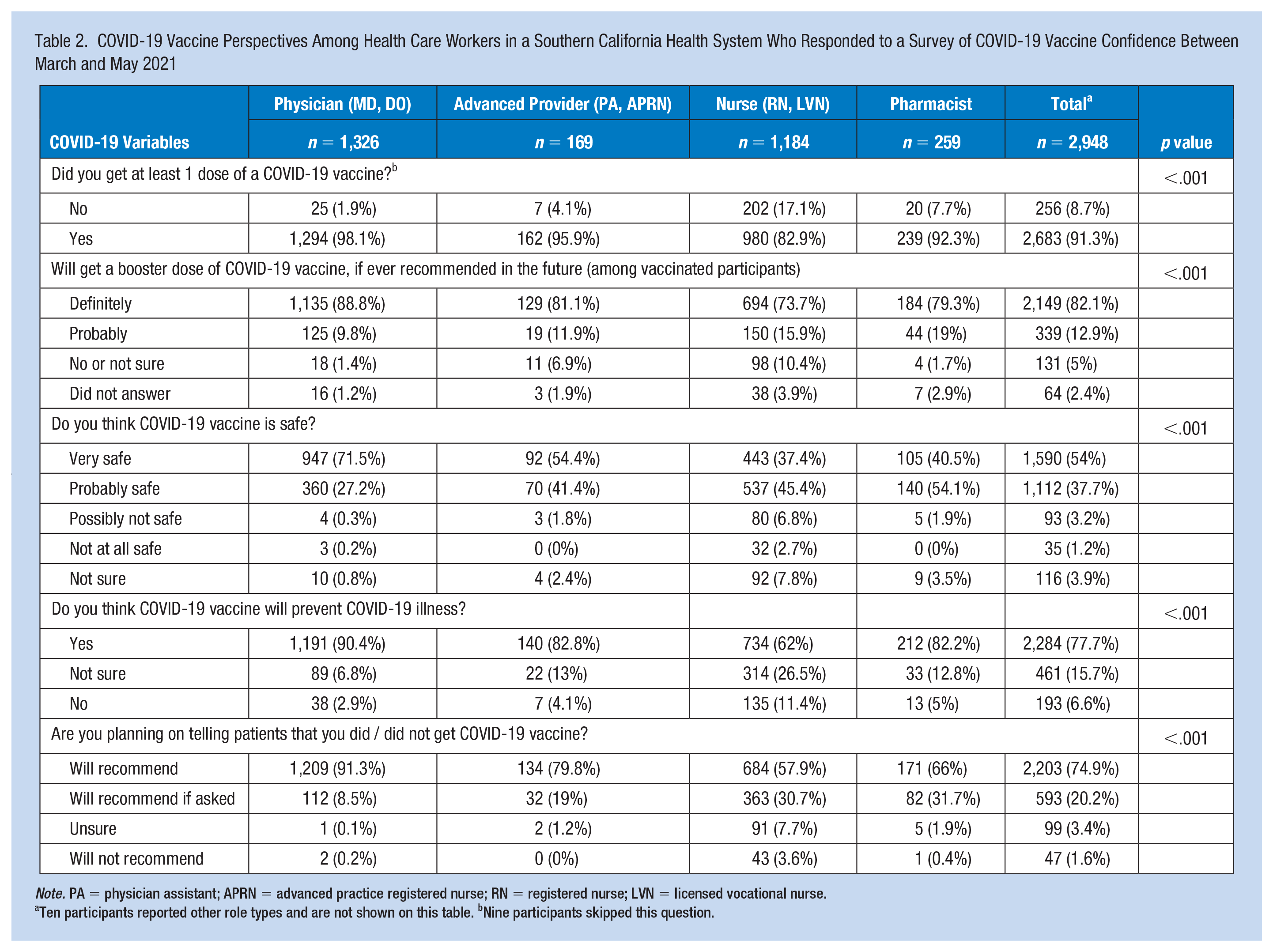
Note. PA = physician assistant; APRN = advanced practice registered nurse; RN = registered nurse; LVN = licensed vocational nurse.
