
Abstract
Background:
Coal miners have been reported to have higher rates of risky/harmful alcohol misuse; however, it is not known if metalliferous mining employees whose working conditions differ in workplace practices, also have increased rates of risky/harmful alcohol misuse. This study aimed to examine alcohol consumption in a sample of Australian metalliferous mining workers and to examine the demographic and workplace factors associated with risky/harmful alcohol use.
Methods:
All employees from a convenience sample of four Australian mine sites were invited to complete a paper-based cross-sectional survey between June 2015 and May 2017. The survey contained questions relating to social networks, health behaviors, psychological distress, demographic characteristics, and risky/harmful drinking. Current alcohol use was measured by the Alcohol Use Disorders Identification Test (AUDIT), a validated measure of risky and/or harmful drinking. Factors associated with risky/harmful drinking were investigated using univariate and multivariable logistic regression.
Findings:
A total of 1,799 participants completed the survey (average site response rate 95%). Overall, 94.8% of males and 92.1% of females reported using alcohol in the preceding 12 months. The odds of risky/harmful alcohol use were significantly higher in those who were male, younger, and reported higher psychological distress.
Conclusions/Application to Practice:
This study identified that metalliferous mining employees engage in at-risk levels of alcohol consumption significantly higher than the national average despite workplace policies and practices that restrict alcohol use. Personal and workplace risk factors that may help target specific employee groups and inform the development of tailored, integrated multicomponent intervention strategies for the industry were identified.
Background
Worldwide, 5.3% of global deaths were attributed to alcohol use in 2018, along with a range of significant health, economic, and social burdens (World Health Organization [WHO], 2018a). The global average per capita alcohol consumption per year was approximately 6.4 liters in 2016, increased from 5.5 liters in 2005 (WHO, 2018a). According to the WHO (WHO, 2018a, 2018b), a reduction in alcohol intake is one of the most effective strategies in noncommunicable disease prevention and control within populations.
Younger, single men are more likely to consume harmful levels of alcohol, be dependent on alcohol, and to suffer from alcohol-attributable diseases and death (Australian Institute of Health and Welfare, 2017; WHO, 2018a). Male-dominated industries such as mining, construction, manufacturing, and agriculture are particularly susceptible to the ill effects of harmful alcohol use by employees (Roche et al., 2015). These industries suffer adverse economic impact related to high absenteeism and presenteeism (Yu et al., 2015), as well as impacts on workplace safety and increased work-related accidents and injury (Cheng et al., 2015).
In Australia, the majority of resource sector employers (commodities including iron ore, coal, natural gas, gold, aluminum, and petroleum) have a zero-tolerance policy on alcohol and other drugs in the workplace (Australian Mines and Metals Association, 2016). Many employers use strategies to detect current alcohol levels, such as mandatory preshift alcohol breath testing as well as random testing for illicit substances (Australian Mines and Metals Association, 2016). While this may prevent employees from working under the acute influence of alcohol, it will not mitigate the chronic negative health effects of harmful alcohol use such as stroke, heart, and liver disease, heightened risk of suicide as well as poorer performance at work (e.g., through fatigue, mood, impact on cognitive performance, and sleep) (Department of Health, 2020; Kenney et al., 2013).
Factors inherent to resource sector workplaces (i.e., mining) may themselves be associated with harmful alcohol use. Long working hours (Virtanen et al., 2015), shift work and working under fly-in fly-out (FIFO) or drive-in drive-out (DIDO) conditions (a practice adopted by more remote, geographically isolated mines, requiring employees to travel considerable distances to the worksite, and to reside in temporary accommodation between shifts and the conclusion of the block of shifts) may compound harmful alcohol use (Rebar et al., 2018). In a study by Tynan et al., (2017) which investigated alcohol consumption in the Australian coal mining industry, findings showed that almost half of male, and almost a fifth of female employees consumed alcohol at levels considered risky or harmful. Problem drinking was significantly more likely in miners who were younger, male, as well as those who reported higher levels of psychological distress, illicit drug use, smoking, and personal financial factors (Tynan et al., 2017). The investigation of associated factors, both individual and workplace, which contribute to alcohol misuse, is important for understanding specific and distinct industry needs and identification of modifiable risk factors (Tynan et al., 2017). This information is vital for guiding the development of tailored workplace policy and practices that can support prevention and intervention initiatives (Khanal et al., 2016).
Metalliferous mining, as defined by the Australian Industry and Skills Committee (2019), includes both mining of surface and underground iron ore, copper, tin, nickel, gold, silver, and zinc as well as gemstone, uranium, and mineral sands. Metalliferous mining in Australia is dominated by FIFO and DIDO workforces (House of Representatives Standing Committee on Regional Australia, 2013), in rural and remote locations often geographically isolated from professional health services. Owing to the location of the mine sites, access to health services is limited (Australian Institute of Health and Welfare, 2019). The consequential increase in financial and time costs associated with distance have been identified as a barrier to accessing treatment for mental health concerns (Handley et al., 2014). Workers in rural and remote areas who participate in FIFO/DIDO work arrangements perceive this arrangement interferes with home, family, and social life, and many indicate feelings of loneliness and social isolation (Barclay et al., 2013; House of Representatives Standing Committee on Regional Australia, 2013). Typical work arrangements include 2-weeks working 12-hour rotating shifts followed by 1 week off. Substance misuse along with fatigue have also been identified as factors that may be associated with poorer mental health in FIFO/DIDO workers (Barclay et al., 2013; House of Representatives Standing Committee on Regional Australia, 2013).
