
Abstract
Manufacturing workers comprise 8.8% of the total U.S. workforce representing a sizable population for disease prevention and health promotion by occupational health nurses within worksite wellness programs. The purpose of this study was to examine the relationship between perceived health status and objective health status including existing chronic disease among rural manufacturing workers. Rural manufacturing workers (n = 114) completed a general health survey and consented to a retrospective chart review. All were participants in a direct incentive wellness program with biometric data available. The majority of participants were males between the ages of 46 and 60 years, and nearly half of the sample had a college degree. A statistically significant difference was observed between number of chronic diseases and lower perceived health status. These findings have implications for occupational health nurses and other health care providers to identify workers at risk for chronic illness through self-perceived health status assessment.
Manufacturing in the United States (U.S.) is an essential part of the economy (Scott, 2015). U.S. manufacturing employees consist of 12 million employees or 8.8% of total U.S. employment (Scott, 2015). Mechanically, physically, or chemically transforming materials or elements into new products is the basis of manufacturing (U.S. Department of Labor, 2016b). Manufacturing employees constitute a large and accessible workforce for introducing disease prevention and promoting health and wellness to combat the burden of chronic illness in the U.S. (Newman et al., 2015; Office of Disease Prevention and Health Promotion, 2018). Manufacturing organizations both large and small may influence health behaviors in the workplace through integrated wellness programs (Egelhoff, Katz, Brosseau, & Hennrikus, 2015; Newman et al., 2015).
Currently, the burden of chronic illnesses in the U.S. is 78% of the total health care spending and is predicted to increase over the next 20 years (DeVol & Bedroussian, 2007). Obesity and related chronic illnesses cost employers around US$93 billion every year in health insurance claims (Centers for Disease Control and Prevention [CDC], 2016). The productivity loss related to chronic illness in companies with 1,000 or more employees, including medical expenditures and absenteeism, is estimated at US$277,000 per year (CDC, 2016). Identifying employees at risk for developing chronic illnesses has the potential to reduce health care costs and improve the quality of life for U.S. manufacturing workers. Worker safety is directly related to the presence of chronic illness and/or disease in workers with conditions resulting in extremity paresthesia, musculoskeletal pain, limitation of movement, and declining vision and/or hearing (Loeppke et al., 2013). Aging manufacturing workers are especially at risk of lost work time and injury with physical limitations resulting from chronic disease (Loeppke et al., 2013).
General health status, including an assessment of an individual’s self-rated health status, is one of four foundational health measures identified as a national objective for healthier Americans by the Healthy People 2020 campaign (U.S. Department of Health and Human Services, 2010). Self-rated health is defined as a single health measure where individuals rate their current health status most commonly using a 5-point scale rating from excellent to poor (Wu et al., 2013). The self-rated health measure has been widely studied across Western populations (Wu et al., 2013) and used by public health researchers (Bombak, 2013). Wu et al. (2013) concluded that self-rated health can serve as a global measure of a population’s health status. There have been few studies evaluating self-rated health within the manufacturing population. Increasing the employee awareness of health is complex, and exploring sociodemographic factors is not within the scope of this study.
One important aspect of a self-rated health status is the relationship between an individual’s response and its association with morbidity and mortality. Individuals who self-report fair or poor health have a higher risk of mortality (DeSalvo, Bloser, Reynolds, He, & Muntner, 2006; Halford et al., 2012). Individuals who reported poor self-rated health status have been shown to have a 2-fold higher mortality rate compared with individuals who reported having excellent health after adjusting for comorbidities (DeSalvo et al., 2006). Self-rated health status has been found to be a strong predictor of mortality in adult populations despite the age of the individual (DeSalvo et al., 2006; McEwen et al., 2009). Self-rated health status may provide important information into an individual’s health problems that are not supplied by an objective assessment (McEwen et al., 2009). Self-rated health is a simple self-administered tool, which has the potential to measure internal perceptions (Bombak, 2013).
