
Abstract
Background:
Exposure to traumatic events is an occupational hazard with potential adverse psychological consequences. Previous research has focused mainly on urban practice settings; therefore, this study explored the distressing experiences encountered by rural/remote nurses and their perception of organizational support.
Methods:
Thematic analyses were conducted on open-ended data from a pan-Canadian survey of 3,822 regulated nurses, where 1,222 nurses (32%) reported experiencing an extremely distressing health care incident within the past 2 years. Among the respondents, 804 nurses (65%) reported that they did not receive psychological support from the organizations leadership following incidents.
Findings:
Three main themes regarding distressing events were: (a) involvement in profound events of death/dying, traumatic injury and loss, (b) experiencing or witnessing severe violence and/or aggression, and (c) failure to rescue or protect patients/clients. Three themes were identified regarding perceptions of organizational support including: (a) feeling well supported in the work setting with debriefing and reliance on informal peer support, (b) lack of acknowledgement and support from leaders on the nature and impact of distressing events, and (c) barriers influencing access to adequate mental health services in rural/remote settings.
Conclusion/Application to Practice:
Findings suggest that rural/remote nurses rely on informal, peer supports; there is a lack of organizational understanding of the potential risks to their psychosocial health and safety. They require more accessible, structured, appropriate, and timely supports within these settings. Increased understanding of the psychological hazards will assist organizations to establish workplace policies and practices designed to protect and support rural/remote nurses.
Keywords
Background
Rural and remote nursing is considered a high-risk occupation (Winters, 2013) in the context of isolated practice settings and limited access to advanced care services (Kulig et al., 2015; Stewart et al., 2005). Due to higher rates of injury and mortality in these settings (Canadian Institute for Health Information, 2011), rural and remote nurses may be at greater risk for exposure to distressing events than their urban counterparts (Gomez et al., 2010). Exposure to such events may alter the nurses’ sense of safety (Council of Remote Area Nurses of Australia, 2017; Opie et al., 2010a), leaving them feeling vulnerable, anxious, and unsafe (Terry et al., 2015). Although exposure to distressing events in rural and remote settings may be viewed as an unavoidable occupational hazard, there are significant concerns regarding the impact on nurses’ psychological well-being (Opie et al., 2010b). Distressing incidents can be overwhelming and challenge nurses’ ability to cope (Caine & Ter-Bagdasarian, 2003). Rural and remote nurses’ experience of distressing events may also be complicated in communities where their work and personal lives are intertwined (Zibrik et al., 2010).
Psychological distress (Terry et al., 2015) and compromised health and safety of nurses working in rural and remote practice settings (Rose & Glass, 2009) have long been acknowledged. Rural and remote nurses commonly deal with injury (e.g., motor vehicle accidents, agricultural and resource industry occupational injuries) and death of people personally known (Molinari & Bushy, 2011), work alone in isolated environments (Misener et al., 2008), and have limited access to trauma-response teams or advanced care services (Simons et al., 2010). Rural and remote nurses also deal with limited or the absence of on-site security or police backup when encountering aggressive or violent patients or family members (Terry et al., 2015).
Nurses who have cared for patients and have experienced a traumatic event have been shown to have a higher risk of experiencing burnout and compassion fatigue (Terry et al., 2015) with long-term outcomes, such as vicarious trauma (Lenthall et al., 2009), secondary traumatic stress (Beck, 2011), and post-traumatic stress disorder (PTSD) (Mealer & Jones, 2013). There is a lack of organizational understanding and support for nurses who are experiencing emotional distress (Kenny et al., 2007; Opie et al., 2010a), with evidence of limited responsiveness and inappropriate management practices in these situations (Law et al., 2011). Nurses have had to rely on informal peer support networks (Moszczynski & Haney, 2002), and other social supports, such as family and friends (MacPhee & Scott, 2002). There are also concerns that levels of insecurity and fear among rural nurses are increasing (Mikkola et al., 2017) and that the risk of exposure to distressing events appears to be on the rise (Peek-Asa et al., 2004). There is little research regarding the specific events of trauma/distress faced by rural and remote nurses, with a limited understanding of how these issues are dealt with in rural and remote practice settings. As such, the purpose of this study was to explore rural and remote nurses’ experiences of distressing events and their perceptions of organizational support following such events.