Despite data suggesting FIFO/DIDO workers consume alcohol at levels above recommended safe guidelines, there is limited empirical evidence investigating if workplace factors are associated with risky or harmful drinking in the mining industry (Joyce et al., 2013; Rebar et al., 2018). In a recent study of coal miners, a number of workplace factors were significantly associated with problem drinking, including the type of mine (underground as opposed to open cut), the work role of the employee, as well as attitudes toward working in the coal mining industry (Tynan et al., 2017). It is unknown the extent to which these findings are translatable to metalliferous mining where there are a number of considerable differences including, but not limited to, the commodity mined, the mining techniques, and mine locations (metalliferous mines often located in more remote geographically isolated areas). The metalliferous sector employs roughly 65,000 workers, and in 2018, there were 259 operating metalliferous mines within Australia (Britt et al., 2019).
The aim of this study was to examine the extent of alcohol consumption in a sample of employees in the Australian metalliferous mining industry and to examine the associated demographic characteristics and workplace factors.
Methods
This study used a self-selected convenience sample of Australian metalliferous mining employers. We recruited mining companies through emails, meetings, and newsletters via the Minerals Council of Australia (MCA; Australia’s leading national minerals industry association). Member organizations of the MCA (n = 53) are located in all states and territories of Australia, including multiple commodity and mining types and many organizations have multiple sites (MCA, 2018). The MCA referred the interested employers (n = 4) to the research team.
The four employers who expressed interest represented different mine types (open cut vs. underground), locations across Australia (one each from the states of Western Australia, Northern Territory, South Australia, and Tasmania), and commodity type (gold, iron ore, copper, and zinc). The general managers of each site were contacted to gain consent for their mine to participate in the study. The research team worked with the health and safety managers at each site to determine the logistical arrangements for data collection.
Before data collection, promotional material (e.g., slides and posters to be displayed in crew common areas) was distributed to each site outlining details of the study to raise awareness of the project. All workers from a range of roles including managers, professionals, technician and trade workers, laborer’s, machinery operators/drivers (including contractors and subcontractors) currently working at participating mines were invited to partake. In total, 1,902 workers were invited to participate. This study was approved by the University of Newcastle Human Research Ethics Committee.
Data Collection
Data collection procedures were designed to minimize disruption to workplace productivity and to accommodate the unique and specific logistical considerations of each site. Each site took between 3 to 7 days to collect the data, which occurred between June 2015 and May 2017. Researchers attended the sites at the time of routine, daily prework meetings to deliver a brief presentation outlining the purpose of the research. Paper-based anonymous surveys were then distributed and completion implied consent. Sample population sizes were provided by mine sites as determined by the number of employees working the days when data collection was conducted, which was used to determine the survey response rate.
Measures
Risky or Harmful Drinking
Current alcohol use was measured by the 10-item Alcohol Use Disorders Identification Test (AUDIT), a widely used validated measure (Barry & Fleming, 1993) of risky and/or harmful drinking (Saunders et al., 1993). This instrument combines the measurement of the quantity and frequency of alcohol consumption (hazardous drinking), control over drinking (dependence), as well as the personal and social problems associated with alcohol use (harmful drinking) over the preceding 12 months. AUDIT scores were summed and stratified using the four categories found in the literature. The categories were, no known risk (<8), risky or hazardous (8–14), high risk or harmful (15–19); and alcohol dependence likely (>19), and assessed alcohol consumption in the past 12 months.
Demographic and Behavioral Characteristics
Demographic information included the participant’s age group (≤34, 35–44, 45–54, 55+ years), gender (male or female), relationship status (not married, married, or separated/divorces/widowed), and highest level of education achieved (<12 years; year 12, certification/diploma, trade/apprenticeship/university/higher degree). Regarding education categories, <12 indicates those who did not complete high school, year 12 for those who finished high school, and certifications and diplomas allude to individuals who obtained vocational training beyond high school.
Participants reported their current smoking status on a 4-point scale (never smoked, ex-smoker, current smoker [less than daily], and current daily smoker). In addition, illicit drug use was measured via a 5-point scale that examined the frequency of drug use (no, have never tried it, “no, not in last month,” “yes, once or twice,” “yes, once a week” and yes, daily). All substance use questions pertained to the last month.
Individual Health History
Mental health disorders diagnosed by a doctor were measured by asking participants to mark all that applied to them including, depression and/or anxiety, and drug and/or alcohol disorders. In addition, using the same format, participants were asked about diagnoses of chronic health conditions (heart attack, high blood pressure, diabetes, other heart disease, stroke, migraine, high cholesterol, cancer, and obesity). Participants were asked to rate on a 5-point scale (poor, fair, good, very good, or excellent), perception of their overall physical and mental health, relationships with others, and their ability to perform tasks. Overall satisfaction with community and life in the preceding month was also measured on a 5-point scale (not at all satisfied, somewhat, moderately, very or extremely satisfied). Individual health history questions were based of a previous survey used in a coal mining population (Kelly et al., 2016).
