
Abstract
Background: High levels of stress and burnout, documented among healthcare professionals, result in high levels of job turnover. However, little is known about personal strategies employed by advanced practice providers (APPs) to mitigate stress. Methods: 3,939 APPs were invited to complete an online, anonymous, cross-sectional survey to examine work stress and burnout among APPs using quantitative and qualitative analyses. The Maslach Burnout Inventory (MBI) served as the measure for burnout. Work-stress reduction strategies were identified by an open-ended question. Findings: 854 APPs (70% of 1,218 respondents) (nurse practitioners, physician assistants, nurse midwives, anesthetists, and clinical nurse specialists) from four different United States health systems completed the free text portion of the survey. Qualitative analyses revealed that almost all of the APPs (94%) reported at least one stress reduction strategy. Four main themes were derived from the free-text responses: “Self-focused” (67.5%), “relational-focused”(16.1%), “job-focused” (11.5%) and “nothing” (4.9%). Quantitative results from the MBI revealed high levels of burnout among APPs with insignificant differences between those who provided a response to the qualitative question and those who did not: emotional exhaustion (p = .188); depersonalization (p = .265); personal accomplishment (p = .213). Conclusion/Application to Practice: Qualitative results highlighted strategies, many evidence-based, that APPs use to mitigate stress. Further research is needed to determine the frequency and consistency of APPs’ enactment of personal strategies. These initial findings provide insights for occupational health practitioners and researchers planning primary prevention and secondary interventions for improving workplace health, enhancing personal wellness, and reducing job-related stressors.
Background
Within the last few years, the primary care physician shortage (Buerhaus, 2018), the growing Medicare eligible population (DesRoches et al., 2017), and the exponential increase in the number of diagnosed cases of chronic diseases such as Alzheimer’s (Buerhaus, 2018) are reported as formidable challenges within the American health care landscape (Shanafelt & Noseworthy, 2017). Advanced practice registered nurses (APRNs) and physician assistants (PAs), also known as advanced practice providers (APPs), play a critical role in increasing the number of providers needed not only within primary care but also in specialty practices, with nurse practitioners (NPs) more likely to serve the needs of those living in rural areas (Buerhaus, 2018; Health Resources and Services Administration, 2016). Various work-related stressors such as heavy workloads (Shanafelt & Noseworthy, 2017), role ambiguity (Klein et al., 2020), and lack of autonomy (Hagan & Curtis, 2018) contribute to the high levels of burnout that are being reported separately in recent studies of physicians (West et al., 2018), nurses (Ahola et al., 2017), and NPs (Dyrbye et al., 2019). In addition, Richardson (2017) summarized new challenges that require further examination, which include the impact of technology-related stressors (Reyt & Wiesenfeld, 2015), workplace telepressure (Barber & Santuzzi, 2015), and workplace incivility on the individual’s physical and psychological health. Changes in communication patterns as described are detrimental to employee well-being (Richardson, 2017).
Work motivation, quality of life, and the intrinsic and extrinsic factors of providers (Schrijver et al., 2016) have also been examined as possible contributors to burnout and reduced job satisfaction. Research has shown that high levels of burnout and low levels of employee well-being are correlated with greater levels of job turnover (Dyrbye et al., 2019), which could undermine APPs’ abilities to positively affect the growing medical provider shortage (Han et al., 2018). Earlier studies, which have demonstrated APPs’ positive contributions to quality of care and patient satisfaction, are laudable reasons supporting their utilization for increased patient access to care (Hoff et al., 2019). Consequently, there is a compelling need to explore the management of work-related stressors by APPs within their everyday work environment (Dill et al., 2013; Hoff et al., 2019).
In a different context, Edmunds (2014) indicated the need for NPs to consider their individual tolerance levels for stress. Yet, few studies in the APP literature describe primary (preventive), secondary (stress symptom reduction), or tertiary interventions for ameliorating work stress for APPs (Ahola et al., 2017; Hoff et al., 2019). Tertiary interventions typically focus on the treatment of stress-related conditions; for example, employee assistance programs (Richardson & Rothstein, 2008).
