
Abstract
This study explored the relationship between effort-reward imbalance (ERI) at work and work productivity among hotel housekeepers. A community-based approach was used to recruit 23 hotel housekeepers who completed the ERI and Work Performance Questionnaires. Work productivity was determined by combining self-report absenteeism and presenteeism. More than 40% of the participants reported high ERI (ERI >1). Also, 59.1% reported low work productivity. Interestingly, despite the individualized high reports of ERI and low work productivity, correlation analysis showed that high ERI was correlated with high presenteeism and work productivity as a whole. This is the first study to explore work productivity among this worker group. Despite the small sample size and the cross-sectional nature of the study, this study points to the need for organization-based interventions to not only improve employee health but also their work productivity.
Keywords
In light of the rapidly growing global capital market, the hospitality industry continues to be at the forefront of the economy both locally and internationally. Hotel housekeepers (often referred to as hotel room cleaners or hotel maids) comprise the largest number of workers in the traveler/accommodations or hospitality industry and are the primary contributor to customer loyalty and thus the growth of the industry (Bureau of Labor Statistics, 2017; Kandampully & Suhartanto, 2000; National Occupational Research Agenda [NORA], 2012). Despite being a driving force in industry growth, hotel housekeepers, a representative group of the low-wage workforce, experience higher rates of occupational health exposures, contingent work, and poor health outcomes (Buchanan et al., 2010; Bureau of Labor Statistics, 2014, 2015; Premji & Krause, 2010; Sanon, 2014). Buchanan et al.’s (2010) review of Occupational Safety and Health Administration (OSHA) log incidents among unionized hotels showed that hotel housekeepers had the highest injury report rate (7.9), highest acute trauma rate (3.9/100), and highest work-related musculoskeletal disorder (WMSD) rate (3.2/100). Hotel housekeepers have also reported high rates of pain and hypertension prevalence and poor hypertension management (Krause & Arias, 2015; Krause, Scherzer, & Rugulies, 2005; Sanon, 2013). NORA includes hotel housekeepers as a vulnerable group of workers in the service industry meriting public attention (NORA, 2013, 2015).
Given the work characteristics of hotel housekeepers, low work productivity is expected. Previous studies have shown a strong relationship between work demands and work productivity (Alavinia, Molenaar, & Burdorf, 2009; Lerner et al., 2003). For example, Alavinia et al. (2009) found that “Lack of job control was the most important factor associated with workers’ productivity loss at work” (p. 53). To date, no published studies have explored how work characteristics and work demands (work stress) of hotel housekeepers affect their health and in turn their ability to physically come to work and work productively. The goal of this study was to explore effort-reward imbalance (ERI) and work productivity among a group of hotel housekeepers.
ERI Model
The ERI model originated in the field of sociology with Siegrist and colleagues (Siegrist, 1996). This model originally was used to predict and explain the onset of cardiovascular-related outcomes (Siegrist, Siegrist, & Weber, 1986). However, its use has been expanded to include the prediction of other health outcomes such as mental health (Vegchel, De Jonge, Bosma, & Schaufeli, 2005). According to the model, work is crucial to the fulfillment of individual self-regulatory needs including self-efficacy, self-esteem, and self-integration (Siegrist et al., 1986).
The ERI model emphasizes that work stress occurs when an imbalance between high effort and low control exists (Siegrist, 1996; Siegrist et al., 1986; Siegrist et al., 2004). Effort refers to job demands and obligations of workers (see Figure 1). Reward refers to money, esteem, job security, and career opportunities. An imbalance between the two leads to sustained strain reactions, therefore increasing the risk for poor health including development of hypertension and cardiovascular disease.