Psychological Distress
Psychological symptoms were measured by the Kessler Psychological Distress Scale (K10), a 10-item instrument designed to measure acute psychological distress in the past month (Kessler et al., 2002), validated for use in assessing psychological distress for an Australian population (Furukawa et al., 2003). Scores were stratified into three categories (10–15 = low,16–21 = moderate, 22–50 = high/very high).
Social Networks
The Social Network Index was used to measure the strength of social and community connectedness (Berkman & Syme, 1979). The Social Network Index assesses participation in 12 types of social relationships. These include relationships with a spouse, parents, parents-in-law, children, other close family members, close neighbors, friends, work colleagues, fellow students, fellow volunteers (e.g., charity or community work), members of groups without religious affiliations (e.g., social, recreational, or professional), and members of religious groups. One point is assigned for each type of relationship (out of 12) when respondents indicate that they communicate either in person or over the phone to someone in that relationship at least once every 2 weeks (Cohen et al., 1997). Scores were stratified into four categories (1 = low, 2–5 = medium, 6–7 = high, and 8–12 = very high).
Workplace Factors
Workplace factors measured included, employment status, current role (seven role options), years of experience in the mining industry, commute type (FIFO, DIDO residential), and length of shift (five responses ranging from less than 8 hours to more than 12 hours). Additional questions examining work schedule, rotating shift (five responses included a regular day shift to a rotating shift), and self-reported estimate of proportion of days spent at work (open-ended question concerning consecutive days at work and at home/away from work on a typical roster) were also asked. Other attitudinal characteristics were measured including job satisfaction, reasons for working in mining (a 5-point Likert-type scale ranging from strongly disagree to strongly agree assessing participants feelings toward love of working in the mines, pay, roster schedules, and financial commitments) and concern over losing job. Mental ill-health stigma was measured via a 5-point Likert-type scale ranging from strongly disagree to strongly agree, assessing participants feelings toward statements concerning people who experience mental illness would be treated differently by their friends, colleagues, and in their current workplace.
Data Analysis
Demographic characteristics and workplace factors were analyzed using descriptive statistics. AUDIT scores were separated into two categories (No Known Risk [AUDIT < 8], risky/harmful drinking [AUDIT ≥ 8]) to produce a binary outcome variable and to allow for comparison with other studies. As the AUDIT consists of three independent subscales; participants’ data were excluded if they missed more than one question from any of the three domains. For instances where one question was missed, the AUDIT domain scores were then based on averaged (or prorated) responses for the available items. For example, if it were a 3-item subscale and they answered two questions. We took the average of the two responses and multiplied by 3 (which was then rounded to nearest integer). This basic imputation was done to preserve the relative scores on the subscale, based on the answers provided.
Both univariate and multivariable logistic regression analyses were performed to estimate odds ratios (OR) and 95% confidence intervals (CI) for factors associated with risky/harmful drinking. Univariate analysis assessed the independent association of each factor with risky/harmful drinking. Factors that were significant at the .05 level in the univariate analysis were included in the multivariate stepwise logistic regression model. The first step included examining all the demographic variables. The second level included factors directly associated with the participant’s health and factors known to influence health. Specifically, this included current psychological distress and history of mental ill-health diagnoses, as well as a range of behaviors likely to affect health (e.g., smoking and illicit drug use). Each of these factors were simultaneously entered into the model, adjusting for demographic variables. In the final level, the multivariable model included workplace factors, which were also entered simultaneously and therefore adjusted by demographic and health history variables. While FIFO/DIDO/residential status were modeled as an interaction, no significant associations were found. Analyses were conducted using SAS version 9.4 (SAS Institute Inc, 2013), with the alpha level set at 0.05.
Findings
A total of 1,799 participants completed the survey (response rate = 95%). Of these, 65 participants had missing data and were excluded resulting in a final sample of 1,734. These participants were employed in one of four metalliferous mines (gold, iron ore, copper, and zinc) across Australia, one each from the states of Western Australia, Northern Territory, South Australia, and Tasmania. The mines varied in size with 254 participants, 289 participants, 578 participants, and 678 participants, respectively (data not shown).
Participants were more likely to be male (87.9%), less than 35 years of age (43.2%), married or in a de facto relationship (69.3%). Almost half of the participants reported having no dependent children (49.3%) (data not shown). Nearly half (49.5%) had no known risk alcohol use as measured by the AUDIT, followed by risky or hazardous (35.8%), high risk or harmful (7.8%), and high risk, dependence likely (6.9%) (data not shown).
Overall, 94.8% of males and 92.1% of females reported that they consumed alcohol in the preceding 12 months (data not shown). Almost a third of both males (29.8%) and females (30.7%) reported consuming alcohol at least 2 to 3 times per week (data not shown). Being female was associated with lower odds of risky/harmful drinking (adjusted odds ratio [AOR] = 0.37 [95% CI = 0.26, 0.53]), with men almost three times more likely to engage in risky/harmful drinking than females. Being in a married or de facto relationship was also associated with lower odds of risky/harmful alcohol use compared to being not married AOR = 0.68 [95% CI = 0.52, 0.89]. Increasing age was associated with lower odds of risky/harmful drinking (35–44 years: AOR =0.51 [95% CI = 0.40, 0.66]; 45–54 years: AOR = 0.33 [95% CI = 0.25, 0.44]; 55+ years: AOR = 0.20 [95% CI = 0.13, 0.30]). However, there was a significant gender difference in the proportion of participants who reported risky/harmful drinking behavior (i.e., AUDIT score ≥ 8), with males (52.8%) significantly more likely to report risky drinking behavior, compared to female (31.9%) participants (Table 1).