Ten participants reported other role types and are not shown on this table. bNine participants skipped this question.
Vaccine uptake also differed by race/ethnicity (Supplement 1). There was 100% uptake by providers who identified as Native American, Alaskan Native, and Native Hawaiian/Pacific Islander, though these groups were small (n = 18). Participants who identified as White and Asian also had high levels of uptake (90.2%/n = 976% and 95.5%/n = 1101, respectively) relative to those who identified as Black/African American (84.7%, n = 83), Hispanic/Latinx (86.4%, n = 293), and Multiracial (84.8%, n = 139). These same racial/ethnic groups with low uptake reported lower vaccine confidence across all outcomes.
In adjusted models, nurses relative to physicians were 15% less likely to perceive the COVID-19 vaccine to be safe (RR = 0.85; 95% CI = 0.83–0.87); 27% less likely to perceive the vaccine to prevent COVID-19 (RR = 0.73; 95% CI = 0.69–0.76); and 11% less likely to recommend the vaccine to others (RR = 0.89; 95% CI = 0.87–0.91) (Table 3). Pharmacists also had significantly lower likelihood of all three vaccine confidence outcomes in relation to physicians, though RRs were smaller in magnitude than nurses. Race/ethnicity differences in vaccine confidence were less pronounced in adjusted models. Participants who identified as Asian were 6% more likely to perceive the vaccine to be safe (RR = 1.06; 95% CI = 1.04–1.09) as well as 5% more likely to recommend the vaccine to others (RR = 1.05; 95% CI = 1.03–1.07) in adjusted models, relative to participants who identified as White. Participants who identified as Hispanic/Latinx were 10% less likely to perceive the vaccine to prevent COVID-19 (RR = 0.90; 95% CI = 0.83–0.98) relative to participants who identified as White.
