
Abstract
Violence toward nursing staff occurs frequently, particularly in intensive care units and closed or intensive psychiatric facilities, which have been studied previously. However, violence toward community nurses has not been investigated. The purpose of this study was to explore the frequency of violence toward community nurses in Slovenia. More than 56% of study respondents were verbally abused by their patients during the past year. More than 42% of all cases of horizontal violence were directed at community nurses.
Health care professionals encounter many occupational risks when providing services to individuals and communities (Ozturk & Babacan, 2014). Occupational injuries in health care occur frequently; the frequency may be even higher than reported because up to 70% of incidents toward nursing staff are unreported (M. Gates, Gillespie, & Succop, 2011; Stokowski, 2010). Nurses have reported indirect threats (48%), direct threats (40%), and violent acts (40%), and 45% of nurses have witnessed violence and threats toward other staff members (Josefsson & Ryhammar, 2010).
In Jordan, more than three quarters of study participants (75.8%) were exposed to at least one form of violence (Albashtawy, 2013). The incidents of verbal violence were approximately 5 times more frequent than incidents of physical violence. Findings from a Swiss study showed that in the previous 12 months, 72% of nurses had experienced verbal violence, whereas 42% of nurses had experienced physical violence perpetrated by patients and visitors (Hahn et al., 2010). Furthermore, 23% of nurses suffered physical injuries and 1.4% of nurses took leaves of absence for one or several days. Nurses reported significant distress due to violent patient or visitor behavior. A study of Emergency Department (ED) workers in the United States found that approximately 25% of respondents had experienced physical violence more than 20 times in the past 3 years, and almost 20% reported experiencing verbal abuse more than 200 times during the same period (Gacki-Smith et al., 2009). Respondents who experienced frequent physical and/or verbal abuse were afraid of retaliation and reported little support from hospital administration and ED management, barriers to reporting workplace violence. A study conducted in Hong Kong showed that nurses had experienced verbal abuse (73%), bullying (45%), physical abuse (18%), and sexual harassment (12%; Kwok et al., 2006). To cope with verbal abuse, most (82%) nurses confided in friends, family members, or colleagues about the abuse.
Physical aggression occurs more frequently in nursing homes (83.9% of employees) than other health care workplaces; verbal abuse is more common in psychiatric hospitals (96.7% of employees; Franz, Zeh, Schablon, Kuhnert, & Nienhaus, 2010). In the United States, the highest incidence of workplace assault is perpetrated against nursing assistants employed in long-term care settings (D. Gates, Fitzwater, & Succop, 2005). Aggressive behavior poses not only a challenge but also a burden for caregivers working in nursing homes. In the study conducted by Zeller and colleagues (2009), 40% of the staff were exposed to workplace violence during the previous year and 18% reported experiencing workplace violence on a daily basis. A significantly higher number of employees working in nursing homes reported violent behavior compared with employees working in other settings (Zeller et al., 2009). In total, 35% to 80% of all health care employees reported experiencing at least one physical assault at their workplaces, nursing staff being the most vulnerable (Clements, De Ranieri, Clark, Manno, & Kuhn, 2005).
Clements et al. (2005) reported health care workers, particularly nursing staff, were most frequently the recipients of psychiatric patients’ violent behavior. However, other employees working with psychiatric patients also experienced workplace violence: police officers, security officers, paramedics, and nursing home staff.
In 2013, an extensive study examined the prevalence of violence toward employees in psychiatric hospitals, psychiatric homes, nursing homes, special education classrooms, and work and care centers (SEWCC) in Slovenia (Gabrovec, Eržen, & Lobnikar, 2014). More than 92% of respondents reported experiencing verbal aggression by patients in the previous year; more than 84% of respondents had been physically abused during that same period and more than 63% of respondents had suffered injuries inflicted by patients. Almost 41% of staff had been verbally abused by patients’ family members. This study established the high prevalence of workplace violence in the Slovenian health care industry (Gabrovec et al., 2014). However, given the extensive literature on violence toward health care workers, little research has been published on violence toward community nurses.
