
Abstract
The opioid epidemic is a national public health crisis. It began with the misuse of commonly used prescription opioid pain relievers and has led to the increased use of heroin and illicit fentanyl. Large-scale initiatives have begun on the federal and state level and place an emphasis on improved opioid prescribing, which have important implications for the workplace. Treatment of work injury may initiate the use of prescription opioids and result in misuse and possible overdose. Prescription drug abuse affects all aspects of society so potentially any workplace could be affected. A multifaceted approach is needed to reduce opioid morbidity and mortality and the occupational health nurse should be actively involved. The intent of this article is to provide an overview of the epidemic and its impact on health, the challenges for the workplace, and recommended strategies for the occupational health nurse to impact the problem.
Introduction
According to the Office of the Surgeon General, U.S. Department of Health and Human Services (2016), in 2015 over 27 million people in the United States (US) were diagnosed with a substance use disorder. Over 75% of those people were employed either full- or part-time. Workers who abuse drugs are more likely to have issues at work including unexcused absences, leave their jobs soon into employment or be fired, be involved in workplace accidents, and file workers’ compensation claims. Work loss related to misuse of prescription opioids has been estimated to be US$ 26 billion. (Substance Abuse and Mental Health Services Administration [SAMHSA], 2017a, 2017b). A 2017 study found that annual health care costs for an employee with a pain medication use disorder was more than 3 times as much as those for a healthy employee (Goplerud, Hodge, & Benham, 2017).
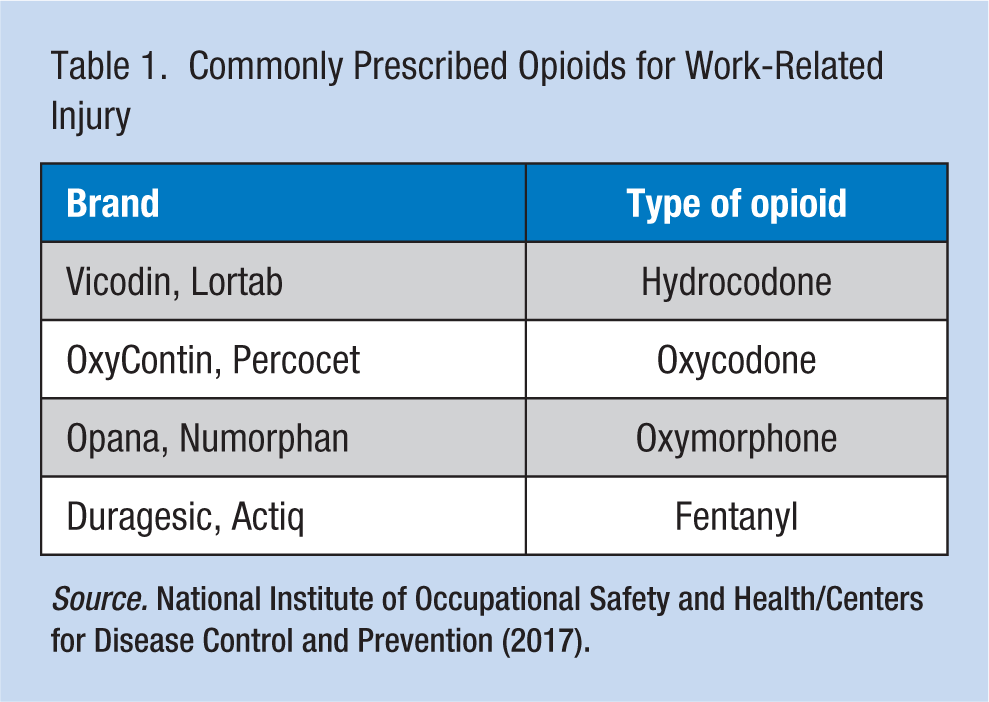
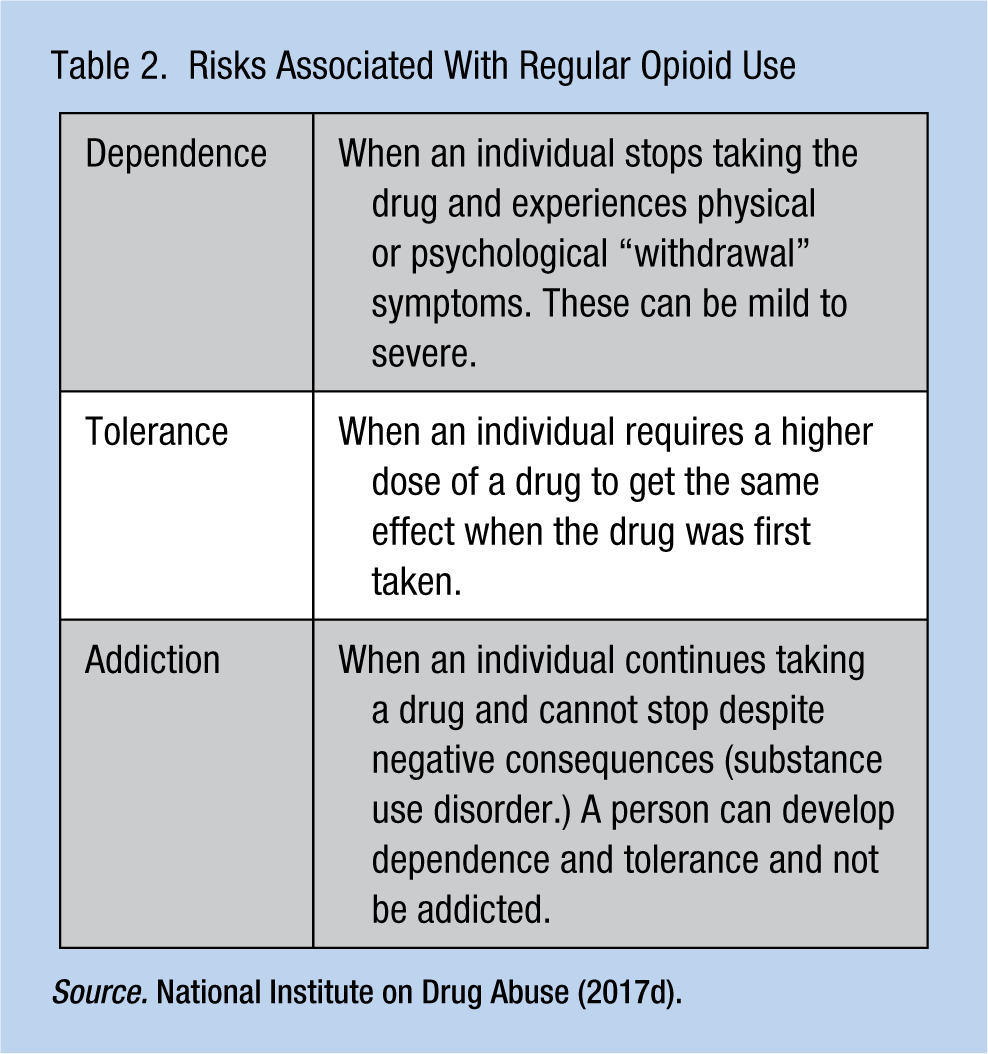
Opioids are powerful narcotic analgesics which are often prescribed following surgery or injury, and for medical conditions such as cancer. Opioids include natural and semisynthetic prescription pain relievers (e.g., morphine, codeine, Percocet, oxycodone), synthetic opioids (e.g., methadone, fentanyl and tramadol), and illicit drugs (e.g., heroin) (Centers for Disease Control and Prevention [CDC], 2017c). Examples of commonly prescribed opioids for work-related injury are listed in Table 1. Regular use, even with a prescription, can lead to dependence, tolerance, and in some cases addiction (Dowell, Haegerich, & Chou, 2016; National Institute on Drug Abuse [NIDA], 2017a; Table 2). Once opioids are prescribed, transition to long-term use can occur quickly, as early as day 3 of the prescription (Shah, Hayes, & Martin, 2017). Over the last two decades, the increased use of prescribed and illicit opioids has resulted in excessive numbers of drug overdoses and deaths. This trend has become a serious national crisis that affects public health as well as social and economic welfare (NIDA, 2018). This review discusses the evolution of this problem and the impact on public health, the challenges for the workplace, and recommended strategies for the occupational health nurse to impact the problem.
