
Abstract
Background: Smoking is the leading cause of preventable deaths in the United States. The rates of smoking remain elevated in rural, low income populations in comparison with the rest of the United States. Thus, prompting the process improvement project of implementing the Ask–Advise–Connect (AAC) method to the national quitline in a nurse practitioner–managed clinic for an automotive manufacturing plant in rural Tennessee. Methods: Ask–Advise–Connect method was added to the current smoking cessation program. The employees who utilized the clinic were assessed for smoking status at each visit and subsequently counseled on cessation. Individuals interested in cessation were connected to the national quitline with the AAC method. Pharmaceutical options and nicotine replacement therapy was also offered at no cost to the employee. Findings: In the 4-month period, the clinic provided 102 tobacco cessation counseling visits to workers who smoke. Twenty-four employees enrolled in the cessation program. The participants reported a cessation rate of 12.5% and 21% had a significant decrease in the number of cigarettes smoked. Of the participants, 12.5% (n = 3) engaged in behavioral counseling with the quitline. Conclusion/application to practice: The addition of the AAC method as part of the smoking cessation program had limited success. As smoking cessation is difficult to achieve, any success greater than 7% can be considered an achievement. The 12.5% cessation rate of the participants was above the national average. Thus, demonstrating the benefit of having a workplace cessation program and incorporating the AAC method to the current smoking cessation program.
Introduction
Smoking contributes to multiple health conditions and medical costs. Tobacco use has been attributed to numerous forms of cancer and chronic diseases, such as vascular disease, heart disease, and lung disease (Hyland et al., 2017). It is the leading cause of preventable deaths in the United States and the world (Toll et al., 2014). Worldwide over 7 million premature deaths were linked to smoking in 2016 (American Cancer Society and Vital Strategies, 2019). With over 480,000 deaths annually in the United States and over US$300 billion in direct and indirect costs linked to smoking, the impact of tobacco use remains high (Centers for Disease Control and Prevention [CDC], 2018a), indicating the necessity for programs aimed toward smoking cessation.
Jamal et al. (2012) found that 70% of adult smokers want to stop smoking. However, less than 5% are successful without the assistance of cessation tools, such as medication and/or counseling (West, 2017). Authors suggest that the use of the national quitline (1-800-QUIT-NOW) is thought to increase the rate of cessation (Zhu et al., 2012). Unfortunately, only 1% of smokers access this free and readily available service tool (Neri et al., 2016). Perhaps this lack of use is because neither smokers or providers are aware of the benefits of the quitline as an adjunct to smoking cessation (Rutten et al., 2011).
Quitlines were established in 2004 by the U.S. Department of Health and Human Services in conjunction with the CDC to provide smoking cessation services (CDC, 2014). The no cost telephone-based cessation services are available in each of the 50 states, U.S. territories, District of Columbia, and Pacific Islands (Saul et al., 2014). The quitlines provide cessation services such as behavior counseling, printed materials, medication education, and referrals to other smoking cessation resources (Toll et al., 2014). All statewide quitlines are accessible through 1-800-QUIT-NOW (CDC, 2014).
Multifaceted Approach to Cessation
During the past 20 years, the use of nicotine replacement therapies (NRTs), nonnicotine medications, such as Zyban and Chantix, and behavioral therapies with and without quitlines have been implemented and evaluated (Zhu et al., 2012). Researchers have found that all cessation modalities are beneficial with greater efficacy occurring when behavioral counseling and medications were used in combination—resulting in an increase in cessation rates up to 82% (Babb et al., 2017; Knox, 2017).
The quitline employs behavioral counseling as an element of the service. The behavioral counseling that the quitline provides can double the cessation rates (Knox, 2017). Gordon et al. (2010) discovered that referring smokers to the quitline either through a brochure with the quitline number or by a faxed referral sheet, were equally effective. For example, the cessation rates for both quitline referral methods demonstrated similar results at the 12-month evaluation. Saul et al. (2014) found that when quitline counselors proactively contacted smokers after referral, cessation rates were higher than when the smoker contacted the quitline themselves. Therefore, evidence suggests that incorporating the use of quitlines into an individual’s cessation plan increases success rates; however, when counselors initiated the contact a higher rate of smoking cessation was achieved (Whittaker et al., 2012).