Demographic Factors Associated With the Proportion of Respondents Who Are in the Harmful/Risky AUDIT Score Group
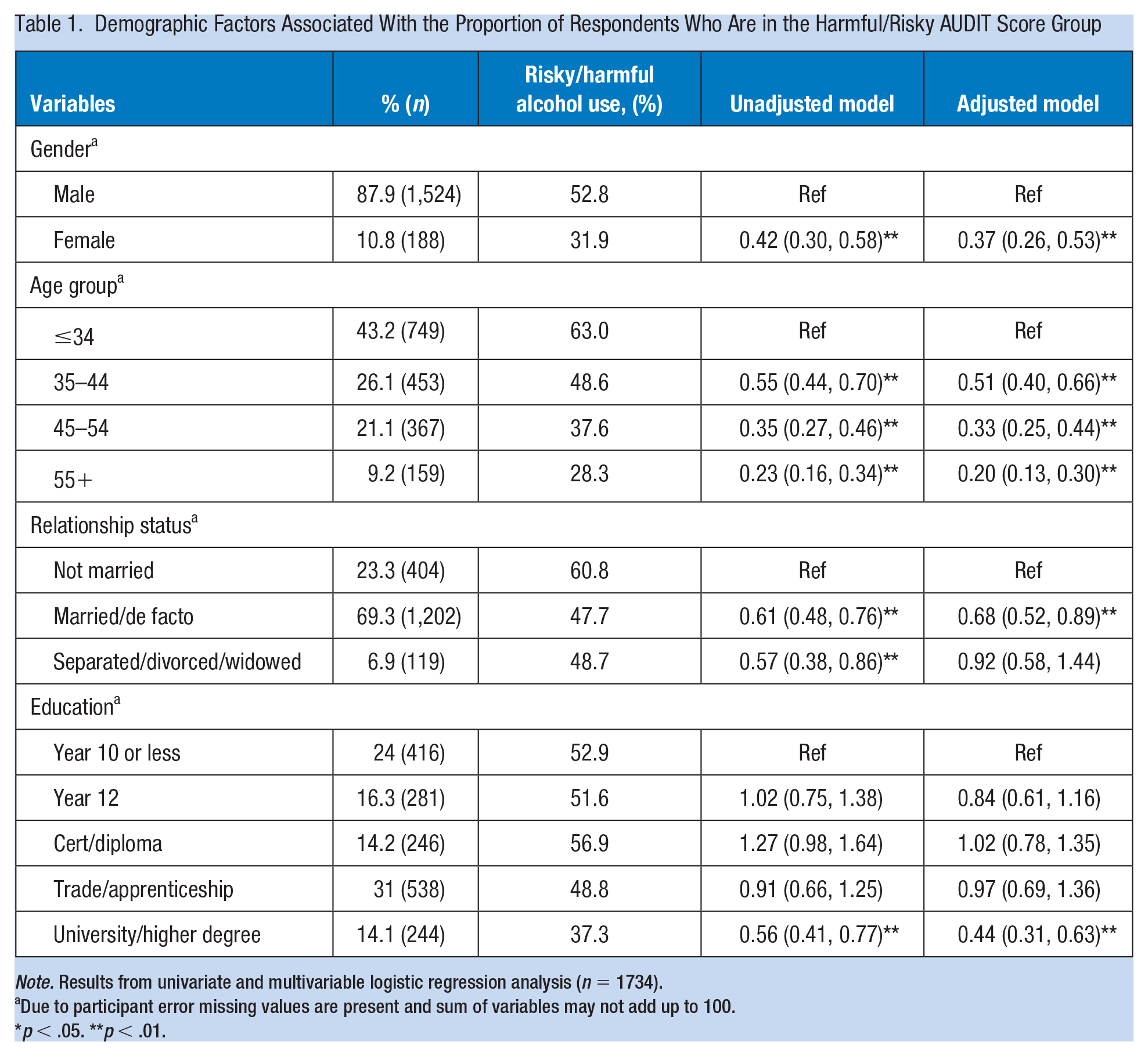
Note. Results from univariate and multivariable logistic regression analysis (n = 1734).
Due to participant error missing values are present and sum of variables may not add up to 100.
p < .05. **p < .01.
A previous history of depression and/or anxiety (AOR = 1.36 [95% CI = 1.01, 1.82]), or of drug/alcohol problems (AOR = 3.56 [95% CI = 1.68, 7.52]) were all associated with increased odds of risky/harmful drinking (Table 2). Being a daily smoker (AOR = 2.03 [95% CI = 1.55, 2.67]), using marijuana in the past month (AOR = 2.19 [95% CI = 1.18, 4.07]) and use of illicit drugs in the last month (AOR = 5.31 [95% CI = 1.71, 8.32]) were all associated with increased odds of risky/harmful drinking. Moderate (AOR = 1.44 [95% CI = 1.12, 1.84]) and high/very high level of psychological distress (AOR = 1.41 [95% CI = 1.04, 1.93]) were both associated with increased odds of risky/harmful drinking compared to a low level of recent psychological distress. Social network score was not significantly associated with increased odds of risky/harmful drinking, Low (Ref), Medium (AOR = 1.00 [95% CI = 0.77, 1.29]), Medium High (AOR = 1.23, [95% CI = 0.88, 1.73]), High (AOR = 0.82 [95% CI = 0.53, 1.27]; data not shown).