Although studies have been conducted among many populations, little evidence involves the specific population of rural manufacturing workers and their perceived health status. Halford et al. (2012) reported a significant relationship between lower self-rated health status and increased use of sick leave, disability benefits, hospital admissions, and mortality. Defining the rural manufacturing worker’s perceived health status is an important addition to research within this specific population. In addition, comparing the perceived health status with objective health findings will allow definition of potential relationships in the manufacturing population.
The purpose of this study was to examine the relationship between perceived health status and objective health status including existing chronic diseases among rural manufacturing workers. First, the difference among rural manufacturing workers’ perceived health status across age, gender, educational level, and presence or absence of reported chronic diseases was examined. Second, the difference in the perceived health status of rural manufacturing workers with the objective health measures (body mass index [BMI], blood pressure, lipid values) was explored. Finally, the correlation of self-rated health status and the number of reported chronic diseases was evaluated.
Method
Study Design
A descriptive cross-sectional design was conducted. The manufacturing setting included a primary care clinic accessible to and utilized by employees located within the facility. Services offered included disease prevention counseling and laboratory evaluation for employer contributions to the individual employee health savings account. The corporate email system was chosen for dissemination of the survey as all employee groups had work email. No specific employee groups were targeted. All employees had existing employee medical records, with objective data acquired in the previous 12 months, and no outside health data were accessed. The consent form for the study gave explicit consent of the participant for the primary researcher to access the participant’s medical chart. The data were de-identified after collection. Participants were informed that their participation was completely voluntary and that they could stop at any time during data collection. Incentives were given for participating in the study. Participants were provided an opportunity to enter drawings for retail gift cards and an electronic tablet for completing the consent form and health survey. Letters of cooperation and corporate approval were obtained from the manufacturer, and Western Kentucky University’s institutional review board (IRB) approval was obtained.
Population and sampling methods
A convenience sample was recruited from a large manufacturing facility located in a rural southern region of the U.S., which currently employs just over 1,000 people. All employees of the facility were invited by email to participate with the following inclusion criteria required: (a) must be a current full-time employee and (b) must be over the age of 18 years. The specific aims, purpose, and goals for the study were explained through an email letter and through scheduled meetings with department leaders and representatives. Eligible participants were then sent the self-rated health questionnaire to be completed online. After completed questionnaires were received, a retrospective medical chart review was conducted to collect the necessary objective data.
Measures
An electronic format of the Short Form Health Survey-36v2 (SF-36v2) (license purchased) delivered by employee email was utilized. The SF-36v2 Health Survey was self-administered by electronic survey with an option provided for paper and pencil for those who preferred that method of administration. The SF-36v2 focuses on eight health concepts (Ware, 2000). Our study focused on the single health concept of general health perception and perceived change.
Reliability of the SF-36v2 has been established in numerous studies using both internal consistency and test–retest (Brazier et al., 1992; McHorney & Ware, 1994; McHorney, Ware, & Raczek, 1993; Ware, 2000). The overall reliability in these studies exceeded a Cronbach’s alpha of .80 and some exceeded .90 (Brazier et al., 1992; McHorney & Ware, 1994; McHorney et al., 1993; Ware, 2000). General health perception Cronbach’s alpha is .80 (Jenkinson, Stewart-Brown, Petersen, & Paice, 1999). The SF-36v2 has been validated extensively involving more than 130 diseases including the assessment and comparison of disease burden as well as treatment effectiveness in chronic health conditions (Bayliss et al., 2012; Fortin et al., 2004; Ware, 2000).