Cessation Interventions
There are a number of ways to connect workers to the quitline. Workers can be referred using the 5A’s (Ask–Advise–Assess–Assist–Arrange) method, the AAR (Ask–Advise–Refer) method, or the AAC (Ask–Advise–Connect) method. The 5A’s and AAR both rely on the smoker to contact the quitline while the AAC connects the smoker to the quitline (Vidrine et al., 2013). All quitline referral methods have been found to increase the quit rates at 3-month and 12-month follow-up when compared with traditional counseling alone (Gordon et al., 2010). Vidrine et al. (2013) found the AAC to be more effective than the AAR in connecting patients to the quitline, suggesting a 13-fold increase in quitline access. Regardless of the access method, research suggests that quitlines increase smoking cessation rates. Findings also suggest that cessation rates double when tobacco quitlines are utilized and triple when quitlines are used in conjunction with NRT or pharmaceutical aids (Knox, 2017).
Quitlines are utilized by more than 400,000 tobacco users each year in the United States and are available in all 50 states (Saul et al., 2014). However, this represents a low number of referral candidates to quitlines. This relatively low number may be due to lack of provider knowledge and awareness regarding the ease of referral to the quitlines (Lichtenstein et al., 2011; Marshall et al., 2017). Many patients are not being referred, or if they are receiving referral information, they are not contacting the quitline (Vidrine et al., 2013). Barriers such as time constraints on providers, lack of staff motivation, and poor provider/staff training may affect the number of smokers being referred to the quitline (Cantrell & Shelly, 2009). Although Vidrine et al. (2013) discovered that referral rates are low, 68% of those who were connected to the quitline by AAC had an interaction with the quitline. Thus, increasing their opportunity for success with cessation. Hence, reinforcing the importance of connecting the worker during their visit.
Role of Workplace and State Tobacco Control Policies
Researchers suggest that workplace smoking policies and cessation programs increase quit rates (Ham et al., 2012). Tobacco control policies in conjunction with cessation programs such as quitlines, NRT, and prescription medications, increased cessation success rates (Dahne et al., 2017). Employees have approximately a 2 times greater likelihood of cessation when working in environments with comprehensive smoke-free workplace policies in effect compared with those without smoke-free policies (Dahne et al., 2017). Therefore, companies can increase cessation attempts by establishing smoke-free policies along with quitline referrals using AAC, along with traditional smoking cessation strategies.
Barriers to Referral
Barriers exist regarding the process to connect patients to the quitline. Greenwood et al. (2012) explain that lack of staff and provider training on the importance of the quitline as a referral was a factor in accessing the quitline. Difficulty with the referral process, lack of a support system, and dated technology can serve as barriers often leading to dissatisfaction with the process (Cantrell & Shelly, 2009). Referral to the quitline was also impeded by limited provider to patient interaction and time to initiate the referral (Whittaker et al., 2012).
An additional barrier noted was that certain groups were more likely to be targeted for cessation interventions. For example, investigators found that referrals to quitlines were often targeted to higher income patients (Whittaker et al., 2012), while others found that younger smokers were less frequently targeted for referral to quitlines (Jamal et al., 2012). This is especially concerning because research suggests cessation programs can be highly successful in smokers younger than 35 years of age (Pierce et al., 2012).
Problem Statement
Tobacco abuse is a widespread problem in the rural, low income populations, such as the rural Appalachian residents in Tennessee (CDC, 2018b). Of those who smoke in this population, a daily smoking rate as high as 88% has been found (Pinsker et al., 2015). Despite the decreased prevalence of smoking in the general population, smoking rates in rural, low income groups do not reflect this diminishing pattern (CDC, 2018b). Rural Appalachian residents have a disproportionately higher nicotine use when compared with the rest of the United States (CDC, 2018b). In addition, this population has an increased risk of health disparities that include comorbid conditions, secondary to the negative effects of tobacco use (Graves et al., 2015).
