
Abstract
Colorectal cancer (CRC) is the second leading cause of cancer-related deaths among men and women in the United States. To increase statewide CRC screening rates, the Alabama Department of Public Health (through a Centers for Disease Control and Prevention [CDC] Colorectal Cancer Control Program grant) partnered with The University of Alabama in Huntsville (UAH) and The University of South Alabama (USA) to provide free CRC screening opportunities to eligible University employees and dependents. Resources were invested at both universities to ensure participant education, tracking, and monitoring. In total, 86 fecal immunochemical tests (FITs) were distributed at the UAH campus and 62 were returned for testing; 146 FITs were distributed on the USA campus with 111 returned. Fecal immunochemical test return rates were over 70% at each site. Most notably, 21 positive FITs were identified among UAH participants and 25 at USA. Findings from both efforts suggest that employer-based screening initiatives are a systematic and replicable means of improving CRC screening.
Colorectal cancer (CRC) is the second leading cause of cancer mortality in the United States and is the third most common cancer in men and women (Centers for Disease Control and Prevention [CDC], 2016). According to the National Cancer Institute, in 2013, an estimated 1,177,556 Americans were living with colon and rectal cancer, with an estimated 134,490 new cases in 2016 (National Cancer Institute, 2016). Currently, the lifetime risk for an individual to develop CRC is 4.4%. Colorectal cancer is most frequently diagnosed among adults aged 65 to 74 years with the median age at death from CRC at 68 years (National Cancer Institute, 2016).
The CRC stage at diagnosis influences prognosis (Stegeman et al., 2012). Earlier detection of CRC and removal of its precursors (e.g., precancerous polyps) results in lower morbidity and mortality (Inadomi, 2017). The term polyp refers to a discrete mass that protrudes into the intestinal lumen (World Gastroenterology Organization, 2007). Based on colonoscopy data, the prevalence of adenomatous polyps is in the range of 20% to 53% of the U.S. population older than 50 years of age (Strum, 2016).
The detection of CRC in asymptomatic patients at a curable stage underscores the importance of screening (Flitcroft, Irwig, Carter, Salkeld, & Gillespie, 2012; Inadomi, 2017; Quintero et al., 2012; Stegeman et al., 2012). According to the CDC, cancer-screening tests are effective when they detect disease early, leading to more effective treatment. Screening asymptomatic adults aged 50 to 75 years has substantial benefit because survival improves when CRC is detected early (U.S. Preventive Services Task Force [USPSTF], 2016).
Colorectal Cancer Screening in the Workplace
The Alabama Department of Public Health (ADPH) was one of 23 state health departments awarded a grant from the CDC for CRC prevention and detection. The goals of this grant were to increase screening rates among men and women aged 50 to 75 years, to promote USPSTF screening guidelines and quality assurance for CRC screening, to promote screening through worksite wellness programs, to reduce barriers to screening access, and to educate patients about USPSTF recommended screening options for CRC (ADPH, 2016).
Conducting health screenings at the workplace is a promising population health strategy for the early detection and prevention of diseases. Workplaces are ideal for health screenings because large numbers of employees can be reached which is especially important for those who do not see their health care providers on a regular basis (Walsh, Potter, Arora, Gildegorin, & Terdiman, 2014).
Recognizing that workplaces are optimal for health screenings, the ADPH supported screening university employees for CRC at the University of Alabama in Huntsville (UAH) and the University of South Alabama (USA). Worksite screening increases adherence to annual testing and brings screening to the individual in a convenient and timely manner. Eighty percent of Alabamians aged 50 to 75 years who are not current on CRC screening have some form of health care coverage (ADPH, 2014). Employees at UAH and USA have insurance coverage for screening and diagnostic colonoscopies and resulting treatment. Most of the large employers in Alabama cover not only their employees but also spouses and retirees (ADPH, 2014). Despite the effectiveness of CRC screening, more than 40% of CRC diagnoses in Alabama are made in Stage 3 or 4 and only 66% of current Alabamians 50 years of age and older have been appropriately screened (ADPH, 2016).