Associations of Health Care Provider Type and Race/Ethnicity With COVID-19 Vaccine Confidence in a Survey of COVID-19 Vaccine Confidence Conducted From March and May 2021
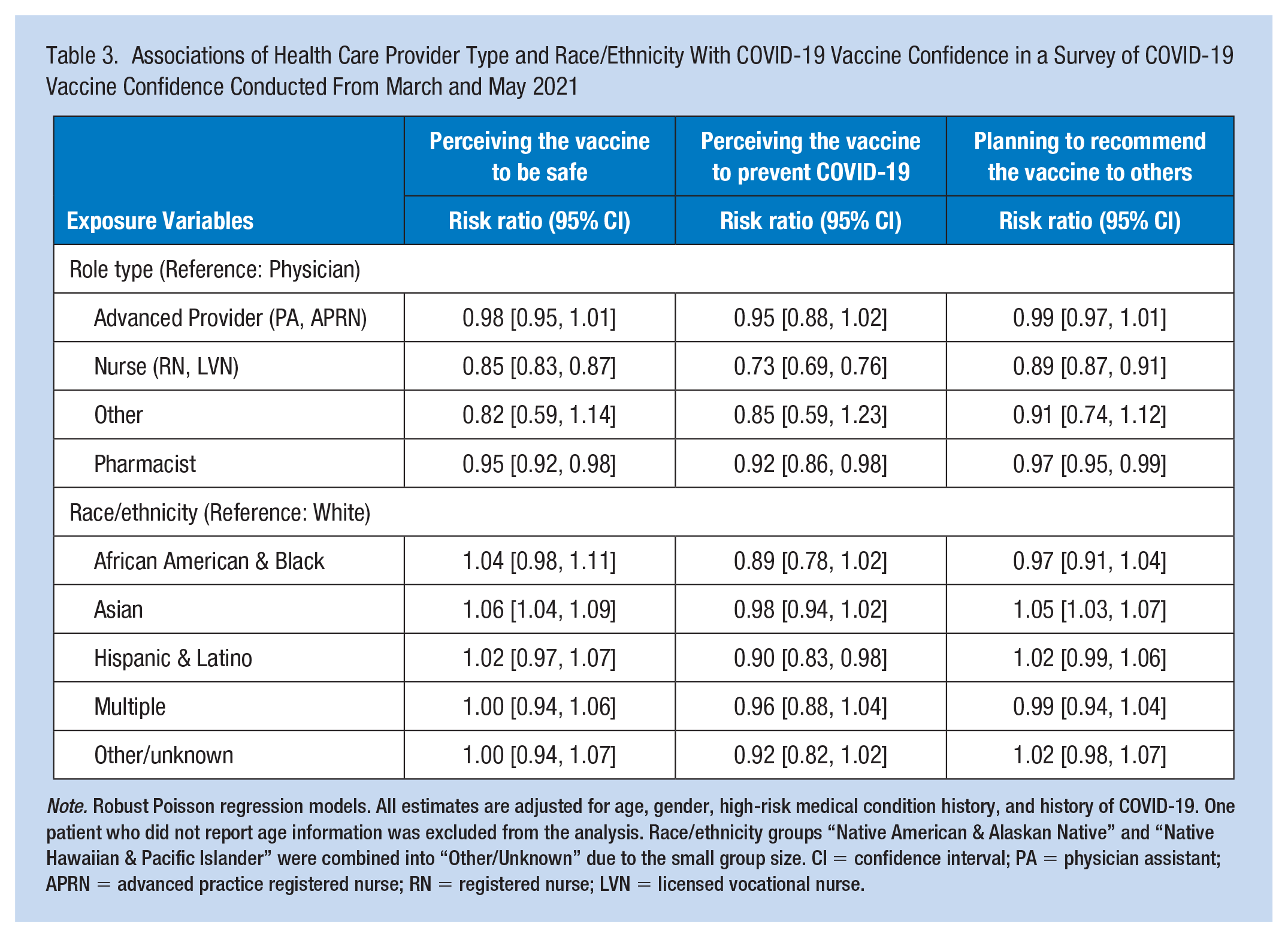
Note. Robust Poisson regression models. All estimates are adjusted for age, gender, high-risk medical condition history, and history of COVID-19. One patient who did not report age information was excluded from the analysis. Race/ethnicity groups “Native American & Alaskan Native” and “Native Hawaiian & Pacific Islander” were combined into “Other/Unknown” due to the small group size. CI = confidence interval; PA = physician assistant; APRN = advanced practice registered nurse; RN = registered nurse; LVN = licensed vocational nurse.
Perspectives on Vaccine Acceptance or Declination
Reasons for vaccine acceptance or declination by provider type are shown in Figure 1. Qualitative data triangulated with survey data validated these reasons, and also provided detail about how providers, especially nurses who had lower levels of vaccine uptake and lower odds of vaccine confidence, perceived COVID-19 vaccines. While there were some strong beliefs for or against vaccines, many providers expressed uncertainty and described themselves as “on the fence” about the COVID-19 vaccine, in the words of one nurse. Reasons for vaccine declination were more varied from what was reported in the survey, as described in themes below.