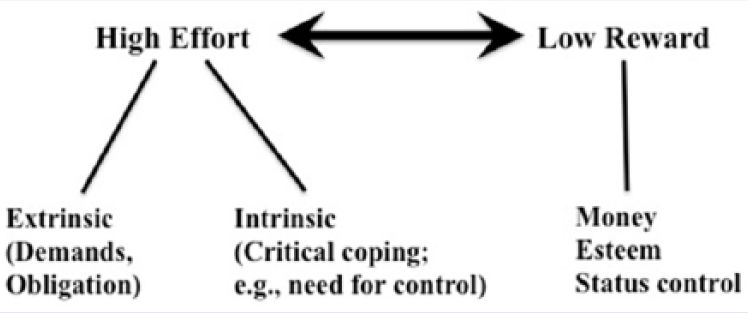
ERI model.
Three assumptions are associated with the ERI model (see Figure 2). The first assumption is that extrinsic ERI is a combination of high efforts and low rewards, which increases workers’ risk for poor health (Peter & Siegrist, 1999). The second assumption is that intrinsic overcommitment, high overcommitment, increases workers’ risk for poor health. And last, the interaction assumption hypothesizes that employees with extrinsic ERI and high overcommitment have a higher risk for poor health.
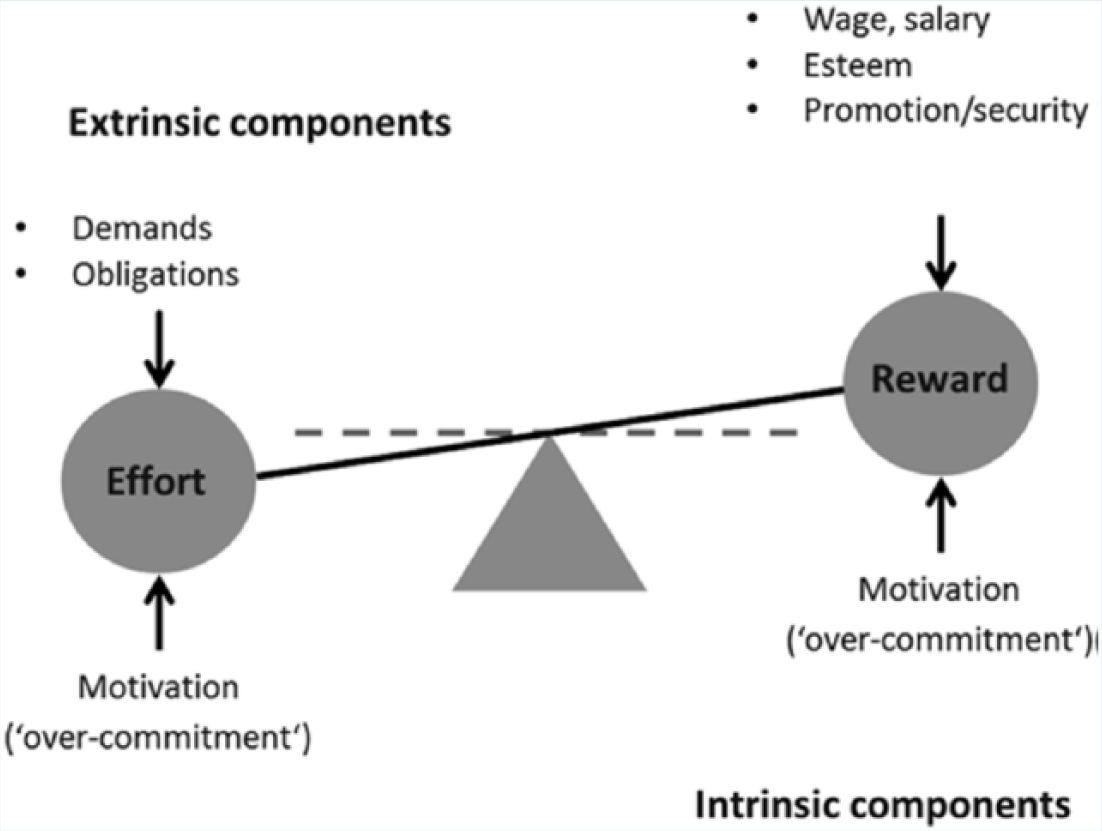
The model of effort-reward imbalance at work.
