
Abstract
Work-related stress can negatively impact health care providers’ (HCPs) ability to provide care. We examined the sources of work-related stress experienced by HCPs who provided medical care for people living with HIV/AIDS and the impact of the stress on HCPs’ well-being and work performance. We conducted in-depth interviews with 46 HIV/AIDS HCPs in Guangxi, China. The interviews were audio-recorded, transcribed, and imported into NVivo V.11 for data management and data analysis using a thematic approach. We found that the key sources of stress at work included general work-related sources and HIV/AIDS-related sources. All stress was seen to have a substantial impact on the HCPs’ individual well-being, family and social life, and quality of care they provided. We recommended that government and health care facilities should take measures to improve institutional culture and professional development for HIV/AIDS HCPs. More professional training schemes should be provided to strengthen HCPs’ competence, improve universal protection from occupational exposure, and reduce the stigma toward HIV/AIDS patients and their care providers.
Introduction
Stress has been identified as an important factor which can affect individual well-being and professional development. Work-related stress may contribute to negative outcomes, including burnout and poor work performance (Quick & Henderson, 2016) and ultimately result in negative issues for the employers. For health care providers (HCPs), their work-related stress in clinical settings is often related to the quality of care they provide to their patients. According to the World Health Organization (WHO), health services should include competent and motivated health care professionals, effective communication, and community engagement to achieve desired health care quality (WHO, 2018). Thus, the HCPs’ well-being, working competency, effective communication, and passion are a necessity, in part, to achieving the desired health services outcomes (Graham, James, & Spertus, 2018; Waqas et al., 2015).
Current research shows that work-related stress may have a negative impact on HCPs’ well-being, daily life (P. Sun et al., 2017; Tong et al., 2018), patients’ medical outcomes (Schroder et al., 2016; Sigsbee & Bernat, 2014), and precision in medication administration (Salam et al., 2019). Stress is a risk factor for cardio-metabolic diseases and is associated with altered metabolic profile and increased systemic inflammation (Loerbroks et al., 2017). Besides the impact on physical health, stress is also proven to be related to the risk of decreased work performance and reduced work ability (Schroder et al., 2016). Stressful work environment may cause the HCPs to change jobs or even quit the practice earlier than planned (Ahsan, 2011).
Existing research has largely focused on general work-related stress among HCPs, such as workload, work demand, work environment and staff shortage (Qiao et al., 2016; Zheng et al., 2014) but not much on stress that is related to a specific patient medical condition, such as human immunodeficiency virus (HIV) infection or acquired immune deficiency syndrome (AIDS). People living with HIV/AIDS (PLWHA) often experience both deterioration of physical health and elevation of psychological stress resulting from the infection, as well as associated stigma and discrimination (W. Sun, Wu, Qu, Lu, & Wang, 2013). As a result of immunosuppression, these patients may also have comorbidity or opportunistic infections, such as extrapulmonary tuberculosis (TB; Naing, Mak, Maung, Wong, & Kassim, 2013), oral human papillomavirus infection (Beachler & D’Souza, 2013), hepatitis B and/or C viruses (Zhang et al., 2017).
The complexity of medical conditions and challenges of PLWHA physical, psychological, and social situations, as well as the large number of PLWHA could possibly contribute stressful work situations for health care workers caring for these patients (Qiao et al., 2016). In 2014, the Joint United Nations Program on HIV and AIDS (UNAIDS) set the “90-90-90” target aiming to diagnose 90% of all PLWHA, provide antiretroviral therapy (ART) for 90% of those diagnosed, and achieve viral suppression for 90% of those treated by 2020. This target could result in 81% of all PLWHA on treatment and 73% of all PLWHA achieving viral suppression (UNAIDS, 2014). Since 2015, the updated WHO guidelines for antiretroviral treatment have extended the treatment to all HIV-infected patients, irrespective of the level of immunosuppression and the CD4 count (Tshikung & Calmy, 2016). In align with the recent treatment strategies, most of the treatment and care of HIV/AIDS takes place at community-based facilities where many HCPs may not have adequate training schemes on how to care for the complex medical conditions (Ma et al., 2015).
Advances in treatment have improved survival rates in HIV-infected individuals, and AIDS has been shifted from a fatal disease to a chronic illness (Huang, Tian, Dai, & Ye, 2013). At the same time, the expanded access to treatment and the lifelong care for patients with possible opportunistic infections, side effects, comorbidities, and psychosocial vulnerability post significant demands and challenges to the health care professionals who provide HIV/AIDS clinical care, especially in resource-poor settings (Lekas, Siegel, & Leider, 2011).
In spite of the documented challenges associated with HIV/AIDS treatment and care, there are very few studies focusing on HIV/AIDS HCPs’ working experiences. Therefore, the main purpose of this study was to qualitatively examine the sources and the impact of work-related stress among HIV/AIDS HCPs to inform future efforts to improve the HIV/AIDS health care quality in China and other resource-poor settings.