Commonly Prescribed Opioids for Work-Related Injury
Risks Associated With Regular Opioid Use
Evolution and Impact of the Opioid Epidemic
In much of the 20th century, opioid use was limited due to concerns about addiction, but later in the 1990s this trend changed. Several factors contributed to the current epidemic including the aggressive production and marketing of prescription opioids by pharmaceutical companies, a more accepting attitude toward the use of prescription opioids by prescribing health care providers, and the introduction of heroin and illicit fentanyl into U.S. communities (Christie et al., 2017; Kolodny et al., 2015).
Rise in Opioid Consumption
An opioid prescription production surge began with the introduction of a controlled release of OxyContin in 1995. From 1999 to 2010, opioid prescription sales to hospitals, pharmacies, and practitioners nearly quadrupled in the US (Paulozzi, Jones, Mack, & Rudd, 2011). Leaders in pain management and some health care organizations promoted pain as the “fifth vital sign” and encouraged more aggressive use of prescription opioids for chronic, noncancer pain. Annual opioid prescription rates increased gradually from 2006 (72.4 per 100 persons) until 2012 (80.0 per 100 persons) and then declined through 2016. In 2016, prescription rates were still high at 66.5 opioid prescriptions for every 100 Americans (CDC, National Center for Injury Prevention and Control, 2017). Among prescribing health care practitioners, a 2013 study (Levy, Paulozzi, Mack, & Jones, 2015) found that primary care specialty groups (44.5%) prescribed opioids most followed by nonphysician prescribers (11.2%). Rates of opioid prescribing were highest in the specialty areas of pain medicine (48.6%), surgery (36.5%), and physical medicine/rehabilitation (35.5%).
When taken as prescribed and for very short periods (e.g., a few days) people can use opioids to manage pain safely and effectively (NIDA, 2017d). Factors that may prompt people to misuse opioids and precipitate addiction and overdose include the specific opioid type, the dose, number of doses, route of administration, formulation, and release time (immediate or extended). High doses and longer use of opioids make people especially vulnerable to misuse (Christie et al., 2017). Misuse or “nonmedical” use is defined as using prescription drugs to self-treat a medical condition with someone else’s prescription or with left-over medication from an earlier medical problem, taking a larger dose than prescribed for a stronger therapeutic effect, or using prescription drugs for the feeling you can achieve (SAMHSA, 2017a). A common reason for opioid use for individuals who misuse prescription opioids is to relieve physical pain. Those who misuse prescription opioids obtain them most often for free from friends or relatives, and the original source of the opioids from these contacts is usually physicians (Han et al., 2017). The most abused prescription opioids are methadone, oxycodone (OxyContin), and hydrocodone (Vicodin; CDC, 2017f).
