
Abstract
Minimal contact lifestyle interventions with multiple components coupled with health screening have the potential to improve worker health. The purpose of this study was to test a minimal contact multiple component lifestyle diet and exercise intervention. The multiple components that were included in this project included a worksite health screening, brief counseling session, emailed newsletter, and a pedometer. In response to the intervention, participants reported an increase in green salad, fruit, and vegetable consumption as well as an increase in self-efficacy for consuming three servings of fruits and vegetables a day. Study participants also demonstrated a significant increase in physical activity as shown by their responses to the question, “During leisure time I walk.” A minimal contact multiple component worksite health promotion program with relatively high feasibility and low cost can improve workers’ health-related behaviors, and participants can become more aware of their health.
Diets high in fat and low in fruits and vegetables have been associated with chronic diseases and risk factors including cardiovascular disease, stroke, cancer, diabetes, and obesity (de Souza, Swain, Appel, & Sacks, 2008; Moore & Thompson, 2015). Unfortunately, despite nutrition education and health campaigns, more than 80% of Americans do not meet dietary recommendations (DeSalvo, Olson, & Casavale, 2016). Similarly, the disease outcomes mentioned above are also related to low levels of physical activity (Booth, Roberts, & Laye, 2012). More than 23% of adults report no leisure-time activity and less than half of American adults meet the Centers for Disease Control and Prevention (CDC)/American College of Sports Medicine physical activity recommendations (Arias-Palencia et al., 2015).
Large-scale programs such as CDC’s 5-A-Day Program and National Physical Activity Initiative have increased awareness for many Americans, but changes in actual behavior are small (C. Rooney et al., 2016). In part, this lack of behavior change may be due to campaigns that have not incorporated behavior-change principles (i.e., personally relevant motivators, goal setting, and targeted change for specific groups of individuals). In-person counseling can and does use those principles and it is possible to improve health behaviors through intensive counseling and intervention (Stonerock & Blumenthal, 2016). However, intensive interventions may not be feasible for public health settings, and program cost may limit their usefulness in worksite settings (Hannon et al., 2012). Effective and efficient program designs and delivery methods are needed.
Multi-component interventions are more desirable than one-dimensional strategies. The literature has demonstrated that one-dimensional approaches (e.g., mailing a letter) do not effectively impact behavior change (Schroer, Haupt, & Pieper, 2014). Projects that include two or more intervention strategies tend to demonstrate significant, positive changes in behavior and outcomes (Schroer et al., 2014).
Because approximately 142 million Americans are active in the U.S. labor force and employers provide health care coverage to approximately 70% of these employees, offering worksite health screenings is both logistically and economically advantageous (Hewitt, 2015). If worksite health screenings are offered broadly, risk factors for chronic disease can be identified and treated at an early stage prolonging years of life and improving quality of life. Worksite health screenings may better accomplish cost and health objectives than individual clinical interventions because transportation, appointment time, and other access barriers are eliminated at the worksite and the legitimacy of preventive health services at the worksite is promoted. Standard office-based approaches have had limited success; nurse-based care with health education has demonstrated greater efficacy (Berra, Miller, & Jennings, 2011). Worksite interventions are often nurse-based and stress health promotion, disease and injury prevention, health education and health coaching. Thus, the worksite is an ideal setting for the delivery of health promotion and health maintenance services.
Minimal contact lifestyle physical activity interventions have been moderately successful at increasing physical activity (Croteau, 2004b; DuVall, Dinger, Taylor, & Bemben, 2004; B. Rooney, Smalley, Larson, & Havens, 2003). These interventions are relatively low cost, require little face-to-face interaction between participants and those delivering the interventions, and encourage worker involvement in self-selected physical activity throughout the day. For some of these interventions, participants received pedometers to monitor their ambulatory physical activity. In addition, some studies have used interventions specifically based on pedometer measurements with participants recording steps per day thus increasing participant self-efficacy and motivation to be physically active (Croteau, 2004b; Dinger, Heesch, Cipriani, & Qualls, 2007; Pinto et al., 2002). The purpose of this study was to test a minimal contact multiple component lifestyle diet and physical activity intervention. The multiple components that were included in this project were a worksite health screening, brief counseling session, a monthly emailed newsletter, and a pedometer that was used to encourage workers to participate in the program.