Health and Social Factors Associated With the Proportion of Respondents Who Are in the Harmful/Risky AUDIT Score Group—Results From Univariate and Multivariable Logistic Regression Analysis (n = 1,734)
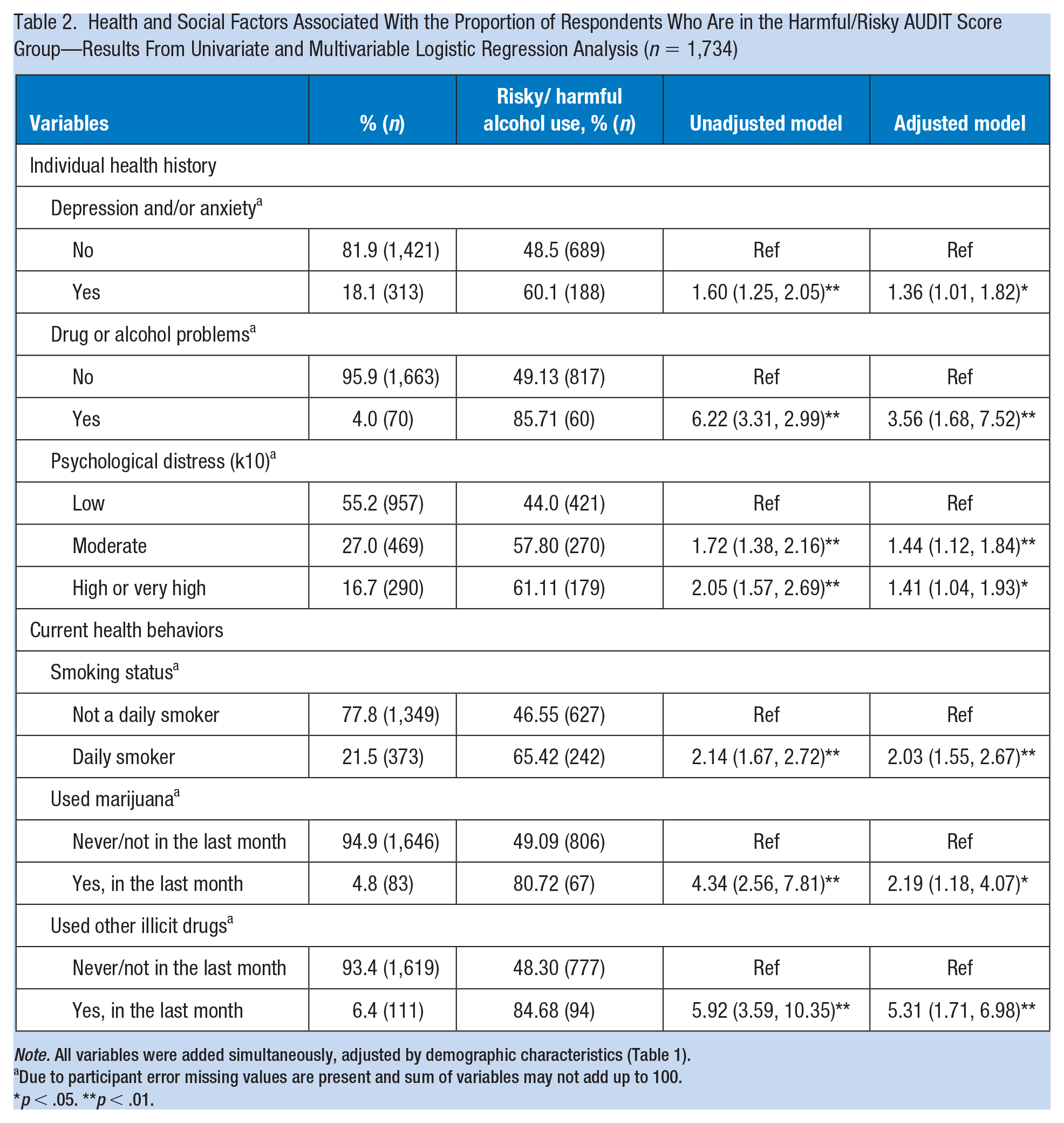
Note. All variables were added simultaneously, adjusted by demographic characteristics (Table 1).
Due to participant error missing values are present and sum of variables may not add up to 100.
p < .05. **p < .01.
Most participants reported a trade or apprenticeship as their highest level of education (31.0%); worked FIFO (85.3%) and on a rotating shift (61.9%), with the most common shift length of 12 hours or less (62.1%). Participants were also more likely to work in a machinery operator/driver or laborer role (45.0%) with a work tenure in mining between 3 and 10 years (49.1%).
Participants who had a positive view of the roster (AOR = 1.39 [95% CI = 1.06, 1.82]) was associated with higher odds of risky/harmful drinking (Table 3).