Method
The data for these analyses are from a pan-Canadian survey of nurses in rural and remote practice with the data collection period from April 2014 to August 2015 (Macleod et al., 2017). A research team in consultation with an advisory team of nursing leaders from across Canada developed the 27-page survey questionnaire based on an earlier survey on nursing practice in rural and remote areas (Stewart et al., 2005). The questions focused on the connections between the work setting, individual, community, nursing practice, and personal/professional well-being (Macleod et al., 2017), and nurses responded via mail or online. Rural was defined as people living in communities outside of urban centers with a population of 10,000 or more (du Plessis et al., 2001). Remote was not separately identified, although the study encompassed northern and outpost areas, so we use the term, rural and remote. Prior to data collection, ethical approval for the study was received from the University of Northern British Columbia (E2013.0320.037.00), University of Saskatchewan (13-222), University of Lethbridge (2013-047), Laurentian University, Hôpital Maisonneuve Rosemont (affiliate of the Université de Montréal) (13,046), Dalhousie University (2013-3131), Aurora College (15,426), Nunavut Research Institute (05 007 14N-M), and the Prince Edward Island Research Ethics Board. Survey distribution was organized through 29 separate provincial/territorial nursing organizations. A total of 10,072 surveys were mailed out to registered nurses (RNs), nurse practitioners (NPs), licensed practical nurses (LPNs), and registered psychiatric nurses (RPNs) employed in rural or remote practice across 10 Canadian provinces and three territories, with a response rate of 3,822 (40%) out of 9,622 eligible participants.
The current analyses of two open-ended survey questions included a subsample of nurses (n = 1,222, [32%]) who responded “yes” to a question of whether they had “experienced a health care incident that was extremely distressing to you as a nurse” in the past 2 years in their primary work community. Open-ended space was provided to specify the type of incident they experienced. The second question focused on whether nurses received “psychological support from leadership in their organization,” with 804 nurses (65%) overall, indicating that “no” they did not receive the psychological support from the leadership in their organization and 656 providing a response on whether they got the kind of support that they needed with options of “yes,” “partly,” and “no,” followed by open-ended space to explain their choice of option.
Data Analysis
The open-ended data from the two survey questions (ranging from a few words/phrases to longer paragraphs) were analyzed separately. Thematic analysis was utilized in this study, as it provided a flexible method to analyze the large datasets of open-ended cross-sectional data (Guest et al., 2012). This technique also supported the research team’s aim to identify important patterns and underlying ideas, provide understanding, and interpret the meanings surrounding rural/remote nurses’ experiences of distressing incidents. NVivo software version 10 (Bazeley & Jackson, 2013) was used to manage the open-ended raw data. The demographic data and characteristics of the sample were analyzed using descriptive statistics (frequencies, proportions, means, standard deviation) with SPSS v24 (IBM Corp., 2016).
Trustworthiness of the thematic analysis involved consideration of the criteria of credibility, confirmability, dependability, and transferability (Nowell et al., 2017). For example, records of the raw data and documentation of the analysis process were kept to establish a clear audit trail. An iterative process of investigator triangulation was also employed to improve credibility and auditability and to reduce potential bias. All members of the research team engaged with the data from both questions for a prolonged period and used a structured process of reviewing, sharing, and comparing of interpretations as the analyses progressed. Initial codes were generated based on the context, interpretation, and core meaning of each response, then labeled as words or phrases. These codes were reviewed independently by the researchers and collectively agreed upon to support credibility and confirmability. In the second phase of coding, labels with the attached data were grouped into larger, more meaningful thematic categories and relabeled as broader themes and subthemes based on the recurring patterns identified. The researchers reviewed the final themes against the data and then refined them to ensure they captured the core substance of the participants’ responses. Dependability was ensured through logical and clear documentation of the decision-making throughout this process and refinement of the final thematic categories. Thick descriptions of the final themes were also developed to encourage transferability.
Findings
Of the 3,822 nurse respondents to the survey, 1,222 (32%) had experienced a health care incident that was extremely distressing to them in the previous 2 years. The majority of the sample were female, practicing as RNs, with an average age of 47.1 (±11.2, 23–75) years (Table 1). The overall response from nurses about their health was positive, reporting both good general health (M 3.7 ± 0.9, 1–5) and good mental health (M 3.6 ± 0.9, 1–5). Half of the sample worked in acute-care settings, followed by almost 25% of the sample working in long-term care, 14% in primary care, and 13% in mental health. Around 14% of the sample worked in communities that were only accessible by plane, with the majority living and working in communities with populations of 1,000 to 9,999 people.
