
Abstract
Using a case study, this article reviews the health risks associated with prolonged sitting and the reasons sedentary workers are at risk for musculoskeletal injuries. Other health issues associated with prolonged sitting or sedentary behavior as well as the benefits of exercise are also explored. Finally, evidence-based interventions to reduce health risks associated with prolonged sitting may increase productivity.
MN is a 56-year-old woman who has worked as an accountant for a computer company for the past 15 years. She spends at least 6 hours a day at the computer, which requires prolonged sitting. During a recent move from one office to another, MN was assisting another employee lift a cabinet when she felt a sharp pain in her left lower back. MN reported to employee health, was diagnosed with a left sacroiliac strain, and was instructed not to push, pull, or lift, but continued with computer tasks.
MN has a body mass index (BMI) of 33 and was recently diagnosed with osteoporosis for which she was prescribed bisphosphonates. She is currently taking Coumadin due to a blood clot in the left leg 3 years ago. MN is also on lisinopril for hypertension and a statin for hypercholesterolemia. She was instructed to take calcium and vitamin D supplements every day; however, she takes these medications “when I remember.” Surgical history includes a hysterectomy at the age of 39 and laparoscopic surgery for gall bladder disease 10 years ago. She denies any history of smoking or alcohol use. Her commute consists of 0.5 hour each way. On the weekends, she loves to see movies. During an average workday, MN states that she may sit at least an hour without standing but may stretch her legs.
Prolonged Sitting in the Workplace
Workplaces in the United States (U.S.) now house a number of jobs that require computer work, driving, and telephone-based activities. Office workers may spend up to three-fourths of their workday sitting (Brakenridge et al., 2016), a sedentary behavior that requires an energy expenditure of less than 1.5 metabolic equivalent of task (MET; measure of the energy and intensity of an activity; Bauman, Chau, Ding, & Bennie, 2013). The more vigorous the activity, the higher the MET. It may take longer for a sedentary employee to move from resting metabolism to working metabolism to meet the energy demands of an activity. This article reviews the health issues of prolonged sitting and sedentary lifestyles that increase employees’ risk for injury and chronic disease.
Prolonged Sitting Promotes Deconditioning and Early Muscle Fatigue
Sitting promotes deconditioning, which negatively affects employees’ abilities to meet the demands of increasingly physical workloads. Deconditioning is a form of exercise intolerance in which employees’ abilities to perform physical tasks are impaired beyond normal expectations (Quittan, 2016).
Cardiovascular issues may develop when an ordinarily sedentary employee participates in physical activity (Bauman et al., 2013). The heart may not be able to pump sufficient blood quickly to muscles for proper oxygenation, which may lead to early muscle fatigue (Wickens, Lee, Liu, & Gordon-Becker, 2011). An oxygen deficit, nutrimental depletion, and lactic acid accumulation may contribute to early fatigue, so these employees must take breaks and participate in light activities in which energy demands can easily be met by oxidative metabolism (Wickens et al., 2011), the process by which oxygen is used to transform glucose into adenosine triphosphate (ATP) in the mitochondria for energy. Inactivity may lead to less mitochondrial density in the cells (Bogdanis, 2012).
Whole body fatigue develops quickly. Fatigue, measured by a depletion of ATP and creatine phosphate, has subjective indicators (e.g., feelings of exhaustion) and objective indicators (e.g., more lactic acid and less glucose; Wickens et al., 2011). Sedentary employees may not meet the demands of an increasing workload due to their inability to transition from aerobic respiration to anaerobic respiration effectively (Wickens et al., 2011).
Local muscle fatigue may also occur (Wickens et al., 2011). Increasing workloads require adequate muscle contractions that encourage blood flow to the muscles. Early muscle fatigue may result during a transition from slow to fast myosin (Herzog, Powers, Johnston, & Duvall, 2015). Slow myosin contains many mitochondria and therefore high oxidative metabolism; fast myosin have fewer mitochondria and are less vascular with lower oxidative metabolism.
Sedentary behavior may also affect pulmonary function (Kang, Son, & Ko, 2016). Workers’ postures (e.g., slumping or kyphosis) may influence pulmonary function via the effects of gravity on the diaphragm, which impedes the movement of the diaphragm. Prolonged sitting contributes to less lung volume during inspiration. Upon expiration, muscle contraction becomes less effective. Air flow obstruction may occur due to workers’ inability to breathe deeply (Kang et al., 2016). Sedentary behavior may also contribute to muscle stiffness with reduced elasticity and less range of motion in the torso that may lead to restrictive airway disease (Kang et al., 2016).