Workplace Factors Associated With Participants’ Total AUDIT Scores—Results From Univariate and Multivariable Logistic Regression Analysis (n = 1,734)
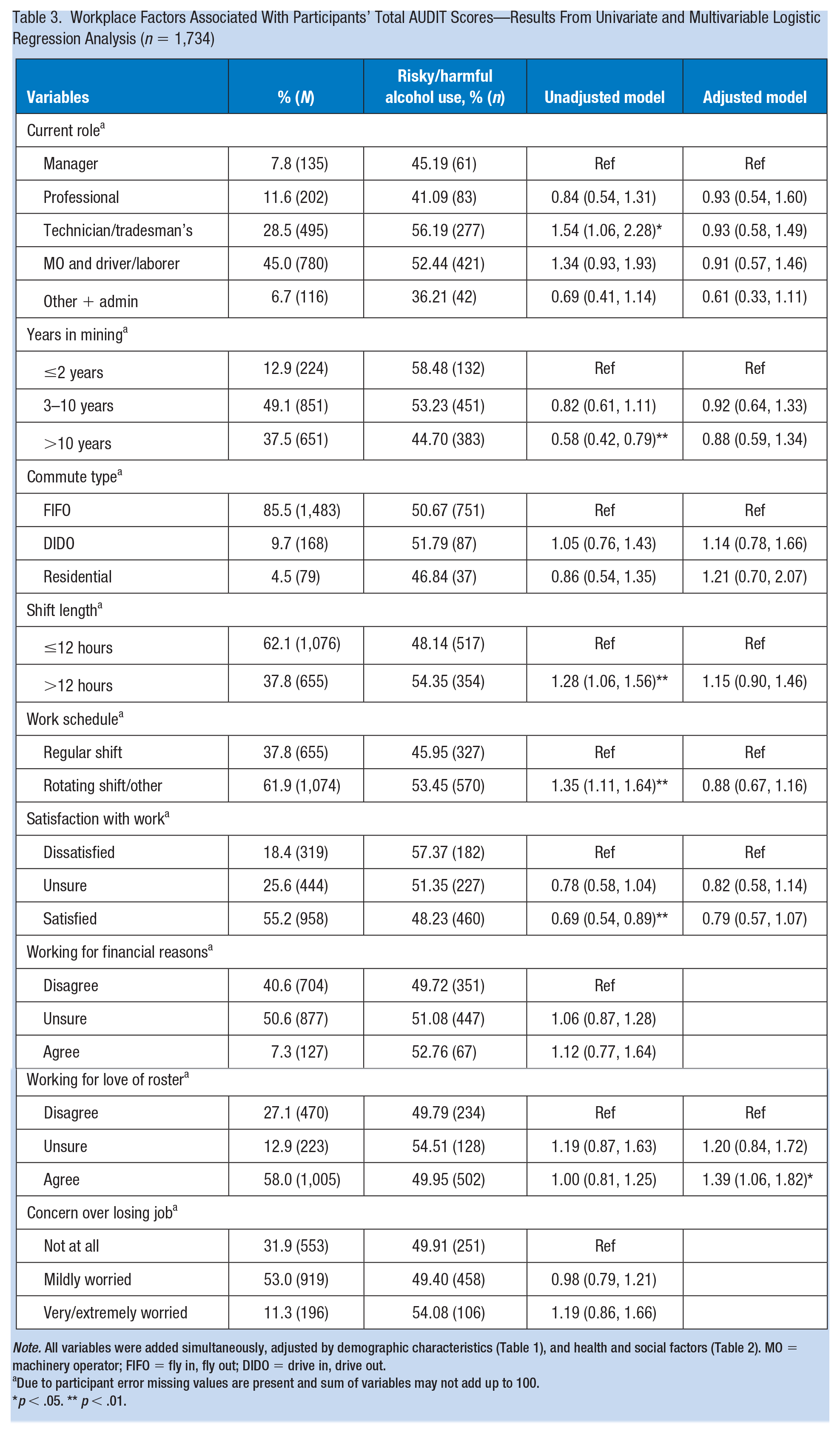
Note. All variables were added simultaneously, adjusted by demographic characteristics (Table 1), and health and social factors (Table 2). MO = machinery operator; FIFO = fly in, fly out; DIDO = drive in, drive out.
Due to participant error missing values are present and sum of variables may not add up to 100.
p < .05. ** p < .01.
Discussion
This study investigated alcohol use by employees of the metalliferous mining industry, and the associated demographic, health, psychological, social, and workplace characteristics.
There is heavy alcohol use in this industry, overall levels of drinking in this mining sample were high with 94.8% of males and 92.1% of females reporting that they had consumed alcohol within the preceding 12 months, compared to 77% of the adult Australian population, and only 38.2% of people worldwide (Australian Institute of Health and Welfare, 2017; WHO, 2018a). Reported use of alcohol at levels considered risky or harmful (i.e., AUDIT > 8), was concerning in males (2.8%) and females (31.9%) because it was much higher than the Australian community population (Australian Institute of Health and Welfare, 2017; Saunders et al., 1993). Similar to other research, there was also a significant association between alcohol use, age, and gender, with both male and younger participants significantly more likely to score higher on the AUDIT (Australian Institute of Health and Welfare, 2017; WHO, 2018a). Mining specific comparisons is limited, studies which have examined this factor have consistently shown alcohol use in the mining industry higher than the general public (Tynan et al., 2017).