Methods
Research Site
We conducted this study in Guangxi Zhuang Autonomous Region (Guangxi), China. The number of PLWHA is growing in China (Niu, Luo, Liu, Silenzio, & Xiao, 2016). In September 2018, the official number of PLWHA in China was 850,000; however, it is believed to exceed more than 1.2 million with 30% who may not know they are infected (Liu, 2018). Guangxi reported a total of 124,282 HIV/AIDS cases as of December 2017, representing a 78.70% increase since June 2011 (69,548 cases), placing Guangxi third among China’s 31 provinces in terms of the documented seropositive cases (Guangxi Center for Disease Control and Prevention [CDC], 2018). In Guangxi, there is one designated primary public hospital (specifically its HIV/AIDS clinic) in each urban district/rural township that is working under the direction of the city/county CDC to conduct clinical management and semi-annual follow-ups for all HIV/AIDS patients in the district/township. These HIV/AIDS clinics served as the context of this study.
Participants
We recruited and interviewed a convenience sample of 46 HCPs from nine HIV/AIDS clinics in Guangxi in March 2018. Inclusion criteria included the willingness to participate in this research, working as a full-time HCP in an HIV/AIDS clinic for at least 1 year, and providing medical service to patients with HIV/AIDS directly. All the participants provided written informed consent before participating in face-to-face interviews.
Interview Guide and Themes
A team of trained interviewers conducted in-depth individual interviews using a semi-structured interview guide. We developed the initial interview guide based on existing literature pertaining to stress in HCPs. We then revised the guide based on input from experts and research staff in Guangxi CDC through informal discussions. The final interview guide consisted of open-ended questions and supporting probes covering several topics, including (a) demographic information; (b) perceived or experienced stress from both general work-related sources and HIV/AIDS-specific resources; (c) perceived or actual impact of the stress; (d) perceived social support and other strategies in coping with stress from both sources; and (e) suggestions on means of reduction of stress from both sources.
Interview Procedures
We conducted individual interviews in private rooms at the HIV clinics where the participants were recruited. The five interviewers (three women and two men) were researchers with a master or doctoral degree in nursing, public health, or psychology. All the interviewers had received extensive training on qualitative methodology, research ethics, and general skills of in-depth interviewing. The interviewers approached potential participants at HIV clinics, described the study protocol, and assured the confidentiality of their responses. The interview took about 40 minutes on average. Our study protocol received ethic approval from the institutional review boards at the Guangxi CDC in China and University of South Carolina in the United States.
Data Management and Analysis
We conducted data collection and data analysis iteratively. All interviews were audio-recorded and transcribed in simplified Mandarin Chinese by the interviewers. We used NVivo V.11 (QSR International, Burlington, MA) to manage and analyze the data using a thematic approach (Grossoehme, 2014). We developed an initial coding framework and then categorized quote excerpts and coding memos by the boarder categories (e.g., sources of stress and impact of stress) on the basis of the themes and subthemes (see Figure 1). The following themes and subthemes from the interview guide were identified in the current analysis: (a) Sources of stress (general work-related and HIV/AIDS specific); and (b) impact of stress (e.g., impact on individual well-being, family and social life, and quality of care). We selected and translated representative quotes into English to illustrate key findings. The translations were verified by the research team and any disagreements were resolved through group discussions.
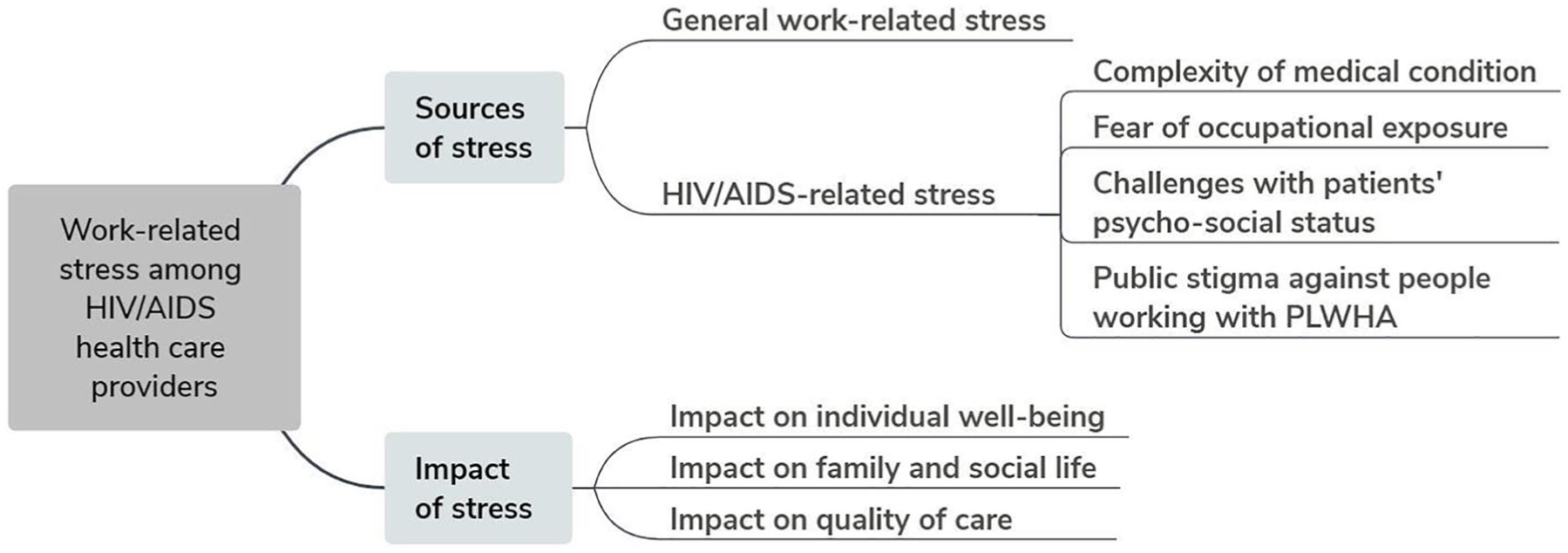
Themes of work-related stress among HCPs working with PLWHA identified in the data analysis.