Transition From Prescription Opioids to Heroin and Synthetic Opioids
Data from the US federal government’s National Survey on Drug Use and Health (NSDUH) show that a small proportion (4%) of those that misuse prescription opioids transition to heroin. However, four out of five heroin users report they began opioid use with prescription opioids (Muhuri, Gfroerer, & Davies, 2013). People transition to heroin because of prescription opioid dependence and the low price, high purity, and more euphoric effect of heroin (Christie et al., 2017; Rudd, Aleshire, Zibbell, & Gladden, 2016; U.S. Department of Justice, Drug Enforcement Administration [U.S. DOJ, DEA], 2016). Some of the greatest increases in heroin use have occurred in groups with historically low rates of heroin use, including women, the privately insured, and people with higher incomes (CDC, 2015). Users inject, sniff, snort, or smoke heroin and it is highly addictive (NIDA, 2017b). Recent evidence indicates that heroin is increasingly being used without prior use of prescription opioids (Cicero, Ellis, & Kasper, 2017).
Use of illicit fentanyl and its analogs (subtypes) is the new danger in the community. Fentanyl is 30 to 50 times more potent than heroin and potentially lethal even at very low doses (CDC, 2017a; U.S. DOJ, DEA, 2015). It is frequently mixed with and sold as heroin to users who are often unaware of the adulteration and the consequent potency (U.S. DOJ, DEA, 2016). Fentanyl and fentanyl analogs are fast-acting and trigger rapid progression to loss of consciousness and death requiring multiple doses of naloxone to reverse the overdose (Daniulaityte et al., 2017; O’Donnell, Halpin, Mattson, Goldberger, & Gladden, 2017).
Deaths From Opioid Overdose
Misuse of opioids has resulted in escalating rates of opioid overdose deaths over time, and these deaths are now being attributed more often to heroin and fentanyl compared with other opioids (Figure 1). In 2016, the CDC reported 63,632 drug overdose deaths and opioid-related overdoses accounted for two thirds (66.4%) of all overdose deaths. Opioid-related deaths continue to increase; the 2016 opioid drug overdose death rate (13.3 per 100,000 population) was a 27.9% increase from 2015 (10.4 per 100,000 population). In 2016, the largest overall rate increases occurred among deaths involving synthetic opioids (100%) and cocaine (53.4%; Seth, Scholl, Rudd, & Bacon, 2018). Increases in deaths involving heroin and synthetic opioids are mainly due to the availability of heroin and the mixing of illicit fentanyl into the heroin supply (O’Donnell, Gladden, & Seth, 2017).
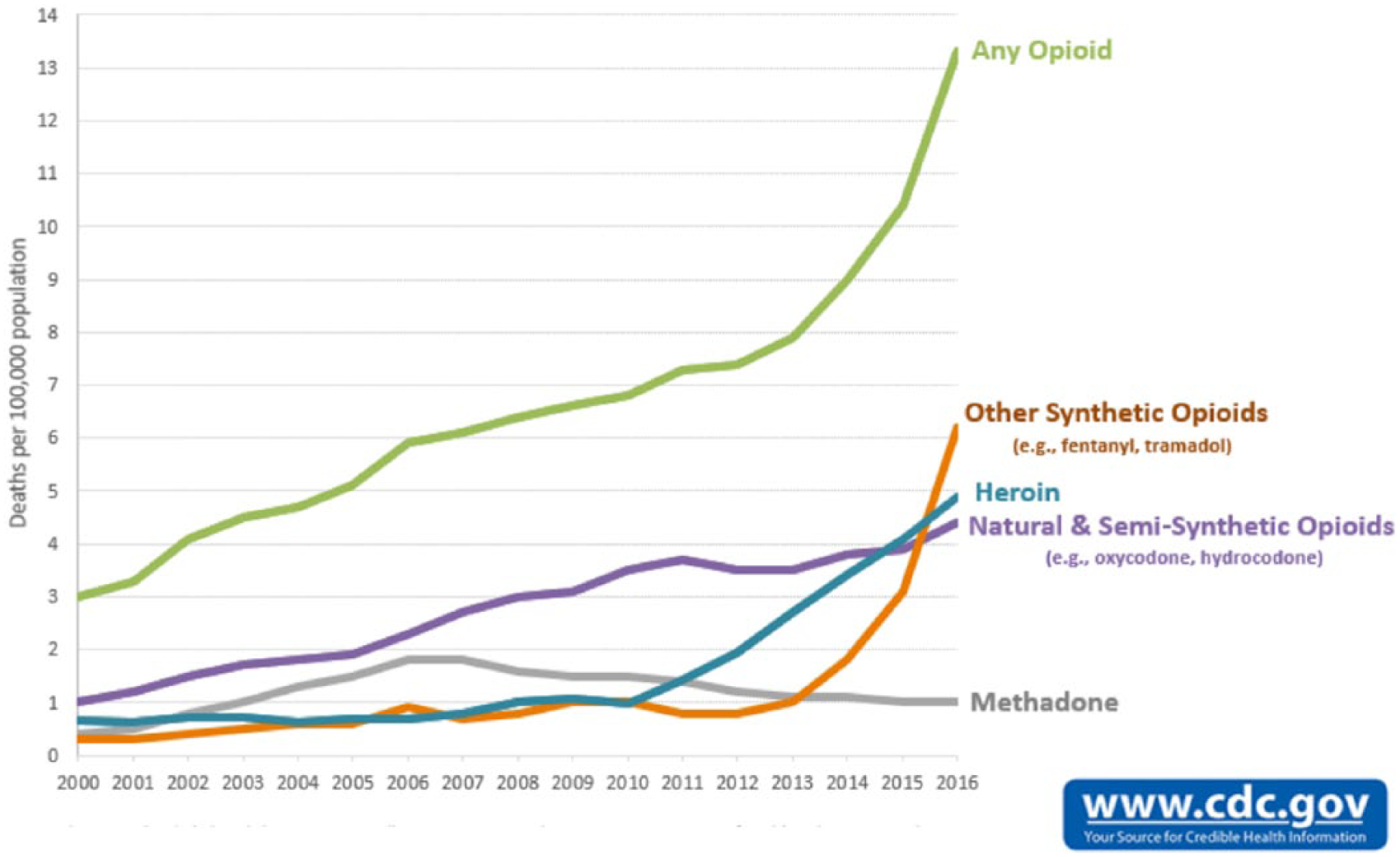
Overdose deaths involving opioids, United States, 2000-2016.