The very high proportion of mine employees drinking at risky/harmful levels in this study suggest that the mining industry may benefit from industry specific, tailored health promotion, and intervention programs focusing on harmful levels of alcohol consumption. The WHO recommends that when an employee’s AUDIT scores is between 8 and 15 the most appropriate intervention is simple advice focused on the reduction of hazardous drinking; those with scores between 16 and 19 should receive simple advice plus brief counseling and continued monitoring; those with scores of greater than 20 warrant further diagnostic evaluation for alcohol dependence (Babor et al., 2001). In our sample, 36% of men and 27% of women were identified as having audit scores below 15 and therefore fit into the WHO category that suggests they would benefit from simple advice about hazardous drinking. For example, in Australia, the “Health e-Mines” initiative provides an online portal for information and support for people with mental health and substance use problems (Tynan et al., 2019) which is appropriate for employees whose AUDIT scores are between 8 and 15 but would not be sufficient for those whose scores are above 15. The Health E-Mines online portal would need to be augmented with brief counseling and continued monitoring for those with higher levels of alcohol consumption (Lee et al., 2014).
Demographic and Health Characteristics Associated With Risky or Harmful Drinking
Higher AUDIT scores were significantly associated with higher psychological distress. The link between alcohol usage and mental health is well known (Hay et al., 2017; Rehm & Probst, 2018); however, given the cross-sectional study design, it is unknown whether risky or hazardous alcohol use was associated with a deterioration in health and a corresponding increase in psychological distress, or psychological distress was high, and alcohol was used as self-medication. The Australian mining industry has previously given consideration to the issue of mental health with the development of the Blueprint for Mental Health and Mining (Kelly et al., 2015), with higher levels of psychological distress identified in the coal mining industry, and subsequent strategies to address mental health based on the Mates in Construction program (Considine et al., 2017; Kelly et al., 2016). Our study provided evidence that metalliferous mining sector would also benefit from similar industry tailored and relevant mental health programs.
Social Network Factors
Surprisingly, in our study Social Network scores did not show significant association with alcohol consumption. Despite the nature of FIFO work resulting in participants often being displaced from family and social support networks, many participants scored medium to high on the Social Network Index. This may be linked to availability of virtual methods to stay connected to family and friends (Clark et al., 2017). Further investigation of the specific nature of social supports for FIFO workers is necessary, to explore the impact of displacement from family and usual social networks on related friendships and work-related social supports. In addition, further investigation into identifying the potential contribution of specific social network components on alcohol use would be warranted.
Workplace Factors Associated With Risky or Harmful Drinking
Worker perception of mine commitment to mental health has previously been associated with lower odds of risky or harmful drinking in mining which suggests the beneficial impacts of addressing workplace mental health within the mining industry in Australia (Gullestrup et al., 2011; Kelly et al., 2015, 2016). Another workplace factor associated with lower odds of risky or harmful drinking in this study, although being more individually focused, was being satisfied with work, which may be linked to the culture of the workplace and work environment (Belias & Koustelios, 2014). Despite these positive findings, worker role (technicians); length of time in the industry (worked in mining for 10 years or more); and those with a university degree were more likely to engage in risky or harmful drinking as noted in the unadjusted model (however, these findings were not significant in the adjusted model). In addition, those working rotating shifts and shifts of greater than 12 hours were more likely to engage in harmful drinking. This could be linked to the work schedule where miners work for blocks of time and then have blocks of time off work when they can go home. It maybe that alcohol is more available at home where there are also no concerns related to the mandatory preshift breath test for alcohol, and random testing for illicit substances employed at most mine sites (Australian Mines and Metals Association, 2016). Interestingly, commute type was not associated with risky or harmful drinking. When considering the link of psychological distress and alcohol use, this is in contrast with previous research that links FIFO status with increased psychological distress (Torkington et al., 2011).
This study adds to the evidence of alcohol use in the mining industry with high rates of harmful and risky alcohol use concerning. This is despite robust health and safety policies, procedures, and processes within the mining industry in relation to the detection of alcohol and drug use at the mine site. Australia has a drinking culture particularly within male-dominated environments, and miners are known to drink on their way home from work. Alongside this, employees within mining are highly paid and have the means and ready access to alcohol when not at the worksite. The known relationship between mental health and alcohol and the significant association of higher alcohol use and higher psychological distress in our study support consideration of both mental health and alcohol use as part of a holistic approach to workplace health within the mining industry. Despite good occupational health and safety policies, the workplace could focus upon increasing employees’ awareness of the risk associated with hazardous levels of alcohol consumption and the longer-term health impacts to increase knowledge and understanding within this population. Alcohol and drug use is a sensitive issue; however, it is important that this is routinely considered within workplace health and safety education and as part of occupational health service provision to allow appropriate advice and support to be provided to this population. It is also important to be cognizant of the social networks and health services available at the location of the mine or the home to support individual employees with change.
The known relationship between mental health and alcohol and the significant association of higher alcohol use and higher psychological distress in our study support consideration of both mental health and alcohol use as part of a holistic approach to workplace health within the mining industry. The complex interplay between personal, social, and workplace factors that contribute to alcohol use need consideration for effective strategies to be implemented both within and external to the workplace for overall improvements in worker health.