Screening Tests
Several methods are available for CRC population screening (Stegeman et al., 2012). Colorectal cancer screening in the average-risk population is both diagnostic and cost-effective (Heitman, Hilsden, Au, Dowden, & Manns, 2010; Hewitson, Glasziou, Watson, Towler, & Irwig, 2008; Levin et al., 2008; Mandel et al., 2000). Recommended strategies for CRC screening are divided into two broad categories: stool tests and structural (visualization) examinations (i.e., flexible sigmoidoscopies, colonoscopies, and computed tomographic [CT] colonography; Quintero et al., 2012; Stegeman et al., 2012).
Stool tests
Colorectal cancers may cause the shedding of blood and other tissue components that can be detected in the stool long before the development of clinical symptoms. This fact has prompted the search for fecal analyses that support early detection of cancer in asymptomatic individuals (Inadomi, 2017). The most common method has been the detection of occult blood in stool. Several randomized studies demonstrated the reduction of mortality from CRC by 15% to 33% in cohorts and 45% in compliant participants (Heitman et al., 2010; Hewitson et al., 2008; Levin et al., 2008; Mandel et al., 2000).
The guaiac smear test is one of the most common tests used for the detection of occult blood in feces. The guaiac test reacts to the peroxidases of heme. However, the test can also react to the presence of other peroxidases in the stool (e.g., certain fruits, vegetables, and red meat). Therefore, dietary restrictions are necessary to avoid any false positives (World Gastroenterology Organization, 2007). The sensitivity of the fecal occult blood test (FOBT) is only 50% to 60% for one-time use but may be as high as 90% when used every 1 to 2 years. Low-sensitivity resulting in false negatives can lead to false reassurance. In addition, FOBT effectiveness depends on compliance with testing over many years (World Gastroenterology Organization, 2007).
The guaiac smear tests are being replaced by the fecal immunochemical tests (FITs) which identify intact human hemoglobin in stool using sensitive and specific techniques. The FIT has better sensitivity when compared with guaiac stool tests for detecting CRC (Lin et al., 2016) and requires only one test (small stool sample) rather than three tests recommended for guaiac stool tests. The FIT also has better compliance because no prior planning (e.g., dietary or drug restrictions such as aspirin) is required (Lin et al., 2016).
An emerging screening strategy for fecal testing is the multitargeted stool DNA test (FIT-DNA test). The specificity of the FIT-DNA test is less than the FIT alone; the FIT-DNA could have 3 times as many false positives that would require colonoscopies if only the DNA test was used for screening. The FIT-DNA test requires a whole stool specimen and costs US$400 to US$800 (FIT alone costs US$3 to US$40). The multitarget stool DNA combines a FIT test with a test for altered DNA biomarkers in cells shed in the stool (Imperiale et al., 2014).
Structural (direct visualization) tests
Structural tests include flexible sigmoidoscopies, colonoscopies, double-contrast barium enemas, and computerized tomography (CT) colonography, which provide direct visualization of the colon. Flexible sigmoidoscopies allow direct examination of the inner surface of the large bowel up to 24 inches from the anal margin (Flitcroft et al., 2012). Advantages of a flexible sigmoidoscopy include less time consuming than a colonoscopy, bowel preparation is easier and faster, morbidity is scant unless polypectomy is needed, and in some cases no sedation is needed. The major disadvantage is that right-sided lesions are missed because only the left colon is visualized (Lin et al., 2016).
Colonoscopy is the gold standard for CRC screening. A positive result on any screening test (FOBT, FIT, sigmoidoscopy, CT, barium enema) requires a colonoscopy. Colonoscopy allows the examination of the entire colon with detection and removal of polyps and biopsy for cancer. Specificity and sensitivity in detecting polyps and cancer are about 95% (Lin et al., 2016). Population-based studies have demonstrated that colonoscopy markedly reduces the incidence of CRC by eliminating precancerous polyps (Brenner, Chang-Claude, Seiler, Rickert, & Hoffmeister, 2011).
Double-contrast barium enema allows evaluation of the entire colon, but its sensitivity (48%) and specificity are inferior to colonoscopy, and any abnormalities found during the enema require a colonoscopy. Computerized tomography colonography offers sensitivity and specificity of 93% and 97%, respectively, for polyps greater than 10 mm, and when polyps are smaller than 10 mm, the sensitivity and specificity drop to 86% and even lesser for smaller polyps. Flat lesions are more likely to be missed with CT. Other disadvantages include ionizing radiation exposures and visualization of polyps requires a subsequent colonoscopy (World Gastroenterology Organization, 2007).