Deaths related to prescription opioids are higher for non-Hispanic Whites, males, and those aged 45 to 54 years (Rudd, Seth, David, & Scholl, 2016). Those who abuse or overdose on prescription opioids tend to live in rural areas, have lower income, have mental illness or history of other substance abuse, take high daily doses of prescription opioids, and likely doctor shop for prescriptions (CDC, 2017f). In contrast, those at risk for heroin addiction tend to be 18 to 25 years old, non-Hispanic White males. These individuals reside in large urban areas, have low income, have no health insurance, and have a history of prior substance abuse that includes opioid pain relievers (CDC, 2015).
Related Health Concerns
There are other possible health consequences when individuals misuse opioids. Serious concurrent health issues are associated with injection drug use and include an increased risk of Hepatitis C, HIV, Hepatitis B, bacterial infections of the skin, endocarditis, and sepsis (CDC, 2015; NIDA, 2017b).
The Workplace and Opioids
The opioid epidemic presents important implications for the workplace, and occupational health nurses need to be aware of the serious risks associated with the prescribing of opioids. Treatment of workplace injuries may initiate opioid use. Opioid prescription medications have the potential to impact a worker’s performance on the job and cause workplace accidents, even when taken as prescribed.
Risks associated with workers taking prescription drugs for on-the-job injuries are not a new concern for occupational health nurses. Prescription opioids are powerful drugs and may cause impairment, errors, and injury even when taken as prescribed. In preparation for updating opioid prescribing guidelines in 2014, the American College of Occupational and Environmental Medicine (ACOEM; Hegmann et al., 2014) performed an extensive literature review and found studies indicating that prescription opioids of varying strengths were positively associated with an increased risk of motor vehicle crashes. Included in this review was a study done by Gibson et al. (2009) where researchers examined motor vehicle crash data for 49,821 individuals aged 18 to 74 years from 1986 to 2004. The results of the analysis suggested that the risk of a motor vehicle crash was increased by the use of benzodiazepines, opioids, and compound analgesic preparations containing acetaminophen and an opioid for the duration of their usage, the risk decreasing once the medication was discontinued. They found modest to no evidence of increased risk of a motor vehicle crash for those using other categories of drugs such as hypnotics, selective serotonin reuptake inhibitors (SSRIs), antihistamines, antidepressants, or beta-blockers. The ACOEM review found no epidemiological studies that addressed other high-risk activities such as forklift driving, heavy equipment operation, and so forth, but they did stipulate that acute or chronic opioid use was not recommended for these and other safety sensitive jobs. It has been found that the use of prescription pain medications for worker injury can increase workers’ compensation costs (White, Tao, Tairefa, Tower, & Bernacki, 2012) and decrease work productivity by delaying recovery and return to work from a work-related injury (Franklin, Stover, Turner, Fulton-Kehoe, & Wickizer, 2008; Webster, Verma, & Gatchel, 2007).
The new challenge for the occupational health nurse is that while prescription opioids have been relied on historically to treat workers, misuse is now a consideration (American Association of Occupational Health Nurses, 2018). There is evidence of substantial risk for opioid misuse and potentially any workplace could be affected. The CDC’s National Center for Injury Prevention and Control (2017) states that while opioid prescription rates have declined in recent years, the rate at which health care providers are prescribing opioids is still high with estimates of 66.5 prescriptions per 100 Americans. In 2016, it was estimated that more than one third of the U.S. population used prescription opioids (Han et al., 2017) and many access opioids through workers’ compensation systems. For example, in 2014 when prescription drugs were ranked by share of total workers’ compensation prescription drug costs, four out of the top 10 drugs contributing to the cost were opioids (OxyContin, oxycodone–acetaminophen, hydrocodone–acetaminophen, and oxycodone HCL; National Council on Compensation Insurance, 2016). In 2017, the U.S. Department of Labor reported that the opioid crisis was affecting people at home and increasingly on the job. Overdoses related to the nonmedical use of drugs or alcohol while on the job increased 32% from 2015 to 2016 and overdose fatalities increased 25% annually since 2012 (U.S. Department of Labor, Bureau of Labor Statistics, 2017).
A multifaceted approach is needed to protect workers and businesses. The occupational health nurse should work in partnership with their employers, occupational health medical providers, and others, to institute best practices that will decrease or eliminate the possibility of opioid misuse related to a workplace injury. Understanding current public health strategies to prevent opioid misuse is the first step to becoming informed and developing a response.
CDC Recommended Public Health Strategies to Address the Opioid Epidemic
Primary Prevention
The aim of primary prevention is to reduce the risk of disease through specific protective actions (Rogers, 1994). Public health authorities stipulate a paramount step in curtailing the opioid epidemic is to control the oversupply of opioids (CDC, 2017d; Rudd, Aleshire, et al., 2016). At the clinical level, occupational health care providers should prescribe opioids for acute and chronic pain with more caution. The occupational health nurse should be trained and poised to identify and understand proactive measures to take to help prepare health care providers for wiser use of prescription opioids and educate patients about risk. Understanding opioid prescribing guidelines is essential.