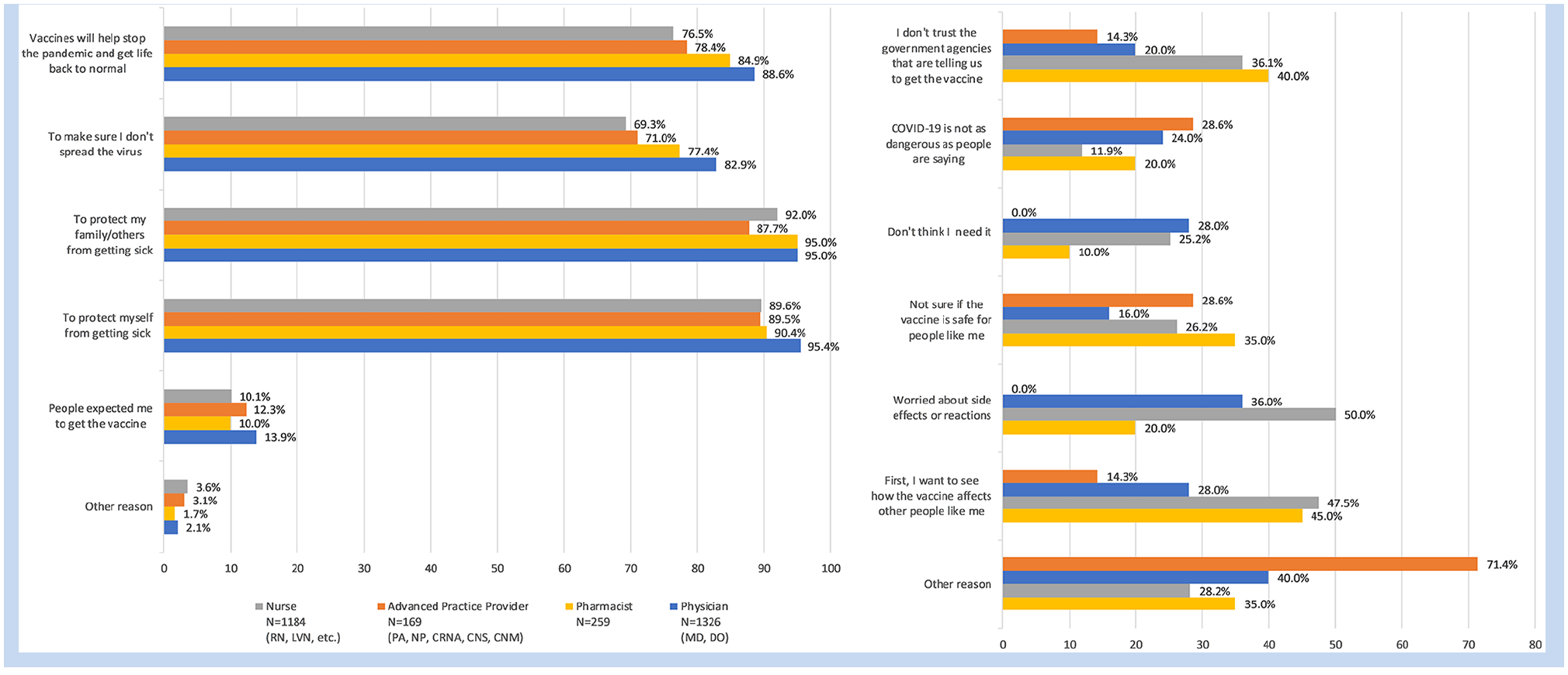
Reasons for vaccine acceptance and declination by provider type.
Protecting Self, Family, and Patients and Ending the Pandemic
Providers described wanting to “end the pandemic” (pharmacist, accepted) and “live a normal life” (nurse, accepted vaccine). There was also an emphasis on getting the vaccine to protect providers’ families, communities, and patients. A physician-accepter stated, “I wanted to protect myself and protect my family, particularly my two small kids. I wanted to protect my patients.” Similarly, a breastfeeding nurse-accepter stated, “I wanted to have antibodies for my baby.”
Not Seeing Need for the Vaccine
Many providers who declined the vaccine did not see a need for or benefit to getting the vaccine. This view was frequently expressed in the context of having already had COVID-19 or perceiving oneself to be young, healthy, and not at high risk. For example, a physician-decliner stated, “I had COVID right before the vaccines were available, so I did not get a vaccine. Because I’m not seeing patients, my risk for spreading it is low.” Likewise, a pharmacist-decliner said, “I really don’t need the vaccine. I’ve had COVID.” A nurse-decliner said, “I don’t think it’s [COVID-19] as dangerous as people say,” as did a third nurse: “I don’t live my life in fear. It’s not that I’m belittling or minimizing the fact that it’s killed people . . . There’s also a lot of people that got COVID who are alive and well and breathing.” This lack of perceived need for the vaccine held true even for some participants who worked with COVID-19 patients.
Related to not perceiving oneself to be at risk from COVID-19, some providers did not perceive any benefit to receiving the vaccine. A nurse-decliner stated, “You can still get COVID, you can still transmit COVID, so what’s the point?” Another nurse-decliner connected her perceived lack of benefit to mask-wearing:
If the whole community decided as a whole that it was safe there was no mask wearing or anything like that, then there would be some sort of benefit to getting the vaccine and not having to wear masks everywhere you go. But that’s not what happened.