To compare the perceived health status with the identified variables, five questions were used from the health survey that corresponded with health perception. The items included, “Your health is . . .”; “Compared with 1 year ago, your health is . . .”; “I am as healthy as anyone I know . . .”; “I expect my health to get worse . . .”; My health is excellent . . . .” These questions were chosen because they identify the participants’ perception of their overall health. They further identify perceptions of overall health compared with 1 year ago, compared with next year, and compared with their peers. These questions were chosen after consultation with the statistician. Some questions were recoded for analysis, so each question response was ordered best possible to worst possible across a 5-point Likert-type scale. A single summed score was obtained from the selected questions. A higher total score showed a higher perceived health status. Cronbach’s alpha for selected five items was acceptable, reported at .70.
The independent variables measured were age, gender, educational level, blood pressure, BMI, lipid values, and number of chronic diseases. A retrospective chart review provided objective health data of blood pressure measurement, BMI, and lipid values. Blood pressure was defined as normal (<120/80), prehypertensive (120-139/80-89), or hypertensive (140/90 and greater) according to the American Heart Association (AHA; 2016). BMI was defined as underweight (<18.5 kg/m²), normal/healthy weight (18.5-24.9 kg/m²), overweight (25.0-29.9 kg/m²), and obese (30.0 kg/m² and greater; CDC, 2015). Total cholesterol levels were defined as normal <200 mg dL or high in levels of 200 mg dL or greater; triglyceride levels were defined as normal <150 mg dL or high in levels of 150 mg dL or greater; high-density lipoprotein (HDL) levels were defined as normal >40 mg dL or low in levels of 40 mg dL or less; and low-density lipoprotein (LDL) levels were defined as normal <100 mg dL or high in levels of 100 mg dL or greater (Jellinger et al., 2012).
Data Analysis