Since 1992, Slovenia has had a Bismarckian-type social insurance system with a single payer for statutory health insurance, fully regulated by national legislation and administered by the Health Insurance Institute of Slovenia (HIIS). In Slovenia, health insurance is universal, based on employment status or legally defined dependent status (i.e., minors, unemployed spouses, registered unemployed citizens, and individuals without income). Community nurses are independent, postsecondary, or higher education graduates assigned to health care centers under municipality governance (Dzananovic, 2010). Community nurses provide health promotion, prevention, treatment, and palliative care to adolescents, healthy older adults, the chronically ill and disabled, and pregnant women and their infants (Albreht et al., 2009). Community nurses are primary care providers who promote the active participation of individuals, families, and communities in solving and managing health-related problems (St. John & Keleher, 2006).
The purpose of this study was to establish the prevalence of violence toward community nurses in Slovenia. In addition, this study aimed to establish correlations between individual nurse’s emotional states that result from aggressive behavior, security for community nurses, and education related to security. Furthermore, this study focused on the relationship between employees’ experiences with patients’ verbal violence and subsequent fear of future inappropriate or aggressive patient behavior as well as the relationship between feeling safe at work and knowing how to manage patients’ aggressive behavior.
Method
The authors used a nonexperimental research method for this study. The study instrument was a structured questionnaire developed after reviewing previous studies, situations faced by employees during and after an aggressive outburst, and the quality and safety of patient treatment in psychiatric facilities, rescue services, and retirement homes (Clements et al., 2005; Gabrovec & Eržen, 2016; Gabrovec et al., 2014; M. Gates et al., 2011; Hahn et al., 2010).
The questionnaire consisted of 49 questions divided into five sections: work and violence at the workplace (21 questions), organization of work (nine questions), influence of various factors on employee safety and patient treatment (nine questions), education (six questions), and demographic characteristics (four questions). Risk management was the dependent variable; the independent variables included availability of supplies, a clear understanding of risks involved, awareness of work-related errors, attention to measures for increased safety, attention to the importance of safety within the institution, handling violent outbursts, supervision, personnel motivation and incentives, sufficient number of employees, protocols in case of violent outbursts, reporting about violent events, team work and support, and measures for improvement. A descriptive Likert-type scale was used (i.e., strongly disagree, disagree, partly agree, agree, strongly agree). The instrument was shown to have moderate to very good internal consistency as measured by Cronbach’s alpha (Cencič, 2009; Mohsen & Reg, 2011). The external validity of the questionnaire was evaluated prior to data acquisition by a focus group of master of science in nursing (MSN) students.
The survey was conducted in April and May 2015. The web survey was sent to all Slovenian community nurses (816) electronically because these nurses use computers for their daily work activities. Participation was voluntary and participants’ anonymity was ensured. The administration ethics committee of participating institutions gave their consent for nurses to participate in the study (No.: ZDCe: 028/2015 and 079/2015). The data were analyzed using IBM SPSS Version 21.0 and IBM AMOS Version 21; descriptive statistics, Pearson’s r, the Kolmogorov–Smirnov test, Mann–Whitney U test, and linear regression with a p < .05 level of significance were calculated.
Results
The questionnaire was returned by 337 of the total sample of 816 community nurses. Of the 337 questionnaires submitted, 285 questionnaires were complete. Of the 285 respondents, five (1.8%) were men and 280 (98.2%) were women. Respondents’ ages were categorized as 21 to 30 years (3.5%), 31 to 40 years (31.6%), 41 to 50 years (24.6%), 51 to 60 years (36.8%), and 61 years and older (3.5%). Fifteen (5.3%) respondents were Assistive Support Workers (i.e., 2-year high school nursing program), 75 (26.3%) were Registered Nurse Assistant (i.e., 4-year high school nursing program), 175 (61.4%) were Registered Nurses (i.e., 3-year undergraduate nursing program) and 20 (7%) were Advanced Practice Nurses (i.e., 2-year master’s nursing program).