Employee wellness programs have historically been implemented as separate initiatives from employee assistance programs, with wellness programs classified as preventive (Richardson, 2017). Secondary interventions such as mindfulness-based stress reduction programs and others have been suggested in the nursing and medical literature as a way to improve personal resilience (Fortney et al., 2013; Potter et al., 2013). In addition, quiet moments and other non-patient-care-related activities were suggested as focuses for future research of job satisfiers for NPs (Fournier et al., 2019).
The need for multi-faceted approaches to improve the mental health and well-being of employees has been recommended by authors of two different systematic reviews of job-stress intervention studies focused on general practitioners and physicians (Murray et al., 2016; Panagioti et al., 2018). Conversely, Richardson and Rothstein (2008) determined from a meta-analysis of stress management intervention studies that cognitive behavioral approaches alone were most effective at reducing work stress, with a caveat that educating employees on strategies for work-stress reduction adds value. Encouraging personal strategies which can augment other preventive and secondary interventions may be beneficial, although limited evidence describes those individual strategies that are most commonly used by APPs. Likewise, in their systematic review, Park and Jang (2019) suggested the need for randomized controlled trials that evaluate workplace exercise interventions in combination with other approaches (mindfulness and improved work environment) as there is little support of the effectiveness of exercise at work in minimizing job stress.
One of the objectives of this study was to examine the various interventions used by APPs to manage their stress during their working hours. Patient care and safety depend on providers whose work efforts are not affected by burnout and job-related stressors (Shanafelt & Noseworthy, 2017); thus, this study provides insights for occupational and environmental health practitioners interested in designing primary prevention programs and secondary interventions, which support healthy work habits.
Methods
A large cross-sectional, exploratory study of APP burnout and job stressors was undertaken in 2017. A convenience sample of PAs and APRNs working within primary care and specialty practices in large hospital/health care systems was recruited from four states (Klein et al., 2020). Four of eight leaders from different health care systems across the United States responded affirmatively to recruitment into the study using email and direct communication, with consideration of the following criteria: (a) employment of APPs in outpatient and inpatient settings, (b) Magnet® recognition as a system or at least one hospital as a Magnet-recognized organization, and (c) interest in participating in multi-site research. The Magnet designation criterion served as an identifier of organizations that are required to be engaged in nursing research (Klein et al., 2019). The study received institutional review board (IRB) approvals before initiation as an exempt protocol (University of Illinois, College of Medicine at Peoria, IRB 1; Protocol No. 966948-3).
An online survey methodology with techniques to improve survey responses (Fan & Yan, 2010) was used to invite 3,939 APPs working in various settings ranging from metropolitan to rural areas. A designated study site coordinator worked with the multi-site principal investigator to determine APP sample composition according to inclusion criteria, to coordinate study logistics, and to streamline and personalize implementation locally. The survey was available for a 6-week period at each site during the latter half of 2017. The survey was administered using Qualtrics. The initial invitation, survey link, and three reminder requests were sent via internal email addresses. No personal identifiers were collected and participants were assured anonymity through use of an implied consent process with survey completion.
The anonymous survey included four standardized scales to measure variables within a hypothesized conceptual model. For the purposes of this analysis, only the Maslach Burnout Inventory (MBI)–Human Services Survey (HSS) used for the measurement of burnout is described and reported (Maslach et al., 2016). The MBI-HSS contains 22 items that are ranked on a 7-point frequency Likert-type scale from 0 (never) to 6 (every day). Emotional Exhaustion (nine items, α = .90), Depersonalization (five items, α = .79), and Personal Accomplishment (eight items, α = .71) are the three subscales used to assess burnout. Emotional exhaustion refers to the physical symptoms associated with burnout such as fatigue, weakness, and lower energy levels. Depersonalization is described as a development of a calloused or cynical attitude toward recipients of care or services. The lack of personal accomplishment is exemplified by feelings of low professional self-esteem and feelings of insufficiency (Maslach et al., 2016). The tool has established internal reliability and convergent validity and is considered the “leading measure” for burnout (Maslach et al., 2016). Participants were then asked an open-ended question of “What do you personally do to reduce stress at work?” Perspectives of APPs were deemed as a necessary component for examining burnout prevalence, contributing factors, and determining possible interventions within the workplace.
