
Abstract
Oral diseases, including dental caries, periodontitis, and edentulism (toothlessness), affect about 3.5 billion people worldwide. A cross-sectional study was conducted to assess the oral health status and treatment needs of government employees employed at an organization in New Delhi. Oral health information was recorded using the standard World Health Organization’s (WHO) Oral Health Assessment Tool. A total of 476 employees at various levels of administration were screened at their worksite. Dental caries and periodontal disease were present in more than half of the participants. Around 56% had decayed teeth, 20% had missing teeth, and 16% had filled teeth. Bleeding from gums was seen in 71% and periodontitis in 59% of participants. Preventive treatment and oral health promotion was required in at least 41% of the screened individuals. Annual workplace oral examinations may help in decreasing the oral disease burden and create awareness on the oral health among employees.
Keywords
Introduction
Oral diseases, including dental caries, periodontitis, and edentulism, affect about 3.5 billion people worldwide (Kassebaum et al., 2017). Oral diseases are the fourth most costly disease to treat in industrialized countries (Petersen, Bourgeois, Ogawa, Estupinan-Day, & Ndiaye, 2005). Routine oral hygiene practices are important for preventing oral disease and maintaining good oral health (Kumar, Tadakamadla, & Johnson, 2016).
Occupational environment refers to the sum of external conditions and influences, which prevail at the place of work, which have a bearing on the health of working population (Park, 2015). The World Health Organization (WHO) states that protecting workers’ health is important to household income, productivity, and economic development, and work-related health problems result in an economic loss of 4% to 6% of gross domestic product (GDP) for most countries (WHO, 2017).
According to a report by WHO (2017), workplace health initiatives can help reduce sick leave by 27% and health care costs for companies by 26%. A study conducted among the Jeep™ factory workers in Southern India reported that the participants had an average of one decayed, missing, or filled teeth; 46.2% of workers required oral prophylaxis and 1.71% required periodontal surgery (Jyothi & Giriraju, 2017). In a study conducted among the Japanese workers, findings indicated that behavioral modification interventions improved the oral health behaviors of the workers (Toyama et al., 2018).
This study was conceptualized to assess the oral health status among employees in New Delhi, as very little literature is available on oral health checkups in the occupational work setting in India. This study aimed to assess oral health status and treatment needs of government workers employed at Nirman Bhavan in New Delhi.
Method
This was a descriptive, cross-sectional study conducted among the employees working in a government setting. On the occasion of World Oral Health Day (2017), an oral health checkup was planned at Nirman Bhavan in New Delhi. We provided an overview of the study to officials at the organization, who then provided permission to conduct the study. Once the venue, date, and time were scheduled, the officials informed all department leaders who then verbally invited all of their workers to participate in the study. The study participants included administrative professionals, clerks, semi-skilled and skilled workers and the study setting was their workplace. The inclusion criteria included all the workers who were present on the day of study and who also gave consent for an oral examination. Written informed consent from the participants was obtained prior to their inclusion in the study and a time slot for oral examination was provided. Ethical approval for the study was obtained from the Institutions Ethics Committee, All India Institute of Medical Sciences (AIIMS), New Delhi.
Data Collection
Data were collected pertaining to employee demographics, their oral hygiene practices such as frequency and materials used to brush their teeth, lifetime smoking (Yes/No) and chewing tobacco use (Yes/No), as well as lifetime alcohol use (Yes/No). Oral examinations were conducted with each participant seated in a portable dental chair. Oral health status was recorded using the standard WHO Oral Health Assessment Tool (WHO, 2013) for adults. This tool provided a sound basis for assessing the current oral health status of these workers, as well as future oral health care needs. More specifically, we used this as a guide to measure the dentition status, periodontal status, oral mucosal lesions, dental fluorosis, dental erosion, and dental trauma. The form also guided us with providing recommendations to workers for future treatment, if needed.
An expert dentist trained nine investigators, who were also dentists, at the Center for Dental Education and Research (CDER), AIIMS in New Delhi, with a substantial agreement for oral exam observations and measurement (Kappa = 0.8) between investigators. In addition, a team of support staff included nurses, health attendants, and housekeeping attendants for purposes of simulating a typical dental office set-up for oral health examination (Figure 1).

Oral health checkup setting.