Deconditioned workers may have impeded blood flow that prevents blood vessels from dilating and less production of nitric oxide contributing to early muscle fatigue. A subjective indicator of local muscle fatigue is pain, with objective indicators of impaired coordination of muscle actions and more muscle tremors. Fatigued muscles are more likely to suffer microtraumas and strains with overuse (Wickens et al., 2011). Muscle fatigue may also lead to ligament and tendon injuries.
Sedentary lifestyles may lead to less muscle mass and vascularization. Contributing factors include shifting from slow to fast-twitch fibers that rely more on glycolysis. Smaller mitochondrial size and less oxidative enzymes contribute to heart failure (Downing & Balady, 2011). Increased production of inflammatory mediators (e.g., tumor necrosis factor and interleukin-6) occurs in the pathogenesis of skeletal muscle wasting and fatigue (Downing & Balady, 2011).
Less muscle elasticity and atrophy contribute to muscle and joint stiffness (Bogdanis, 2012). Muscle fibers composed of sarcomeres, the functioning units of striated muscles, shorten during inactivity, which contributes to muscle stiffness (Herzog et al., 2015). Less hyaluronic acid, a major component of synovial fluid that lubricants the joints, and less blood supply may also contribute to joint stiffness. Lack of exercise may lead to joint contractures, a constriction or stiffness of joints (Moriyama, 2017).
Sedentary workers need longer warming periods to lengthen sarcomeres and increase hyaluronic acid to overcome muscle and joint stiffness. Lack of weight-bearing exercises is a risk factor for developing osteoporosis. Sedentary behavior decreases the production of hormones (e.g., osteocalcin, insulin growth factors, and growth hormone) that promote healthy bone formation. Post-menopausal women are at increased risk for less bone formation due to loss of potent estrogens.
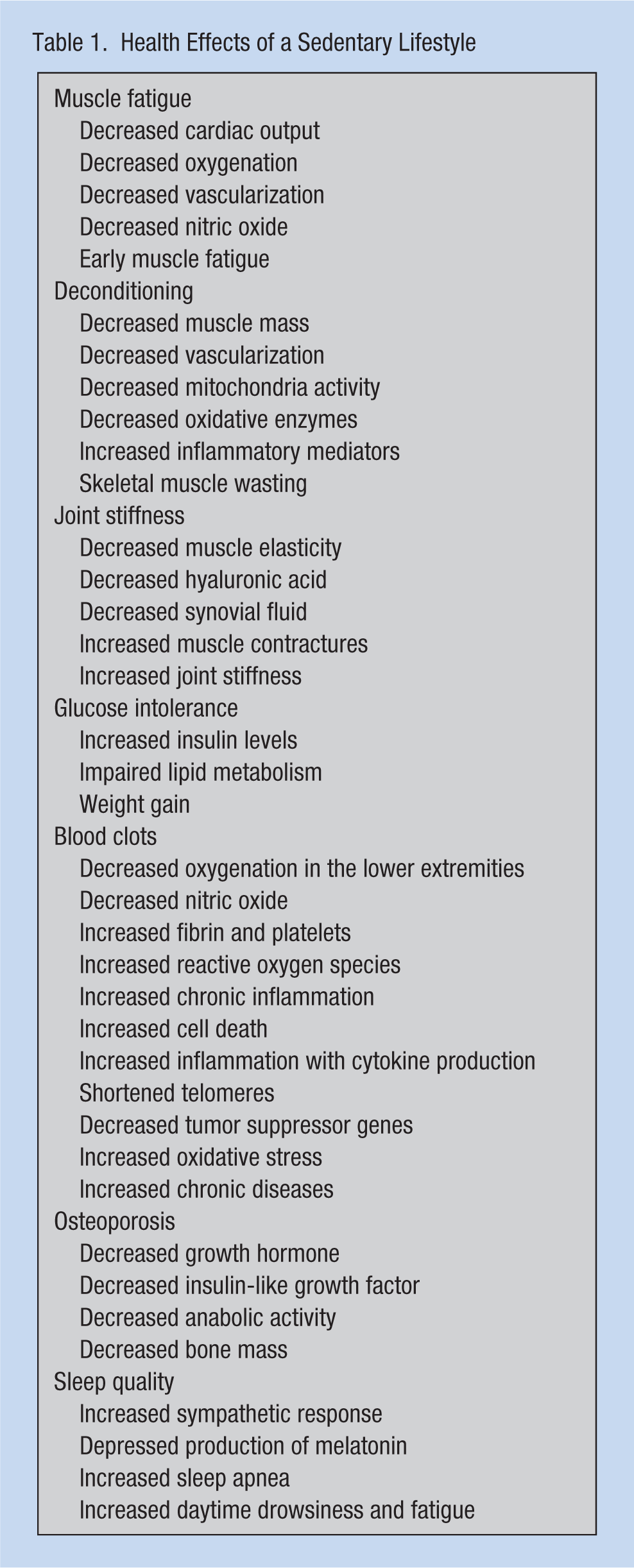
Osteoarthritis and joint inflammation may also be associated with sedentary lifestyles. Obesity is associated with osteoarthritis because of the heavy mechanical loads on the joints and cartilage. In addition, the production of adipokines, pro inflammatory and catabolic cytokines that destroy joints and cartilage, is also associated with sedentary lifestyles and obesity (Villalvilla et al., 2016). A sedentary lifestyle has many negative health effects, as summarized in Table 1.
Health Effects of a Sedentary Lifestyle
Chronic Diseases Associated With Prolonged Sitting and Sedentary Lifestyles