Data Analysis
The respondent characteristics and original data responses to the open-ended question were downloaded from the Qualtrics survey platform. The data were imported into Dedoose Version 8.0.42, a tool used for coding and analyzing themes. Responses were summarized using a rich thematic description of the entire data set. Inductive content analysis was used to convert large volumes of text data into categories (manifest content) representing similar meanings (latent content) that were condensed into themes and codes (Hsieh & Shannon, 2005).
Following the method outlined by Hsieh and Shannon (2005), three members of the research team read all the responses and used an iterative approach to identify emergent codes derived from verbatim words and phrases that described personal strategies. Each listed strategy was considered as a separate unit. This process considers participants’ responses without the application of theoretical categories to the data (Hsieh & Shannon, 2005). The codebook was further refined using Cohen’s kappa to measure interrater agreement between the members of the research team. After a kappa value >.85 was established, which represents a very high interrater agreement according to Bernard (2011), the codebook was applied across the complete data set. All members of the research team reviewed all coded responses/themes. As commonalities, patterns, and frequencies across the data were identified, codes were then organized into hierarchical tree diagram consisting of themes, subthemes, and codes (Hsieh & Shannon, 2005).
Results
A total of 1,218 of 3,939 APPs responded to the survey (31%) and 854 participants (70%) provided a response to the open-ended question. Table 1 provides the demographic profile of the respondents. Representation of all roles of APPs were noted within this subset of the respondents for this research study with 556 (65.1%) working as advanced practice nurses and 298 (34.9%) as PAs.
Demographics and MBI Characteristics of Participants (N = 854)
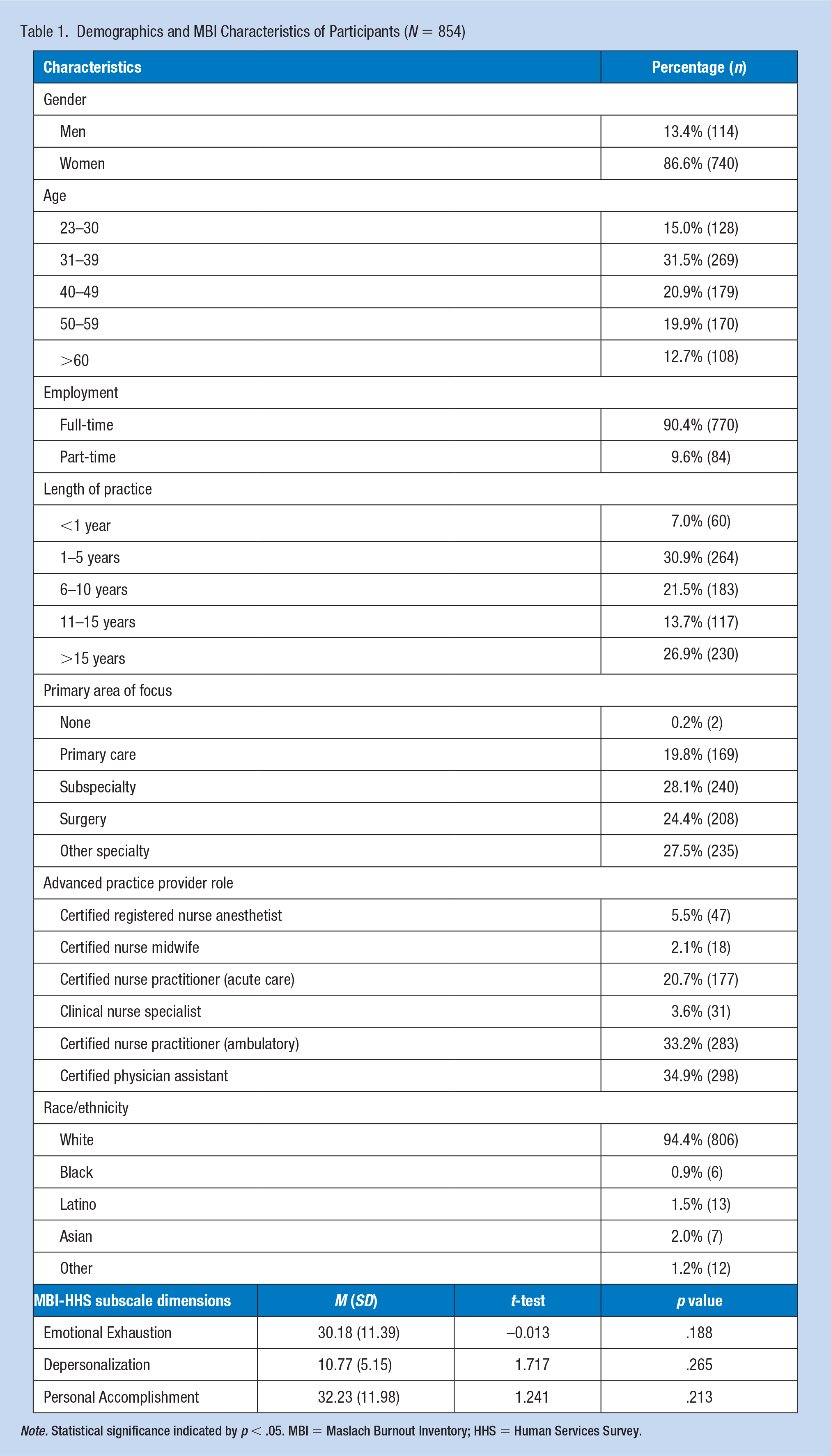
Note. Statistical significance indicated by p < .05. MBI = Maslach Burnout Inventory; HHS = Human Services Survey.