Results
Sample Characteristics
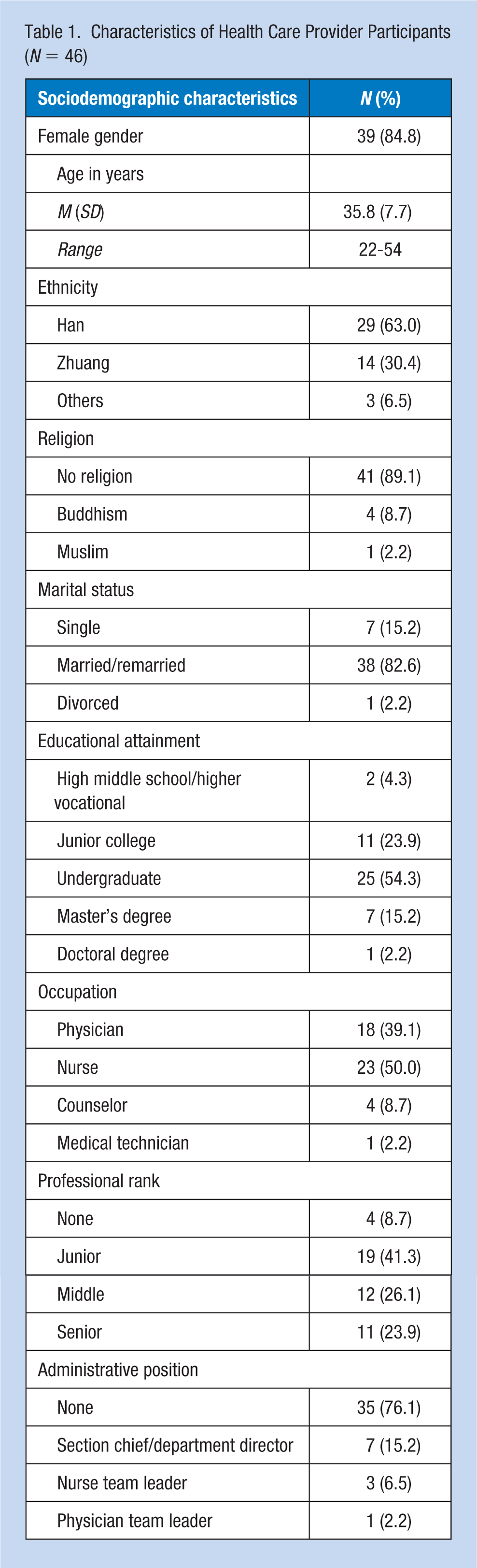
Details about the participants’ demographic characteristics are presented in Table 1. Among the 46 participants, 39 (85%) were women, and 33 (71.7%) had a college degree. The mean age was 35.8 ± 7.7 years, with a range of 22 to 54 years. The participants had worked in HIV/Infectious disease facilities for an average of 6.8 ± 6.45 years. One-half (n = 23) of the participants were nurses, and the remaining were physicians (n = 18) and other health care professionals (n = 5). A total of 29 (63%) were Han Chinese, and 38 (82.6%) were currently married. More than three quarters (76.8%) did not hold any administrative position.