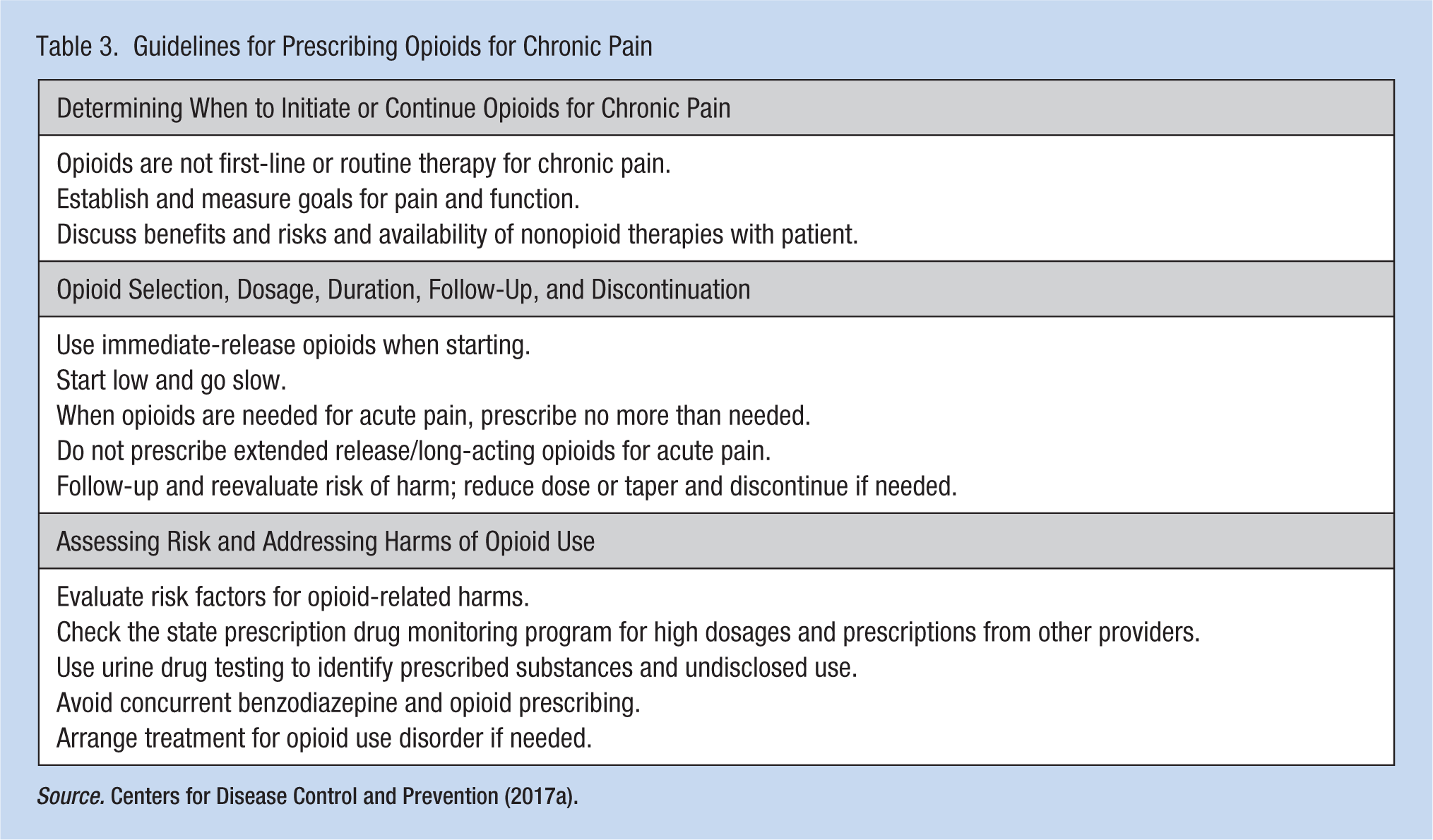
In 2016, the CDC published the CDC Guideline for Prescribing Opioids for Chronic Pain to assist primary care providers in choosing treatment options for chronic pain, including section 6 that addresses acute pain (CDC, 2016). Recommendations are provided to determine when to initiate or continue treatment with opioids; opioid selection, dosage, duration, follow-up, and discontinuation; and how to assess risk and potential harm including how to manage specific subgroups like the elderly and pregnant women. The first step in initiating opioid treatment is a discussion between the health care provider and the patient to set realistic goals for pain management and function based on the diagnosis. Recommendations stipulate that nonpharmacologic therapy and nonopioid pharmacologic therapy are preferred for chronic pain. If initiated, opioid treatment should be “low and slow,” avoiding extended release opioid products. If opioids are prescribed for treatment of acute pain, a ⩽ 3-day supply is recommended. Assessing risk and occurrence of harmful behaviors while using opioids is now a critical step for prescribing health care providers while managing a patient on opioids to avoid abuse and overdose. At a minimum, health care providers are advised to assess for behaviors that are risk factors for a substance use disorder such as previous alcohol history, illicit drug use, and nonmedical use of prescription drugs. Key components of the guidelines are presented in Table 3. More cautious prescribing also reduces the amount of opioids available in the community and prevents diversion (transfer from the person with the prescription to another person for nonmedical use). Health care providers should be educated about opioids using the CDC prescribing guidelines. Patients should understand the risk and benefits of opioid treatment and be educated to secure their opioid medications in the home and to properly discard any unused opioid medication (CDC, 2017b; Dowell et al., 2016; Kolodny et al., 2015).