Prolonged sitting and sedentary lifestyles may lead to premature aging and contribute to chronic disease, prelude to lost productivity. Deconditioning may result in glucose intolerance, elevated insulin levels, and impaired lipid metabolism due to less regulation of certain enzymes (e.g., glucose transporter 4 protein [GLUT4] and lipoprotein lipase), which may contribute to the development of type 2 diabetes, weight gain, and cardiovascular disease (Bauman et al., 2013). The down regulation of GLUT4 decreases glucose uptake by the skeletal muscle (Forsig & Richter, 2009).
Post-menopausal women are at risk for insulin resistance and weight gain due to the lack of potential estrogens (Davis et al., 2012). Potential estrogens increase insulin sensitivity in younger women, and thus, glucose more readily enters the mitochondria and creates ATP for energy. As a result, younger women move from aerobic to anaerobic metabolism more effectively. In post-menopausal women, due to the lack of potential estrogens, glucose does not enter cells as easily to create ATP, and thus, these women experience less exercise capacity, weight gain, and increases in abdominal girth (Davis et al., 2012; Gupta et al., 2008).
Prolonged sitting may lead to blood clots due to oxygen deficiency in the lower extremities (Bates et al., 2012). Immobilization decreases nitric oxide levels and increases fibrinogen levels. Less nitric oxide decreases vasodilation; more fibrinogen creates more fibrin. Fibrin and platelets create blood clots. Hypoxemia results in reactive oxygen species that lead to chronic inflammation.
Sedentary lifestyles may promote cell aging, rapid cell death, and inflammation, which lead to chronic health problems such as diabetes and dementia. Leukocyte telomeres are found in most cells and hold genetic information that protects the cell from diseases such as cancer. Exercise lengthens the telomeres so that protective genetic information is not lost due to cell death. Sedentary behavior shortens telomeres, and valuable genetic material is lost. For example, tumor suppressor genes as well as oxidative stress can lead to early cell death (Edwards & Loprinzi, 2017).
Sedentary workers are at risk for osteoporosis. Growth hormone (GH) and insulin-like growth factors (IGF-1) are critical to bone formation due to their anabolic effects (Locatelli & Bianchi, 2014). Insulin-like growth factor can protect against estrogen-deficiency bone loss (Locatelli & Bianchi, 2014), growth hormone contributes to muscle development, and the combination of GH/IGF-1 contributes to the development of chondrocytes. Declining levels of GH/IGF-1 are marked by less muscle mass, more adiposity, less bone density, and less energy. It is believed that declining levels of GH/IGF-1 may contribute to insulin resistance as well (Puche & Castilla-Cortazar, 2012). Anabolic activity stimulates the production of these hormones, which decrease when sedentary.