In addition to the oral examination, participants in the study received oral health education, which included a demonstration of routine oral hygiene measures like brushing and flossing methods (Figure 2). A video screen was placed outside the screening unit with videos on oral health. Education materials on oral health promotion included the pamphlets, brushing calendar, five different kinds of games on oral health, badges, and stickers depicting brushing twice daily which were distributed to all the study participants either for themselves or for their family members. In addition, Training Manual on Oral Health Promotion for Health Workers (2018) was used as a resource. All the tobacco users were given individual tobacco cessation counseling, emphasizing the importance of quitting the tobacco use, ill effects of tobacco on oral and systemic health. The individuals with dental treatment need were referred to CDER-AIIMS for further management. All the tobacco users were referred to tobacco cessation clinics CDER-AIIMS for further assistance in quitting tobacco.

Delivery of oral health education.
Data Analysis
The data were entered in Microsoft Excel by the data entry operators hired for this oral health camp study. Statistical Package for Social Sciences (SPSS, IBM version 20.0) was used to calculate overall samples, frequencies, means, and standard deviations of main study measures.
Results
A total of 476 individuals participated in the study, of which 18% were females and 82% were males (Table 1). Most of the participants were administrative professionals (61%), and more than (57%) half had graduate-level education. The majority of participants (71%) reported cleaning their teeth only once a day (rather than the recommended twice per day), and the most common materials used for cleaning were tooth paste (80%) and tooth brush (53%), respectively. Participants also reported the habit of smoking tobacco (12%), smokeless tobacco (8%), and alcohol use (8%) in their lifetime.
Demographic Details and Oral Health Habit History of Government Office Workers (N = 476).
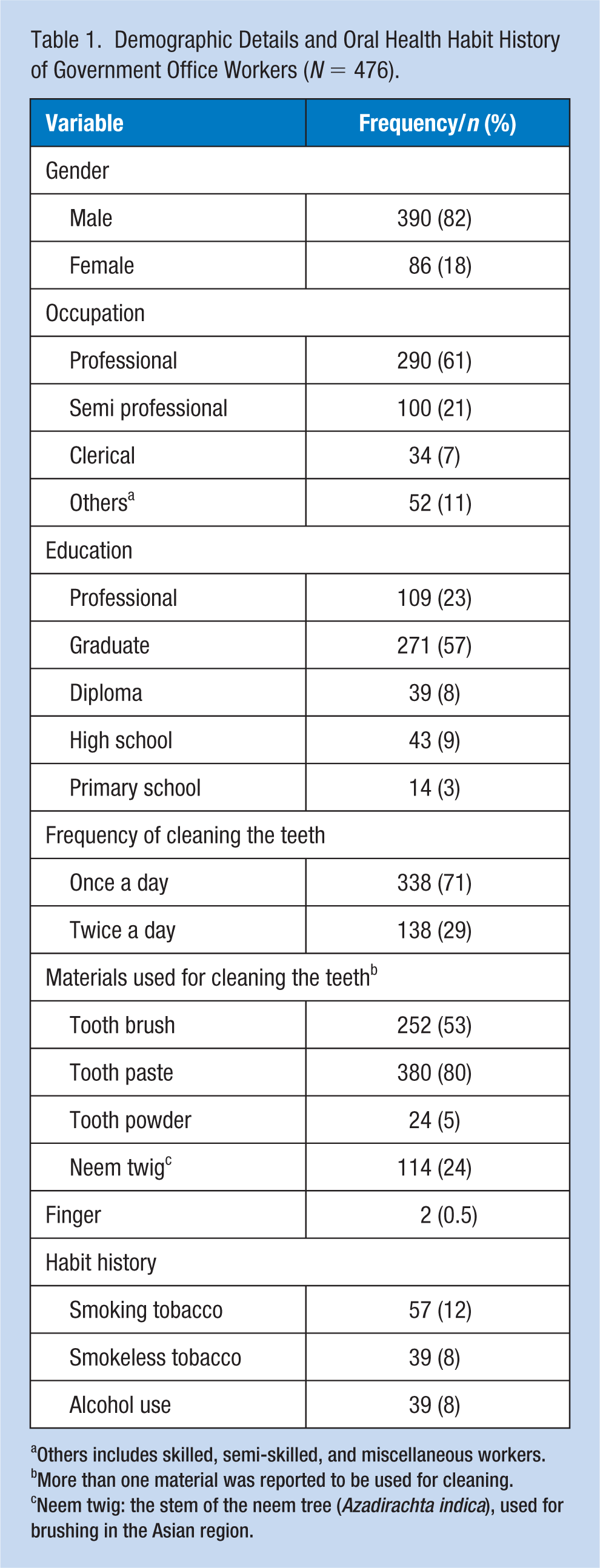
Others includes skilled, semi-skilled, and miscellaneous workers.