Distrusting Vaccine Safety Research, Mechanisms, and Roll-Out
Some participants expressed discomfort with mRNA vaccines, as described by a pharmacist-decliner: “I’m willing to do the Johnson & Johnson, it’s just, the Pfizer and Moderna, the mechanism of how the vaccine was made is different, it’s a new mechanism. So I’d rather do the Johnson & Johnson.” A physician-decliner expressed a similar preference for the non-mRNA, as did a nurse-decliner.
Some provider-decliners were concerned by the short timeframe from development to emergency use authorization and worried about health risks in the short or long term. A nurse-decliner shared, I’ve heard of this doctor who died in Florida, healthcare worker in California who got it the same day or shortly after and died, and they just say “There’s no correlation”—I just find that very hard to say, that it didn’t have anything to do with it.
Other nurses said, “I felt like it came out way too fast” and “The amount of people that were in the studies were like, grains of sand compared to the amount of people that are in the world.” Providers often described watching or waiting before they made a decision, indicating that they were still uncertain about safety research. A physician-decliner said, “I won’t rush to be at the front of the line for the vaccine because I’m not at high risk.”
Parenting Barriers
Several participants noted barriers related to their children. A pharmacist-decliner worried about vaccine side effects with no child care available post-vaccine stated “babysitting is a real issue for us.” A nurse-decliner, on the other hand, was unwilling to get the vaccine when her children could not, stating, “I actually felt selfish. I felt like, well why is it OK for me to be protected or semi-protected and for my kids to be vulnerable to this? . . . Once my children are able to get it, I’m definitely going to get it.”
Changing One’s Mind and Regretting Not Getting the Vaccine
Some participants discussed changing their minds between the time when they took the survey and the time when they were interviewed. This including providers with allergies, who eventually became reassured that allergic reactions to the vaccines were rare, and those who were breastfeeding or with other specific medical conditions (e.g., autoimmune disorders). These providers cited concerns about a lack of research on their specific conditions, but tended to have favorable views about the COVID-19 vaccines and expressed a desire to get the vaccines in the future. One nurse-decliner expressed regret over not getting the vaccine once she became ill with COVID-19. She stated, My views on the vaccine have truly changed . . . It’s been a struggle. I was OK with not getting the vaccine until I got sick. As soon as I tested positive, I really thought about it and I was like “Gosh, I feel, a lot of remorse, a lot of regret.” More so I was upset not because I was sick, I was like, what if my kids were sick?
The views of this participant related to the theme of getting the vaccine to protect one’s family. She further expressed changing her views on her perceived risk for COVID-19: “I’m healthy. And yet COVID got me . . . COVID is real.”
Framing Vaccine Decisions Around Personal Beliefs
Generally, providers framed their views on vaccines as an issue of personal beliefs and values. One nurse-accepter described herself as “a true believer” in vaccines, and another said, “I believe in it [vaccines] . . . I haven’t really thought about it.” Pharmacists and physicians spoke similarly about “belief” in vaccines. Those who were certain in their decision to decline the vaccine also talked about their views as personal beliefs, though they strongly rejected being identified “anti-vax.” For example, a nurse-decliner stated, “It’s not that I’m anti-vax, I just don’t believe that there need to be vaccinations.” Similarly, a nurse-decliner expressed that she did not “believe” in the vaccine so strongly that she refused to administer the vaccine to patients. Nurses also tended to express a belief that vaccines should be optional. Several spoke about their disagreement with past flu shot requirements, and even a nurse-accepter who was strongly in favor of the COVID-19 vaccine stated, The vaccine should be an option and not mandatory. If they are worried or concerned or don’t feel like they need to, they should keep their values and management should honor that belief . . . we just have to treat healthcare workers as people and understand that they are human beings too.