ERI and Hotel Housekeepers
To date, only one study has explored ERI among hotel housekeepers. Krause, Rugulies, and Maslach (2010) conducted a study exploring the relationship between ERI and self-rated health (SF 36) among hotel housekeepers. They found that 50% of study participants reported ERI and that those in the upper quartile of ERI ratio were 2 times to 5 times more likely to experience poor or fair general health. Krause et al.’s (2010) study reported on ERI in relation to health. However, no published studies have explored ERI in relation to the worker’s ability to perform at work or missing work hours or days. This study addresses this literature gap.
Work Productivity
Work productivity is based on a combination of presenteeism and absenteeism. Presenteeism is generally defined as decreased performances or effectiveness while at work and absenteeism is time lost from work (Burton & Conti, 1999). Prior studies have demonstrated a relationship between high physical workload, working environment, and health risks such as chronic diseases in relation to the loss of work productivity (Letvak & Buck, 2008; Meerding, IJzelenberg, Koopmanschap, Severens, & Burdorf, 2005; Tan & Netessine, 2014). Health-related work productivity impairments have been reported to cost U.S. employers US$225.8 billion annually (Stewart, Ricci, Chee, & Morganstein, 2003). Work productivity has not been explored among hotel housekeepers. This study is needed because the hospitality industry is entirely dependent upon these workers’ output for customer loyalty, industry ratings, and economic growth (Kandampully & Suhartanto, 2000; Lockyer, 2003).
Method
A university Institutional Review Board approved the study protocol for a feasibility pilot study that explored the researchers’ ability to collect blood samples and explore stressors among hotel housekeepers. The study used a community participatory-based approach to recruit study participants through the community, local union, and word of mouth in Michigan. During a 1 hour to 2 hour appointment, anthropometric and biometric measures (e.g., waist, hip, blood pressure measurements, and blood sample collections) were collected and participants completed a survey booklet that included the ERI questionnaire and Health’s Work Performance Questionnaire (HPQ). Written consent was required from all study participants prior to data collection.
Measures
ERI Questionnaire
The ERI questionnaire was developed by Siegrist and colleagues (Siegrist, 1996). This well validated tool is composed of 17 Likert-type-scaled items (11 items focus on rewards, and six items focus on efforts). The answers range from strongly disagree to strongly agree. Examples of questions include the following: “I have constant time pressure due to a heavy work load”; “I am treated unfairly at work”; “Considering all my efforts and achievements, I receive the respect and prestige I deserve at work”; and “Considering all my efforts and achievements, my salary/income is adequate.” An imbalance between effort and reward is determined to exist when the ratio of effort score to reward score is greater than 1 (Siegrist, 1996; Siegrist et al., 2004).
World Health Organization HPQ
The World Health Organization HPQ is a widely used measure that includes questions assessing work productivity, both absenteeism and presenteeism (Kessler et al., 2004; Kessler et al., 2003). Absenteeism is measured by hours lost per month with a higher score indicating more absenteeism. Absolute absenteeism is calculated by subtracting actual work hours from expected work hours over a 4-week period. Relative absenteeism is computed as a percentage of expected hours which ranges from a negative number (work more than expected) to 1 (always absent) (Kessler et al., 2004; Kessler et al., 2003). Presenteeism is a measure of actual performance in relation to possible performance with a higher score indicating less lost performance. Absolute presenteeism is calculated by multiplying the number “10” by actual performance, which ranges from 0 (total lack of performance) to 100 (no lack of performance). Relative presenteeism is expressed as a ratio of actual performance to the performance of most workers, which is restricted to a range of 0.25 (25% or less of other workers’ performance) to 2 (200% or more of other workers’ performance). Before combining absenteeism and presenteeism, relative hours of work is calculated as one minus relative absenteeism. The combined score is the multiplication of relative hours of work and relative presenteeism. If the total score is greater than 1, the respondent compensates for lost hours with higher work productivity (Kessler et al., 2004; Kessler et al., 2003).