More than one material was reported to be used for cleaning.
Neem twig: the stem of the neem tree (Azadirachta indica), used for brushing in the Asian region.
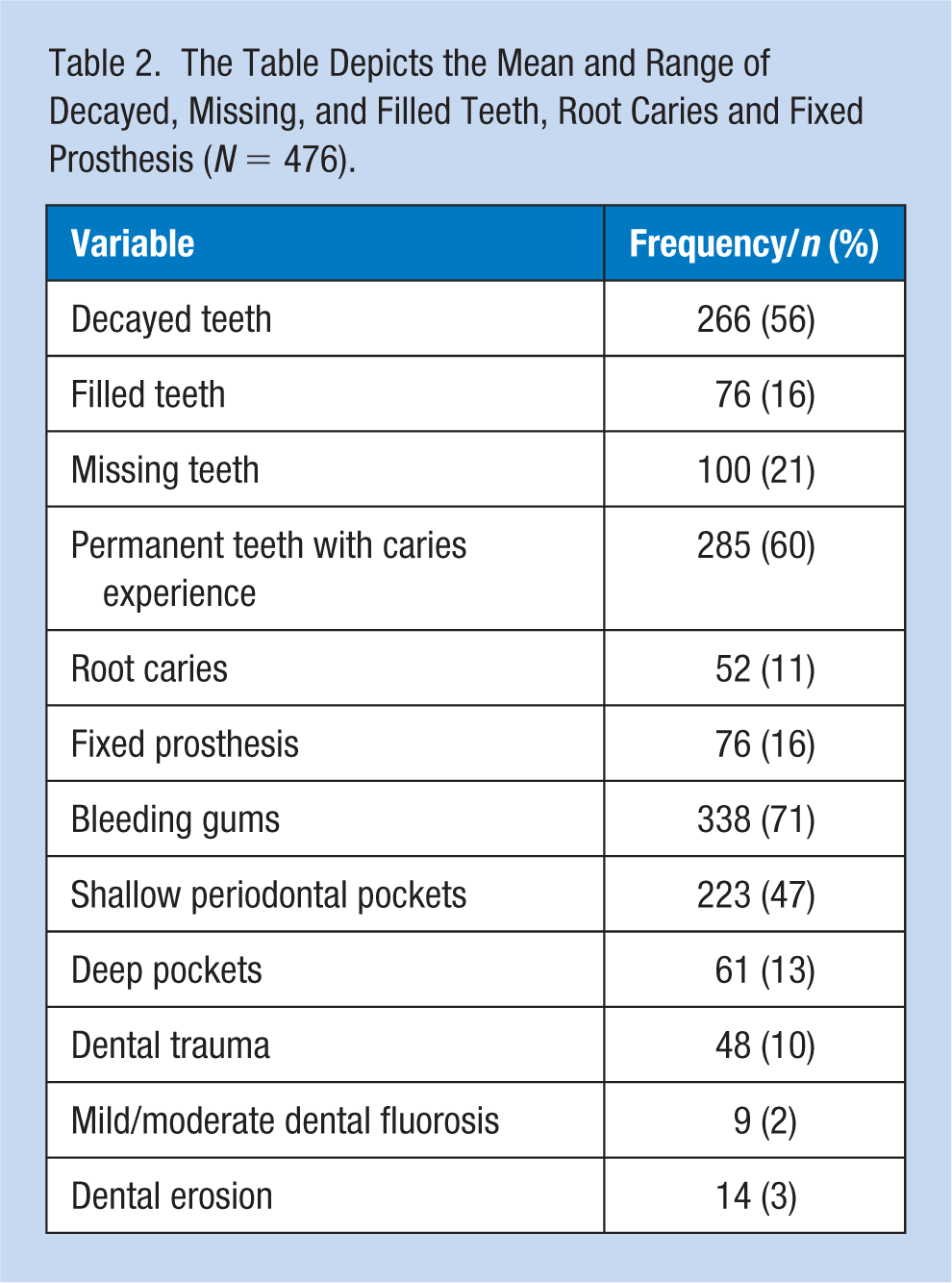
On average, the caries experience (decayed, missing, filled teeth—DMFT) was 3.92 ± 5.42 (standard deviation). Approximately 56% had decayed teeth, 16% had filled teeth, and 21% had missing teeth. Fixed prosthesis was present in 16% participants and only 1% of participants wore removable denture wearers. Around 60% of the individuals had natural (sound) teeth and one-tenth (11%) participants had root caries.