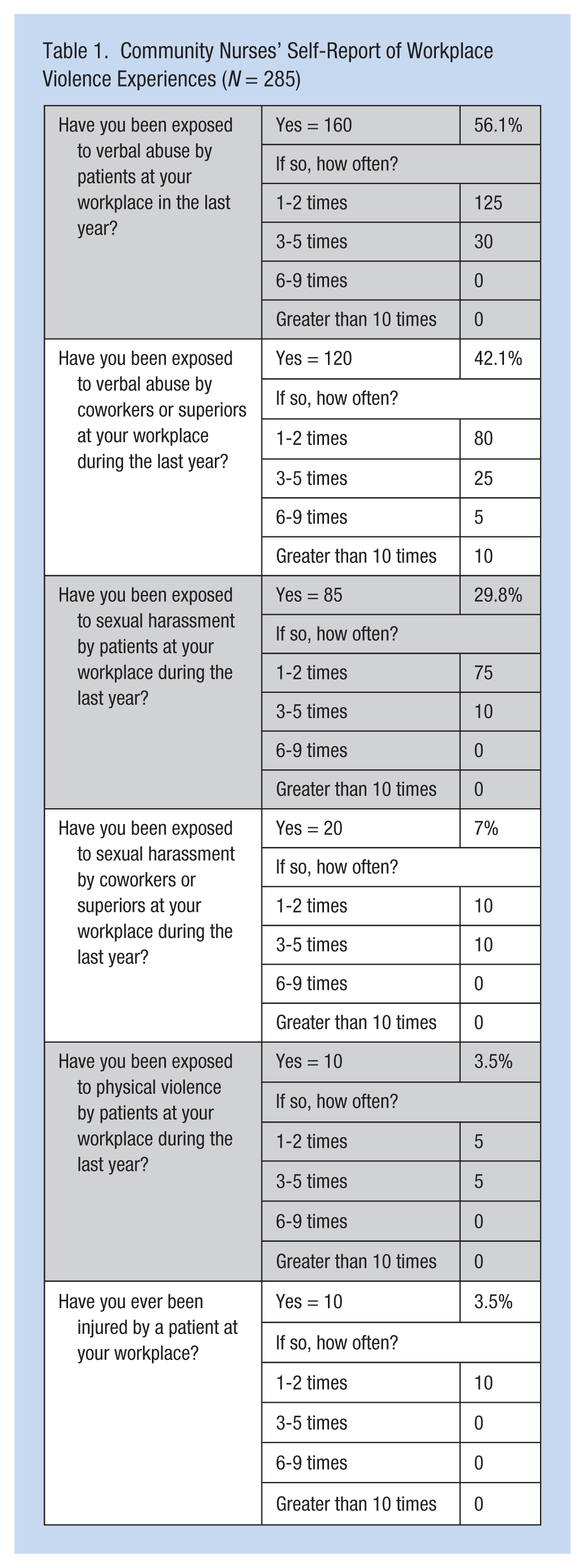
More than 56% of respondents reported verbal abuse by patients in the last year. Cases of horizontal or lateral verbal violence were observed by 42% of community nurses at the workplace. Almost 30% of respondents reported sexual harassment by patients during the past year. Seven percent of community nurses reported they were targets of sexual harassment by their colleagues or superiors. In the past year, 3.5% of community nurses reported physical violence.