MBI Results
The APPs who provided a response to the open-ended question at the end of the survey demonstrated a high level of burnout as measured by the MBI-HHS subscale dimensions (Table 1). Reported ranges for each of the three dimensions are 0 to 54 emotional exhaustion, 0 to 30 for depersonalization, and 0 to 48 for personal accomplishment, with higher reported scores of the respondents in the first two dimensions as attributable to burnout. Cronbach’s alpha estimates within this study were similar to those previously reported. Results from t-test analyses (Table 1) showed no significant differences in the three subscale dimensions (p values > .05) between the survey respondents who did (N = 854) and did not complete the free-text response question (n = 364).
APP-Reported Strategies for Work-Stress Reduction
Table 2 depicts an overview of the qualitative findings from 854 participants who provided 1,190 codes that illustrate what they do to reduce stress at work. The data were ordered into 24 codes, 10 subthemes, and four themes. Three of the four themes consist of the various strategies that APPs use to manage their stress at the work place: (a) self-focused, (b) relational-focused, (c) job-focused, and (d) nothing. Representative quotes reflecting core themes give voice to the APPs and describe their particular self-directed actions at work. Each discrete quotation represents a different APP respondent’s typed-in response. Individual identifiers have been omitted intentionally as a way to preserve and protect anonymity in accordance with IRB approval.
Overview of Findings: Relation of Themes, Subthemes, and Codes
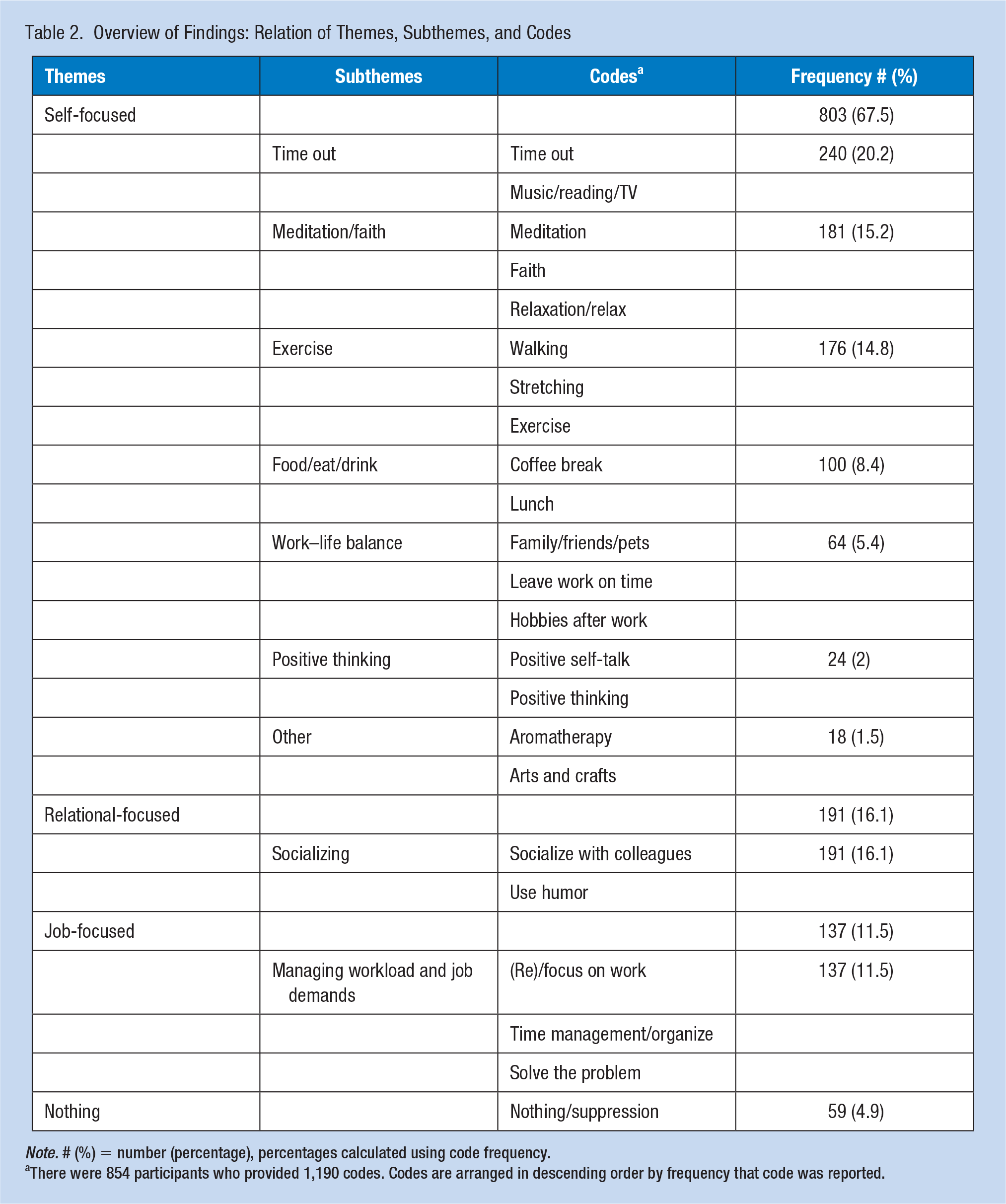
Note. # (%) = number (percentage), percentages calculated using code frequency.
There were 854 participants who provided 1,190 codes. Codes are arranged in descending order by frequency that code was reported.
Self-focused