Screening at Worksites
Increasing CRC screening rates has become a national priority supported by several leading authorities including the CDC, the National Colorectal Cancer Roundtable, the ADPH, and the American Cancer Society. A 2014 initiative focused on improving national colorectal screening rates to achieve an 80% screening rate by 2018. In 2013, the CRC screening rate among Alabamians aged 50 years and older was approximately 68% (National Cancer Institute, 2017). To improve health outcomes for Alabama residents and increase statewide CRC screening rates, the ADPH, through a grant funded by the CDC Colorectal Cancer Control Program, partnered with several large employers to offer screenings for their employees. Two of those large employers were UAH located in northern Alabama and USA (ADPH, 2016).
Program Implementation at the UAH
The University of Alabama at Huntsville is considered a “very high research” university by the Carnegie Foundation mainly because of its engineering and science programs (U.S. News & World Report, 2016). The Grant (US$16,561) from the ADPH and the CDC was awarded to UAH and funded all activities pertaining to CRC screenings. Institutional Review Board (IRB) approval was not required because the project was not considered research as defined by the Department of Health and Human Services (UAH IRB, written communication, February 16, 2015). The work related to the screening was completed at the Faculty and Staff Clinic, the on-site employee health clinic located at the UAH campus.
Prior to the screening, the staff at the Faculty and Staff Clinic launched a health communication event to raise awareness of CRC and the value of early detection and prevention. The staff at the clinic and the ADPH designed a poster (Figure 2) to attract attention and reflect the “rocket city” nomenclature given to Huntsville because of its relationship with the National Aeronautics and Space Administration (NASA) and the Marshall Space Center; the poster was distributed throughout campus about a week prior to the event. To aid the CRC screening campaign, an undergraduate student was hired on the grant to accompany the nurse practitioner to various university departments and faculty and staff senate meetings and be in the clinic to answer any questions and field phone calls regarding the screening. In addition, under the direction of the nurse practitioners, the student worker assisted in participant education and FIT tracking.
Those individuals who had positive FIT were called on the phone to discuss the result with the nurse practitioner and an additional visit to the clinic was offered. The clinic also made referrals to a gastroenterologist for those employees who did not have a previous relationship with a gastroenterologist. Those individuals with negative FIT tests were contacted via a mailed letter and offered a call/or a visit to the clinic if they had any questions. The clinic provided ongoing support through additional phone calls and visits. Employees who participated in the CRC screening program verbalized that having the clinic on-site where they could pick up the FIT and then drop it off for testing was very convenient and in some cases was the trigger for screening (FITWAY Participant, personal communication, March 16, 2016).
The CRC screening program was implemented at UAH from March (National Colorectal Cancer Awareness Month) to April 2015. University employees, dependents, and retirees aged 50 years of age and older were eligible to receive a free take-home FIT as a screening modality. The FIT was chosen as a screening test because it was considered “patient-friendly” and more likely to enhance compliance. The FIT can be used at employees’ and retirees’ homes with no changes in diet or medications, no recommendations for special liquids, and no requirements for time off from work. The test was returned to the UAH Faculty and Staff Clinic to be analyzed. A drawing for a US$500 gift card was offered as an incentive.
In addition to the age requirement, eligible participants were required to have no personal or family history of CRC or precancerous polyps, no history of inflammatory bowel disease (e.g., ulcerative colitis or Crohn’s disease), and no history of genetic syndromes such as familial adenomatous polyposis (FAP) or Lynch syndrome. The recommended screening for individuals with the above conditions is a colonoscopy. Participants were advised that if the FIT was positive, a diagnostic colonoscopy was needed; workers were referred to a gastroenterologist of their choice for colonoscopies. At UAH, 86 FITs were distributed and 62 were returned for a return rate of 72.1%. Of the 62 returned FITs, 21 were positive. Eleven of the 21 positive FITs had normal colonoscopies, seven had polyps identified with two graded as precancerous, three had diverticulosis.
