
Abstract
Background:
U.S. meat and poultry processing workers experienced a disproportionate burden of COVID-19 illness following the declaration of the COVID-19 pandemic. Managing prevention and surveillance activities for COVID-19 prevention required additional work for occupational health nurses. The purpose of this project was to conduct a cost analysis for two staffing options to address the increased workload for occupational health nurses.
Methods:
An economic quality improvement design was used for this study. The project was performed at a meat and poultry processing plant with 1,800 employees and six occupational health nurses. Two staffing options were considered. Option 1 was to continue to pay current occupational health nurses overtime, and Option 2 was to hire a COVID-dedicated nurse to manage the increased workload. A cost analysis was conducted for wages per hour plus benefits at three time points: 3 months, 1 year, and 3 years.
Findings:
Costs for Option 1 (continuing overtime) at 3 months, 1 year, and 3 years were estimated at US$27,370, US$109,517, and US$328,550, respectively. Costs for Option 2 (hiring a COVID-dedicated nurse) at 3 months, 1 year, and 3 years were estimated at US$44,279, US$94,979, and US$230,179, respectively.
Conclusions/Application to Practice:
Hiring a dedicated COVID nurse would save the processing plant extensive salary costs by Year 3. Reducing overtime had the potential to decrease the COVID-19-related workload and potential experiences of fatigue and burnout in occupational health nurses.
Background
In March 2020, the Director-General of the World Health Organization (WHO) declared the spread of coronavirus disease (COVID-19) a global pandemic (WHO, 2020). While the pandemic led to stay-at-home orders in many states in the United States, some businesses remained open due to their critical mission for continuing the U.S. food supply chain. The U.S. Department of Homeland Security (2020) listed food and agricultural workers, specifically food manufacturer workers in processing plants, as essential critical infrastructure workers.
During the early period of the COVID-19 pandemic (April 1, 2020-July 31, 2020), Herstein et al. (2021) studied COVID-19 spread and safety practices used by Nebraska meat and poultry processing plants during this 4-month period. They identified 5,002 confirmed cases of COVID-19, which accounted for 19% of the Nebraska meat and poultry processing workforce. Of the workforce testing positive for COVID-19, the majority were symptomatic (85%, n = 4,237) and self-identified as Hispanic or Latino (67%, n = 3,343). At the time of their study, the use of masks and physical barriers between employees and in common areas such as breakrooms was inconsistent. Waltenburg et al. (2021) found similar results when examining data provided by 31 states for meat and poultry processing workers. By May 31, 2020, there were 28,364 (15.2%) of 186,011 meat and poultry processing workers with a confirmed COVID-19 diagnosis; the majority (83.2%, n = 4,957) were symptomatic. The percentage of meat and poultry processing workers diagnosed with COVID-19 was significantly higher, and the rate of COVID-19 mortality was generally higher than the U.S. population as of April 26, 2000 (Asher et al., 2021). Asher et al. (2021) posited that the higher burden of COVID-19 in this population was likely due to the close proximity these workers conduct their work as well as a lack of COVID-19 safety guidelines before April 26, 2000. These early findings demonstrated the importance of screening all workers for fever and other COVID-related symptoms prior to entry into the plant to prevent the spread of COVID-19 among this workforce (U.S. Centers for Disease Control and Prevention [U.S. CDC], 2020b).
A common challenge for COVID-19 prevention is reducing workers’ exposures before coming to work (Rubenstein et al., 2020). For example, Rubenstein et al. (2020) reported that workers could be potentially exposed in nonwork settings, such as grocery stores (73.8%), gas stations (52.4%), laundromats (19.5%), and liquor stores (14.2%). Another potential source of infection occurs during carpooling to the processing plant with nonfamilial coworkers. In May 2020, Rubenstein et al. (2020) queried poultry processing workers on wearing a mask when carpooling. While approximately 71% of U.S.-born and 93% of foreign-born poultry processing workers reported wearing a mask while carpooling, there was still a portion of workers, particularly those who were U.S.-born who did not. In addition, the actual use of mask-wearing may be less than reported because respondents in the study were selected by plant management, and the consistency of mask-wearing was not reported. Carpooling posed a unique risk to workers because their chance of infecting one another increased as well as the spread to their respective families and social networks. An important consideration for occupational health is to query employees with fever or other COVID-19 symptoms about their commuting practices and the need to conduct contact tracing to quarantine coworkers who carpool with them.