Sedentary lifestyles may contribute to poor sleep quality leading to early fatigue (Ambrose & Golightly, 2015). Sedentary lifestyles are associated with weight gain, which may contribute to obstructive sleep apnea that promotes daytime drowsiness and fatigue (de Oliveira Diniz, Barreto, de Bruin, & de Bruin, 2016). Sedentary behaviors may depress production of melatonin, a neurotransmitter associated with sleep quality and wakefulness (McPherson et al., 2011). Fatigue and impaired sleep increases the sympathetic response, elevating resting heart rate and blood pressure, contributing to cardiovascular disease.
The Benefits of Exercise
Exercise may improve glucose uptake in cells by increasing levels of GLUT4, which deplete muscle glycogen stores (Forsig & Richter, 2009). Physical activity improves glucose transport and metabolism. Exercise prevents cell aging by reducing anti-inflammatory cytokines, naturally occurring cytokine inhibitors, and chemokines associated with diseases such as type 2 diabetes and cancer (Forsig & Richter, 2009; Pedersen, Steenberg, & Schjerling, 2001). Exercise also increases tumor necrosis factor-alpha that suppresses cancer and induces apoptosis of damaged cells (Ambrose & Golightly, 2015). Exercise may also increase skeletal muscle interleukin-6, which plays a role in muscle repair after anaerobic exercise and lipolysis (Meckel et al., 2009)
Exercise improves oxygenation in the lower extremities, increases nitric oxide levels, and reduces fibrinogen, which decreases the risk of blood clots (Bates et al., 2012). Exercise and proper hydration may prevent leukocytes and platelets from forming blood clots. Exercise also promotes fibrinolysis (i.e., fibrin clots are prevented from forming blood clots).
Exercise stimulates calcium absorption. Weight-bearing exercises stimulate bone formation by decreasing apoptosis and increasing osteoblast formation. Exercise, mainly weight-bearing exercises, stimulates signaling pathways that promote osteoblastic cell growth. Found in the bone marrow, one notable signaling pathway is interleukin-11, which promotes cortical thickness and strength in the long bones. Exercise produces insulin growth factor-1 (IGF-1) and transforming growth factor beta (TGF-β1), which enhance cartilage homeostasis (Villalvilla et al., 2016).
Exercise stimulates the production of osteocalcin, which promotes bone mineralization, calcium absorption by the bones, and calcium ion homeostasis. Exercise decreases parathyroid hormone, thus allowing calcium ions to supply osteoblasts with growth material, preventing osteoporosis and promoting proper bone growth (Barry et al., 2011). Parathyroid hormone is responsible for maintaining serum calcium levels; if serum calcium levels are low, the parathyroid may take calcium from the bones so workers must maintain healthy calcium intake.
Aerobic and anaerobic exercises enhance bone formation. Aerobic exercise stimulates mitochondrial biogenesis and the synthesis of proteins. Resistance exercise stimulates the formation of the myofibrillar proteins needed for muscle contraction. Exercise also stimulates the production of osteocalcin, a hormone responsible for the catabolism of glucose and fatty acids, the main source of nutrition for myofibers. Exercise stimulates the pancreas to release insulin and, in turn, to release adiponectin from adipose tissue, which increases cells’ sensitivity to insulin that may add to weight loss.
Staying active may improve osteoarthritis. Exercise may improve blood supply to the circulating joints and may also increase the production of synovial fluid in the joints, which may reduce friction. Weight-bearing exercises are necessary but no additional mechanical stress that may cause damage should be exerted on the bones (Moriyama, 2017).
Exercise has positive influences on cognitive abilities, increasing the level of brain-derived neurotrophic factor (BDNF) responsible for the growth and survival of neurons. Brain-derived neurotrophic factor increases synapses to improve memory and learning in the hippocampus, part of the hypothalamus (Gomez-Pinilla & Hillman, 2013). It is BDNF that increases the volume of the hippocampus, preventing atrophy. Another positive effect of exercise is that it increases the levels of IGF-1 and vascular endothelial growth factor (VEGF; Gomez-Pinilla & Hillman, 2013). Insulin growth factor-1 stimulates neuron cell growth and inhibits apoptosis. In addition, VEGF promotes angiogenesis in the central and peripheral nervous systems.
Sleep quality improves with exercise. Workers, who are physically fit, usually have a low resting heart rate. This vagal response is a reflection of the efficiency of the parasympathetic system, depressing the sympathetic system and decreasing catecholamines that may interfere with sleep quality (Uchida et al., 2012).