The most commonly discussed method reported by APPs to reduce stress in the workplace were categorized as a self-focused theme (n = 803). They consist of activities that APPs do by themselves, such as taking a time out to gather their thoughts, calm down, or to take a mental break. Interestingly, almost every APP, aside from those who answered “nothing” used some of these strategies throughout the day, and sometimes used more than one. However, it was frequently mentioned how difficult it was to do these basic self-care activities. Quotes from several participants exemplify their typical presentation: “Take break and walk away for a few minutes,” “Go to my office and take a minute to relax,” and “Take small breaks to gather my thoughts.”
Other responses indicated that APPs also take time to do simple low-intensity physical interventions such as walking outside or within the hospital/clinic setting, stretching, or doing simple exercises such as yoga. Specific quotes from APP participants within the exercise subtheme show the diversity of activities: “Small exercises like calf raises,” “Take a quick walk outside for fresh air,” and “Stretch my muscles.”
Meditation, deep breathing, relaxation techniques, and faith-related activities such as prayer or scripture reading were listed separately or as a combined strategy for 181 (21.2%) of the APP respondents. Examples of expression of these techniques are as follows: “Walk away from my computer and close my eyes and focus on breathing for 5 to 10 minutes,” “Meditation and deep breathing,” and “Take a few minutes of quiet time or prayer.”
Less frequently, APPs mentioned that finding time for lunch, a coffee break, positive thinking, or finding time to talk to their family were all strategies that they use to control their daily stress. Refer to Table 2, Subthemes for specific percentages. These little breaks throughout the day to refresh, be alone, and “de-stress” were seen as important components of reducing stress levels and not being able to do them was seen as problematic by some. The following is a sample from the subtheme category Food/eat/drink: “I read at lunch to get my mind off of work issues. When I don’t get a lunch, or don’t have time to read, it increases my stress.” However, some APPs recognized how difficult it can be to find time for these activities, which could be the reason why participants listed some of the self-focused strategies that required a greater time commitment less often: “Hard to catch a breath at times; deep breathing is what I might have time for.”