Analysis
Means and standard deviations, median, and percentages were computed to describe sample demographics, ERI, absolute and relative absenteeism, absolute and relative presenteeism, and work productivity. Correlation analyses were used to examine the relationships between ERI and absolute and relative absenteeism, absolute and relative presenteeism, and work productivity. SPSS 22.0 was used for all analyses.
Results
Twenty-three individuals from different hotels participated in this study (Table 1). The average age of the sample was 42 years (SD = 11). Nearly 41% of participants were married, only 13.6% were White, 39.1% were born in Mexico or Africa, only 9.1% had some college or an associate’s degree, and only 12.9% were paid more than US$14 per hour. Thirteen percent of participants self-rated their health status as fair or poor and the SF-12 physical and mental health scores were 48 (SD = 8.7) and 46.9 (SD = 11.5). Eighty-seven percent of participants had at least one chronic disease.
Sample Sociodemographic Characteristics of Hotel Housekeeping Employees
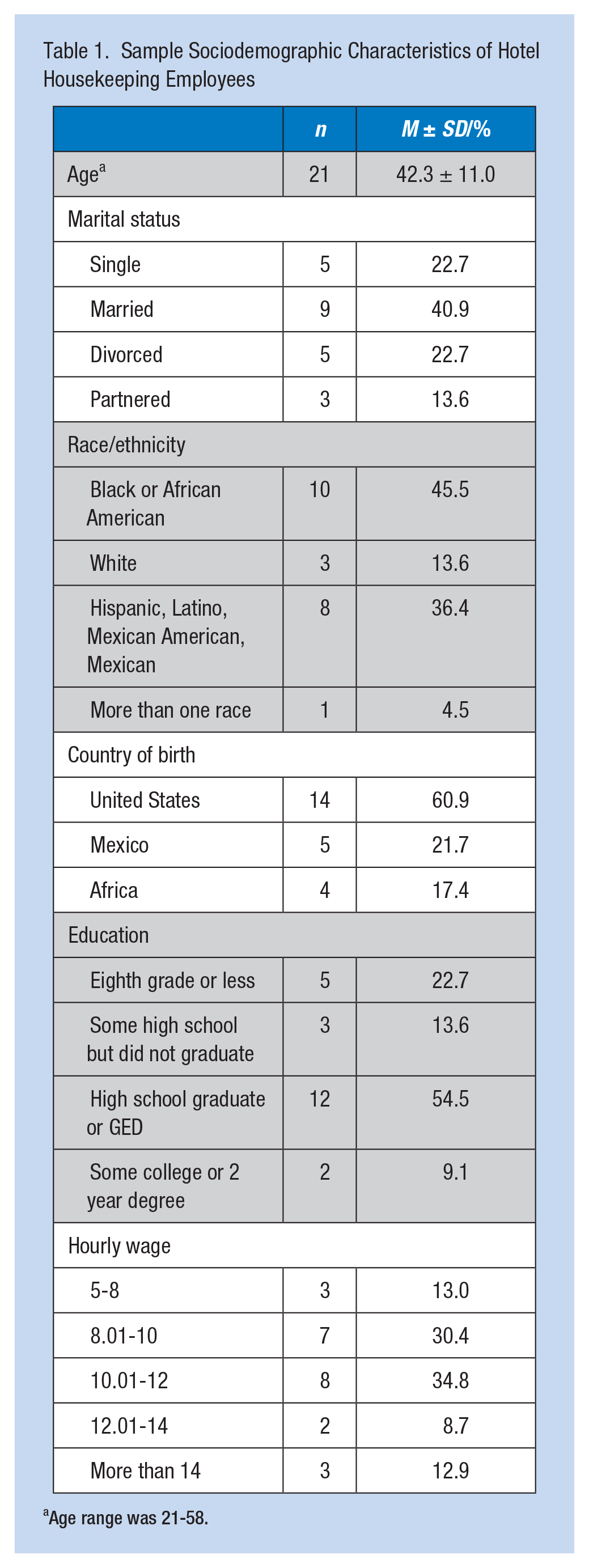
Age range was 21-58.