Program Implementation at USA
All USA employees (and their dependents), aged 50 years and older, were eligible to participate in the CRC screening initiative at USA. Members of the Cancer Control and Prevention (CCP) team at USA Mitchell Cancer Institute (MCI) effectively initiated the employee wellness program (EWP) in March of 2015. All USA employees and their dependents, aged 50 years and older, were mailed an informative postcard on CRC and screening modalities, encouraging them to schedule some form of screening if they were not current. The postcard presented some basic facts on CRC in Alabama, listed the physical locations with dates and times where they could pick up a take-home FIT, and provided the number to the USA Digestive Health Center if they would prefer to schedule an appointment for a colonoscopy.
During a 6-week period (from March 1 to April 10, 2015), free take-home FITs were made available to all eligible USA employees and their dependents. Due to the geographic magnitude of campus-affiliated academic and medical centers, take-home FIT tests were available for pick up Monday to Friday, during normal clinic hours, at the USA Urgent Care Center (Main Campus) and USA Family Medicine Clinic (Springhill Campus). Nine additional distribution efforts were made at various campus locations (i.e., USA Medical Center, Children’s & Women’s Hospital, USA Center for Healthy Communities, Campus Recreational Center, USA Bookstore, and Academic Health Sciences Building) for employee convenience as well as providing extra educational impact opportunities. Tables were set up in high-traffic flow environments (e.g., outside the cafeteria and main entries) and included various CRC brochures, information packets, and small give away items (e.g., T-shirts, hats, and pens). At both universities (UAH and USA), prior to receiving a take-home FIT, participants were asked to complete a three-page packet that contained the following: (a) an informed consent to participate in the initiative, (b) basic demographic and contact information, (c) health history as it pertained to eligibility (e.g., past screenings and current symptoms), and (d) current primary care physician (if applicable). Once complete, the participants received folders containing additional education and contact information, as well as a preaddressed, prestamped take-home FIT test.
Each participant was called approximately 7 to 10 business days after receiving their take-home FIT, reminding them to return their kit in the mail. All returned FITs were tested and interpreted at the USA Family Medicine Clinic. Participants choosing to schedule colonoscopies were contacted by the USA Digestive Health Center for an appointment.
Negative FIT results were communicated via a mailed letter that thanked the participant for completing the screening, provided the date and location in which the screen was analyzed and MCI contact information. The letter also emphasized that the take-home FIT was an annual test and should be completed again in 2016 to be compliant with recommended screening guidelines. Positive FIT results were initially contacted via phone call and subsequently referred to the USA Digestive Health Center (or physician of their choice) for a diagnostic colonoscopy. In the event that phone contact was unsuccessful for these participants, letters were mailed that informed them of their test results and recommended that appropriate diagnostics ensued.
Participants were incentivized to return their FITs or schedule screening through colonoscopy by entering them into a US$500 gift card drawing. The USA employees and their dependents, compliant with current colorectal screening guidelines, were also encouraged to enter the drawing with proof of screening from their primary care physician.
The EWP was supported by the USA Employee Wellness Initiatives Committee and approved by the USA IRB. Approximately 146 FIT tests were distributed to USA employees and dependents, aged 50 years and older, during the 6-week project period. In addition, approximately 25 colonoscopies were scheduled with the USA Digestive Health Center during the same time frame. Of the 146 total kits distributed, 111 were returned to the USA Family Medicine Clinic for analysis, a return rate of approximately 76%. Of those participants who returned FIT tests (N = 111), 86 negative and 25 positive results were recorded (Figure 1).