Implications for Occupational Health Nurses
Occupational health nurses understand that sedentary employees are at risk for musculoskeletal injuries as are employees who are active. Workers who are considered deconditioned usually have poor cardiovascular fitness but may not show any objective signs of cardiac or pulmonary disease. Occupational health nurses may observe this phenomenon during pre-placement or annual physicals that require employees to perform various physical activities. The inability to perform expected tasks or tasks employees were previously able to perform warrants further investigation by the occupational health nurse (Quittan, 2016).
Sedentary employees should be encouraged to exercise every day. Education should include the importance of an initial warming period to allow blood flow to the muscles prior to any physical activity. Exercise routines may include aerobic and anaerobic activity with flexibility training. Walking and yoga are examples of aerobic and anaerobic exercise. Education about the health effects of sitting (e.g., blood clots, osteoarthritis, osteoporosis, and diabetes) should be offered. Workers may be instructed to change positions and use a variety of muscle groups. Standing and walking also increase muscle pressure that encourages blood vessels to contract, reducing swelling and discomfort.
It may be necessary to assess for genetic disorders (e.g., deficiencies of protein C, protein S, antithrombin, or factor V Leiden, and non-O blood type) that could affect blood coagulation (Bates et al., 2012). The occupational health nurse may also assess for histories of smoking or estrogen therapy. Pregnant workers or workers that recently had surgery must be cleared by their health care providers prior to returning to work. At-risk workers, especially those who may have knee replacements, should be monitored frequently (Bates et al., 2012). These workers should be advised to apply Ted hose prior to standing to reduce swelling, if not contraindicated, by their primary care provider (Bates et al., 2012). If swelling occurs, Ted hose may be difficult to apply.
Occupational health nurses should document if workers are taking calcium and vitamin D supplements; education should include the need for weight-bearing exercises to achieve the full benefit of bone growth. Sunlight exposure improves Vitamin D levels as well as bone health (Holick, 2004). Sunlight exposure may also improve sleep (Hartescu, Morgan, & Stevinson, 2015).
An ergonomic consult may be needed to erect a sit–stand station (Mayo Clinic, 2017). Supplying employees with pedometers or electronic monitors to increase activity has been met with mixed results (Brakenridge, 2016). One obstacle to routine exercise is employees fear lost productivity when leaving their work stations for exercise breaks (Hamilton, Healy, Dunstan, Zderic, & Owen, 2008). However, exercise may actually increase productivity because exercise is known to improve cognitive performance and decrease mental stress (Hamilton et al., 2008). Exercise also improves subjective perceptions of energy (Hamilton et al., 2008). An educational program that includes employees and employers promoting physical activity at work actually adds to productivity (Hamilton et al., 2008). One recommendation for sedentary workers who sit for 7 hours or more a day is to interrupt their work with light activity such as walking or simple resistance activities for 3 minutes every 30 minutes (Asvold, Midthjell, Krokstad, Rangul, & Bauman, 2017). Employees should be reminded that vigorous activity prior to the workday is beneficial, but it is important to stay active all day (Hamilton et al., 2008). Occupational health nurses should encourage management to support workplace activity. One intervention that may be considered is an activity tracker that monitors and measures daily activity (Brakenridge et al., 2016). It is recommended that the average adult exercise at least 150 minutes a week in moderate-to-vigorous physical activity (e.g., a 30-minute workout, 5 days a week; World Health Organization, 2010). Prolonged sitting may reverse the benefits of vigorous exercise (Hamilton et al., 2008). Physically active employees may have positive economic effects on productivity by reducing absenteeism and health care seeking (Ambrose & Golightly, 2015).
Conclusion
MN was encouraged to exercise, walk, and stretch every day at work and at home. Employees were provided with an education program that focused on the risks of prolonged sitting and deconditioning. Due to her deconditioning, MN was referred to physical therapy for strengthening and stretching exercises. She was instructed to keep a diary of her daily activities that she could share with the occupational health nurse to monitor her progress. MN was prescribed heat therapy in addition to physical therapy. She was prescribed Coumandin for blood clots, and therefore, aspirin and nonsteroidals should not be prescribed due to the increased risk of bleeding. MN was given a prescription for topical lidocaine and a topical nonsteroidal.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Ann R. Lurati is a nursing lecturer at California State University Monterey Bay.