Periodontal status of the participants revealed that 71% had bleeding gums, 47% had shallow periodontal pockets, and 13% had deep pockets. Dental trauma was present among 10% of the participants. Mild and moderate forms of fluorosis (discoloration due to fluoride) were seen in 2% of participants, while dental erosion was seen only in 3% (Table 2).
The Table Depicts the Mean and Range of Decayed, Missing, and Filled Teeth, Root Caries and Fixed Prosthesis (N = 476).
Only 16% of the participants did not require any treatment, 42% required preventive treatments, 36% required prompt treatment such as oral prophylaxis or restoration of decayed teeth, 4% required immediate treatment due to dental pain or infection, and 2% of the participants were referred for comprehensive evaluation or other medical treatment (Table 3).
Treatment Needs Identified Among Study Participants (N = 476).
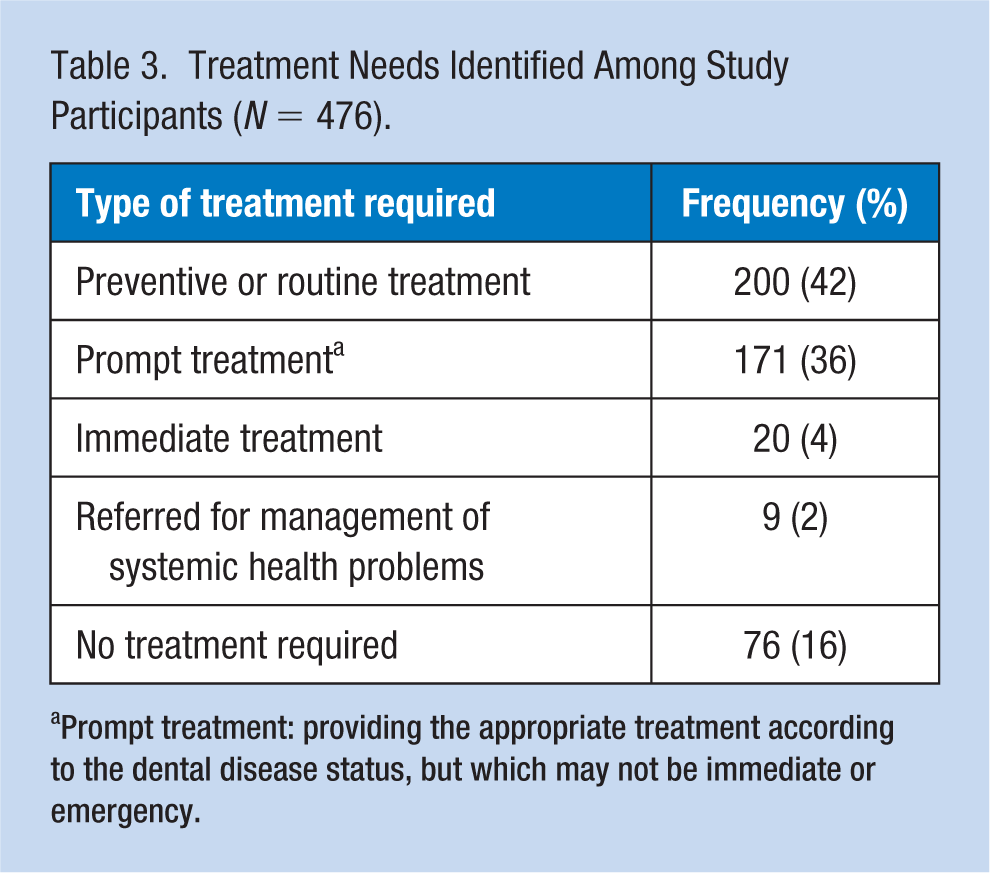
Prompt treatment: providing the appropriate treatment according to the dental disease status, but which may not be immediate or emergency.