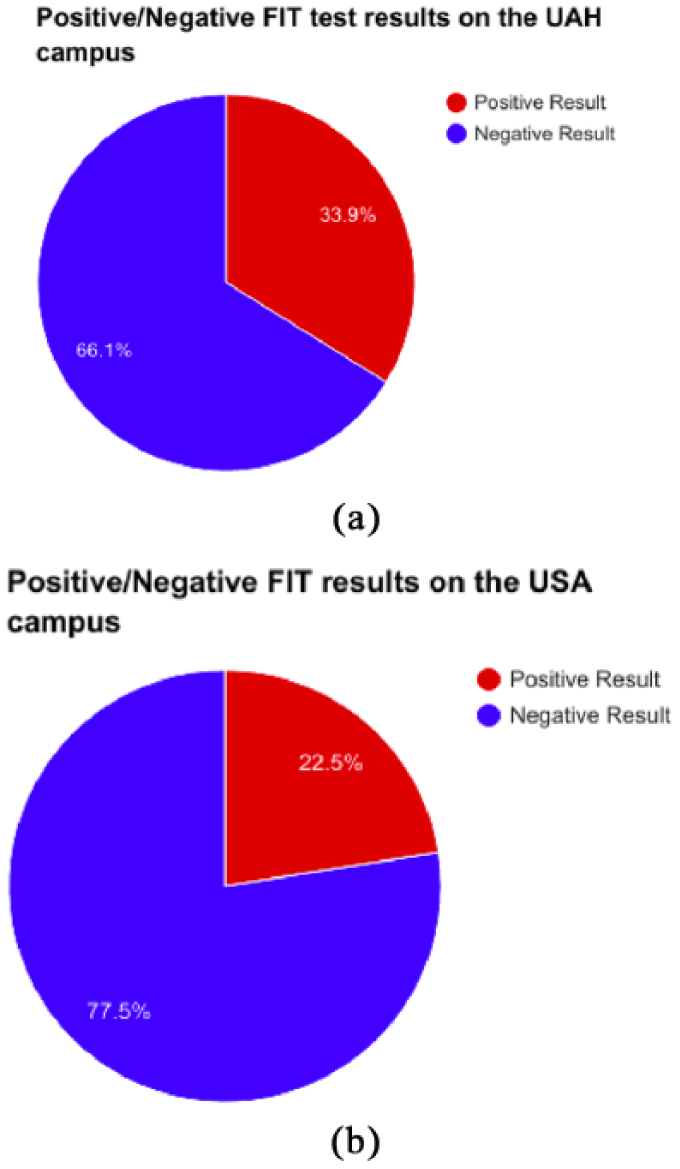
Positive/negative FIT test results on the (a) UAH campus and (b) USA campus.
Following the completion of the EWP (FIT only), 113 USA employees and dependents were current with recommended CRC screening guidelines. These results show a 34.4% increase in CRC screening among participants.
The EWP successfully distributed 146 take-home FITs, scheduled approximately 25 screening colonoscopies and educated hundreds of USA employees and dependents, aged 50 years and older, about the benefits of CRC screening. Although the screening initiative had the potential to impact a much larger employee population, the results of the current project have the potential to shape more effective interventions and worksite screening programs in the future. With the support of the USA Employee Wellness Initiatives Committee, the CCP team at MCI continued to offer the workplace cancer screening initiative in 2016 and has an initiative planned for March 2017. The total grant award was US$88,394, and this amount included the USA worksite intervention as well as other employer worksite interventions and a practice-based intervention at all USA primary care sites using automated telephone reminders to prompt workers to schedule CRC screenings, if not current.
Discussion
University-based CRC screening initiatives represent a systematic approach to generating awareness about screening. By providing free take-home FIT screening tests, the overall health and well-being of University employees, dependents and retirees improved. At the time of the screening (March to April 2015), UAH had a total of 1,291 full-time (FT) employees. Of this number, 504 employees were eligible to participate by virtue of age. The authors do not know the number of employees and retirees who were excluded due to conditions such as a personal and family history of CRC or other exclusion criteria. The majority of employees at UAH are White (78%) with African Americans comprising 13%, Asian Americans 7%, and Hispanics and Native Americans 1% each (UAH Human Resources Department, personal communication, March 10, 2015). According to the cancer screening literature, interventions that increase screening prevalence include mailed letters, e-mail notifications, availability of free test kits, and postscreening phone calls and letters (Coronado et al., 2014; Gupta et al., 2013; Marx, Tse, Golden, & Johnson, 2015). The UAH Faculty and Staff Clinic reached out to employees via presentations, posters, campus e-mails, and letters (Figure 2).
Program poster.