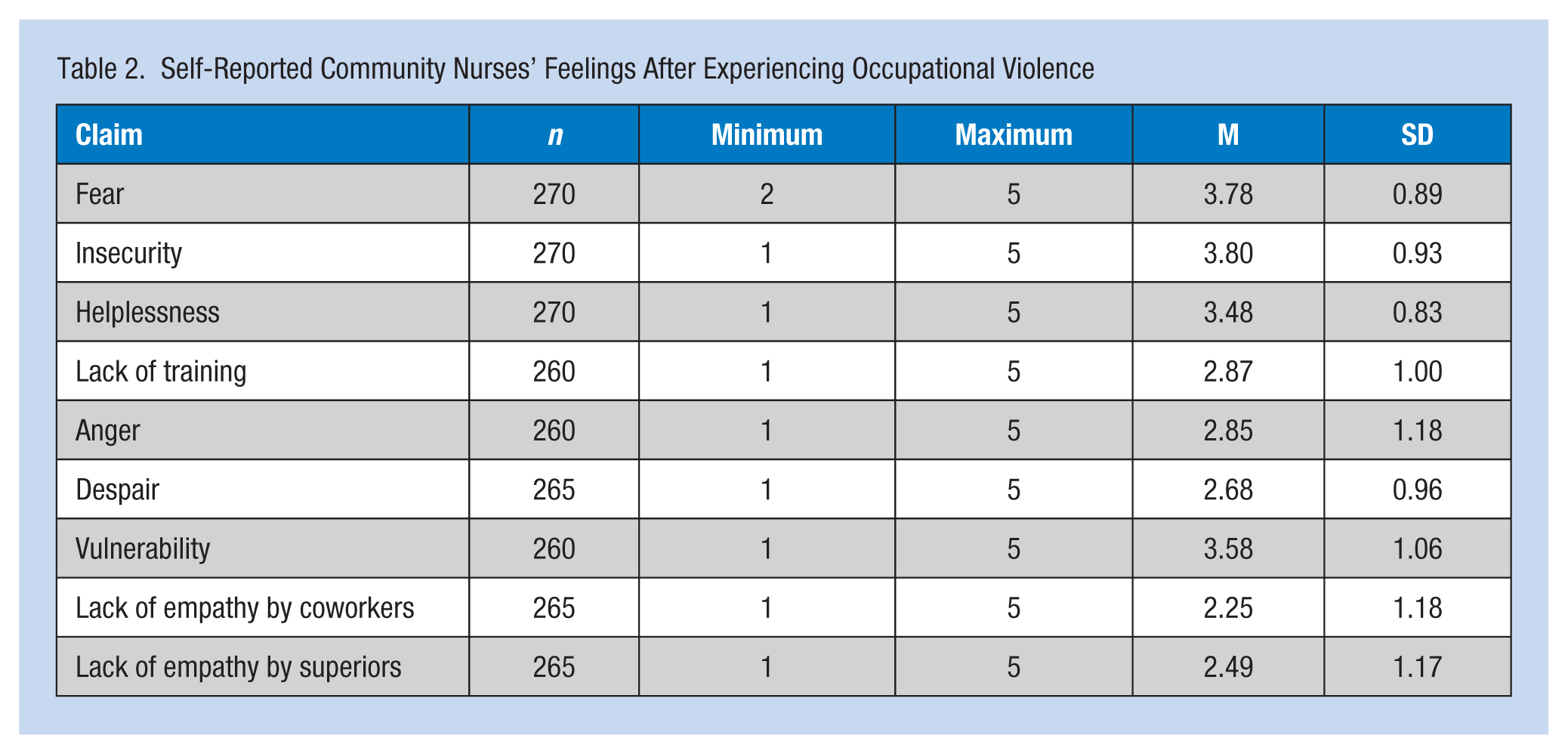
Community nurses reported feeling safe at their workplaces (M = 3.8, SD = 0.64 on a scale of 1 to 5; Table 1). Emotions and conditions experienced by community nurses during patients’ aggressive behaviors are summarized in Table 2. When faced with patients’ aggressive behaviors, community nurses most frequently felt insecure (3.80), fearful (3.78), vulnerable (3.58) and helpless (3.48), and least frequently felt superiors (2.49) or coworkers (2.25) lacked empathy. Furthermore, a correlation analysis of different types of violence reported by study participants established relationships between physical violence by patients in the past year and workplace injury (r = .481; p < .01), helplessness and vulnerability (r = .508; p < .01), lack of training and anger (r = .519; p < .01), vulnerability and despair (r = .535; p < .01), vulnerability and fear (r = .696; p < .01), and lack of empathy by coworkers and lack of training by superiors (r = .879; p < .01). The correlations between the independent variables of “feelings of safety at the workplace” and “insecurity,” “fear,” and “vulnerability” are shown in Figure 1. Variables of “insecurity,” “fear,” and “vulnerability” explained 16% of the variance in “feelings of safety.” “Vulnerability” and “insecurity” were significant predictor variables (Figure 1).