Guidelines for Prescribing Opioids for Chronic Pain
Secondary Prevention
The aim of secondary prevention is to detect a condition after its onset but before it progresses or results in disability. Efforts to identify and treat those addicted to opioids early on are likely to reduce the risk of abuse and transition to injecting opioids (Kolodny et al., 2015). The occupational health nurse should understand the screening activities available to health care providers to help identify those that may be misusing opioids such as use of a prescription drug monitoring program (PDMP).
Individuals who misuse opioids may try and obtain prescriptions from multiple providers or “doctor shop”; however, those attempting this can be identified through use of a PDMP. This is a statewide electronic database that enables users to track all controlled substance prescriptions and those authorized to use it can view information regarding medications that have been dispensed and their dosages. PDMPs are available in all states except Missouri (Jaffe, 2016). Health care providers can use the PDMP to identify those trying to obtain prescriptions from multiple providers, calculate the total amount of opioids prescribed in 1 day, and identify other substances patients may be on that increase the risk of opioid addiction and overdose. The PDMP should be checked prior to every opioid prescription and on a routine basis. Opioids should be prescribed by a single provider. In addition to checking the PDMP, providers can try and assess opioid use by conducting urine drug tests (UDT). UDT can be used to verify prescription compliance, noncompliance (and possibly stockpiling for diversion), or use of other illicit or incompatible drugs (CDC, 2017e; Dowell et al., 2016; Kolodny et al., 2015; National Safety Council [NSC], 2015).
Tertiary Prevention
Tertiary prevention strategies involve minimizing the degree of disability associated with a certain condition. Treating with regard to opioid addiction, the goal is to provide assistance that will help prevent overdose deaths, medical and psychological complications, transition to injection drug use, and injection-related infectious diseases (Kolodny et al., 2015). The occupational health nurse should become the subject matter expert for the workplace on the identification of and response to those with a substance use disorder. Treatment for those addicted to opioids is specialized and may appear somewhat unconventional.
Substance use disorder is difficult to treat due to brain changes that occur over time with drug use. It is a chronic illness, much like diabetes or asthma, but with a compulsive predilection for drug use (NIDA, 2016). Cognitive behavioral therapy (CBT) is utilized for opioid addiction and can be done on an inpatient or outpatient basis. It provides individuals with the knowledge of what may trigger a relapse and positive coping mechanisms to replace the previous unwanted behaviors. CBT can be utilized alone or in conjunction with opiate agonists (methadone and buprenorphine) or an opiate antagonist such as naltrexone (NIDA, 2017c). This combination treatment is referred to as Medication-Assisted Treatment (MAT). Tertiary prevention strategies also include harm-reduction steps such as syringe exchange programs to prevent secondary infection and expanded access to naloxone. Naloxone will effectively and quickly reverse respiratory depression that can occur during an overdose (CDC, 2017d; Kolodny et al., 2015).
The Role of State Laws
State lawmakers have the authority to develop polices to ensure public health strategies are implemented in the community to control opioid misuse and overdose. It is very important that occupational health nurses become familiar with their respective state policies and laws related to all facets of opioid prescribing, dispensing, use, and addiction treatment. Successful strategies to impact the opioid epidemic reported by states include maximizing use of PDMPs; closer monitoring and regulation of pain clinics that have been shown to dispense large quantities of opioids for pain with little medical justification (Johnson, Paulozzi, Porucznik, Mack, & Herter, 2014); closer evaluation of prescribing policies of health plans like workers’ compensation and Medicaid that have the power to put checks in place to prevent overprescribing; increasing access to substance abuse treatment services; expanding first responder access to naloxone, an essential harm reduction tool now necessary to prevent overdose deaths; promoting use of the CDC Guideline for Prescribing Opioids for Chronic Pain; and working with communities where drug addiction is common (CDC, 2017g). To help improve its ability to control the oversupply of prescription opioids in the community, North Carolina passed new workers’ compensation laws in 2018. For those health care providers treating work-related injury, these laws require documentation that nonpharmacologic and nonopioid therapies were insufficient to treat pain; a cap of 5 days for the first opioid prescription for acute pain; and utilization of an opioid risk assessment and screening tool prior to writing a second opioid prescription (North Carolina Medical Society, 2018). States have varying levels of prescription pain management regulations. Fifty out of 51 (50 states and the District of Columbia) have PDMPs that are updated either daily, every 3 business days, or weekly. Nineteen out of 51 (50 states and the District of Columbia) have limits on the number of days the prescription can last. Thirty-four out of 51 require a substance use disorder assessment prior to opioid prescription, 36 of 51 mandate pharmacies check a personal form of ID to confirm identity before dispensing medications, and 18 of 51 require continuing medical education (CME) for clinicians who prescribe opioids. An occupational health nurse can check their state’s opioid regulations at AthenaInsight at Athenahealth.com: https://www.athenahealth.com/insight/infographic-opioid-regulations-state-by-state (Athenahealth, 2017).
Next Steps for the Occupational Health Nurse
Occupational health nurses are in a key position to help employers adapt CDC’s prevention strategies for the workplace to protect workers from opioid misuse and addiction. Specific action steps are found in the publication from the NSC (2015), The Proactive Role Employers Can Take; Opioids in the Workplace. This document outlines a “Call to Action” which prioritizes specific actions occupational health nurses can take in the workplace to respond to the opioid crisis. Other resources for occupational health nurses can be found in Table 4.