Relational-focused
Collegiality and social support within the work setting emerged as important relational-focused strategies for 191(22.4%) APPs for managing stress and promoting engagement. Aside from being able to take a time out to be by oneself, APPs frequently mentioned the importance of being able to socialize with coworkers, peers, and colleagues. The following quotations show APPs’ expression of the socializing subtheme category: “Talk in confidence to friends about what’s annoying me” and “Discuss issues with coworkers to allow stress to dissipate.” However, in others, it was to build meaningful relationships, commiserate, or just laugh—“Engage in the social life of my colleagues” and “Vent about it though I probably shouldn’t, or I make a joke about the stress.”
In any of the aforementioned strategies, APPs emphasized the importance of taking time throughout the day to interact with those around them, and through “giving and receiving support,” they are better able to manage the daily stress of work. Specific details about how relationships were used as support and to de-stress APPs are illustrated in these two quotes from providers; “Eat lunch with my colleagues; laugh; give support to and receive support from members of my work family” and “Maintain a good working relationship with my coworkers and collaborating physicians—our stressors are usually directly related and we get each other through a rough day together.”
Job-focused
The third theme, categorized as job-focused, which APPs utilize, relates to how they try to adapt to their work environment and stay on task. As the least reported strategies, they could be the hardest to implement as expressed by some individuals who mentioned that the day-to-day workflow made it hard for them to “keep up” or “leave on time.” Nevertheless, most of these strategies deal with personal control over their time and response, rather than changing the work environment. Representative comments were, “Focus and take one thing at a time,” “Stay focused on the patients and not the drama of work,” and “Set achievable goals and a time to leave for the day.”
Other strategies were described as means to increase productivity, which in turn might reduce stress. They include organizing and keeping up with the workflow. The following are samples from the subtheme of time management/organize: “Try to prioritize and try not to get overwhelmed”; “Try to stay on schedule, keep up with notes”; and “Organize prior to seeing patients.”
In a few situations, APPs also try to solve the problem or to fix the cause of their stress. Usually this occurs through talking about issues, problem solving, or turning to others for help. Unlike other strategies, in which the APP describes an attempt to adapt to a stressful situation, addressing the problem may also mitigate future stressors and suggests that an APP believes that the health care system and/or coworkers are receptive to change. Typical comments from the subtheme of Solve the problem were, “I am surrounded by an experienced and supportive team that I can turn to if I have any issues or concerns,” “Talk to my coworkers about the stress and discuss solutions to the problems,” “Discuss doubts with attending physician,” and “Team meetings and daily debriefings.”
Nothing
A small number (n = 59) of APP respondents typed a response of “nothing” or “suppression” and these responses were considered as a specific theme, nothing. Coded answers indicate their inaction, which may be different from those who did not respond to the open-ended question.
Discussion
Minimal studies exist that address APP well-being and burnout, and those that do, have limited data analyses (Benson et al., 2016; Hoff et al., 2019). Comparison of these findings with other health care professionals requires use of physicians as benchmarks until more research regarding APPs is completed. In a recent study by Edwards et al. (2018) that examined primary care practices, physicians and APPs had a higher odds of burnout than either the office managers or non-clinical staff using a one-item burnout measure. Studies to date of APPs’ work-stress reduction are primarily focused on job satisfaction and intent to leave using quantitative study designs (Han et al., 2018; Hoff et al., 2019; Shea, 2015). The MBI measures in this study, although insignificant in terms of differences between groups, approximate the baseline characteristics of physicians reported in earlier studies (Goodman & Schorling, 2012; Lee et al., 2016) with higher scores in the emotional exhaustion and depersonalization subscales and overall physician burnout reported in intervention studies (West et al., 2014). Interestingly, APPs within this study presented with the lower scores in the personal accomplishment dimension as well; a finding reported previously in comparisons of registered nurses with physicians (Schaufeli & Enzmann, 1998).