Characteristics of Health Care Provider Participants (N = 46)
Sources of Stress
General work-related sources
During the interview, most of the participants reported stress that was caused by general work-related conditions such as heavy workload, working overtime, staff shortage, large patient volume, unrealistic work demands, and poor institutional culture. All these factors were interrelated and exacerbated the ongoing stress. Participants’ work days were often filled with patient care, clinical education, and medical or nursing documentation. Some of the participants said they could not stop to have a drink or go to the restroom. Considering the patient volume, they often needed to work overtime to finish the required work. Some of them planned or wished for a vacation but often could not do so because of staff shortages or increased work demands, as one participant highlighted, People in other occupations have weekends and holidays. But as physicians, we don’t have a vacation. During the Spring Festival [Chinese lunar New Year], I only had a break on New Year’s Eve and the first day of the new year. We are very tired, especially on holidays and festivals, because the patients who are admitted at this time are always in severe condition. (Female doctor, aged 41)
Unrealistic work demands referred to the manner through which the constant demands for high-quality medical service and frequent work-quality inspections were implemented. None of the participants questioned the need for, or the value of, high-quality medical services, but the demands and inspections were often implemented with personal threats, such as penalty or disciplinary actions. When a medical error occurred, the HCP would need to pay fines and their name would be posted on the hospital website. As a result, many HCPs would make every effort to cover up any medical errors, which in turn, resulted in additional stress to the HCPs, as one nurse highlighted, When we are busy, we work like a machine, some mistakes may be made without being noticed. Every month we have a discussion about nursing errors. If there are some mistakes in your nursing record, you will be charged some money to pay for your mistakes, maybe 100 yuan [Chinese currency, about half a day’s salary for a young nurse]. (Female nurse, aged 27)
Participants also mentioned if they wanted to have a professional promotion, research grants and publications were two of the most important criteria. But considering their heavy clinical responsibilities, promotion was extremely difficult for them.
Institutional culture included leadership style, relationships with colleagues and leaders, and working conditions. Among most of the participants, their relationships with colleagues was much better than that with leaders. A small proportion of participants complained that the leaders with poor management styles disturbed the daily routine. A few also made complaints that focused on the bureaucracy and personal power, which engendered a “survival of the fittest” culture: When making decisions on ward management, some of them [leaders] would ask for our advice some of them just gave orders and you can’t defy their decisions. When a new leader came, he or she would give us his or her own rules and demands which may be different from the existing ones. We have changed several leaders in the last two years. So far, we haven’t established stable work responsibilities, such as shift responsibility and time tables for different shifts. Some of them were not good at management and just copied practices from somewhere else without appropriate adjustment. (Female nurse, aged 26) There are some leaders who want to show their personal power. They assign others to a heavy workload. I don’t want to stay at this kind of unit. I hope leaders could be relatively fair, taking others’ needs into consideration, such as family issues or health problems. (Male doctor, aged 45)
However, one participant as a leader in an HIV clinic told the other side of the story but equally suggested the same problem of poor communication between workers and leaders. He thought he had devoted a lot of time to the work, but his fellow colleagues often did not appreciate what he had been doing. He said he doubted if his work was deserving of his effort. He also emphasized that the communication between workers and leaders needed to be improved.
HIV/AIDS-related sources
Many participants also reported stress that was specifically related to HIV/AIDS including the challenges associated with HIV/AIDS-related medical conditions, fear of occupational exposure, perceived public stigma against people working with PLWHA and difficulties incurred when working with PLWHA.
Complexity of medical condition
In our research, participants stated that PLWHA often had complex medical situations. The co-infection of viral hepatitis and TB among PLWHA made the treatment of HIV even more challenging, as there was a higher mortality and morbidity rate among PLWHA with co-infections. Patients’ families may not understand disease deterioration which may cause hospital disputes and violence. For example, one participant stated, I had an AIDS patient with lymphoma. His tumor was relatively large and we had already talked about the side effects before chemotherapy. But his complications appeared very quickly. On the second day of chemotherapy he encountered severe respiratory distress and failure. We did the resuscitation immediately but failed. His wife cried, his brother rushed over and blocked me in the corner. I was very scared and trembling the whole time. Physicians and nurses in our department have been beaten by patients or patients’ relatives several times so far. (Female doctor, aged 39) If the patient’s disease is complex, we may think over the correct treatment protocol the whole night. And I may feel chest tightness and insomnia sometimes. (Male doctor, aged 35)
Fear of occupational exposure
Most participants said they were worried about being infected with HIV at work. They said they may touch the patients’ body fluid while delivering invasive or noninvasive medical interventions in an emergency. In addition, lots of participants worried about being infected with TB. They thought that they would be safe from HIV exposure as long as they took precautions when in direct contact with the patients, but TB is air-borne and could spread through droplets. One participant said, Suppose the patient has a contagious pulmonary condition. Though he had received treatment in the hospital, I still worried a lot when he came to us for medication. (Female pharmacist, aged 37)
Some participants were worried about being infected with herpes or herpes zoster since these are contagious. They were worried about bringing these viruses back home to their children.