The U.S. CDC (2020a, 2020b), Herstein et al. (2021), and the U.S. Occupational Safety and Health Administration (U.S. OSHA, 2020) provided recommendations to prevent COVID-19. General recommendations for all employers included requesting employees to prescreen at home; screening employees prior to plant entry for fever and other COVID-related symptoms; wearing cloth masks; maintaining 6-feet of social distancing; cleaning and disinfecting workspaces, common areas, and equipment on a regular basis; minimizing the number of employees simultaneously working in the plant; increasing ventilation in rooms; and implementing stress reduction messages (Herstein et al., 2021; U.S. CDC, 2020b; U.S. OSHA, 2020). Specific recommendations for meat and poultry processing plants included adding touch-free hand sanitizer stations, adding additional clock in/out machines, staggering work shifts and break times, adding shifts to reduce the number of workers per shift while maintaining overall production goals, reconfiguring workers’ positions in relation to their coworkers including spreading workers to be a minimum of 6 feet side-by-side, adding partitions between employees, and removing workers from working immediately across a conveyor belt (U.S. CDC, 2020b). When workers need to work in tandem, a partition can be installed above the belt laterally between workers to allow food movement on the belt while reducing the spread of COVID-19 between coworkers across the belt (U.S. CDC, 2020b). The use of personal fans can be reduced to prevent COVID-19 infection between workers. Herstein et al. (2021) noted that after full implementation of mask usage and physical barriers in Nebraska meat and poultry processing plants, infection rates decreased in the majority of their study sites.
The responsibility for implementing COVID-19 safety precautions is the responsibility of the occupational safety and health team, including occupational health nurses. As the workload of occupational health nurses increases, they are more likely to experience exhaustion, fatigue, and burnout (Benfante et al., 2020; Schlak et al., 2021; Sriharan et al., 2021; U.S. OSHA, n.d.). As plants extended their operating hours to stagger shifts and add shifts per U.S. CDC (2020b) recommendations, occupational health nurses needed to increase their shift hours through overtime to lead COVID-19 prevention efforts. Overtime is the number of hours worked after having already worked 40 hours in a single week (U.S. Department of Labor, n.d.). The increased hours spent working in a stressful environment coupled with fatigue can lead to nurses making errors in patient care or harming another person unintentionally (Caruso, 2014; Caruso et al., 2017; Committee on the Work Environment for Nurses and Patient Safety et al., 2004; Keller, 2009; Schlak et al., 2021).
The workload burden and community fear of COVID-19 can also promote symptoms of acute and chronic stress and burnout symptoms resulting from worrying about becoming infected, spreading COVID-19 to family members, and evolving work conditions and workload (Benfante et al., 2020; Sriharan et al., 2021; Zhang et al., 2020). These negative outcomes including negative general well-being, depression, anxiety, and burnout coupled with the perceived inability to control the spread of COVID-19 could negatively impact occupational health nurses’ ability to prevent work-related accidents (Garcia et al., 2019; Ünal, 2020).
For the current project, the implementation of COVID safety precautions became the responsibility of the plant’s occupational safety and health department. As the plant adopted safety practices including increased surveillance, additional shifts to reduce the number of employees in the plant at any time, and so on, the occupational health nurses needed to extend their work days resulting in overtime hours. To balance the increased expense of COVID-19 precautions and additional workload for the occupational health nurses and mitigate occupational health nurses’ reports of experiencing burnout, the occupational safety and health department manager considered two options. Option 1 was to continue paying overtime to the existing six occupational health nurses until the work conditions returned to a pre-COVID-19 normal state. Option 2 was to hire a COVID-dedicated occupational health nurse eliminating the need for ongoing occupational health nurse overtime. The purpose of the current project was to conduct a cost analysis for these two options to address the increased workload for occupational health nurses.
Methods
This project was an economic quality improvement project. The project was conducted in a meat and poultry processing plant in the Southwestern United States, which had an occupational health department. Salary costs to manage COVID-19 were compared for six occupational health nurses employed at the time the project was conducted to salary costs for an additional COVID-dedicated occupational health nurse.