Method
This study used a pre-experimental one-group, pretest–posttest design with outcome variables collected at baseline and immediately following the 8-month intervention. All data collection took place at the worksite from 2007 through 2008. Participants were recruited from an automotive company located in southeastern Michigan. Inclusion criteria included white-collar workers who mainly worked in offices and performed tasks requiring mental effort, were age 18 years and older, and had no physical limitations. A total of 347 workers volunteered to participate in this study and were asked to complete a self-administered questionnaire, along with height, weight and blood pressure measurements. Twenty-seven respondents were excluded from the study due to omission of questionnaire responses (i.e., at least half of each survey scale was omitted), leaving 320 workers who began the study. After 1 year, 189 participants were no longer employed at the worksite due to layoffs and transfers and thus could not complete the second questionnaire. A final sample of 131 (41%) participants completed the intervention and the postintervention data collection.
Intervention
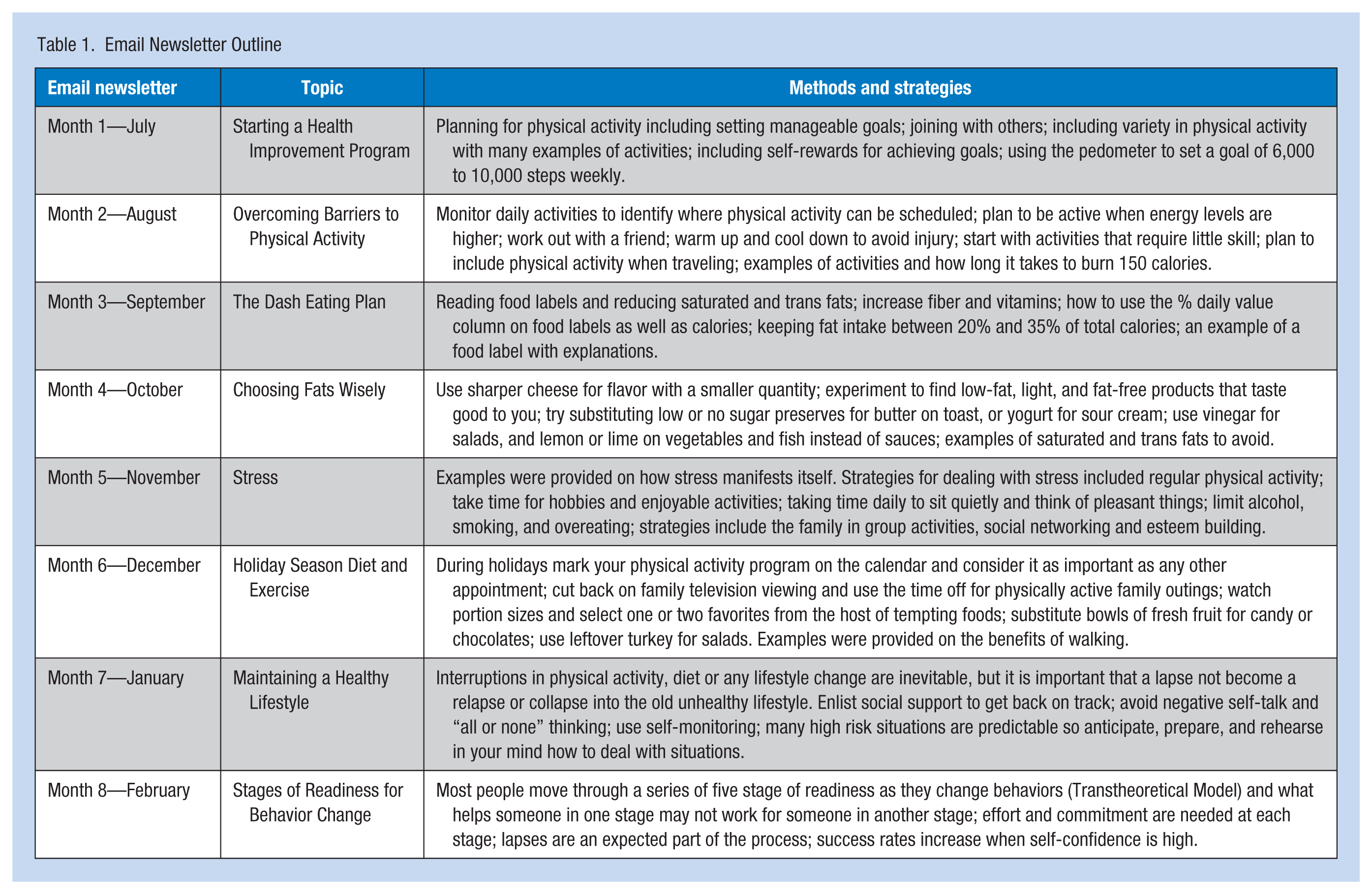
Participant screening included height, weight, blood pressure, dietary habits, and physical activity habits. Participants then received a short 15-minute counseling session from a nurse tailored to the information from the screening. A monthly newsletter was emailed to all the employees at the worksite (Table 1). The primary focus of the newsletter was to increase self-efficacy for improving dietary habits and increasing physical activity. Self-efficacy plays an important role in both the adoption and maintenance of lifestyle behaviors in adult populations (Stoutenberg et al., 2016). Self-efficacy is the confidence individuals have in their ability to perform a specific behavior such as physical activity and diet. In both descriptive and experimental studies, self-efficacy has been shown to be a consistent predictor of short- and long-term success in changing health-related behaviors, including physical activity and healthy eating (Hamilton, Warner, & Schwarzer, 2016; Stoutenberg et al., 2016).
Email Newsletter Outline
Measures