ERI and Work Productivity
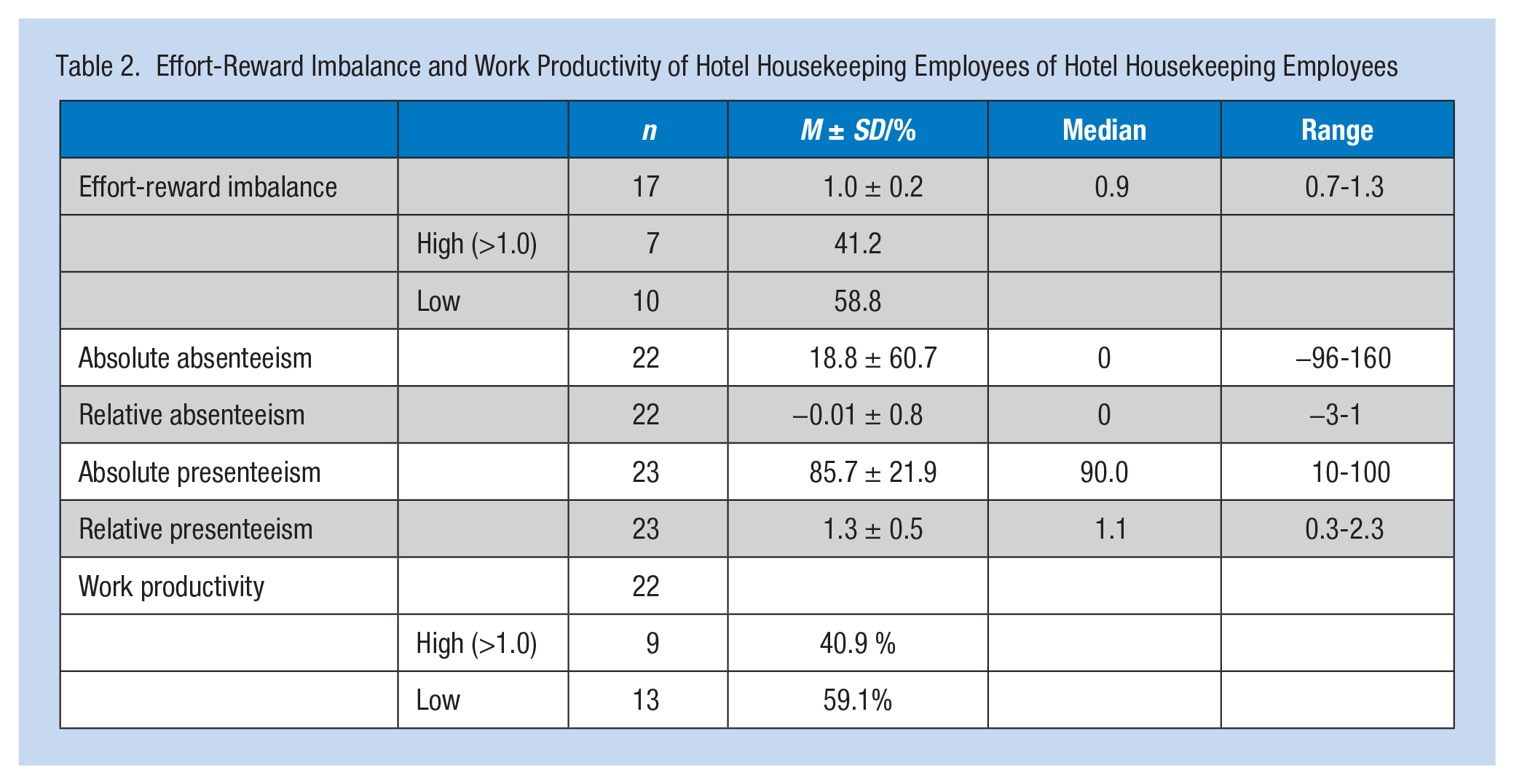
As shown in Table 2, 41.2% of participants had high ERI (>1.0) and 59.1% had low work productivity (≤1.0). The average lost work hours in the past 4 weeks was 18.8 (SD = 60.7). The correlation analyses (Table 3) showed that higher ERI was significantly associated with higher relative presenteeism (r = .50, p = .042) and higher work productivity (r = .53, p = .036). No significant correlations were found between ERI and absolute and relative