This study provides evidence of the prevalence of risky or harmful alcohol use in the metalliferous mining industry in Australia. It used a cross-sectional survey design thus causal associations were unable to be determined. The time span from the first site’s data collection in June 2015 to the last site’s in May 2017 should also be acknowledged. The minerals industry in Australia during this period was evolving in terms of production due to economic influences, and this could have potentially negatively affect participant scores. This study did not explore how unionization of miners could implicate participant scores; however, it should be noted that unions are noncompulsory, and this may be an area of examination for future research. Potential bias in the recruitment of sites (self-selected convenience sample) should also be acknowledged. Possible bias due to self-report is acknowledged, particularly given that usage of illicit substances and alcohol at hazardous levels is a sensitive social issue, although, the findings suggest this bias was not present. Accessibility to alcohol on predominately FIFO mine sites was not measured; the difference between alcohol use while at a worksite compared to at home was not measured; and neither was any workplace alcohol-related culture which are areas that would benefit from future investigation and research.
Implications for Occupational Health Practice
The findings of this study provide a platform of new evidence on which to develop future initiatives aimed at preventing harmful alcohol and other drug use in the mining industry.
For example, using the AUDIT tool, and WHO criteria for action, occupational health nurses can integrate alcohol screening into existing onsite health service. In addition, they can offer simple advice focused on reduction of hazardous drinking, simple advice plus brief counseling and monitoring, and diagnostic evaluation for alcohol dependence (Babor et al., 2001; Campbell & Burns, 2015). This alongside other health and wellness interventions and health promotion strategies allows for a holistic approach to workplace wellness through improvements to overall health and well-being of employees. Increased employee wellness has been linked to decreased absenteeism and increased workers productivity (Baicker et al., 2010; Pereira et al., 2015).
Finally, decreasing levels of risky/harmful alcohol consumption may improve employee mental health and psychological distress. Our findings are suggestive that occupation health policy and procedures would benefit from a coordinated approach to address both mental health and alcohol use. Mining is recognized as having strong policies and procedures to attempt to minimize the impact of alcohol on the workplace, with preshift compulsory alcohol testing and a mandated 0.00 mg/100 mL blood alcohol concentration. Nevertheless, a focus on the broader impacts of harmful alcohol use beyond the workplace is recommended to assist employees address the physical and mental health implications of harmful alcohol use. This may be within organizations themselves through the occupational health facilities provided at a site or organizational level or through industry bodies and leaders more broadly.
Applying Research to Occupational Health Practice
Findings suggest that mine employees engage in drinking outside of work that puts them in the ‘risky or hazardous category’ of alcohol use. This may have a negative influence on mental and physical health and on workplace health and safety. Occupational health nurses can integrate alcohol screening into existing on-site health service. In addition, they can offer simple advice focused on reduction of hazardous drinking, simple advice plus brief counseling and monitoring, and diagnostic evaluation for alcohol dependence. This alongside other health and wellness interventions and health promotion strategies allows for a holistic approach to workplace wellness through improvements to overall health and well-being of employees. The Alcohol Use Disorders Identification Test (AUDIT): guidelines for use in primary health care is available at the following link: https://www.who.int/publications/i/item/audit-the-alcohol-use-disorders-identification-test-guidelines-for-use-in-primary-health-care
Footnotes
Acknowledgements
The authors would like to thank the Minerals Council of Australia and mine sites for supporting this research, and the mine employees who willingly participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this work was received from the Minerals Council of Australia (grant no. G1401530).
Author Biographies
Carole L. James is acting Head of School, School of Health Sciences, at the University of Newcastle. A/Prof James’s research centers on work; people’s engagement with, or lack of engagement with the occupation of work. A/Prof James has lead research in a variety of areas, including: investigating musculoskeletal injuries and prevention in the workplace; functional capacity evaluations; obesity; and mental health with a focus on understanding the scope of these issues in the workplace and investigating sustainable interventions to promote improved health for workers.
Ross J. Tynan is a researcher in the Mental Health—Research, Evaluation, Analysis and Dissemination (MH-READ) team as part of Hunter New England Mental Health (HNEMH), and a conjoint lecturer with the School of Medicine and Public Health at the University of Newcastle. Dr Tynan has lead research in a variety of areas, with a particular focus on research to better understand the extent of mental health problems in the workplace, identification of factors that are associated, as well as the development and evaluation of tailored online tools to promote mental health and prevent mental ill-health.
Aaron T. Bezzina is a PhD candidate at the University of Newcastle, as well as an Accredited Practicing Dietitian (APD). His research focuses on the complex issue of overweight and obesity within the Australian mining industry. His other research interests include workplace wellness interventions, obesity, human factors, and an array of occupational health and safety issues within heavy based male-dominated industries and the workplace more broadly.
Md Mijanur Rahman is a research fellow (applied statistics) at the Australian Health Service Research Development, University of Wollongong. He is also an Associate Professor (on leave) of Statistics at Comilla University, Bangladesh. He has over 10 years’ experience in teaching statistical courses to undergraduate and graduate-level students. His research interests include modeling trajectories of health and aged care service use across later life, determinants of healthy aging and health life expectancy, mental health and health service outcomes and policy evaluation.
Brian J. Kelly is Head of School, School of Medicine and Public Health, at the University of Newcastle. He is also a Clinical Academic, Consultation-Liaison Psychiatrist at John Hunter Hospital. Professor Kelly has conducted significant mental health–related workplace interventions and research in primary industries, including coal mining, playing a key role in informing mental health policy. His work in population mental health has yielded international collaborations in South East Asia addressing workplace mental health and impacts of environmental adversity.