Elevated tobacco use was found to be widespread at an automotive manufacturing plant located in rural Tennessee, which led the management team at the manufacturing plant to explore smoking cessation as a means to a healthier workforce. To address the large number of employees who smoked, a process improvement project was implemented at the onsite, nurse practitioner–managed, employee health clinic. The goal was to increase the number of referrals to the national quitline, 1-800-QUIT-NOW, as an adjunct to traditional smoking cessation strategies.
Methods
The primary outcomes we aimed to measure for this project were the number of workers assessed for smoking status at each clinic visit, the number of workers advised on the need for cessation, and if interested, referred to the national quitline. Ask–Advise–Connect method was employed to decrease the barriers patients face with connecting to the quitline (Vidrine et al., 2013). Workers who were referred to the quitline were followed monthly for a period of 4 months to determine whether they utilized the quitline. A secondary outcome was smoking cessation or decrease in the number of cigarettes smoked.
Setting and Population
The project occurred at the onsite nurse practitioner–managed clinic at an automotive manufacturing plant located in rural Tennessee. The clinic services are available to approximately 800 employees and their dependents. The clinic operates Monday through Thursday and is staffed by two nurse practitioners and a medical assistant. The services are primarily used by the blue-collar employees. The project participants were a convenience sample of patients who utilized the services of the clinic. Consent for participation was obtained for the study and referral to the quitline. All employees who smoked (cigarettes, pipes, and cigars) and were above 18 years of age were eligible. The project began in September 2018 and concluded at the end of January 2019 (a 4-month period). Implementation of the project occurred after an expedited review and approval from the East Tennessee State University institutional review board (IRB).
Project Design
All employees and their family members have access to the clinic at no cost. The clinic services are a benefit provided by their employer. Each employee/patient that chose to utilize the clinic was assessed for smoking status at each visit by the medical assistant, and subsequently advised on the dangers and importance of cessation by the nurse practitioners. The patients who chose to participate in the smoking cessation program were connected to the national quitline (1-800-QUIT-NOW), as well as being offered traditional smoking cessation strategies such as pharmaceutical therapy (Chantix, Zyban, and/or NRT) at no cost regardless of their participation in the study. These medications were prescribed by the nurse practitioners which is the standard of care in the clinic.
Data Analysis
Data were extracted from the electronic health record (EHR) to determine the number of smokers involved in the project. This was achieved by evaluating the total number of tobacco cessation visits that were conducted and the subsequent percentage of those who enrolled in the study. Electronic health record was used to evaluate those who smoked and those who were interested in cessation. It was also utilized to obtain the number of patients who: (a) smoked, (b) participated with the AAC method, that included the quitline referral, (c) obtained pharmaceutical assistance to quit smoking, and (d) were successful at quitting smoking or decreasing the number of cigarettes smoked per day. We followed workers for 4 months (September 1, 2018–January 31, 2019) to assess cessation rates or a decrease in smoking. All data were self-reported. Descriptive statistics were used to analyze the primary and secondary outcomes using Microsoft Excel for Office 365 by the project coordinator.
Results
The clinic provided 102 tobacco cessation counseling visits to the patients who were identified as smokers during the 4-month project evaluation. During that time, 24 employees indicated that they desired to quit smoking and were enrolled with the national quitline, resulting in a 23.5% (n = 24) participation rate in the smoking cessation program.