Sample Characteristics of Rural/Remote Nurses Who Experienced Distressing Events
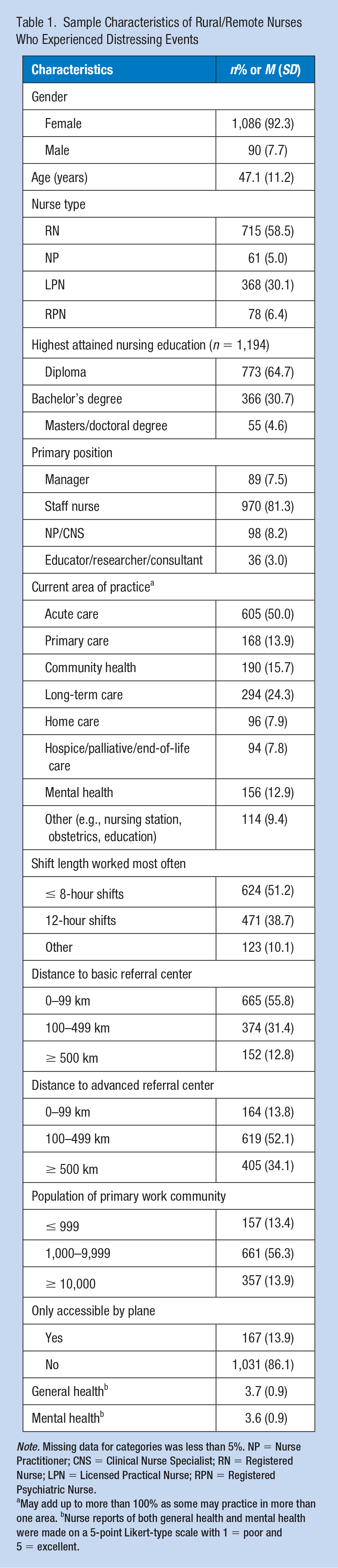
Note. Missing data for categories was less than 5%. NP = Nurse Practitioner; CNS = Clinical Nurse Specialist; RN = Registered Nurse; LPN = Licensed Practical Nurse; RPN = Registered Psychiatric Nurse.
May add up to more than 100% as some may practice in more than one area. bNurse reports of both general health and mental health were made on a 5-point Likert-type scale with 1 = poor and 5 = excellent.
Although the first survey question focused on the types of distressing events experienced, many open-ended responses included descriptions of the actual events, the surrounding context of what happened, and the emotional/mental impacts they experienced as a result. Three main themes were identified regarding rural and remote nurses’ experiences of distressing incidents: (a) involvement in profound events of death/dying, traumatic injury, and loss, (b) experiencing or witnessing severe violence and/or aggression, and (c) failure to rescue or protect patients or clients. A summary of examples of distressing incidents and representative quotes are outlined in Table 2.
Main Themes Regarding Rural/Remote Nurses’ Experiences of Distressing Incidents
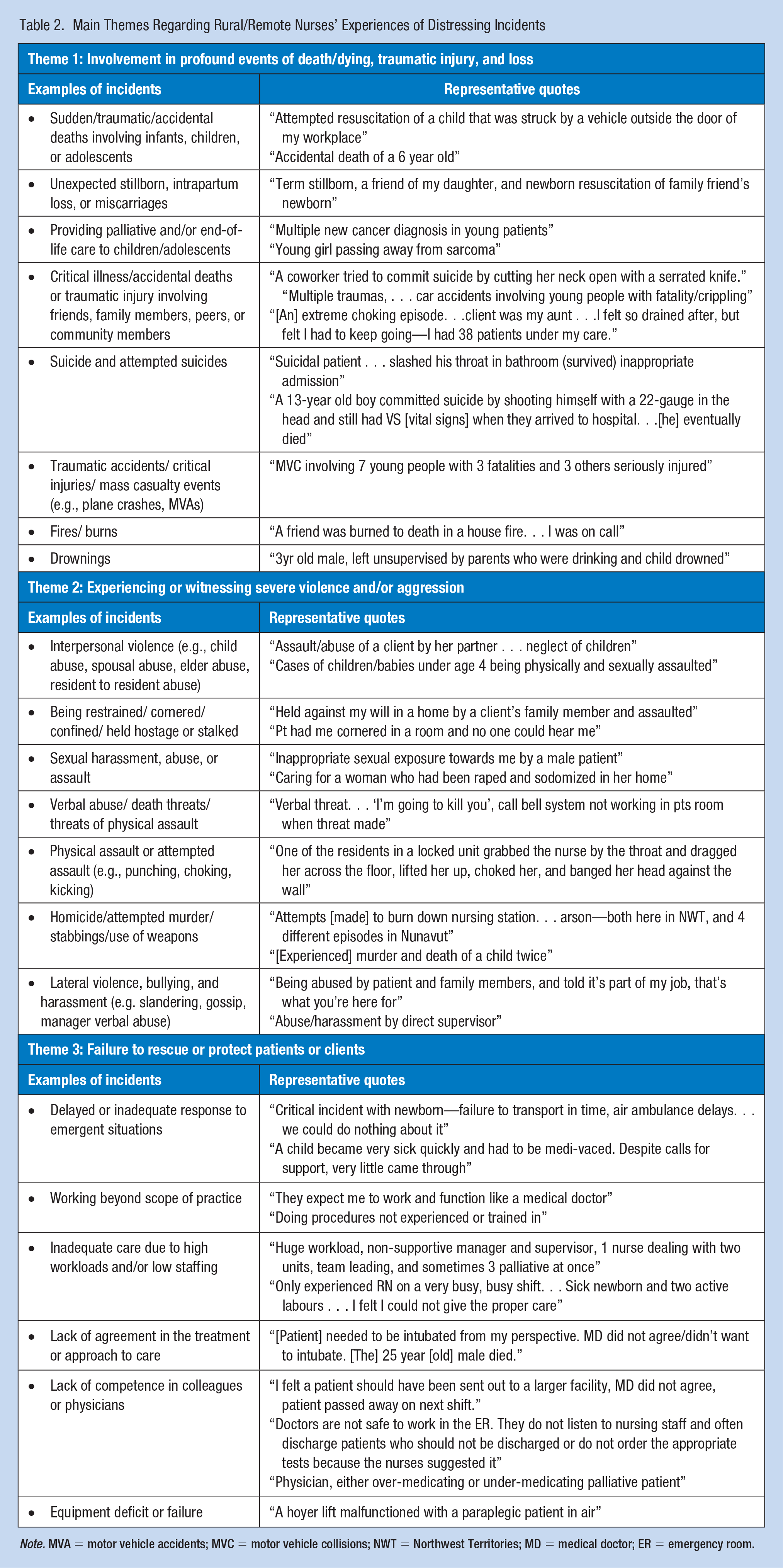
Note. MVA = motor vehicle accidents; MVC = motor vehicle collisions; NWT = Northwest Territories; MD = medical doctor; ER = emergency room.
Main Themes Regarding Rural/Remote Nurses’ Experiences of Distressing Incidents
Theme 1: Involvement in Profound Events of Death/Dying, Traumatic Injury, and Loss
The distressing or disturbing nature of events involving death/dying, traumatic injury, and loss was identified as the most profound and emotionally affecting health care incidents, with 713 responses coded in this theme. Deaths were often described as unexpected, tragic, or occurred in a manner that was extremely disturbing in some way (e.g., suicide by hanging, accidental overdose of children, animal attacks). In many cases, the young age of patients/clients contributed to the nurses’ experience of distress. Exposure to traumatic incidents without loss of life was also emotionally taxing, often involving patients receiving critical or mutilating injuries from serious motor vehicle or recreational vehicle accidents, or patients who had experienced extensive burns (e.g., house fire). The graphic and vivid nature of what nurses witnessed was