Discussion
The present study assessed the oral health status and treatment needs of the employees at Nirman Bhavan as a part of the World Oral Health Day celebration.
The participants reported a low prevalence of smoking tobacco (12%), smokeless tobacco (8%), and alcohol (8%) use which were relatively less compared with the Indian national average (Tata Institute of Social Sciences, Mumbai and Ministry of Health and Family Welfare, & Government of India, n.d.). Similar to the present study, tobacco use (6.3%) was also low among law enforcement personnel in India (Priyanka, Rao, Rajesh, Shenoy, & Pai, 2016).
The caries experience of the current study population (M ± SD: 3.92 ± 5.42) was found to be high compared with the findings of a study among the teaching (2.18 ± 1.99) and nonteaching employees (2.62 ± 2.35) at a university in India (Swamy, Sogi, Sudan, Vedi, & Sharma, 2018). In contrast, a study conducted among the information technology (IT) workers in South India (Acharya & Pentapati, 2012) reported a higher caries experience of 4.23 ± 3.47 compared with the present study.
Bleeding from gums was observed in the majority of the participants, and more than half of the participants had periodontitis. These findings are similar to the high burden (60%) of gingival disease among state government employees in Shimla, India (Bhardwaj, Veeresha, & Sharma, 2012).
A low proportion of participants were found to have a fixed prosthesis, and more than half had sound (healthy) natural teeth. This could be due to the high education level, occupation, and income levels of the study participants. Dental erosion was found in 2.5% of participants; in contrast, 49% of the industrial workers had dental erosion in Himachal Pradesh (Bansal, Singh, Bector, & Dogra, 2018). These differences could be due to the nature of industrial work and exposure to chemicals at workplace.
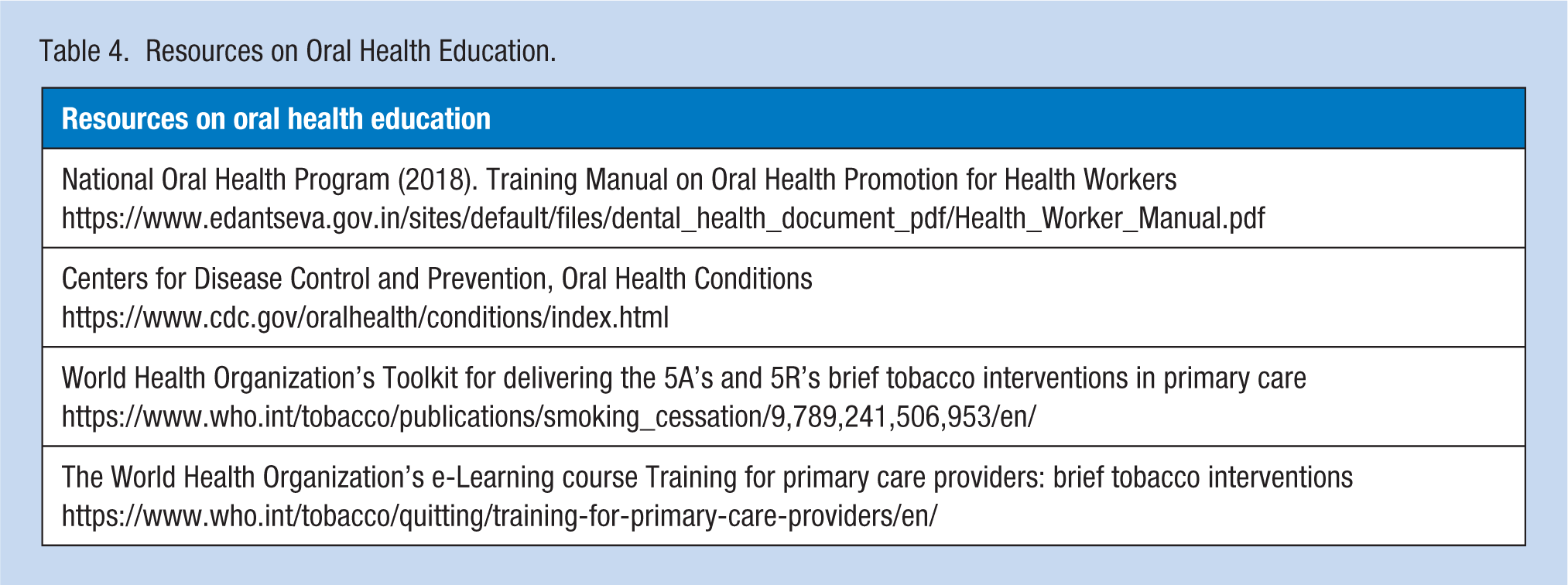
The strength of this study was that each participant was given a 15-minute time slot for an oral examination by which the waiting time was reduced without disturbing their regular work schedule. During this time, oral health education and tobacco cessation was provided using various modes such as LED screens showing videos, brushing models, posters, and banners (Table 4). This study was limited in that participants’ perceptions on dental checkup and their pre- and post-knowledge on the oral health were not assessed.