Challenges with patients’ psychosocial status
In our study, the interactions with PLWHA also presented some challenges to HIV/AIDS HCPs. Participants reported that some PLWHA were injection drug users. Drug users were at risk for committing suicide or doing harmful things to other people that put HCPs in high stress, as some participants said, The number of [HIV] patients who used drugs is now decreasing year by year. But they are still the hardest to treat. Once, three patients who used drugs were hospitalized in our ward for half a year. When the Chinese New Year came, they put a death ritual table in the room and “celebrated” their (future) death by singing and dancing; this seriously disturbed other patients’ treatment and life. They did not stop after our initial request, so we called the police, but even the police could do nothing with them. For drug users, their diagnosis of AIDS was just like an “imperial sword” or an “imperial yellow jacket” [symbols of highest honor in ancient Chinese culture that provide the individual with highest protection from an emperor]. (Female nurse, aged 39) For some drug users, especially those with low literacy, they wouldn’t follow physicians’ instructions. They left their syringe on the bed. When nurses made their beds, they could be stuck. It was very dangerous. Besides, blood veins of drug users were destroyed by frequently injecting drugs, so it was extremely difficult for nurses to find good veins. (Female nurse, aged 47)
Some participants said that it was stressful working with patients with poor psychological status. Health care providers said they often served as an emotional “trash can” for those patients because patients poured their bad emotions and negative experiences on them. Patients’ psychological status affected the HCPs, especially at the initial stage of diagnosis when many patients had emotional instability and may commit violence and/or suicide, as one participant said, It [the incident] wasn’t long after I came to this hospital. I was on the night shift . . . It was my first time to encounter this kind of thing, so I had a lot of stress. I was making my rounds at night, finding the patient was not in the ward. I began to look for him and called him . . . But we just found his shoes and a cup of water on the ground. Opening the window, we found he had jumped to his death. It was so fearsome that I couldn’t get to sleep for a month without turning on the light. His posture on the ground was always in my mind . . . (Female nurse, aged 28)
Participants also said that sometimes patients were abandoned by their family after the diagnosis of HIV/AIDS. They neither have care-givers nor can afford the medical expense. This situation demanded HCPs to take more time and energy to care for them, most of which would end up as voluntary and free. One participant said, Once we had a female AIDS patient who came from [another city], but she had a friend here. Her disease deteriorated suddenly when she was here. She was in a coma and was sent to our hospital by her friend. Her parents cut her off after she was diagnosed with HIV. The rescue was unsuccessful, and she died in our hospital. Because she didn’t have an ID card, and her parents and friend refused to sign the death certificate, her corpse remained in the hospital. The communication and coordination among the mortuary house, police, and her parents put me in great distress during that period. (Male doctor, aged 49)
Public stigma against people working with PLWHA
According to the participants, HCPs who took care of HIV/AIDS patients were often stigmatized by others both in and outside of clinical settings. Some participants said that they would not tell others about their job because of the stigma or lack of respect from others. Several nurses and physicians said they could not find life partners because of the stigma associated with their work. Further, many other medical staff avoided contact with HIV/AIDS HCPs, as some participants highlighted, I have many [non-physician] friends. Some of them may know something about HIV/AIDS, but most are worried that I would transmit HIV to them. They have different viewpoints about this problem [HIV]. When they introduce me to others, they just say “This is my friend.” They will not tell my job to others, because others may be afraid. And they deem that my work is dirty. (Female doctor, aged 41) When we accompany our [HIV] patients to an invasive examination which needs a medication infusion before the procedure, those physicians [in the examination center] will refuse to do it for us. Our section director and physicians have reported the situation to the leaders of our hospital, but no improvement happens. So many of us want to work in other departments. Once a nurse in our department went to the Department of Obstetrics to consult about giving birth to a baby, she was observed [by the staff in the Department of Obstetrics] from head to toe, and she thought she was treated with discrimination. (Female nurse, aged 29) Once our nurse went to the pharmacy to get some medication, when the pharmacist saw the tag “HIV/AIDS clinic” on the basket, they shouted “Put your medication basket on the ground not on the table.” (Female doctor, aged 37)
Impact of Stress
Impact on individual well-being
Many participants had physical complaints including digestive disorders (e.g., losing appetite and stomach discomfort), cardiovascular disorders, sleep disorders, and poor immunity function. Some nurses complained about backaches from prolonged standing to draw blood samples. Some physicians complained about shoulder and neck pain from spending too much time working at a desk. Some participants also complained about poor immunity function with symptoms of fever and extreme tiredness. In addition, some said they felt short of breath, had sleep disturbance (e.g., nightmare and insomnia), and sleep deprivation, which they attributed to work stress, as one participant reported, When I think of the heavy workload of the next day, I can’t fall sleep. Insomnia happens about twice a week. The workload gives me lots of stress. I couldn’t sleep, so I take some sleeping pills . . . such as diazepam and alprazolam. (Female nurse, aged 28)
Furthermore, many HCPs, especially men, complained about cardiovascular symptoms, such as high blood pressure, tachycardia, and premature heartbeat as the result of their stress or heavy workload, as one reported, Our clinicians have many cardiovascular diseases, such as high blood pressure. And many of us look fat. That is not because we don’t know how to control weight but because our endocrine function is affected as a result of the work. When we are on the night shift, we rescue the patients and do a lot of work, so we need to eat something, that is why we are fat and it is hard for us to lose weight. (Male doctor, aged 49) Sometimes my heartbeat is fast and irregular. I can feel it when I am tired, after a night shift, or no sleep after night shift. I know we need some exercise, but after work, we are too tired to do exercise. (Female nurse, aged 33)