The USA is one of the largest employers in the Mobile area with approximately 6,000 employees; 2,361 FT employees were 50 years of age and older. The majority of USA employees are White (61.4%), with 23.4% Black or African Americans, 3.4% Asian, 2.7% Hispanic/Latino, and 1% American Indian and Native Hawaiian (Forbes America’s Top Colleges, 2016). The baseline colorectal screening rate from provider claims data was nearly 60% (59.6); the authors determined that the proposed EWP had the potential to increase colorectal screening to 40% of the USA workforce, aged 50 years and older, or approximately 955 individuals.
Although EWPs vary by institution in both depth and content, their popularity among employer groups is steadily increasing. The workplace is an ideal location to conveniently provide routine preventive health services, foster healthy lifestyle choices among employees, and reduce long-term health care–related expenditures. An additional benefit to EWPs is the ability to implement routine preventive services to employees on an annual and scheduled basis. The colorectal screening initiative was implemented in March, which is also National Colorectal Cancer Awareness Month. Employee wellness programs can create lasting associations between monthly public health awareness initiatives and needed preventive services, which can motivate employees to create and sustain healthier lifestyles both in and out of the workplace.
The relationship among the universities (UAH and USA) and the ADPH was collegial. The ADPH worked with the universities to design the posters and forms used during the screening. The strengths of the colorectal screening program at UAH and USA included employer-initiated screening, screening was brought to the employees, and existing clinics educated employees about CRC. High FIT return rates indicated strong participant compliance when provided a convenient screening modality (Figure 3). The identification of precancerous polyps supported the screening initiatives’ impact on reducing the burden of CRC in this population.
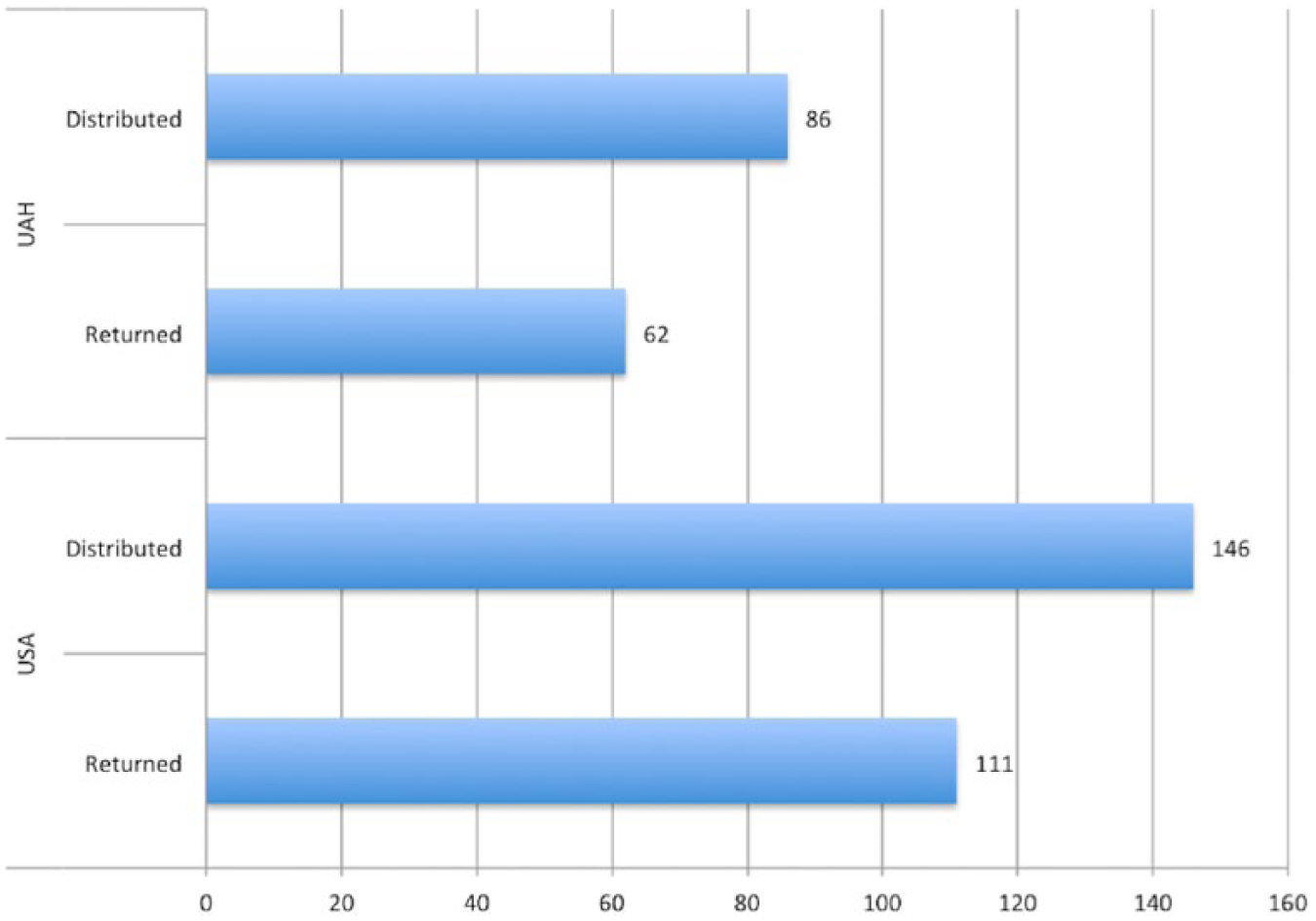
Distribution and return of FITs by campus location.
Conclusion
Workers represent a convenient population to screen, and more importantly detect, CRC at an early stage. Findings from both efforts suggest that employer-based screening initiatives represent a systematic, replicable, and opportune means of improving CRC screening rates and saving lives. Key stakeholders from both campuses have expressed interest in making CRC screening an annual wellness service provided and sustained through University funding. These ongoing efforts will contribute to the overarching goals of reducing the prevalence and late-stage diagnoses of CRC in Alabama.