absenteeism or absolute presenteeism (p > .05). The study also tested the relationships between ERI and SF-12 physical and mental health scores and found that higher ERI was significantly correlated with lower SF-12 mental health scores (r = –.50, p = .040; data not shown).
Effort-Reward Imbalance and Work Productivity of Hotel Housekeeping Employees of Hotel Housekeeping Employees
Correlations Between ERI and Work Productivity
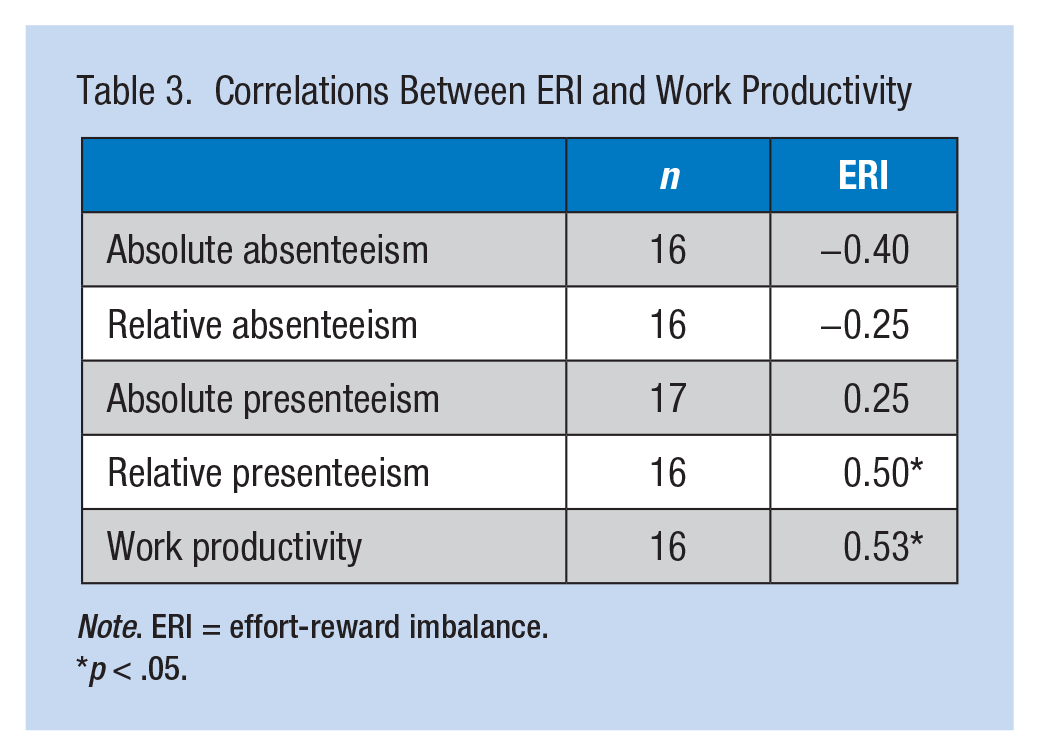
Note. ERI = effort-reward imbalance.
p < .05.