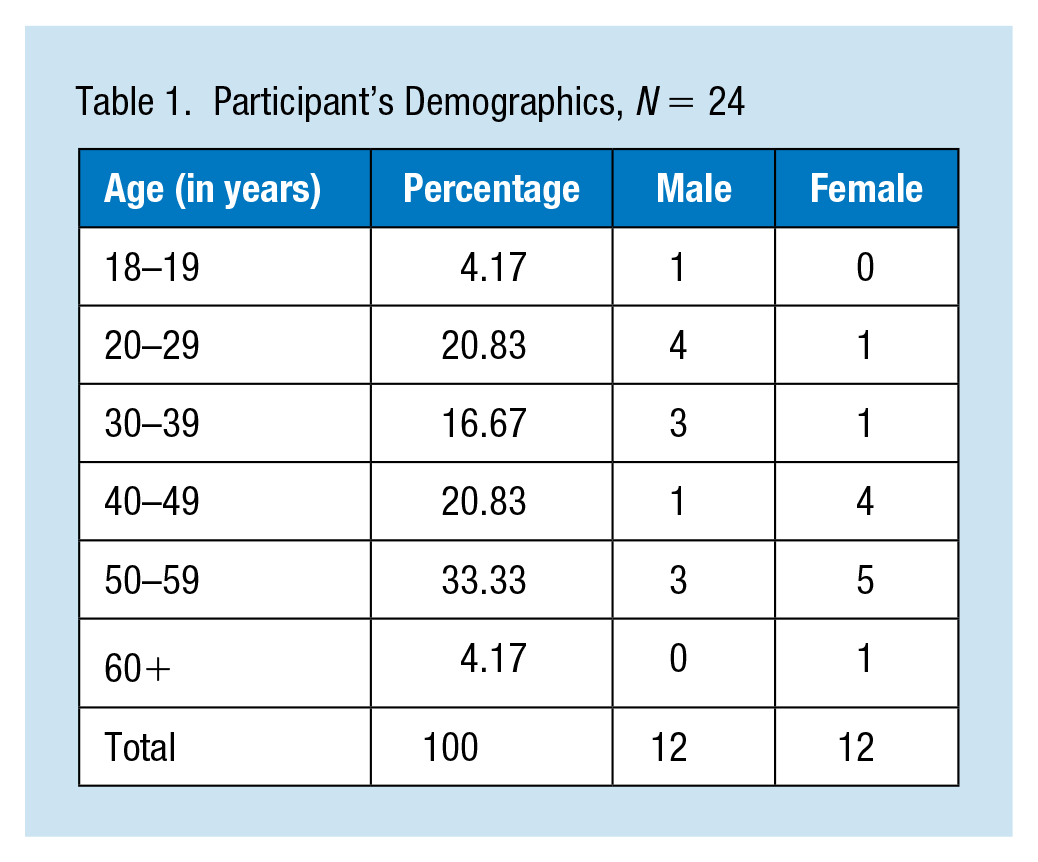
The mean age of the participants was 42 years (SD = 13.51), ranging from 18 to 63 years of age (Table 1). The total number of participants was (N = 24) including 12 women and 12 men. All the participants were Caucasian, blue-collar employees. The majority (66.7%) of the participants utilized the medications offered (e.g., Chantix, Zyban, and NicoDerm patches). Of the medications offered, Chantix was utilized by 54.2% and NicoDerm patches by 12.5%.
Participant’s Demographics, N = 24
Overall, the 24 employees enrolled in the cessation program reported a cessation rate of 12.5%, and 21% had a decrease by 50% or more in the number of cigarettes smoked. Of the participants, 33.33% quit or significantly decreased the number of cigarettes smoked per day. For those able to quit smoking, 66.7% used medication. Although all 24 participants (N = 24) were connected to the national quitline by faxing an enrollment form, the rate of participation with quitline counselors was 12.5% (n = 3). Among these three participants who used the quitline one individual was able to quit resulting in a cessation rate of 33.3%.
Discussion
The implementation of the AAC method as part of a smoking cessation program at an onsite nurse practitioner–managed clinic for an automotive manufacturing plant had positive results. All employees who utilized the clinic were assessed at each visit for their smoking status and counseled on the dangers of smoking and the importance of cessation. The smokers who were interested in smoking cessation were offered pharmaceutical assistance at no cost and were connected to the national quitline (1-800-QUIT-NOW). The blue-collar workers who were interested in cessation were found to be receptive to the quitline referral.