detailed in the responses, with a primary focus on events that were startling, extreme, or horrific in some way. Some nurses highlighted the intense emotional pain and anxiety they experienced and difficulty in processing these types of events, whereas others reported more profound and traumatizing repercussions. Specific responses within the open-ended data referred to feeling/experiencing “vicarious trauma,” “post-traumatic shock,” and “PTSD.” Nurses often focused on the total volume of experiences over time and the heavy emotional toll they felt as a result. There was also a sense of powerlessness, especially when caring for people with whom they had a relationship within the community. Many of the victims involved in these events were friends, family, or family of friends, with one nurse stating, “in a small community, your patients become your friends and your friends become your patients.”
Theme 2: Experiencing or Witnessing Severe Violence and/or Aggression
There were 410 responses from nurses who experienced and/or witnessed an array of incidents related to severe violence or aggression. Common direct experiences of violence included verbal abuse and harassment, threats of physical harm or death, sexual harassment, and/or being lunged at, restrained, cornered, or confined. Nurses also reported experiencing and witnessing sexual assault and physical assault, sustaining injuries leading to their own permanent disability, and in one attack, the patient was charged with attempted murder. An increasing trend of unpredictably hostile and combative behaviors from patients and community members was evident in the data, with underlying issues of nurses feeling completely unprepared to deal with the impact of these events. Some nurses expressed frustration about the lack of security in their work environment to protect them or ensure their safety. Respondents noted that “it’s not safe to work in ER,” and “in the workplace the nurses put themselves in danger.” Violence and aggression by family members of patients/clients and increased number of incidents involving weapons (e.g., knives, guns) while in the hospital were also expressed. In one example, a nurse reported having a loaded gun pointed to her head. Nurses reported feelings of distress when caring for victims of interpersonal violence (e.g., spousal/elder abuse) and extreme anguish/sorrow when dealing with neglect, physical abuse, sexual assault, or violence directed toward children.