Opioid Prescribing and Use Resources for the Occupational Health Nurse, Health Care Providers, and Employees.
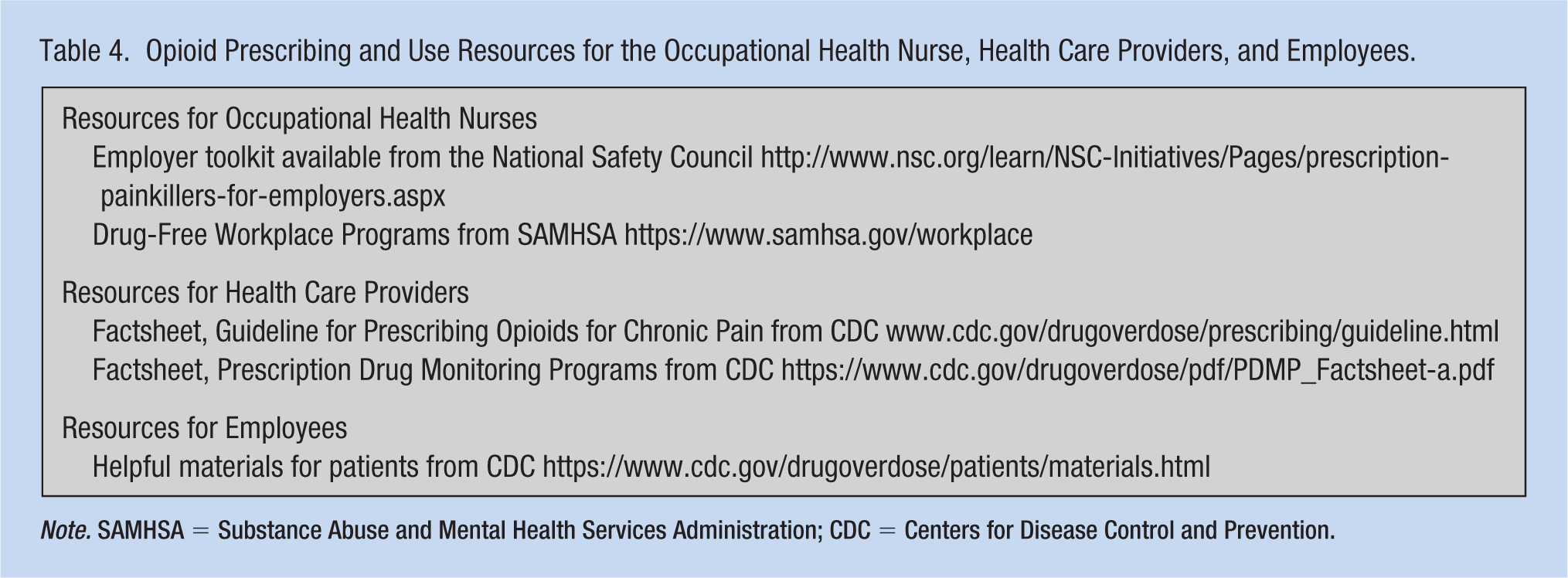
Note. SAMHSA = Substance Abuse and Mental Health Services Administration; CDC = Centers for Disease Control and Prevention.
As recommended by the NSC, essential steps that the occupational health nurse should consider taking are outlined below.
Partnering With Medical Care and Benefit Providers
Occupational health nurses should work with their occupational health providers to educate them on proper opioid prescription practices and advocate for better monitoring of prescriptions for patients. Education should include information about the CDC Guideline for Prescribing Opioids for Chronic Pain, the state PDMP, and urine drug testing (NSC, 2015; Woods, 2018). It is important that health care providers be familiar with state-specific laws that regulate opioid prescribing and address related initiatives such as required CME education. Focused education and monitoring should be implemented with high-volume opioid prescribers such as frontline primary care providers and surgeons. Occupational health nurses should consider coordinating with rehabilitation nurses during workers’ compensation claim management to educate health care providers about cautious use of opioids. Resources to help educate health care providers can be found in Table 4.
Any conversation with a patient about pain management should begin with clarifying the goals of pain control. It is important to stress that the purpose of pain control is to improve function with minimal pain rather than a less achievable goal of complete elimination of pain. This information should ease the acceptance of alternative therapies and may prevent requests for increases in doses. Health care providers should work in tandem with the occupational health nurse to assess an individual’s knowledge regarding their expectations of pain control and consider alternative treatment modalities that include nonnarcotic pain relievers, massage, physical therapy, CBT, and individual exercise plans (Ferriolo & Conlon, 2012; Woods, 2018).
Education and advocacy should also include benefit providers. Benefit providers include workers’ compensation carriers, state-run health plans, company health care plans, Medicaid, and Prescription Benefit Managers (PBMs). A PBM is a third-party administrator that typically manages the prescription drug component of an employer health plan. Benefit providers can act as gatekeepers for opioid use because they can intervene at the point of prescribing if necessary. Without diligence by benefit partners opioids may still be overprescribed, dispensed by health care provider offices directly versus pharmacies (more expensive), or prescribed for too long. Some recommended strategies to address these challenges include prior authorization, drug utilization review, patient review, and restriction programs. Occupational health nurses should work closely with their benefit providers to understand claim utilization data and consider adopting recommended strategies to impact prescribing behaviors and opioid claims (NSC, 2015). Occupational health nurses may establish or already have periodic reviews set up with benefit partners and opioid plans could be discussed during these meetings.