Discussion
This mixed methods investigation of vaccine uptake and confidence among health care providers in Southern California found high overall levels of COVID-19 vaccination, relative to the general public. Most providers perceive a clear benefit to receiving the vaccine to protect themselves, their families, and their patients, as well as a way to end the pandemic and return to normal life. High vaccination levels observed in this population may be due to provider health literacy and education on the benefits of vaccination, high potential occupational risk for exposure to COVID-19, and witnessing the harm of COVID-19 firsthand in clinical encounters during the pandemic. Prior research suggests that health care providers generally have higher vaccine confidence than non-providers, and this pattern held true in our study even with new COVID-19 vaccines (MacDougall et al., 2015). There is also a history of influenza vaccine requirements for health care providers, usually accompanied by mask requirements for those who decline the vaccine, which may have increased acceptance of COVID-19 vaccines in the health system (Poland et al., 2008; Tilburt et al., 2008).
Although overall vaccination levels were high, survey results indicated nurses had lower levels of vaccine uptake and lower vaccine confidence than physicians. As of August 2021, approximately 88% of nurses nationally report that they received or plan to receive a COVID-19 vaccine, which is comparable to the 83% of nurses who reported having received a vaccine in our survey (American Nurses Association, 2021). Nurses were 11% to 25% less likely than physicians to perceive the vaccine to be safe, perceive the vaccine to be effective, and to plan to recommend the vaccine to others in adjusted models. This pattern is potentially concerning, given that nurses may have higher occupational exposure to SARS-CoV-2 and that there is emerging evidence for benefit to COVID-19 vaccination even after natural infection (Andreano & Rappuoli, 2021; Jackson et al., 2020). In addition, our finding that providers who are most likely to be administering vaccines (nurses, pharmacists) were less likely to recommend the vaccine to others may indicate a need for interventions or care processes to ensure that patients considering COVID-19 vaccines have access to comprehensive vaccine information. Studies suggest that people tend to trust their personal health care providers, and negative provider views about vaccinations may influence patient uptake (Smith et al., 2006; Ylitalo et al., 2013). There is a need for provider-specific COVID-19 vaccine interventions that target modifiable reasons for vaccine declination and care processes for that promote vaccine confidence among patients, regardless of the recommendations or views of their individual care providers. Provider interventions may include vaccination incentives, evidence-based information about vaccine safety, paid time for seeking a vaccination and recovering from side effects, and educational materials that include accessibility information.
Our findings suggest racial differences in vaccine uptake, with lower levels of vaccine uptake among providers identifying as Black/African American, Hispanic/Latinx, or Multiracial. In adjusted models, Hispanic/Latinx providers were 10% less likely to perceive the vaccine to be effective relative to White providers, while Asian providers were 5% to 6% more likely to perceive the vaccine to be safe and to plan to recommend the vaccine to others relative to White providers. These findings align with prior surveys on health care provider vaccine uptake, as well as findings on race disparities in vaccine uptake in the general U.S. population (Grumbach et al., 2021; Moniz et al., 2021). Vaccine uptake and confidence were highest among Native American Indian, Alaskan Native, and Native Hawaiian/Pacific Islander providers, though the sample sizes for these groups were very small. Vaccine uptake among Native populations has been consistently higher than other racial groups, due in part to successful distribution strategies by tribal leadership and Indian Health Service personnel (Hill & Artiga, 2021). Successful tribal approaches of cultural tailoring, engaging trusted local leaders, and ensuring local accessibility should be considered for other populations where vaccine uptake is low.