Theme 3: Failure to Rescue or Protect Patients or Clients
Many rural and remote nurses experienced distress when they were not able to rescue or protect patients under their care, with 324 coded responses within this theme. Nurses reported events involving delayed or inadequate response times, emergent situations with complications, and deficient equipment or equipment failure that negatively influenced patient outcomes. Nurses commonly noticed the earliest warning signs of a deteriorating situation but were unable to obtain the assistance or support required due to limited human resources. Some described unsuccessful attempts to escalate physician intervention and responsiveness after a sudden change in a patient’s health status, or dismissal of their attempt to achieve a patient transfer to a more advanced care facility. Nurses in these settings depended largely on the mobilization and timely response of physicians and reported frustration with colleagues who refused to respond or were ill-equipped to deal with complex situations. When negative patient/client outcomes occurred, many nurses were also overwhelmed with self-blame and shame.
Main Themes Regarding Rural/Remote Nurses’ Perceptions of Organizational Support
Overall, there were 804 nurses (65%) who indicated “no” that they did not receive psychological support from the leadership in their organization. A total of 656 rural and remote nurses provided a response regarding whether they received the “kind of support needed” from their organization following an extremely distressing incident. Of these nurses, 270 indicated “yes” (41.2%), 257 indicated “partly” (39.2%), and 129 indicated “no” (19.7%). Participants used the open-ended space to elaborate on their experiences of organizational support, with three main themes identified: (a) feeling well supported in the work setting with debriefing and reliance on informal peer support, (b) lack of acknowledgment and support from leaders on the nature and impact of distressing events, and (c) barriers influencing access to adequate mental health services in rural and remote practice settings. Table 3 provides a summary of main themes and representative quotes.
Main Themes Regarding Rural/Remote Nurses’ Perceptions of Organizational Support
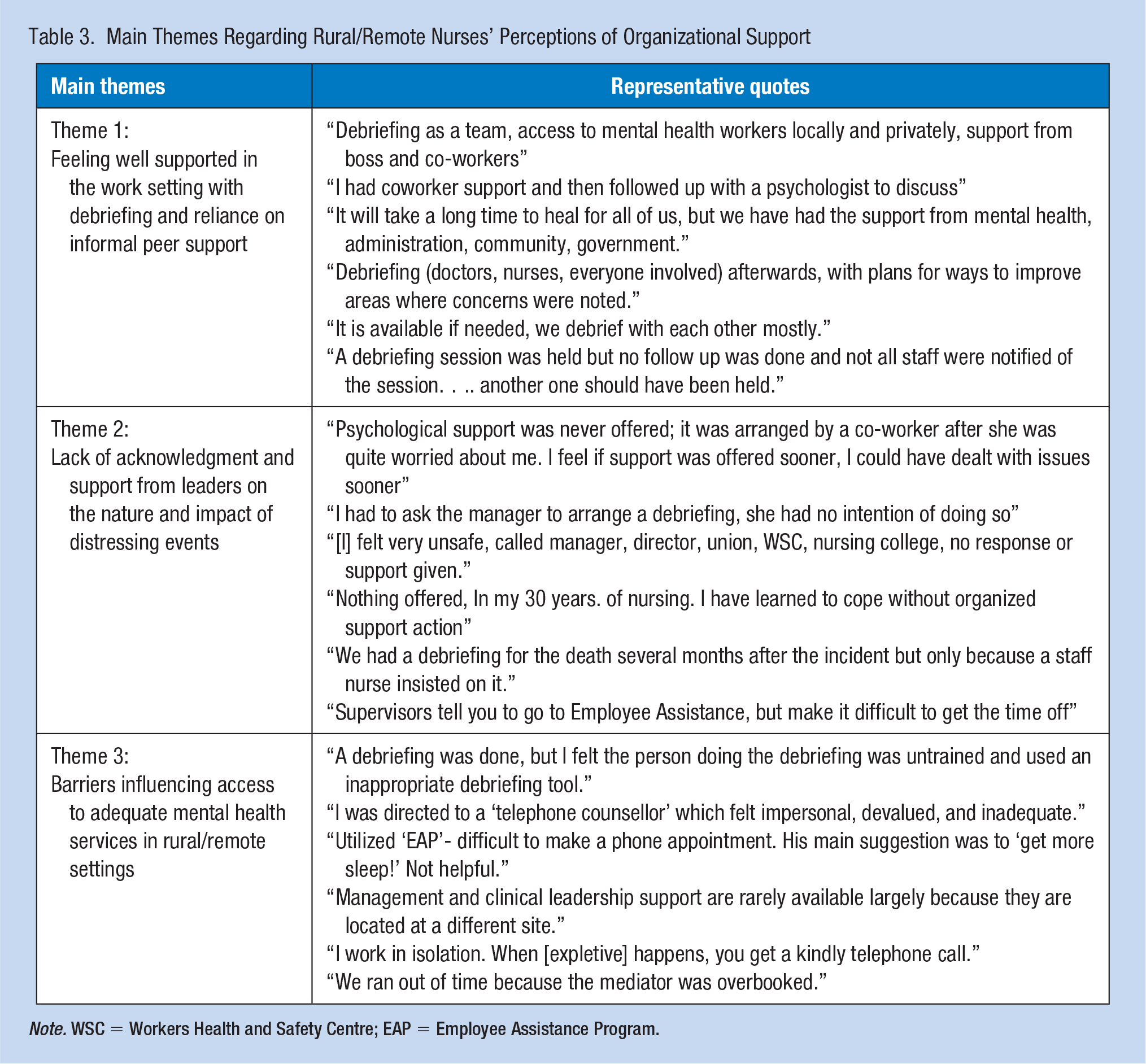
Note. WSC = Workers Health and Safety Centre; EAP = Employee Assistance Program.
Theme 1: Feeling Well Supported in the Work Setting With Debriefing and Reliance on Informal Peer Support