The Statistical Package for the Social Sciences (SPSS) version 24 (IBM Corp., Armonk, NY, USA) was utilized with an alpha level set at .05, for all statistical tests. Descriptive statistics were used to describe the study population. t tests were used to compare the participant’s perceived health status with gender and the presence or absence of a chronic disease. ANOVA was used to compare the participant’s perceived health status among age groups, educational levels, BMI, blood pressure, and lipid levels. Pearson’s correlation coefficient was used to identify correlation among the number of chronic diseases reported by the participant and perceived health status including the five questions previously described.
Results
Participant Characteristics
The manufacturing facility utilized for this study had approximately 1,100 employees. In total, 139 full-time adult participants provided written consent and were sent the self-rated health questionnaire. A total of 114 questionnaires were completed with subsequent medical chart reviews conducted. Participant ages ranged from 23 to 72 years, with the largest participant group being the 46-60 age group (n = 65; 57%; Table 1). There were 77 participants who were male (68%) and 37 were female (32%).
Characteristics of Study Participants (n = 114)
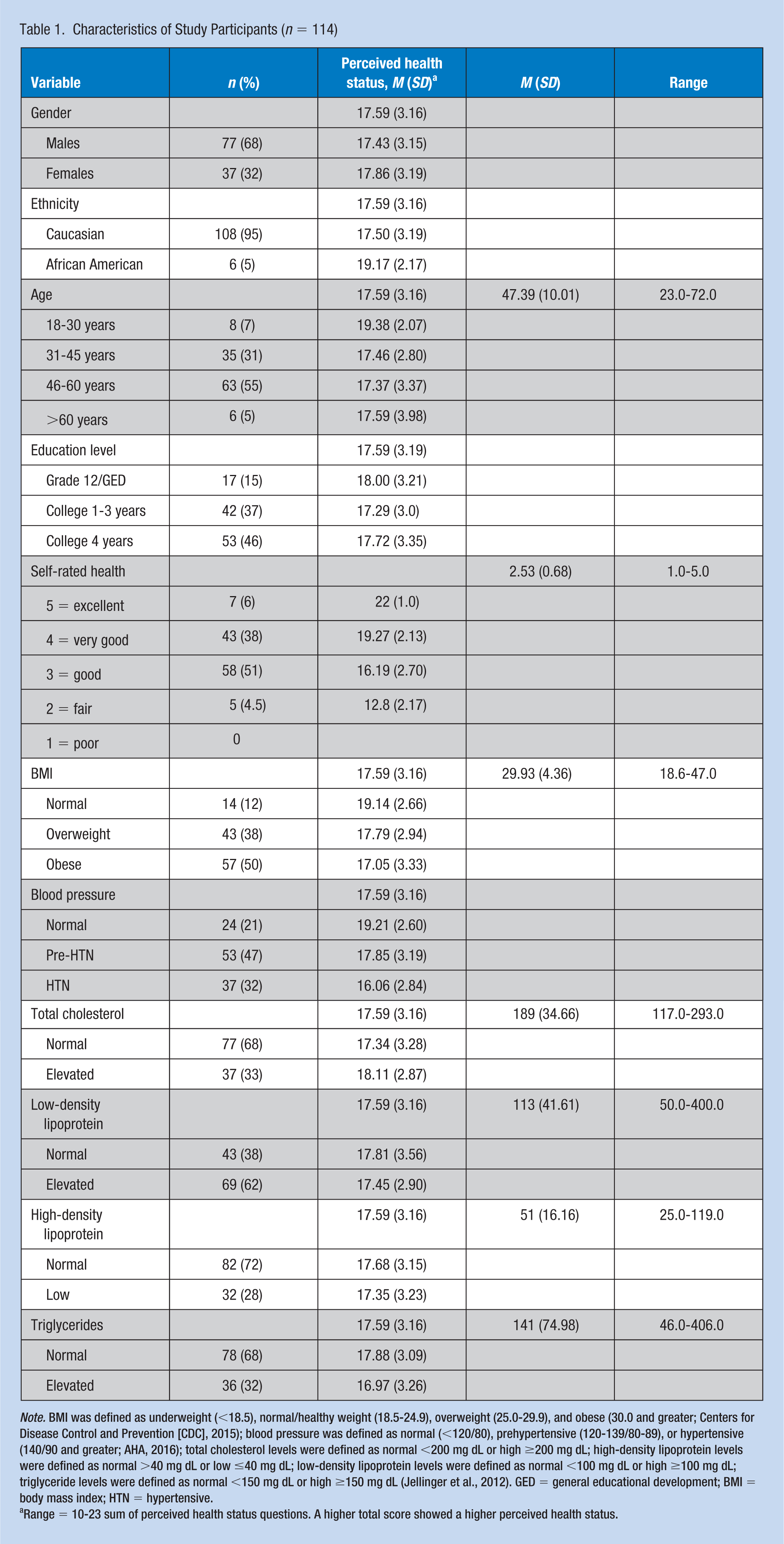
Note. BMI was defined as underweight (<18.5), normal/healthy weight (18.5-24.9), overweight (25.0-29.9), and obese (30.0 and greater; Centers for Disease Control and Prevention [CDC], 2015); blood pressure was defined as normal (<120/80), prehypertensive (120-139/80-89), or hypertensive (140/90 and greater; AHA, 2016); total cholesterol levels were defined as normal <200 mg dL or high ≥200 mg dL; high-density lipoprotein levels were defined as normal >40 mg dL or low ≤40 mg dL; low-density lipoprotein levels were defined as normal <100 mg dL or high ≥100 mg dL; triglyceride levels were defined as normal <150 mg dL or high ≥150 mg dL (Jellinger et al., 2012). GED = general educational development; BMI = body mass index; HTN = hypertensive.
Range = 10-23 sum of perceived health status questions. A higher total score showed a higher perceived health status.
In total, 48% (n = 54) reported having a 4 year college degree or higher. The majority of participants identified themselves as Caucasian (n = 108), followed by African Americans (n = 6). No other races were reported. In addition, 81 (71%) participants reported at least one chronic disease.