Reevaluating the Drug-Free Workplace Program and Drug Testing
A Drug-Free Workplace Program (DFWP) is essential in addressing opioid use and abuse in the workplace. In 1988, the federal government passed the Drug-Free Workplace Act. The law requires that any federally funded agencies meeting certain criteria must have and maintain a DFWP. Components include a formal written drug-free workplace policy, employee education, reporting requirements, violations notification and specific response, and ongoing review (SAMHSA, 2015). Companies with a DFWP achieve a significant decrease in workplace injuries compared with companies without a program, have higher rates of abstinence, and demonstrate a performance benefit (Slaymaker & Owen, 2006; Weisner et al., 2009; Wickizer, Kopjar, Franklin, & Joesch, 2004). Many private employers have adopted the standards put in place by this legislation. It is important that occupational health nurses assist employers to reevaluate and modify the DFWP to address the use of prescription opioids at work. The first step is to develop a clear and well-written substance abuse policy. The policy should spell out what is and is not acceptable for prescription drug use; the employee’s obligation in using prescription drugs and safe job performance; and consequences of prescription drug misuse along with how employers will identify, evaluate, treat, and apply any disciplinary action. Employers should seek input from legal counsel, Human Resources, and the company Medical Review Officer to ensure that all federal and state-specific guidelines, including Americans With Disabilities Act (ADA), are reflected in the policy (NSC, 2015; SAMHSA, 2017a).
In the revised substance abuse policy, employers must also clarify the terms and indications for drug testing. In doing so, the employer should not overlook the possibility that they may still be utilizing a five-panel test (opiates/heroin, cocaine, tetrahydrocannabinol (THC), phencyclidine (PCP) amphetamines) that may miss oxycodone and other abused drugs. Employers should consider adopting a seven-panel drug test including benzodiazepines, opiates, oxycodone, methadone, cocaine, amphetamines, and THC (NSC, 2015). The U.S. Department of Transportation (U.S. DOT) recently updated the list of substances for standardized drug testing to reflect the current state of substance abuse in the US. As of January 1, 2018, the U.S. DOT added hydrocodone, hydromorphone, oxymorphone, and oxycodone to its drug testing panel (Government Publishing Office, 2017). Occupational health nurses are the best individuals to guide employers through revision of a DFWP policy. They are usually familiar with the scope and content of the DFWP and can assist employers to make appropriate changes to better address substance misuse.
Employee and Supervisor Education
Employees who are candidates for opioid prescriptions should understand safe use of these drugs and be able to discuss concerns with the health care provider as soon as opioids are recommended. Consequently, the occupational health nurse should educate employees about the risk of dependency and addiction to opioids, potential signs of abuse, and sources of assistance. Individuals should be encouraged to ask their health care provider whether the opioid will interfere with safe job performance and whether a nonopioid medication could be prescribed instead. Resources to help train employees can be found in Table 4. The occupational health nurse should also discuss safe practices at home. Prescription opioids should be stored securely. Left over opioid prescriptions should be discarded right away. They should not be put in the trash, in the toilet, or down the drain; rather, they should be taken to a pharmacy or Drug Enforcement Agency take-back program or to a police department collections box. Opioids should not be taken with alcohol, sedatives, or other psychotherapeutic medications. Unused pills should not be shared with family or friends nor should anyone borrow the bottle of pills (The American Medical Chest Challenge, 2010; NSC, 2015; Randolph, 2017). Formal training should be conducted with supervisors and management on current trends in drug use. They should also possess a thorough understanding of any changes in the employer workplace drug use policy, signs of impairment, and how to respond to include drug testing. Capable staff will ensure that substance abuse issues are handled in a sensitive, uniform way. Frontline management are key in helping to identify and obtain help for those struggling with a substance use disorder (NSC, 2015).
Access to Treatment
Employee assistance programs (EAPs) traditionally provide employees with confidential services to assist them in dealing with personal or work-related problems that may affect their health, family life, or work performance. EAPs can also support employees with confidential access to treatment for substance misuse and addiction. MAT is the recommended approach for opioid addiction incorporating behavioral therapy, counseling, and certain medications to help detox and stop cravings. The behavioral health portions of health insurance and EAP contracts should be evaluated to ensure that employees are covered for issues related to nonmedical prescription drug use (NSC, 2015; Randolph, 2017; SAMHSA, 2017a). Occupational health nurses are often the conduit between the EAP and the employer and should become the expert on how this resource can be utilized to help workers.
Conclusion
The opioid epidemic presents unique challenges to employers. Opioid use is both a safety and health issue and can impact employer business costs. Opioids prescribed for work-related injury can result in impairment and increase workplace accidents and errors. Misuse may result in addiction and overdose. Cost to businesses includes but are not limited to lost time and increased workers’ compensation costs, productivity declines related to poor performance and absenteeism, and increased employer health plan costs. Occupational health nurses are in a key position to help address these challenges using recommended strategies. Occupational health nurses should begin with assessing their individual workplaces and determining how to respond to the “Call to Action”: working with benefit and health care providers to reduce access to opioids; modifying drug-free workplace policies to address the use of prescription drugs; updating training for workers and management; and ensuring access to quality treatment. Occupational health nurse efforts to take action will help to protect those in the workplace and prevent the spread of the epidemic in the community at large.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Sheila A. Higgins is an occupational health nurse consultant with the Occupational and Environmental Epidemiology Branch, North Carolina Division of Public Health in Raleigh, NC.
Jill Simons has been an occupational health nurse for 20 years and has worked in manufacturing, municipal, health care, and finance settings. She is currently an occupational health manager with Procter & Gamble Co. in Greensboro, NC.