Many nurses described a positive response and strong support from leaders following distressing events. Some reported that their organizations offered formal debriefing and provided opportunities to access other forms of mental health support. Participants also relied on the informal support of peers and colleagues and found conversations with others with similar experiences, to be a comfortable way to discuss the events and personal impact. One nurse wrote, “debriefing was offered but not necessary. I received emotional support from colleagues.” Peer support, in particular, was viewed as an effective technique to process what transpired and cope with the psychological impact of the events. For example, one nurse summarized that “co-workers were able to support and listen to my concerns and I was able to voice my feelings of being traumatized afterward.”
Theme 2: Lack of Acknowledgment and Support From Leaders on the Nature and Impact of Distressing Events
Although some nurses felt relatively well supported, a common theme shared was the lack of acknowledgment from leaders regarding the serious nature of these types of experiences, and the subsequent risks that these nurses faced in terms of lasting emotional distress and trauma. Many nurses indicated that events were downplayed or not taken seriously in their work settings, whereas others described a lack of timely and appropriate follow-up. Nurses also felt personally responsible to seek formal support/assistance, especially if the emotional effects of their experiences lingered on. Others felt isolated and alone in dealing with their grief or feelings of despair.
Many nurses also described the minimal efforts made by leaders to acknowledge their need for safety or learn from violence-related incidents and implement changes to mitigate incidents in the future. One nurse said, “I spoke with both nursing leadership and the Royal Canadian Mounted Police (RCMP), but still feel hospital security could be improved, especially on nights.” A few nurses identified their own emotional trauma and distress as an occupational hazard, working within an organizational culture that normalized the occurrence of traumatic events. As a result, many nurses indicated that they had to rely on informal support in dealing with the aftermath of events, such as turning to their spouses/partners, family members, peers, or friends.
Theme 3: Barriers Influencing Access to Adequate Mental Health Services in Rural and Remote Practice Settings
Even when nurses felt that their leaders were trying to offer formal supportive services following distressing events, nurses noted significant barriers influencing their ability to access these services when and/or where they were needed the most. Support was often slow and inadequate. Even when critical stress debriefing was offered following an incident, there were challenges to participation related to workload, understaffing, and working in isolation. When nurses were instructed to contact their Employee and Family Assistance Program (EFAP), inconsistent availability was a common experience. Specific barriers to accessing EFAP were difficulties with scheduling an appointment, overbooked providers, and a general lack of locally available treatment options.