Perceived Health Status and Age, Gender, Educational Level, or Chronic Disease
There was no significant difference in perceived health scores for males, M = 17.45, SD = 3.15, and females, M = 17.86, SD = 3.19; t(112) = −0.65, p = .52, two-tailed. However, there was a significant difference in scores for those who reported one or more chronic diseases (M = 17.11, SD = 3.27) compared with those who reported no chronic diseases, M = 18.84, SD = 2.48; t(112) = −2.66, p = .009, two-tailed (see Table 2).
Difference in Perceived Health Status across Gender, Age, Educational Level, and Presence/Absence of Chronic Disease
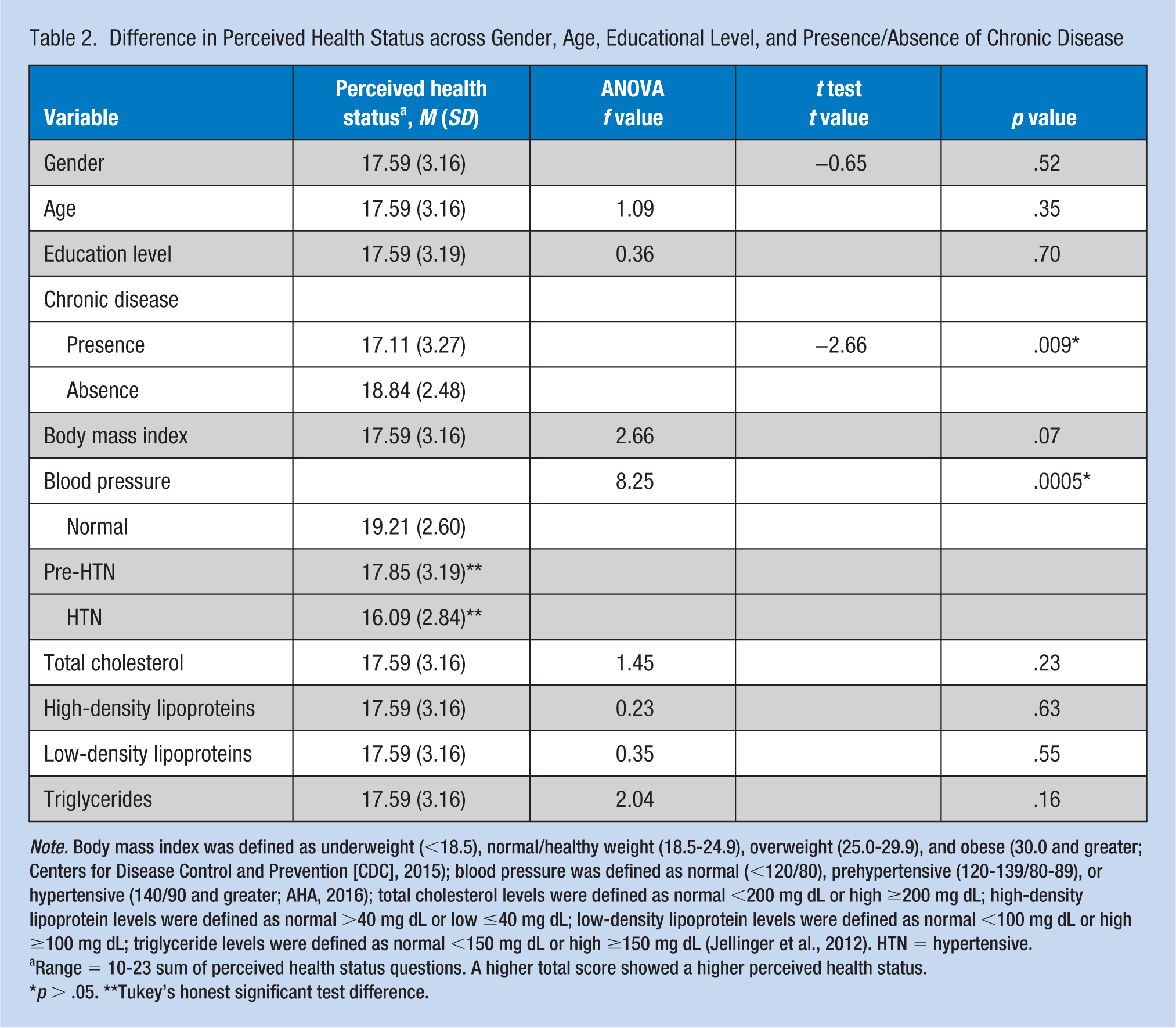
Note. Body mass index was defined as underweight (<18.5), normal/healthy weight (18.5-24.9), overweight (25.0-29.9), and obese (30.0 and greater; Centers for Disease Control and Prevention [CDC], 2015); blood pressure was defined as normal (<120/80), prehypertensive (120-139/80-89), or hypertensive (140/90 and greater; AHA, 2016); total cholesterol levels were defined as normal <200 mg dL or high ≥200 mg dL; high-density lipoprotein levels were defined as normal >40 mg dL or low ≤40 mg dL; low-density lipoprotein levels were defined as normal <100 mg dL or high ≥100 mg dL; triglyceride levels were defined as normal <150 mg dL or high ≥150 mg dL (Jellinger et al., 2012). HTN = hypertensive.
Range = 10-23 sum of perceived health status questions. A higher total score showed a higher perceived health status.
p > .05. **Tukey’s honest significant test difference.
There was no statistically significant difference in perceived health status scores for the six education groups, F(2, 110) = 0.36, p = .70. In addition, there was no statistically significant difference in perceived health scores for the four age groups, F(2, 111) = 1.09, p = .35.
Perceived Health Status and Objective Health Measures
There was no statistically significant difference in perceived health status scores for the four BMI groups, F(2, 111) = 2.66, p = .07 (see Table 2). There was a statistically significant difference in perceived health status scores for blood pressure groups, F(2, 111) = 8.25, p = .0005 (see Table 2). Post hoc comparisons using the Tukey’s honestly significant difference (HSD) test