Participants, especially the young female HCPs also thought that stress at work had a significant impact on their psychological health, such as emotional instability, irritability, annoyance, and depression, as some participants said, I had mood fluctuation; sometimes I felt sad suddenly. I don’t know why. I felt that I didn’t like anything around me. I felt depressed and had no interest in anything. (Female nurse, aged 34) I don’t think I can live as happily as someone else. Stress is always there, I don’t feel relaxed. I feel stressed all the time. (Female nurse, aged 28) Sometimes I want to cry because of inexplicable anxiety, but if I divert my attention, it will be better. I live alone. Sometimes when I get back home, I feel upset and even sad. (Female nurse, aged 29)
Most of the participants expressed sadness. When one of them was asked about the impact of stress on health during the interview, she started crying without saying anything. Another participant connected such feelings with the sudden death of another physician: One doctor, a friend of my colleague, died suddenly some time ago. He had a fruitful career and published a lot of papers. That was terrible. How much did he devote himself to the work? The doctor couldn’t cure himself. (Female doctor, aged 39)
Impact on family and social life
Work-related stress had a negative impact on HCP’s individual well-being and also affected their family and social life. Many participants reported that family life was always affected by their busy work, emotional experiences, and negative experiences at work. Busy work also resulted in a limited social networking for the HCPs. They devoted less time to family and that caused family quarrels or estranged relationships, as some middle-aged female participants highlighted, When my family plan to have fun in the park . . . they never ask me. When they want to drink morning tea, they will not ask me, either. Because they think I am busy. Truly I am not available, because I need to make ward rounds every day. (Female doctor, aged 40) I devoted less time to my family because of my job. My child often complained that I didn’t have time to accompany him. He said his classmates had trips and played basketball with their families. But I don’t have time to do these activities with him. I have rarely taken part in his parent-teacher meetings. Once we planned a trip but had to cancel it at the last minute because of some urgent work assigned from the hospital. He was very disappointed with me. (Female doctor, aged 41) I think if you are a doctor, you don’t need to buy a car and a house. You don’t need to give birth to children, and you don’t need to get married, either. Because you will not be able to devote much to your family. (Female doctor, aged 40)
Most HCPs said the negative impact on family life was due to feeling tired and their work-related emotional instability.According to the participants, most of them tended to release their negative emotions from work onto their spouse and children. Children’s mischief or naughty behaviors caused shouting, criticism, and even beatings: The stress may affect my life. Because of the bad emotions we have at work, we could not release to others [but family]. When we get off work, we just pour it out to our families. For example, if the floor is not clean, I will shout out to my husband. I become irritable, which affects my relationship with my family. (Female nurse, aged 32)
Many participants said they spent less time socializing with friends. When they felt stressed, they had few friends to ask for help or talk to, so they just dealt with the hard times alone. One participant said during the interview, I have been a doctor for more than ten years. In my opinion, a doctor’s job is a doctor’s life. He or she has no time to socialize [with others]. (Female doctor, aged 41)
Impact on quality of care
The quality of care which required full engagement of HCPs was often affected by work-related stress. Some participants thought that long-term and accumulated stress caused poor work performance and even burnout. With emotional and mental discomfort, they may have no intention to communicate with patients: If my stress continued, my work would be affected. I could not focus on my work and I did my work very slowly. It also made the occupational exposure much more likely to happen. (Female nurse, aged 34) Now we have a lot of work to do. We have little time to talk with the patients. Mental care, diet and exercise guidance and medication compliance education were not well completed. (Female nurse, aged 26) If I was in a bad mood, I would not speak much . . . My emotions will affect my interactions with the patients and it may cause a dispute [with the patients]. (Female nurse, aged 32)
Some of the participants also mentioned burnout, and they said they were often emotionlessness toward work and patients. In addition, they were not willing to take part in institutional activities, and they lost passion toward work. One participant said, Sometimes I take a negative attitude toward my job. For example, I am not willing to take part in department activities. I feel tired. (Female nurse, aged 32)
Some participants thought that stress affected their self-development. One of them said that stress made him doubt his own decision-making ability. He used to make decisions directly, but now he is always worried about making mistakes. Moreover, they thought that stress caused worse relationships between work staff and leaders. They would avoid communication as a result of feeling depressed and being afraid to cause conflict, as some participants stated, The stress between our leaders and us could affect our further communication. There is a gap between us. And we need to be careful about doing things or speaking. (Female nurse, aged 26) Sometimes the young physicians treated the patients improperly. I would criticize them. If I failed to control my temper, they may feel hurt. I felt sorry after criticizing them, because they have put a lot into their work. I think they hate me. (Male doctor, aged 49)
Discussions
The findings from this study indicate that in addition to general work stress, HIV/AIDS-related factors also contribute to stress among HIV/AIDS HCPs. Stress from all sources accumulate, interact, and cause a very negative impact on HCPs physical health, emotional and mental health, and their family and social life. The stress also contributed to poor quality of care, inadequate professional development, and inharmonious institutional culture. Thus, we recommend that a great effort from the individual, the institution, and government levels should be taken to minimize the sources of stress, to relieve the negative impact of stress, and to promote HCPs competency to cope with the stress.