Other barriers centered around the ineffectual or inappropriate nature of services. Some nurses indicated that when debriefing support was offered, it was frequently delayed and therefore, viewed as “too late and not helpful.” In other responses, nurses indicated that debriefings were facilitated by individuals who did not possess the expertise or skills necessary to adequately address the nurses’ mental and/or emotional concerns. Nurses were also concerned that the supports available were not always suitable in the context of rural/remote practice. For example, several nurses described their discomfort disclosing the details of their experiences in small support groups in their communities and some preferred to remain private. Others chose not to seek support given their personal ties to the community, issues of confidentiality, concerns for their own reputation, or their sense of professional obligation to deal with it on their own, or “you are expected to suck it up and get back to work.”
Discussion
With almost one third of the national sample having experienced an extremely distressing event within the last 2 years, this issue appears to be widespread; yet there is very little research exploring such events in rural and remote settings. The long-term effects of experiencing or being witness to such events are not known (Mealer & Jones, 2013), particularly if responses to critical incidents are not immediate (Weymouth et al., 2007). There are concerns that the emotional consequences of being immersed in others’ painful circumstances could have a profound and long-lasting impact (Scott et al., 2009).
The impact of dealing with traumatic death or injury was a significant concern for participants, and especially when incidents involved patients who were younger or deaths were distressing in nature (Adriaenssens et al., 2012). Nurses found it much more difficult to cope when they knew or had a relationship with the patient or their family members (Beckstrand et al., 2012). The personal and professional interconnections that often develop in rural and remote communities (Zibrik et al., 2010) were evident in this study and appeared to add considerable emotional distress. There are concerns that rural and remote nurses may be particularly at risk for negative psychological impacts, such as vicarious trauma or PTSD, given their direct exposure to events, isolated practice, strong community ties, and lack of organizational support (Guitar & Molinaro, 2017; Manitoba Nurses Union, 2015). Opportunities for nurses to participate in professional debriefing, access supportive mental health services, and take time away to focus on dealing with the impact of death, dying, and traumatic loss are necessary.
The events shared involving severe violence and aggression were also shocking, with nurses experiencing physical and mental violence directly, and being a witness to abuse, neglect, and interpersonal violence experienced by others. The impact of witnessing or experiencing such events can result in time off work, hospitalization, relocation, resignation, disability, or even an inability to continue in nursing practice (Manitoba Nurses Union, 2015; Reichert, 2017). The nurses’ experiences confirmed that violent acts are often unpredictable or implicit and leave them frightened, feeling threatened, and in danger for their life. Geographical isolation and the lack of support staff cause nurses to feel vulnerable, defenseless, and at risk in rural practice settings (Terry et al., 2015). A pattern of extreme and ongoing episodes of violence in rural and remote nursing has been previously found (Lenthall et al., 2018), including evidence of inadequate security support or inadequate measures in place to protect nurses across the country (Reichert, 2017). There is a need for greater, timely, and consistent responses by leaders to create safer environments, address workplace violence, and protect nurses from violence-related injuries and psychological harm.
The impact of a sense of failure-to-rescue is associated with failure to recognize or respond to a patients’ clinical deterioration (Clarke & Aiken, 2003) or shield them from harm, injury, or death; regardless of actions or extreme efforts (Mushta et al., 2018), often arising from interprofessional disagreement surrounding patient care and assessment (Siedlecki & Hixson, 2015). Gunther and Thomas (2006) have suggested that when nurses are unable to rescue or protect patients from harm, they are burdened with self-blame, guilt, and perceived failure. Nurses feel responsible for early recognition, intervention, and action (Massey et al., 2017) and are highly distressed when they are witness to unfavorable patient outcomes or they are unable to intervene in a timely manner (Flicek, 2012). The broad scope of practice and high level of proficiency expected from rural and remote nurses (Macleod et al., 2017; Misener et al., 2008), coupled with caring for a population they know (Baca, 2011; Macleod et al., 2004), may further complicate their sense of responsibility and feelings of guilt (Ullström et al., 2014).
Nurses in rural practice use the EFAP programs available to them; however, they do not have the same access or timely response to debriefing and mental health supports as is available to their urban counterparts. Professional support services are often inadequate locally, with further barriers related to scheduling limitations, staffing relief coverage challenges, and travel distance to attend counseling and debriefing sessions. For this reason, many rural and remote nurses tend to rely on one another for emotional and mental support (Terry et al., 2015). There is a need to develop rural/remote specific interventions that follow best practice guidelines (Salas et al., 2008), and improved access to professional counseling and debriefing (McCullough et al., 2012). Interventions that may be particularly well-suited for rural/remote practice areas are workplace peer support programs, which are designed to provide education and skills on how to identify those in need and concrete tools to better support one another (Forchuk et al., 2016). Supportive interventions that incorporate more sophisticated modern technology (Silva et al., 2015) may also be more practical for rural and remote nurses because access is not limited to location or timing of events. Enhanced safety strategies that reduce the risk of violence against rural and remote nurses are also important, with an increased focus on training in communication, cultural safety, risk assessment, and techniques in aggression management and de-escalation (McCullough et al., 2012). Organizational leaders at all levels of management have an obligation to initiate, maintain, and support a culture of enhanced safety for rural nurses (Terry et al., 2015).