Community Nurses’ Self-Report of Workplace Violence Experiences (N = 285)
Self-Reported Community Nurses’ Feelings After Experiencing Occupational Violence
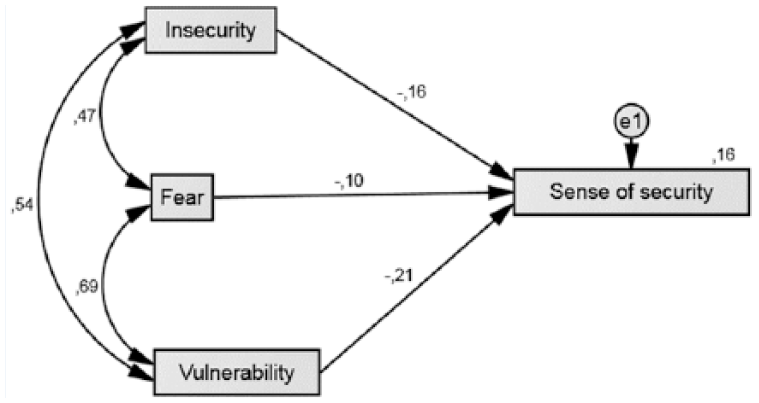
Correlation between individual variables.
Furthermore, the researchers investigated measures used by the organization to ensure safety during patients’ aggressive outbursts as well as the influence of other factors. The statements with the most favorable responses were “Personal characteristics of team members affect the quality of my work” (4.04), “Conflicts among team members can affect the safety and quality of patient care” (3.95), “Administration deals with the violence” (3.67), and “I have all the means to ensure safe patient care at my disposal” (3.54). The statements with the least favorable responses were “Administration supervises the management of patient aggression” (2.61) and “I rely on pure luck that nothing will happen at my workplace” (2.50).
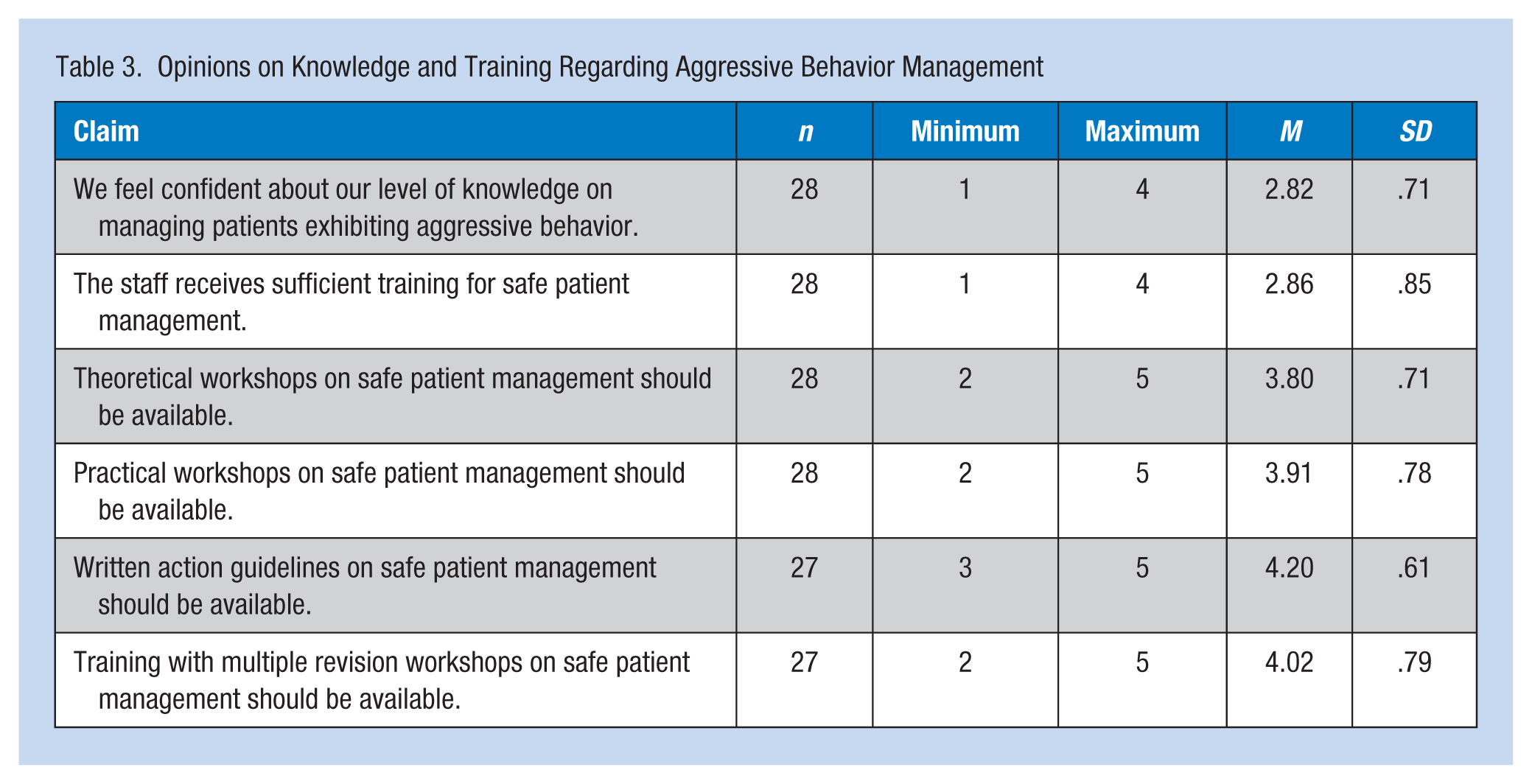
The employees’ opinions about their own knowledge and education on aggression management are shown in Table 3. Community nurses evaluated their knowledge of patient aggression management as 2.82; they reported that routine workshops (4.02) and written guidelines (4.20) were most effective in managing patient aggression. To establish an association between patients’ verbal violence toward community nurses and nurses’ subsequent fear of patients’ inappropriate or aggressive behavior, nonparametric tests were used because the data were not normally distributed (χ2 = 13.215, p > .05). The association was not confirmed as the differences between the groups were not statistically significant. Furthermore, the association between feeling safe at work and sufficient knowledge to manage patients’ aggressive behaviors was also not established (χ2 = 30.357, p > .05).
Opinions on Knowledge and Training Regarding Aggressive Behavior Management
Discussion
The aim of this research was to identify the frequency and intensity of workplace violence toward community nurses in Slovenia. For the purposes of this research, a nonexperimental survey design was used to guide the study. Few studies on violence toward nurses have been conducted in Slovenia; published studies tend to focus on a single nursing specialty and use a variety of research methodologies.