The company had approximately 1,800 employees, and the occupational safety and health department had six full-time occupational health nurses. The occupational health nurses were scheduled to work 8-hour shifts with staggered start times providing coverage 21 hours per day beginning at 6:00 a.m. and ending at 3:00 a.m. Prior to COVID-19, the occupational health nurses’ main responsibilities were assessing, evaluating, and treating injuries and illnesses of employees; assessing non-work-related emergencies; and workers’ compensation case management. Daily activities included employee education in ergonomics, drug testing policies, hearing conservation training and monitoring programs, plant hygiene requirements, blood-borne pathogen exposure, and respiratory fit testing.
In March 2020, COVID-19 surveillance and prevention became a primary and additional focus for the occupational safety and health department. The occupational health nurses were becoming overwhelmed with new and changing guidelines pertaining to the COVID-19 pandemic. To meet the new demands, the occupational health nurses increased the number of hours they worked from 40 hours per week to an average of 46.55 hours per week. The occupational health nurses spent time writing and implementing operational practices created to maintain employee safety. Safety practices included placement of plexiglass barriers between employee workstations, breakrooms, and cafeteria tables. They advised employees to wear facial coverings or masks, practice good hygiene through handwashing or using hand sanitizer with a minimum of 60% alcohol, and social distancing. The company bought sanitizers for each of the main entrances and had the entrances staffed to ensure the use and placed them strategically throughout the facility. Infrared thermometers with cameras were placed by the sanitizer stations. Stickers were placed on floors to remind employees to maintain a social distance of 6 feet.
The occupational health nurses were assigned additional responsibilities for assessing employees, answering increased calls related to COVID-19, testing for COVID-19, contacting outside resources related to COVID-19, conducting COVID-19 screening with employees before they entered the plant, distributing masks as needed, conducting weekly safety walkthroughs, mitigating COVID-19 safety concerns, and continuing to assist in the assessment of safety concerns and needs of the company. In addition, the occupational health nurses contacted employees who called off work using the COVID-19 hotline, performed COVID-19 contact tracing and testing, and answered or responded to increased phone calls.
The occupational safety and health department manager provided the project team with details on occupational health nurses’ average wage per hour, costs for benefits, and average overtime hours worked per week by occupational health nurses, and anticipated wage for a new COVID-dedicated nurse. Average wage for the six occupational health nurses was US$27.48 per hour. Costs of benefits per nurse was 30%. Benefits are additional non-wage compensation provided to employees; some benefits are considered taxable income (Internal Revenue Service, 2021). Examples of benefits are health insurance, adoption and dependent care assistance, group-term life insurance coverage, and retirement fund allocations (Internal Revenue Service, 2021). Overtime wages were calculated as one and one-half times the regular wage rate for the occupational health nurses (U.S. Department of Labor, n.d.). The anticipated wage for a new COVID-dedicated nurse was US$25 per hour based on a pay range of US$23 to US$28 per hour.
Salary expenses were calculated for three time periods (i.e., 3 months, 1 year, and 3 years) for two departmental employment options (Option 1: continue to pay current occupational health nurses overtime; Option 2: hire COVID-dedicated nurse). An end date of 3 years was selected based on the probability for a functional end of the COVID-19 pandemic in the United States (Charumilind et al., 2020). Analysis for Option 1 was based on overtime pay: wage per hour times 1.5 plus 30% costs for benefits. This statistic was multiplied by six to represent the overtime worked by six occupational health nurses. This statistic was then multiplied by 13, 52, and 156 to represent salary costs at 3 months (13 weeks), 1 year (52 weeks), and 3 years (156 weeks).
Analysis for Option 2 was based on the anticipated wage per hour for the new COVID-dedicated nurse plus 30% costs for benefits. This statistic was multiplied by 13, 52, and 156 to represent salary costs at 3 months, 1 year, and 3 years. During the first 3 months of employment for the new COVID-dedicated nurse, the current occupational health nurses would need to continue working overtime. The salary costs for the six current occupational health nurses for 3 months calculated for Option 1 were added as a one-time expense to the Option 2 salary costs for a new COVID-dedicated nurse at 3 months, 1 year, and 3 years.