In addition to providing education and encouraging as many providers as possible to receive a vaccine voluntarily with targeted outreach, health systems may need to consider mandating COVID-19 vaccination for health care workers as a strategy to promote patient safety. Prominent medical, nursing, public health, pharmacy, and other health professional organizations have strongly endorsed mandatory COVID-19 vaccination for health care providers (American Medical Association, 2021), and our findings lend support to a vaccine mandate for several reasons. First, our qualitative data on reasons for vaccine declination revealed that a majority of providers who had not yet received a COVID-19 vaccine expressed uncertainty and potential to change their minds in the future. Among these were providers who did not see an immediate need for the vaccine due to having had COVID-19 and those who wanted to see more long-term research before making a decision. There were also providers who specifically preferred the Johnson & Johnson adenovirus vaccine, which was temporarily paused during the time of our study interviews, and for whom vaccines are now readily available. Those who expressed parenting concerns, such as a lack of child care or waiting until the vaccine was approved for children, may also represent a group whose vaccine decisions are potentially modifiable. For these providers who are “on the fence” and cite modifiable barriers to vaccination, a vaccine mandate may be acceptable. Second, there were a small number of providers who declined the vaccine and who held views negative vaccine beliefs that may not be modifiable and for whom vaccination may not be achieved in the absence of a mandate. Some did not perceive a need for the vaccine because they described themselves as young and healthy, or they simply did not want the vaccine. Others expressed a general dislike of or distrust in vaccines and that they did not “believe” in vaccines. These views were usually accompanied by specific concerns about vaccine ingredients (e.g., preservatives) or more conspiratorial perspectives on the COVID-19 pandemic. The few providers who expressed these views were careful to state that they were not “anti-vaxxers,” despite holding beliefs consistent with anti-vaccination movements (Paterson et al., 2016; Tafuri et al., 2014). Although these negative vaccine perspectives were rare among health care providers in our sample, COVID-19 vaccine mandates for health care workers may ultimately be the only viable strategy for achieving an adequate level of vaccination among health care workers.
The mixed methods approach used in this study is a strength, as prior surveys have not elicited great detail about reasons for vaccine declination that may be amenable to intervention. Our qualitative interviews exploring individual vaccine perspectives, beliefs, and experiences provided depth about reasons for vaccine acceptance or declination that go beyond what could have been learned from a survey alone. We surveyed a large, diverse sample representing multiple health care provider groups and captured some temporal trends in vaccination, such as the temporary pause in administration of the Johnson & Johnson vaccine. Limitations to the study are the cross-sectional, self-report nature of the survey which may be subject to social desirability bias. The survey may have been subject to selection bias where those who received the vaccine were more likely to respond, and there was limited representation of certain racial/ethnic groups, such as Native American participants. We were only able to evaluate a survey response rate at the level of those who opened the survey, as our voluntary response sampling frame and multifaceted recruitment strategy did not allow for determination of an exact number of potential participants reached within the multi-hospital health system. However, levels of vaccination reported within provider groups in our survey are comparable to national averages and other similar survey studies, suggesting that our survey reached a reasonably representative group of respondents (American Nurses Association, 2021; Grumbach et al., 2021; Moniz et al., 2021) . Finally, we did not have sufficient response from advance practice providers for qualitative interviews to explore their perspectives.
Future research on vaccine confidence with health care providers should include clinical support staff (e.g., nurse aides, patient transporters, front desk staff) who may interface with patients. This includes research on culturally tailored strategies for racial/ethnic minority providers whose levels of COVID-19 vaccine uptake may be low in some areas of the United States. Future research on implementation of vaccine confidence interventions should consider modifiable declination targets identified in this study, such as access to vaccines and child care–related time constraints. Given that a majority of nurses (71%) and almost all professional health care organizations support some form of mandatory COVID-19 vaccination (full or limited) within health care settings, policies mandating COVID-19 vaccination should also be considered by employers (American Medical Association, 2021; American Nurses Association, 2021).
Implications for Occupational Health Practice
As COVID-19 vaccination slows in the United States and there is increased focus on increasing vaccine confidence, it is important to develop strategies for vaccine confidence specific to health care providers. Health care organizations should consider providing vaccine outreach, incentives, and education to promote voluntary vaccination among workers. COVID-19 vaccine mandates are now endorsed by almost all major professional health care provider organizations, and as such, health care organizations may also consider implementing policies for mandatory vaccination if voluntary outreach options fail to achieve sufficient levels of vaccination among health care providers. There is also a need to ensure that care processes for vaccination promote vaccine confidence among patients regardless of the views or vaccination status of individual care providers, such as by providing standardized patient education materials that encourage vaccination and note that vaccination is endorsed by major professional health organizations and governmental health organizations.