As recognized leaders in workplace health and safety, occupational health nurses are cognizant that employed groups represent a convenient population to screen, and more importantly detect, CRC at an early stage. Occupational health nurses are uniquely educated for their role in the early detection of illness and promotion of healthy behaviors. Given that CRC is the second leading cause of cancer mortality in the United States and is the third most common cancer in men and women, occupational health nurses can increase awareness about the prevalence and impact of CRC in Alabama and follow recommended guidelines for screening (CDC, 2016).
Footnotes
Acknowledgements
The authors acknowledge the FITWAY Colorectal Cancer Screening Program, the Alabama Department of Health, and the Centers for Disease Control and Prevention.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This screening program was funded by the Alabama Department of Public Health, Family Health Services through a cooperative agreement with the Centers for Disease Control and Prevention (CDC; Grant numbers: 2U58DP002055-06, CFDA#93.283, DP09-903, and DP14-1414), and the FITWAY Alabama Colorectal Cancer Prevention Program.
Author Biographies
Louise C. O’Keefe is assistant professor, College of Nursing and director of the Faculty and Staff Clinic at The University of Alabama in Huntsville. She established the Faculty and Staff Clinic in 2007 and teaches in the Family Nurse Practitioner Program at the College of Nursing.
Margaret M Sullivan has worked in health care for over 30 years in the areas of strategic planning, health policy, oncology service line development, and cancer control and population health. She earned her undergraduate degree in human biology from Stanford University and her master of science in health policy and management from the Harvard T. Chan School of Public Health. She serves as associate director of Cancer Control and Prevention for the University of South Alabama Mitchell Cancer Institute and vice president for Development and Alumni Relations for the University.
Amber N. McPhail is a family nurse practitioner working at The University of Alabama in Huntsville Faculty and Staff Clinic. She previously practiced in a Women’s Health clinic for 8 years before coming “back” to The University of Alabama in Huntsville (UAH). She earned her bachelor of science in nursing and her master of science in nursing from UAH.
Kristen Van Buren has worked in the field of public health since 2011, with particular interests in cancer, occupational, and social epidemiology. She earned her undergraduate degree in biology from the University of the South and her master of public health degree from East Tennessee State University. She is currently a doctoral candidate in epidemiology at the University of Kentucky’s College of Public Health.
Nathan Dewberry is a graduate of The University of Alabama in Huntsville with a bachelor of science in biology. He is currently seeking to continue his education in the field of biomedical engineering.