indicated that the mean score for those with normal readings (M = 19.21, SD = 2.60) was significantly different from those with hypertensive readings (M = 16.09, SD = 2.84). Significant difference was also indicated in the mean score for those with prehypertensive readings (M = 17.85, SD = 3.19) compared with those with hypertensive readings (M = 16.09, SD = 2.84). Those in the normal group did not differ significantly with those in the prehypertensive group.
Lipid levels were compared with perceived health scores among the groups, total cholesterol: F(1, 111) = 1.45, p = .23; HDL: F(1, 111) = 0.23, p = .63; LDL: F(1, 110) = 0.35, p = .55; triglycerides: F(1, 110) = 2.04, p = .16. There was no statistically significant difference among the lipid levels.
Perceived Health Status and Number of Chronic Diseases
There was a moderate, negative correlation between the perceived health score and the number of chronic diseases, r = −.34, n = 114, p = .0002, with lower levels of perceived health status scores associated with an increased number of reported chronic diseases (data not shown). The most commonly reported chronic diseases were high blood pressure, high cholesterol, and diabetes.
Discussion
This study examined the relationship between perceived health status and objective health measures among rural manufacturing workers in a single U.S. plant. Perceived health status scores were compared with objective health findings (BMI, blood pressure, and lipid values) and other self-reported variables (age, gender, education level, and chronic diseases). Number of chronic diseases and higher blood pressure readings were found to be significantly related to lower perceived health status scores, which is consistent with the literature (Wu et al., 2013). However, variables such as age, gender, education level, BMI, or lipid values showed no statistical significant difference self-rated health within this study and are consistent with the finding reported in DeSalvo et al. (2006). About 48% of the manufacturing workers in this study reported having a bachelor’s degree or higher; this U.S. trend of hiring factory workers with higher education levels may be related to an increasing use of computer technology (Selingo, 2017).