Resources on Oral Health Education.
Implications for Occupational Health Nursing Practice
In a prior study, individuals who received a workplace oral health examination every year had better periodontal health status than those receiving an examination for the first time (Oshikohji et al., 2011). A regular workplace oral health checkup should be scheduled to reduce the oral disease burden among workers. Incorporating tooth brushing instructions along with conventional dental checkup has been found to be effective in reducing poor plaque control (Furusawa et al., 2011). Similarly, in the current study oral health education included oral hygiene maintenance and tooth brushing instructions to all the participants individually; this could help them to better maintain their oral hygiene.
The findings of this study imply that there is a large burden of oral disease in the working class population of this work setting. The occupational health nurse is in an ideal setting to conduct oral visual examination, oral health education, diet counseling as it pertains to oral health, and smoking cessation, and demonstration of brushing and flossing methods (see resources in Table 4). This may help in the primary prevention of identifying and reducing the risk of oral diseases such as dental caries, periodontal diseases, and oral cancer.
Conclusion
The dental caries experience among the study participants was found to be high, irrespective of their level of education and occupation. Hence, the oral health examination along with oral health education should be a part of the annual health activities at the workplace. Oral health examination along with oral health education may be effective for the maintenance of oral health of the worker.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
O. P. Kharbanda, MDS, is the chief at the Centre for Dental Education, and research professor and Head of the Department of Orthodontics and Dentofacial Deformities at Centre for Dental Education and Research, All India Institute of Medical Sciences, New Delhi, India.
Harsh Priya, MDS, is an assistant professor in the Department of Public Health Dentistry at Centre for Dental Education and Research, All India Institute of Medical Sciences, New Delhi, India.
Deepika Mishra, MDS, is an assistant professor in the Department of Oral Pathology at Centre for Dental Education and Research, All India Institute of Medical Sciences, New Delhi, India.
Shalini Gupta, MDS, is an assistant professor in the Department of Oral Medicine and Radiology at Centre for Dental Education and Research, All India Institute of Medical Sciences, New Delhi, India.
Anupama Ivaturi, MDS, is a senior resident in the Department of Public Health Dentistry at Centre for Dental Education and Research, All India Institute of Medical Sciences, New Delhi, India.
Priyanka Ravi, MDS, is a senior resident in the Department of Public Health Dentistry at Centre for Dental Education and Research, All India Institute of Medical Sciences, New Delhi, India.
Anu Bhatia, MDS, is a senior resident in the Department of Periodontology at Centre for Dental Education and Research, All India Institute of Medical Sciences, New Delhi, India.
Ashish Prasad, MDS, is a senior resident in the Department of Orthodontics and Dentofacial Deformities at Centre for Dental Education and Research, All India Institute of Medical Sciences, New Delhi, India.
Azhar Ali, MDS, is a senior resident in the Department of Conservative Dentistry and Endodontics at Centre for Dental Education and Research, All India Institute of Medical Sciences, New Delhi, India.
Desmia Haldane, BDS, is a former senior research fellow in the National Oral Health Program at Centre for Dental Education and Research, All India Institute of Medical Sciences, New Delhi, India.