The researchers found that community nurses are threatened by verbal abuse from patients most often, followed by sexual harassment and physical violence. Community nurses often enter the homes of patients alone and do not have the support or protection of colleagues when they encounter violence or harassment. However, this study demonstrated less physical violence against community nurses (3.5%) compared with the physical violence experienced by paramedics (26.8%; Gabrovec, 2015), general hospital nurses (31%; Hahn et al., 2010; Lundstrom, Saveman, Eisemann, & Astrom, 2007), psychiatric nurses (84.2 %; Gabrovec et al., 2014), and long-term care nurses (83%; Franz et al., 2010).
The researchers found less verbal aggression toward community nurses (56,1%) than psychiatric nurses (92.6%; Gabrovec et al., 2014), paramedics (78%; Gabrovec, 2015), general hospital nurses (72%; Hahn et al., 2010), and long-term care nurses (71.7%; Gabrovec & Eržen, 2016). However, the authors found more cases of sexual harassment in this study (30%), then in studies of psychiatric nurses (24.6%; Gabrovec et al., 2014) and paramedics (24.4%; Gabrovec, 2015), but more cases of sexual harassment in a study of long-term care nurses (35.5%; Gabrovec & Eržen, 2016) than in this study.
When faced with aggressive patients, respondents most often experienced insecurity, fear, and vulnerability; these nurses reported that they were least likely to experience lack of understanding from colleagues. However, the prevalence of vertical and horizontal abuse in this professional group is also worrisome. The researchers found statistically significant correlations between physical violence and injury, helplessness and vulnerability, lack of training and fear, vulnerability and despair, and vulnerability and fear. The results of the study are consistent with previous research (Gabrovec et al., 2014).
These results provide a basis for developing comprehensive prevention strategies and employee training tailored to the needs of community nurses (Josefsson & Ryhammar, 2010).
Community nurses evaluated their knowledge of patient aggression management, reporting that routine workshops and written guidelines were most effective in learning to manage patient aggression. According to this research, community nurses should attend routine continuing education workshops designed to teach nurses how to manage aggression directed toward them. Research results can provide a starting point for developing a comprehensive approach to managing aggression toward staff, as proposed and implemented in psychiatric nursing where the preliminary results of applying a comprehensive model have been successful (Gabrovec & Lobnikar, 2014). In addition, agencies must establish a culture of safety by creating systematic training models, taking necessary precautions to ensure safety, and preparing protocols to be used in the event of violent situations (Gabrovec & Lobnikar, 2015).
This study is limited by questionable self-reports and by the lack of qualitative data, which would better explain the occurrence of violence.
Conclusion
This study focused on the prevalence of aggression toward community nurses in Slovenia. Community nurses are exposed to frequent verbal abuse and sexual harassment from their patients as well as vertical and horizontal violence in their professional group. Community nurses need comprehensive prevention strategies and functional training programs to prevent and manage aggression directed toward them. To determine the range of problems encountered before, during, and after violent episodes in the workplace, it would be useful to conduct a survey with the same methodology applied to other aspects of health care, as well as a study using qualitative methodology to expose the characteristics and effects of such violence.
Applying Research to Practice
The study shows that employees in community nursing need to develop a comprehensive approach to managing aggression. The employees require a systematic and comprehensive approach to workplace violence management. They are in need of a recurrent theoretical and practical aggression management training program. The results of the study can therefore be the basis for the development of an organizational model for the control of violence directed at health care workers and treatment quality provision by developing written guidelines. A functional approach to permanent health care staff training would be appropriate.
Footnotes
Acknowledgements
The author thanks the management of health care and nursing facilities, as well as the nursing staff, for participating in this study.
Authors’ Note
This article and its content has not been published or submitted for publication elsewhere. No declaration has been violated during collection of data for this research (Declaration of Helsinki in 1995—as revised in Tokyo 2004, etc).
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Branko Gabrovec is a senior researcher at the National Institute of Public Health of Slovenia. His main interest and expertise is in health systems research, nursing care, and work safety.