The relationship between lower perceived health status scores and reported chronic diseases in this study is in agreement with previous population-based studies (Harrington et al., 2009; Wu et al., 2013). One study found that lower scores have also been associated with any doctor diagnosed illness within the past 12 months (Harrington et al., 2009). Not only was a significant relationship identified between lower perceived health status scores and report of a chronic disease, it was further identified in this study that the perceived health status score of rural manufacturing workers was lower with each additional chronic disease reported. These findings are supported by previous research that many chronic diseases are strongly associated with a lower rated perceived health status (Molarius & Janson, 2002). These include such chronic diseases as cancer, rheumatoid arthritis, neurological disease, depression, and cardiovascular disease (Harrington et al., 2009; Molarius & Janson, 2002). This may explain the significance in lower perceived health status scores in participants with multiple chronic diseases. Increased chronic diseases may lead to a poorer outlook on daily as well as long-term health. The reasons associated with lower perceived health status and the increased number of chronic diseases certainly warrants additional investigation within this population.
Along with chronic diseases, blood pressure readings were also found to be significantly related to lower perceived health status scores in this study. Previous population-based studies are in accordance with this study’s findings (Shin, Shin, & Rhee, 2012). Individuals with hypertension have a poorer perceived health status (Shin et al., 2012).
A between-groups analysis was performed which identified a significant difference in perceived health status scores and higher blood pressure readings. No significant difference was found between the normal and prehypertension groups; however, that was not the case between the remaining groups tested. When compared with both the normal blood pressure group and the prehypertension group, the hypertension group had significantly lower perceived health status scores. This finding is consistent with Wu et al. (2013) reporting a significant increase in disease with a lower perceived health status. Furthermore, the perceived health status scores went down as the blood pressure readings went up. This identifies an area of opportunity for onsite work education programs specifically focused on the importance of blood pressure control in preventing chronic diseases related to hypertension.
The rates of overweight and obese individuals compared with the general population within that state differ from the findings in this study. In Kentucky, 66.2% of adults are overweight (BMI: 25 or greater) and 31.3% are obese (BMI: 30 or greater; CDC, 2016). In this study, the participants are 37.5% overweight (BMI: 25 or greater), and 50% are obese (BMI: 30 or greater). The number of obese participants far exceeded the state average by almost 20%. Only 12.5% of the participants were considered normal or healthy weight. This is an area of focus in improving the health of these rural manufacturing workers.
Interestingly, many studies show significant evidence to support that higher levels of BMI is a predictor of lower perceived health status scores (Haddock et al., 2006; Kwasniewska, Kaleta, Dziankowska-Zaborszczyk, Drygas, & Makowiec-Dabrowska, 2007; Phillips, Hammock, & Blanton, 2005; Prosper, Moczulski, & Qureshi, 2009). Yet, even though 50% of this study’s participants were considered obese, none of the participants in this study rated their general health as poor, and only five participants rated their general health as fair. To further support this study’s findings, a study conducted in rural Appalachia, which included parts of Kentucky, Tennessee, and West Virginia among other states, found that health perceptions compared with objective health data to be incongruent (Griffith, Lovett, Pyle, & Miller, 2011). This study’s findings provide an area of opportunity for education about the risks of obesity on health and wellness.
Previous studies have identified relationships of decreased perceived health status scores for clinical disease biomarkers such as elevated serum lipid results and other factors such as age, obesity, gender, and education level (Molarius et al., 2006; Shin et al., 2012; Wu et al., 2013). This study; however, found no significant differences within these variables when compared with perceived health status scores. A study conducted in rural Idaho concluded there were no consistent significant differences in perceived health status when compared with age and gender (Cleary & Howell, 2006).