Prior to implementation, this economic quality improvement project was reviewed by a member of the University’s Institutional Review Board and determined to be exempt, non-human subjects research.
Findings
A cost analysis was completed for the two staffing options (see Table 1). Option 1 was to continue having current occupational health nurses work overtime for COVID-19 management. The current occupational health nurses averaged 6.55 overtime hours per week per occupational health nurse. The average overtime wage was US$41.22 per hour (US$27.48 per hour × 1.5) plus 30% benefits. The overtime salary costs over 3 months were estimated to total US$27,379. The overtime salary costs for ongoing COVID-19 management at 1 year would total US$109,517 and at 3 years would total US$328,550.
Cost Analysis of Two Options for Managing the Increased COVID-19 Workload of Six Occupational Health Nurses at a Meat and Poultry Processing Plant
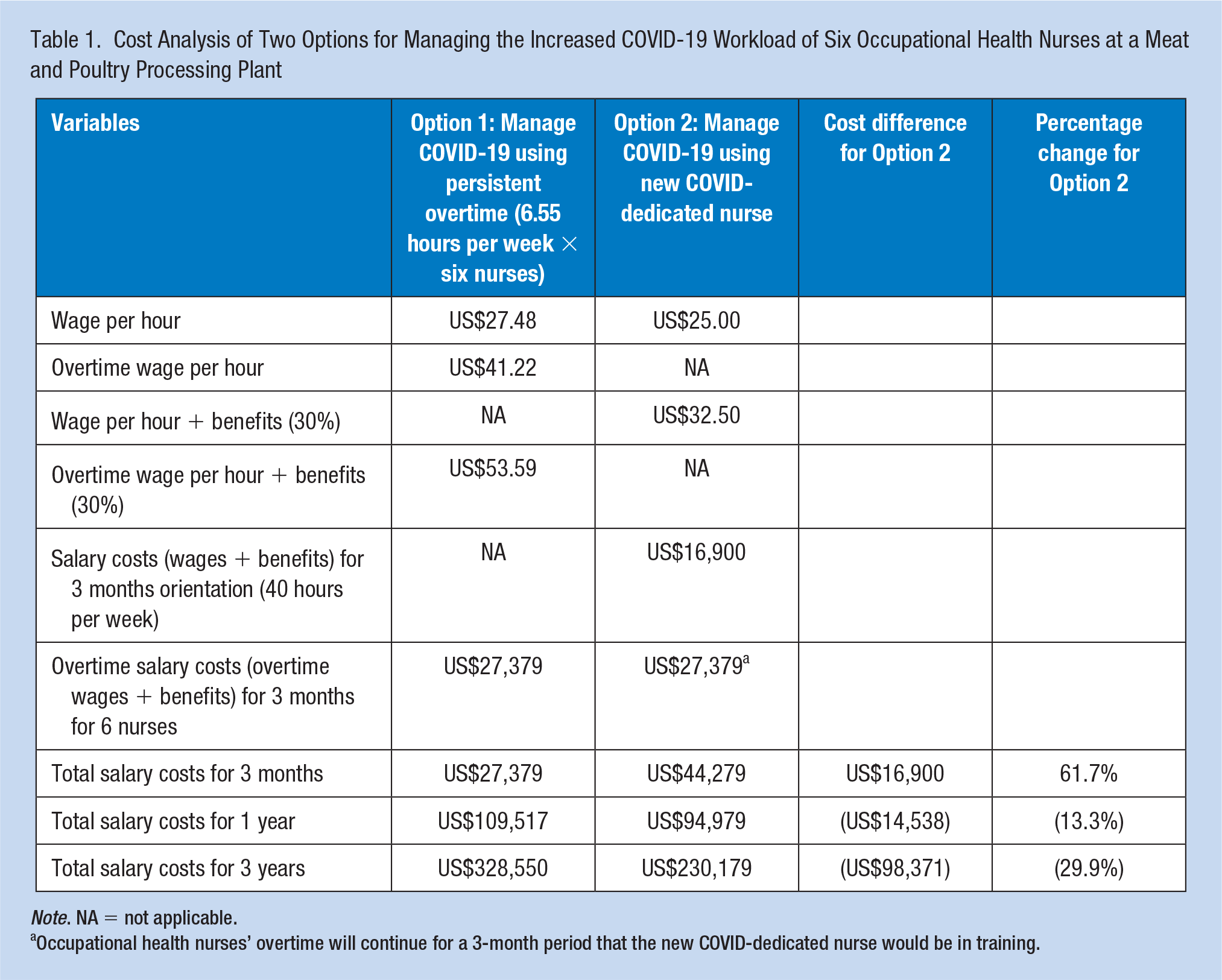
Note. NA = not applicable.