Of the participants, 33.33% had a decrease of at least 50% in the number of cigarettes smoked or were able to achieve cessation. The significant decrease in the number of cigarettes smoked a day is considered a success because the decrease will improve a smoker’s health (Begh et al., 2015). Monetary incentives may have been helpful to those employees achieving total cessation. The plant’s insurance policy premium was structured so that employees who are nonsmokers receive a reduced insurance premium of US$75.00/month for an annual savings of US$900.00. Monetary incentives have been used in the community setting to help smokers quit (Cahill & Perera, 2011; Hahn et al., 2004). However, it is unclear what impact, if any, the monetary reward had on cessation. Employees reported reasons for lack of participation with the quitline were found to be lack of time, poor internet connection, and the participants were unsure of the caller and did not answer the phone.
Limitations of the Project
A limitation of this study is that all data regarding cessation and decrease in the number of cigarettes smoked was self-reported. The study also occurred during the fall/winter months which is typically a period of absence from work and clinic utilization due to vacations, plant closure, and the holiday schedule. The lower utilization could have influenced the number of cessation visits provided.
Implications to the Occupational Health Nurse
Smoking cessation continues to be an essential component for improving an individuals’ health. Providers in the occupational setting develop close relationships with the employees and can provide smoking cessation counseling to include quitline referrals that increase the employees’ opportunity for successful cessation. By incorporating the AAC method to the smoking cessation program, this onsite factory clinic was able to assist their employees in cessation and decreasing their cigarette consumption. Subsequently, improving their health and lowering their health risk factors associated with smoking. This reflecting the goal of occupational nurses of developing a healthier workforce.
Conclusion/Applying Research to Practice
The occupational health-nursing provider can address smoking cessation at every patient contact. By continually addressing this health risk and providing resources to assist with smoking cessation, the patient has an increased opportunity to attempt and subsequently achieve cessation. The implementation of the AAC method to a workplace cessation program provides behavioral support for the smoker as they begin cessation. The addition of the quitline to patient cessation attempts increases the smoking cessation rate, which is the goal for improved employee health. Thus, demonstrating the role of smoking cessation instruction for the occupational health nurse.
Overall, the implementation of the AAC method as part of the smoking cessation program had limited success. As smoking cessation is difficulty to achieve, any success greater than 7% seen nationally can be considered an achievement (Hughes et al., 2004; Jamal et al., 2012). The 12.5% cessation rate with the participants was above the national average. Thus, demonstrating the benefit of having a workplace cessation program and the benefit of incorporating the AAC method to the current smoking cessation program.
Application to Occupational Health Nursing Practice
The occupational health nursing provider can address smoking cessation at every patient contact. By continually addressing this health risk and providing resources to assist with smoking cessation, the patient has an increased opportunity to attempt and subsequently achieve cessation. The implementation of the AAC method to a workplace cessation program provides behavioral support for the smoker as they begin cessation. The addition of the quitline to patient cessation attempts increases the smoking cessation rate which is the goal for improved employee health. Thus, demonstrating the role of smoking cessation instruction for the occupational health nurse.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Julia Blocker, DNP, FNP-BC, is a family nurse practitioner who has been serving the rural Appalachian population for 19 years. She received her MSN and DNP from East Tennessee State University. She is devoted to improving the health and well-being of this population.
Janice Lazear, DNP, FNP-C, CDE is an associate professor at East Tennessee State University. She has a BSN from Ohio State University and a master’s degree from UCLA with a focus on the perinatal clinical nurse specialist role and higher education. She also completed a family nurse practitioner post-master’s program and Doctor of Nursing practice program at the University of Maryland. She has clinical experience in high risk obstetrics, primary care and diabetes care and is a certified diabetes educator.
Lee Ridner, PhD, FNP-BC, is a professor at the University of South Alabama College of Nursing. He has studied tobacco related health risks for nearly 20 years and teaches smoking cessation techniques for primary care patients.