Han et al. (2018) determined that methods to improve the retention of APRNs included three factors: the importance of a supportive practice environment, favorable relationships with physicians and administrators, and improved day-to-day experiences. Organizational strategies related to communication, teamwork, and job control are also deemed as interventions that will help to reduce physician burnout (Panagioti et al., 2018), but tend to be rarely used and remain understudied at this point in time. Our findings indicate that the majority of APPs have chosen to focus individually on managing time and schedules in a way that allows for brief respites and engagement in activities (physical and psychological) that may help to reduce work stressors. The notion of “time out” represented the largest subtheme, which is similar in concept to the discussion of “quiet moments” by Fournier et al. (2019). Notably, some of these activities such as lunchtime walks, exercise, meditation, mindfulness, and relaxation techniques are supported by prior studies (Shapiro et al., 2005; Sianoja et al., 2018; Slutsky et al., 2019; Valley & Stallones, 2018; Weight et al., 2013; Werneburg et al., 2011). A recent qualitative study of physicians indicated their inability to envision adding wellness-related activities to a maximized work schedule (Schrijver et al., 2016). In our current study of self-reported activities by APPs, it is not known how often the APPs are using their strategies as part of their daily routine.
Relational-focused strategies, specifically socializing with colleagues, was described by 191 of the 854 APPs and is a finding that warrants further investigation. The APPs’ descriptions of how they engage with others at work lend credence to the recent research of Perzynski et al. (2018) which measured three facets of social capital at the workplace level in relation to teamwork, employee burnout, and patient satisfaction. Two of the facets, structural and relational, are depicted in the responses of APPs in this study. Information sharing, a structural facet, was defined and measured by Perzynski et al. (2018) by three items that describe how people communicate with each other. The first item considered the degree of open, honest, communication. The other two items asked employees to rate their comfort level in giving and receiving constructive criticism and their willingness to share information with each other. The relational facet measured the operationalization of trust among coworkers in three realms: reliance on coworkers, consideration of each other’s feelings, and confidence in each other (Perzynski et al., 2018). The internal workplace social capital concept, along with its intended and unintended consequences, is worthy of attention for individuals and the organization. The relational-focused strategies in this study pointed to the positive effects of a work family, but some also alluded to job stress associated with social capital (drama of the work or drama within the work setting among coworkers).
Shanafelt and Noseworthy (2017) also described connection and community within the workplace as a more formalized solution designed to improve physician well-being. Previously tested in a randomized controlled trial using small group learning sessions, positive changes in engagement and empowerment were sustained over 12 months (West et al., 2014). In this regard, an organizational focus on events supporting socialization of colleagues as primary preventive intervention may be beneficial, but is distinctly different than what has been described by a larger, more diverse sample of APPs in this study.
The current findings are also consistent with existing older literature where researchers have described the benefit of helping individuals to improve work/lifestyle skills as a way to help manage and reduce work-related stress (van der Klink et al., 2001). Formalized strategies that encompass personal values and time management for work and home setting were also described as one of several components in an intervention study completed with women (Werneburg et al., 2011). These particular job-focused strategies and others related to improving efficiency within the office and better optimization of the electronic medical record have demonstrated value in reducing work stressors and improving engagement of providers (Ricker & Ranjbar, 2019; Shanafelt & Noseworthy, 2017).
Limitations
Although the appreciable size of respondents along with their diverse APP roles and practice settings enhances generalizability of the results, there are some limitations. These limitations include the reliance on self-reported data, a convenience sample, and use of a cross-sectional survey design. With this survey methodology, no communication between respondents and researchers occurs; consequently, conciseness of answers and the inability to ask follow-up questions limit the ability to obtain a more in-depth perspective of any of the identified themes. The selection of health care systems and the inclusion criterion of a Magnet® designated facility limit generalizability because these organizations/systems may be different in terms of policies/practices for employees related to wellness. The sample composition of White (94%) females (86.6%) may not be representative of APPs nationally. Likewise, not all providers work at large health systems; another limitation to be considered. However, many providers are now employed by large systems including those that are multistate (Ricker & Ranjbar, 2019).