Occupational health nurses’ overtime will continue for a 3-month period that the new COVID-dedicated nurse would be in training.
Option 2 was to hire a COVID-dedicated nurse for COVID-19 management. This dedicated nurse would be hired to work 40 hours per week at an estimated US$25 per hour and be required to complete a 3-month orientation period. Salary costs (wages plus benefits) for the nurse during the 3-month orientation period would be US$16,900. Overtime salary costs of US$27,379 for the current six occupational health nurses would continue to be incurred during the 3-month orientation period resulting in total salary costs over 3 months of US$44,279. Salary costs for Option 2 at 1 year including one-time 3-month overtime salary costs during the orientation period would total US$94,979 and at 3 years would total US$230,179.
The difference in salary costs for Option 2 compared to Option 1 was US$16,900 at 3 months. At 1 year, salary costs for Option 1 were US$14,538 greater than Option 2 and at 3 years, salary costs for Option 1 were estimated to be US$98,371 greater than Option 2. By Year 1, the cost analysis indicated Option 2 with a COVID-dedicated nurse would be more cost-effective than continuing the current practice of paying overtime to six occupational health nurses on a long-term basis.
Discussion
Based on the cost analysis, hiring a COVID-dedicated nurse was a more economically feasible option. While the expenses for a new nurse were greater at 3 months compared to current occupational health nurses working nearly 7 hours overtime every week, the expense for a new COVID-dedicated nurse at 1 year was lower and by 3 years was considerably lower compared to persistent overtime. An additional consideration not explored in the cost analysis was whether the new occupational health nurse would be needed after 3 years when COVID-19 would presumably no longer be impacting the safety and health of the processing plant workers. This option may need to consider having a 3-year contract in place when hiring the COVID-dedicated nurse.
Following the cost analysis, the department manager opted to hire a COVID-dedicated nurse. The nurse hired into this role was an experienced occupational health nurse and as a result, the salary costs for Option 2 were higher than those reported in this case. Even with a higher wage per hour, Option 2 remained an economically preferable option. Another consideration introduced by the department manager was the increased burden of training a new nurse. Training a new nurse while simultaneously managing COVID-19 would lead to additional workload and burden for current occupational health nurses.
An added value of hiring a COVID-dedicated nurse was the ability for consistent implementation of a COVID-19 management plan. Due to the high risk associated with COVID-19, a current occupational health nurse at the facility may be best situated to assume this role while the new (but experienced) nurse assumes the general occupational health nurse responsibilities, unless the new nurse has experience managing communicable emerging and re-emerging infectious diseases (e.g., Ebola virus disease, severe acute respiratory syndrome, and influenza A virus) in a comparable industry.
Given the fatigue and burnout symptoms reported for nurses working with COVID-19 patients in the literature and the self-reported burnout being experienced by the occupational health nurses in the current project, interventions were warranted for the occupational health nurses providing COVID-19 management to the processing plant workers. Zhang et al. (2020) discussed that nurses working in Wuhan, China, during the pandemic used a variety of coping activities to address stress and burnout. Coping activities used by the nurses included participating in professional development activities about COVID-19, trying to reverse any negative thoughts that COVID-19 could not be effectively managed, participating in recreational activities, and engaging in health-promoting activities, such as rest, exercise, and eating a balanced diet. Occupational health nurses may need to take more frequent rest breaks during the workday to allow time for their COVID-related ruminations to subside. These breaks can allow time to regain their personal energy and increase their focus after returning to COVID-19 management and other routine occupational health nurse activities. Baskin (2020) reported that a key aspect for COVID-19-related burnout was an imbalance between workload and resources available; resources include human resources. The department manager’s intent to hire a COVID-dedicated nurse was a proactive strategy to address the potential burnout in the occupational health nurses.