The government can play an important role in resolving the sources of work-related stress for HIV/AIDS HCPs. In our research, HIV/AIDS HCPs have stress which may be different from the general medical care population in China (Yao, Wang, Wang, & Yao, 2014; Zhu, Rodgers, & Melia, 2014). HIV/AIDS HCPs not only provide a medical service but also deliver psychosocial support for AIDS patients and their families (Benevides-Pereira & Das, 2007). Work-related fatigue was most common among HIV/AIDS HCPs as a result of work intensity and personal health status (Dawson & Fletcher, 2001; Ho et al., 2013). Fatigue affected HCPs’ neurocognitive functioning and hindered their work performance (Han, Trinkoff, & Geiger-Brown, 2014). Therefore, it is imperative for the government to take measures to increase the number of adequately trained HCPs into HIV/AIDS workforce so as to relieve the imbalance between demands of patients care and number of HCPs and pay attention to HCPs’ physical and psychological well-being. The government could also employ job specific criteria for evaluation and promotion of HCPs. For example, those who worked in clinical settings, especially in community-based clinical facilities, should be evaluated more on their competence and expertise in clinical practices, but less on research grants and scientific publications.
HIV-related stigma in clinical settings is a broad social phenomenon (Chambers et al., 2015). Stigma could affect HIV/AIDS HCPs’ self-identity and professional value. It is harmful for the stabilization, work performance, and professional development of HIV/AIDS medical workforce. The stigma associated with working with HIV/AIDS patients in China may be a result of several factors. First, there was a lack of necessary knowledge on HIV/AIDS. For many Chinese, especially those in the remote and rural areas (such as Guangxi), HIV infection is still dangerous and fatal. Therefore, they might choose to distance themselves away from HIV/AIDS patients and the people working with those patients. Second, there was insufficient knowledge and policy/procedure of universal precautions and post-exposure prophylaxis in medical settings (Li, Liang, Wu, Lin, & Wu, 2008). Third, some elements of the Chinese traditional culture such as Confucius culture may induce stigma. Under the strong influence of Confucianism, Chinese traditional culture emphasizes familial responsibilities. People who were infected through extramarital or premarital sexual behaviors and homosexual behaviors were often seen immoral or lack a sense of responsibility. Some people may view the individuals (or professions) working with these patients as “inferior” in social status.
Findings from our research indicate that a number of strategies to address the HIV-related stigma should be identified including social support, education, self-efficacy, resilience activities, and advocacy. The government could strengthen public education to reduce stigma, including stigma against both PLWHA and their HCPs. The government should also recognize and reward the contribution of HIV/AIDS HCPs. The sense of self-value among HIV/AIDS HCPs could help them mitigate the effect of stress. Previous research showed that a lack of a sense of personal accomplishment contribute to frequency of burnout. Rewards in the form of recognition and support from management may positively influence the institutional culture (Wang et al., 2014).
Some improvement in the institutional culture could help HCPs deal with work-related stress. Previous research has suggested that a transparent, fair, respectful, and supportive institutional culture is crucial for effective communications between HCPs and their leadership (Riley et al., 2018). The negative institutional climate found in our study may be the result of Chinese hierarchical power structure. The institutional culture in China is largely based on command-and-control, top-down management, or authoritarian leadership. This model of management may result in inadequate communication between leaders and employees and is especially damaging in the health care area when collaboration improves care. On one hand, employees need support from leaders to accomplish their creative thinking on quality improvement. On the other hand, leaders, especially new leaders, need a lot of support from their employees to have an effective management. Input from employees is especially crucial because they interact with patients directly (Shuai, Chen, & Jiang, 2011). However, worries of being isolated or being blamed make employees hesitant to speak out their thoughts or opinions. This indicates that both employees and leaders could benefit greatly from a supportive institutional culture.
In our research, care for HIV patients with complex physical, psychological, and social conditions was identified as a source of stress. This finding calls for the institution to provide holistic treatment and care to HIV patients, not only medically but also considering their psychological, financial, and family status (Ratanawongsa et al., 2012). Thus, to address the multiple needs of these patients, institutions need to establish professional teams, which could include physicians, nurses, physical therapists, social workers, and psychological counselors. A team of qualified staff are the basis of health care quality, and it will also help relieve the stress of HCPs.
In addition, our research shows that some measures should be taken to improve HCPs’ professional competency to help them deal with stress, such as professional training schemes aimed at improving their competency to treat complexity of disease, preventing occupational exposure and establishing a timely and effective monitoring process after the exposure. Some training programs on time management and coping strategies are useful for them to cope with work-related stress.
Strength and Limitation
This is one of the few qualitative studies that focused on HIV/AIDS HCPs’ work-related stress in China. The findings regarding HIV/AIDS-specific work-related stressors among HCPs help us to understand their working experience and search for more effective coping strategies to help them to relieve stress in clinical settings and improve care quality. However, this study has several limitations. First, we applied convenience sampling and our participants only came from Guangxi, so the sample may not be representative of the HCP population in other places. Second, we did not compare the stress experienced by gender and age group because of relatively small sample size in each age-and-gender stratus, although our data may suggest that middle-aged female HCPs were experiencing more work-family conflict, while young female HCPs suffered more emotional impact from work-related stress.