Discussion
The purpose of this study was to explore the relationship between ERI and work productivity among hotel housekeepers. Hotel housekeepers comprise the largest worker group in the hospitality industry and are the driving force behind customer loyalty and institution ratings, and thus the growth of the industry. To the authors’ knowledge, this is the first published study that explored ERI and work productivity as an outcome among this vulnerable worker group. Similar to the only previous study that explored ERI among hotel housekeepers (Krause et al., 2010), this study found high ERI among hotel housekeepers. More importantly, the study also found that more than half of study participants had low work productivity due to lost work hours or impaired work performance. For a 40-hour-work week within a month, the average lost work hours was 18.8. Study findings on low work productivity support a previous study (Meerding et al., 2005) that found workers in high physical load jobs had less productivity at work with an average 2 hour a day of lost work time.
Surprisingly, this study found that hotel housekeepers who reported high effort but little rewards were more likely to report high work performance and work productivity, which is contrary to the authors’ hypothesis initially. A possible explanation for the unexpected findings is that the HPQ is self-rated, asking participants to rate their overall work performance, perhaps resulting in reporting bias because individuals self-rate their performance better than their actual or others’ performance. However, the questionnaire does use a calibration approach via the 0 to 10 Self-Anchoring Scale to address these potential biases (Kessler et al., 2004). Despite this acknowledged questionnaire weakness, it remains a valid tool to assess workplace health and work productivity. Future research using employer-rated questionnaires, in addition to the self-rated HPQ, to assess hotel housekeepers’ working performance may better represent the actual performance of workers and the relationship between ERI and work productivity.
Limitation
A limitation of this study was the small sample size. However, this was a feasibility pilot study that assessed the researchers’ ability to explore stressors and collect anthropometric and biometric measurements among this population. Thus, this number was enough to show feasibility.
Implications for Practice
Despite the small sample size, this study is still important to occupational health researchers, policy makers, and employers because it supports previous findings that the high demanding jobs of hotel housekeepers, requiring high effort and little reward, not only can have health consequences (as shown in Krause et al.’s, 2010, study) but also economic implications because low work productivity are linked to less profit and revenues (Stewart et al., 2003). Organization-based interventions are needed to address the ERI and work productivity of hotel housekeepers. Examples of organization-based interventions may include the following: policy level changes related to workload (e.g., number of rooms to clean); consideration of compensation provided to hotel housekeepers reflective of their high occupational effort; activities that foster collegiality and increased sense of support; worker-based trainings that can increase worker skills and confidence, improving their prospects for promotion, higher wages, and career advancement; and health promotion programs.
Applying Research to Practice
Hotel housekeeping employees report high effort-reward imbalance and low work productivity. This calls for the need for occupational health professionals to partner with employers to develop organization-based interventions to address employees’ health and work productivity. Examples of organization-based interventions may include policy level changes related to workload (e.g., number of rooms to clean); consideration of compensation provided to hotel housekeepers reflective of their high occupational effort; activities that foster collegiality and increased sense of support; worker-based trainings that can increase worker skills and confidence, improving their prospects for promotion, higher wages, and career advancement; and health promotion programs.
Footnotes
Authors’ Note
The University of Michigan Institutional Review Board approved the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by the Grant or Cooperative Agreement Number, T42 OH008455, funded by the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Department of Health and Human Services.
Author Biographies
Marie-Anne S. Rosemberg is an assistant professor at University of Michigan School of Nursing with an interest in optimizing the health of low-wage service workers at risk for or experiencing one or multiple chronic conditions.
Yang Li is a doctoral student at University of Michigan School of Nursing. Her research interests focus on biological mechanisms for the impact of maternal trauma and posttraumatic stress disorders on adverse birth outcomes.