The occupational health nurses and department manager can monitor one another for warning signs of excessive stress as demonstrated by cognitive, emotional, behavioral, and/or physical changes. These changes listed by the American Psychiatric Nurses Association (n.d.) may require a purposeful assessment on a regular basis. For example, the department manager could meet monthly with each occupational health nurse to conduct a “check-in.” During this meeting, the manager may describe changes observed in the occupational health nurse or the occupational health nurse may offer self-identified changes since the onset of COVID-19. The two could mutually discuss strategies to help the occupational health nurse return to an optimal state of being. Strategies include a referral to an employee assistance program, practicing yoga, eating regularly scheduled meals, using mindfulness exercises, journaling, team-building activities, web-based stress management programs, Reiki massage, and sleeping 7 to 9 hours per night (American Psychiatric Nurses Association, n.d.; Baskin, 2000; de Oliveira et al., 2019; U.S. CDC, 2021; Zhang et al., 2020).
This project had three limitations. The first limitation was the use of a single site employer as a case study for the cost analysis. The occupational health department in other plants may have different payroll expenses or better capacity to absorb the increased workload with minimal overtime hours. Second, the information received for the cost analysis was self-reported data from the company and based on estimations. Calculating actual overtime salary costs at the individual level may have yielded a smaller difference between options (e.g., overtime may have been predominantly worked by nurses earning less than the average wage per hour for current nurses, which would have resulted in lower salary costs than those reported in this case at 3 months, 1 year, and 3 years). Third, nurse burnout was not measured in this study. It was not known whether hiring a new COVID-dedicated nurse would have improved self-reports of nurse burnout or the impact that state lockdown orders may contribute to perceptions of nurse burnout.
Conclusion
Cost analysis showed a long-term economical preference for hiring a COVID-dedicated nurse in this processing plant company. This approach could be considered in other plants to manage the increased workload assigned to occupational health nurses for COVID-19 management. Additional considerations including length of time to maintain additional human resources and indirect costs related to occupational health nurse burnout, which can be incorporated into decision-making when considering staffing options. Further research is needed to determine the degree of burnout in occupational health nurses working longer shifts in processing plants. In addition, a final cost analysis can be conducted to determine actual costs and relate to them to reductions of COVID-19 infections in processing plant workers.
Applications to Professional Practice
The impact of the COVID-19 pandemic is anticipated to last for several years, and occupational health nurses will be responsible for COVID-19 prevention and surveillance activities. This increased workload can be accomplished by occupational health nurses working extended hours through overtime, which places them at risk of fatigue, burnout, and errors in care. Options such as hiring a COVID-dedicated nurse need to be considered to mitigate the increased workload on existing human resources versus the continuation of overtime for a prolonged period. As options are considered, occupational health leadership can consider salary costs inclusive of overtime, benefits, and training as well as fatigue, burnout, and general well-being of existing occupational health.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Partial funding was provided by the National Institute for Occupational Safety and Health through the University of Cincinnati Education and Research Center Grant #T42OH008432.
Author Biographies
Jennifer Naylor is an occupational health nurse and her background includes medical/surgical, acute psychiatric, correctional, and long-term care nursing. She recently completed her Master of Science in Nursing in the Occupational Health Nursing Program at the University of Cincinnati and plans to further her education.
Gordon Lee Gillespie is professor and director of the Occupational Health Nursing Program at the University of Cincinnati. His research has been funded by the Centers for Disease Control and Prevention (CDC)-National Institute for Occupational Safety and Health, Robert Wood Johnson Foundation, American Nurses Foundation, and Emergency Nurses Association Foundation. His work has been cited by the Occupational Safety and Health Administration, U.S. Government Accountability Office, American Nurses Association, and practitioners and researchers across six continents.
Cynthia Betcher is an assistant professor of clinical nursing. Her background includes serving as a hospital staff nurse, nurse case manager for injured workers, claims auditing manager, school nurse, and occupational health nurse. As faculty at the University of Cincinnati, Dr. Betcher has taught community health nursing and occupational health nursing.
C. Edward Orr is a nurse manager for Occupational Health Services in a U.S. meat and poultry processing plant.