This study showed both positive and negative lipid data for this group of participants. The participants in this study exceeded the recommendations for total cholesterol, triglycerides, and HDL. However, LDL levels fell short of the less than 100 recommendation. The occupational health staff at this facility should take note of the positive results concerning lipid levels and continue their efforts to prevent abnormal lipid levels.
There were several limitations of this study. The sample size may not be representative of the manufacturing population; however, this study did consist of 10% of the research site population. Another limitation involves the self-report of items of the health data as participants may not have answered accurately. The addition of objective data helped to support the study findings as well as the findings of a recent study that validated the self-report of health data such as diabetes (Schneider, Pankow, Heiss, & Selvin, 2012). The research site has a dedicated health and wellness program onsite. The participants receive monetary rewards based on specific health goals as an incentive to improve and maintain health status. The employees’ health perceptions may have been affected and reflect the positive influences of the wellness program and monetary incentives. Finally, the participant answered questions related to their current health status, however, objective data may have been 6 months old. Despite these noted limitations, this study offers new insight into how rural manufacturing workers perceive their health.
Implications for Occupational Health Nursing Practice
The findings from this study identified a relationship between perceived health status of rural manufacturing workers and the report of a chronic disease and elevated blood pressure readings. Specifically, a relationship was identified in the number of chronic diseases reported as well as how high the blood pressure was recorded. Number of chronic diseases and higher blood pressure readings were found to be significantly related to lower perceived health status scores. Not only was a significant relationship identified between lower perceived health status scores and report of a chronic disease, it was further identified in this study that the perceived health status score of rural manufacturing workers was lower with each additional chronic disease reported. These findings; therefore, have implications for occupational health nurses and other health care providers who design, implement, and maintain health and wellness programs within a manufacturing facility. Primary care providers will also discover these findings to be helpful in caring for working aged individuals especially those with chronic diseases including elevated blood pressure. Occupational health nurses should evaluate the perceived health status of their employees and plan health promotion programs to address those groups with lower perceived health status. The use of this simple self-administered tool has the potential to reduce morbidity and mortality, and occupational health nurses play a key role in disease prevention and health promotion of their employees. As manufacturing workers have the highest tenure among all major industries at 5.3 years, occupational health nurses should seize this opportunity to improve employee health (U.S. Department of Labor, 2016a).
Occupational health research must continue to focus on the health of the rural manufacturing worker and further examine perceived health status and its relationship to the health of the employee. The identification of factors that contribute to the adoption of healthier behaviors in employees with poor self-rated health is one area of future research. Future research also might include the identification of interventions that target aging workers with specific chronic illnesses.
Conclusion
Employee health is changing due to the increasing age in the workforce (Anderko et al., 2012). Many workers are burdened with one or more chronic diseases, which makes management of medical conditions more difficult. Therefore, wellness interventions by employers can be very valuable by affecting many diseases at once (Anderko et al., 2012). Obtaining an employee’s perceived health status may provide additional information to assist the occupational health nurse in the management of employee health.
Applying Research to Practice
Manufacturing employees constitute a large and accessible workforce for introducing disease prevention and promoting health and wellness within worksite wellness programs. The relationship between perceived and objective health status in rural manufacturing workers was examined. The number of chronic diseases and higher blood pressure readings were significantly related to lower perceived health status scores. The use of a self-administered perceived health status tool has the potential to reduce workers’ morbidity and mortality by identifying employees at risk. Occupational health nurses could evaluate the perceived health status of their employees to design and implement health promotion programs for these workers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Stacy Logsdon is a practicing family nurse practitioner in a rural manufacturing facility in Kentucky. Her practice focuses on occupational medicine as well as prevention and management of chronic diseases.
M. Laurie Branstetter is an Associate Professor in the School of Nursing at WKU and a family nurse practitioner in a rural health clinic. Her current research interests involve medically underserved populations.
Eve Main is a Professor in the School of Medicine at WKU, a program coordinator, and a family nurse practitioner. Her current research interests include preventative health behaviors, dementia, and the social determinants of health.