Applying Research to Occupational Health Practice
Health care providers have higher levels of COVID-19 vaccination than the general public. Most providers perceive a clear benefit to receiving the vaccine to protect themselves, their families, and their patients, as well as a way to end the pandemic and return to normal life. Although overall vaccination levels among health care providers are high, nurses and some racial/ethnic minorities reported relatively lower levels of vaccine uptake and confidence. In qualitative interviews, most unvaccinated providers described themselves as “on the fence” about receiving a COVID-19 vaccine. Health care organizations should consider providing vaccine outreach, incentives, and education to promote voluntary vaccination among workers. Because COVID-19 vaccine mandates are now endorsed by almost all major professional health care provider organizations and a majority of nurses in the United States, health care organizations may also consider implementing policies for mandatory vaccination if voluntary outreach options fail to achieve sufficient levels of vaccination among health care providers.
Supplemental Material
sj-docx-1-whs-10.1177_21650799211049811 – Supplemental material for “Still on the Fence” A Mixed Methods Investigation of COVID-19 Vaccine Confidence Among Health Care Providers
Supplemental material, sj-docx-1-whs-10.1177_21650799211049811 for “Still on the Fence” A Mixed Methods Investigation of COVID-19 Vaccine Confidence Among Health Care Providers by Kristen Choi, John Chang, Yi X. Luo, Bruno Lewin, Corrine Munoz-Plaza, David Bronstein, June Rondinelli and Katia Bruxvoort in Workplace Health & Safety
Footnotes
Acknowledgements
We thank CIRT and clinical leaders in nursing, medicine, and pharmacy at KPSC for supporting this study and participant recruitment.
Conflict of Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors have no conflicts of interest related to the contents of this article. Y.L. discloses funding unrelated to this study from GlaxoSmithKline, Novavax, Seqirus, Moderna. K.B. discloses funding unrelated to this study from GlaxoSmithKline, Seqirus, Gilead, Dynavax, Pfizer, and Moderna.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from the Care Improvement Research Team (CIRT) within the Department of Research & Evaluation at Kaiser Permanente Southern California. The funder had no role in the design of the study, data collection/analysis, interpretation of data, or writing the manuscript.
Human Subjects Review
This study was approved by the Institutional Review Board at Kaiser Permanente Southern California (KPSC-IRB-12746). All participants gave informed consent.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
Kristen Choi, PhD, RN, is an assistant professor of nursing and public health at the University of California, Los Angeles (UCLA). Dr. Choi drafted the initial manuscript, assisted with data analysis, and reviewed the final version of the manuscript for intellectual content.
John Chang, MPH, is a research assistant in the Department of Research and Evaluation at Kaiser Permanente Southern California. Mr. Chang assisted with qualitative data collection and analysis and reviewed the final version of the manuscript for intellectual content.
Yi X. Luo, PhD, is a research biostatistician manager in the Department of Research and Evaluation at Kaiser Permanente Southern California. Dr. Luo led quantitative data analysis and reviewed the final version of the manuscript for intellectual content.
Bruno Lewin, MD, DTMH, is a family medicine physician with Southern California Permanente Medical Group. Dr. Lewin assisted with conceptualizing the study and reviewed the final version of the manuscript for intellectual content.
Corrine Munoz-Plaza, MPH, is a qualitative research lead in the Department of Research and Evaluation at Kaiser Permanente Southern California. Ms. Munoz-Plaza assisted with conceptualizing the study, assisted with qualitative data analysis, and reviewed the final version of the manuscript for intellectual content.
David Bronstein, MD, MS, is a pediatric infectious disease physician with Southern California Permanente Medical Group. Dr. Lewin assisted with conceptualizing the study and reviewed the final version of the manuscript for intellectual content.
June Rondinelli, PhD, RN, CNS, is a nurse scientist with Southern California Nursing Research at Kaiser Permanente Southern California. Dr. Rondinelli assisted with data collection and reviewed the final version of the manuscript for intellectual content.
Katia Bruxvoort, PhD, MPH, is an assistant professor of epidemiology at the University of Alabama at Birmingham. Dr. Bruxvoort conceptualized the study, led data collection, and reviewed the final version of the manuscript for intellectual content.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.