Implications for Occupational Health Nursing
The findings in this study have some implications for clinical practice, occupational development and well-being of future HCPs. By recognizing the importance of health of nurses and other HCPs from the perspective of delivering high-quality health care to PLWHA, working conditions can be improved to respond to individual workers’ stress reduction. Health care systems and their administrators should pay attention to nurses’ physical and psychological well-being. Public education to reduce stigma in clinical settings is urgently needed. These findings can also be used to inform the professional development and educational activities for nursing professionals programs, like honoring HIV/AIDS health care workers and establishing rewards system could be effective to promote their sense of self-value. In addition, other health care professionals (such as psychological counselors and social workers) should be involved in the AIDS treatment and care continuum to improve the quality of the care. The health care institutions could establish a transparent, fair, respectful, and supportive culture to reduce HCPs’ work-related stress. The health care facilities could also offer them the necessary in-service education and training about policy and procedure on occupational exposure and stress reduction.
Conclusion
Results of this study illustrate the sources of stress from both general and HIV/AIDS-related sources and their impact on HCPs’ physical, social, and mental health. Moreover, the stress and their negative impact on individual well-being could result in poor work performance and retrogressive self-development. This research could help researchers and health care systems to identify various sources of stress and promote HIV/AIDS HCPs’ well-being, which is the basis for medical care quality improvement. It is recommended that government and health care facilities should take measures to improve HIV/AIDS workforce and institutional culture. More professional training schemes should be provided to strengthen HCPs’ competence and protect them from occupational exposure. In addition, public education is urgently needed to reduce HIV/AIDS-related stigma toward both PLWHA and their HCPs. Holistic care approaches to meet HIV/AIDS patients’ mental, physical, and social needs could relieve stress among HCPs as well.
Applying Research to Practice
The findings in the current study have some implications for clinical practice, occupational development, and well-being of HCPs. By recognizing the importance of health of HCPs from the perspective of delivering high quality health care to PLWHA, working conditions can be improved to respond to individual workers’ stress reduction. Health care systems and their administrators should pay attention to HCPs’ physical and psychological well-being. Public education to reduce stigma in clinical settings is urgently needed. These findings can also be used to inform the professional development and educational activities for HCPs, like honoring HIV/AIDS health care workers, and establishing rewards systems could be effective to promote their sense of self-value. The health care institutions could establish a transparent, fair, respectful, and supportive culture to reduce HCPs’ work-related stress. The health care facilities could also offer HCPs necessary in-service training about policy and procedures on occupational exposure and stress reduction.
Footnotes
Acknowledgements
The authors thank Wenjia Liu, Chen Chen, and other research team members for their contribution to data collection. The authors also thank Ms Joanne Zwemer for assistance in manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the National Institute of Health grants R01HD074221 and R01MH0112376 and Guangxi University of Chinese Medicine Grant 2016QN002. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Health.
Author Biographies
Huiru Tong, MSN, RN, is a faculty member and a chief nurse at Guangxi University of Chinese Medicine. Her research interests include nursing education, health promotion for medical professionals, and HIV prevention.
Xiaoming Li, PhD, is a professor and Endowed Chair in the Department of Health Promotion, Education, and Behavior, and director of South Carolina SmartState Center for Healthcare Quality, at the University of South Carolina Arnold School of Public Health. His research interests include HIV behavioral prevention intervention, HIV stigma, and HIV treatment adherence.
Shan Qiao, PhD, is an assistant professor at the University of South Carolina Arnold School of Public Health, Department of Health Promotion Education and Behavior. Her research focuses on HIV prevention and treatment, global health, health promotion interventions, and program evaluation and implementation.
Yuejiao Zhou, MD, is the Deputy Director for the Institute of HIV/STD Control and Prevention at Guangxi Centers for Disease Control and Prevention in China. Her research interests include HIV behavioral prevention intervention among various key populations.
Zhiyong Shen, MD, is the director for the Institute of HIV/STD Control and Prevention at Guangxi Centers for Disease Control and Prevention in China. His research interests include HIV epidemiology, HIV prevention, treatment and care and related governmental policies and regulations.
Xueying Yang, PhD, is a post-doctoral fellow in the South Carolina SmartState Center for Healthcare Quality at the University of South Carolina Arnold School of Public Health. Her research interest is mainly the clinical outcomes of people living with HIV, especially among men who have sex with men.
Quan Zhang, PhD, is a post-doctoral fellow in the South Carolina SmartState Center for Healthcare Quality at the University of South Carolina Arnold School of Public Health. His research interests include HIV treatment adherence, HIV-related stigma, and mental health.
Chengbo Zeng, MPH, is a PhD student in the Department of Health Promotion, Education, and Behavior at the University of South Carolina Arnold School of Public Health. His research interests include quantitative analytical methods and the mental health of people living with HIV.