Implications for Occupational Health Practice
As noted by Schill (2017), it is not enough to expect only behavioral change within an individual; a comprehensive approach for advancing worker well-being is needed. Occupational health professionals are encouraged to seek a broader and more holistic focus for improving employee health. Total Worker Health® (TWH) serves as a conceptual model for occupational health nurses and prioritizes actions for enhancing worker well-being within a hierarchy of controls (National Institute for Occupational Safety and Health [NIOSH], 2018). The hierarchical controls most closely associated with an individual worker’s response include health, safety-related education, and personal change. Elimination of conditions within the work environment that is coupled with education and personal change may be more effective and better address the underlying concerns that contribute to job-related stress and burnout.
Conclusion
In 2017, national attention on the health of physicians, nurses, and clinicians was deemed a priority by the National Academy of Medicine (NAM, 2019a), the American Nurses Association (2017), and the Institute for Healthcare Improvement (Perlo et al., 2017). Self-care influences ones’ ability to care for others. Similarly, the stability of organizations depends on the ability to attract and retain highly qualified practitioners; thus, there is a critical need for APPs’ personal management of their health and well-being (Perlo et al., 2017). Our findings provide a partial answer to the question “Do APPs care for themselves?” posed by Raftery in 2015. Yet, we need to have a better idea of how consistently these activities are used and if they are done in combination with preventive interventions instituted by employers; these questions remain unanswered. We do know from previous research within health care and other disciplines that something is better than nothing; however, these personal strategies may be either insufficient or underutilized, given the reported measures of burnout. The movement in many states toward APPs with independent practice authority and the resulting impact on their everyday work environment requires exploration as well (Edmunds, 2014).
Future studies can build upon this research by including personal techniques/strategies that can be measured. Studies that examine intervention sustainability and those focused on developing personal and professional resilience are also needed (Lin et al., 2019). The growing APP workforce has demonstrated its inherent value to serving the health care needs of the population (Buerhaus, 2018). It is essential that APPs engage in designing preventive interventions planned by their organizations, as well as seeking to implement one or more of the evidence-based strategies used by their peers (NAM, 2019b). Moreover, future research can consider qualitative approaches or longitudinal data to examine the temporal efficacy of comprehensive stress interventions that are primary, secondary, and tertiary in nature. This study brings greater awareness of the possible actions that all APPs can incorporate into their daily work life.
Applying Research to Occupational Health Practice
Similar to physician providers, APPs are not immune to job-related stressors, which raises concerns about employee retention in clinical practice. The qualitative findings of a cross-sectional study revealed the perspectives of activities used by APP providers to reduce workplace stress. Relationship-focused activities such as socialization with colleagues and taking lunch breaks are techniques employed by APPs to increase coping with occupational stress. Additionally, job-focused activities aimed to maintain task organization and keeping on time with schedule constraints were methods described for APP stress reduction. A consideration of the modification of conditions within the work environment that is coupled with education and personal change may be more effective in helping to promote wellness, thereby assisting APPs in clinical practice. Further research by occupational health practitioners to explore the use and benefits of personal self-care activities is needed.
Footnotes
Authors’ Note
All authors have contributed and approve of this manuscript and meet the four criteria as described by the International Committee of Medical Journal Editors (ICMJE) for authorship.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Sister Canisia Gerlach Endowment Fund available through OSF HealthCare Saint Francis Medical Center. Funding supported only the licensure usage agreement and purchase of the online Maslach Burnout Inventory (MBI) instrument from MindGarden, Inc.
Author Biographies
Colleen J. Klein, an education and research scientist within the Center for Advanced Practice, has primary research interests in advanced practice provider burnout and role transition, quality of life, compassion fatigue, and competency-based assessment.
Matthew D. Dalstrom is a medical anthropologist who studies health policy and access to care.
Laurence G. Weinzimmer is an endowed research professor at Bradley University and has primary research interest in nurse resilience and engagement.
Melinda Cooling is Vice President of Advanced Practice, a family nurse practitioner, and holds multiple adjunct faculty positions. Her research interests include APP burnout, APP role transition, and rheumatoid arthritis.
Lisa Pierce is a pediatric acute care nurse practitioner who is the Director of Advanced Practice Education and Fellowship Programs, with research interests in APP burnout, role transition, and transition-to-practice programs.
Shannon Lizer, a family nurse practitioner and educator, has research interests in occupational health, rural health, and advanced practice role assimilation and job strain.