Implication for Occupational Health Nursing Practice
The study revealed limited organizational understanding of the significance and impact of distressing incidents, lack of organizational strategies designed for rural/remote nursing, and the need for future research evaluating interventions in rural/remote settings. Although some nurses felt well supported, protective services were viewed as limited or absent by others with most being self-initiated, not accessible, or non-existent. This research has important implications for occupational health and safety, as it highlights the need to identify and address the potential distressing incidents/hazards encountered by rural/remote nurses. Nursing education curriculum that focuses on peer support training may better prepare novice nurses entering rural/remote practice settings. Preventive education for nurses and managers to identify those at psychological risk may also reduce work-related psychological distress (Skogstad et al., 2013). Qualified and timely mental health support should be more accessible with post-exposure debriefing (Maloney, 2012) and consistent follow-up (Kessler et al., 2015). Enhanced violence-prevention practices and policies, education that focuses on protective approaches to de-escalate hostile or high-risk situations (Tölli et al., 2017), greater patient and family accountability for violent actions through legal means (Vogel, 2016), and strategies to ensure organizational accountability through occupational health and safety legislation should be pursued (Stene et al., 2015).
A particular strength of this study was that it encompassed a nationally representative sample of rural and remote Canadian nurses and included all types of regulated nurses (NPs, RNs, RPNs, and LPNs). Because this survey employed a cross-sectional design, there were a few noted limitations. As the participants’ responses were written, this did not allow for the richness of data that may have been possible through in-depth interviews. For example, in some cases, written responses were only a line or two with the inability of the researchers to ask follow-up questions or have respondents clarify or elaborate on their experiences. Another limitation was the structured questionnaire which did not give nurses the opportunity to elaborate on their response when they reported that they did not receive psychological support from the leadership in their organization following an extremely distressing incident.
Conclusion
The findings of this study indicated that nurses who practiced in rural and remote communities were confronted with a variety of distressing incidents that may have a lasting impact on their psychological health and physical safety. There were concerns that these types of events are under-reported in rural and remote settings, with a lack of supportive action from organizations and limited protective strategies available. Their experiences related to traumatic injury and death, witnessing and/or experiencing various forms of violence, and failure to rescue patients or clients, were particularly distressing. The sense of responsibility and anguish that rural and remote nurses experienced was also magnified when events involved members of their own communities. Although some nurses felt relatively well supported by their organizations (e.g., access to formal debriefing sessions), reliance only on informal social supports (e.g., peers/colleagues, friends, family) was commonplace. The impact of such events needs to be acknowledged and addressed through an improved availability of mental health services, increased education, and enhanced safety measures.
Footnotes
Acknowledgements
This article stems from the study “Nursing Practice in Rural and Remote Canada II,” led by MacLeod, M., Stewart, N., and Kulig, J (![]() ). The authors thank the Advisory Team led by Penny Anguish of Northern Health, and nurses who responded to the survey. They also thank Leana Garraway and Janna Olynick for their contributions.
). The authors thank the Advisory Team led by Penny Anguish of Northern Health, and nurses who responded to the survey. They also thank Leana Garraway and Janna Olynick for their contributions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a trainee stipend from the Rural Dementia Action Research Program (RaDAR). Funding for the study was provided by the Canadian Institutes of Health Research (MOP 130260).
Author Biographies
Sharleen Jahner PhD Candidate, RN—doctoral student with the College of Nursing, University of Saskatchewan with a research focus on the psychological implications of occupational traumatic exposure.
Kelly Penz PhD, RN—Assistant Professor in the College of Nursing, University of Saskatchewan with a research focus on the professional quality of life of nurses in palliative/end-of-life care and nurses in rural and remote practice.
Norma J. Stewart, PhD, B.S.N.—Professor Emerita with the College of Nursing at the University of Saskatchewan with a research focus on rural dementia care and rural nursing practice.
Martha L. P. MacLeod PhD, RN—Northern Health, UNBC Knowledge Mobilization Research Chair, Co-Leader of the UNBC Health Research Institute, School of Nursing professor.