Questionnaires included questions about individual characteristics (e.g., age, sex), physical activity, dietary habits, self-efficacy for exercise, self-efficacy for a healthier diet, self-efficacy for a healthier lifestyle, and stress. One nurse measured height and weight using a clinic-type scale and stadiometer; participants wore light clothing and no shoes. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured twice by trained nursing staff using a mercury sphygmomanometer with an appropriately sized cuff on the right arm while sitting and after a 5-minute rest.
Physical activity, an outcome variable, was assessed with the Baecke Physical Activity Questionnaire, a reliable and valid self-reported questionnaire developed for the assessment of habitual physical activity in epidemiologic studies (Baecke, Burema, & Frijters, 1982; Philippaerts, Westerterp, & Lefevre, 1999). The questionnaire was composed of three indices: work (Items 1-8), sport (Items 9-12), and nonsport leisure-time activity (Items 13-16). Items in each index were scored on a 5-point Likert-type scale, with descriptors ranging from never to always. Three additional items provided data to calculate the simple sport score, including the type of activity and the number of hours weekly and number of months yearly that the individuals participated in the activity. The researchers applied specific scoring criteria for each index; the unitless score ranged from 1 to 5 (Baecke et al., 1982). The three indices were summed to yield a continuous total physical activity score ranging from 3 to 15.
Dietary habits were assessed with the 5-A-Day Food Frequency Questionnaire to estimate fruit-and-vegetable intake in the past month (Di Noia & Contento, 2009). For each of the questionnaire items, participants were asked how often they “ate or drank each of the items of food in the past month.” Answer choices were coded as follows: Never (1); 1 to 3 times per month (2); 1 to 2 times per week (3); 3 to 4 times per week (4); 5 to 6 times per week (5); 1 time per day (6); 2 times per day (7); 3 times per day (8); 4 times per day (9); 5 or more times per day (10).
Intake of French fries or fried potatoes was excluded from the computation of fruit and vegetable servings. Reliability and validity of the questionnaire has been established (Warneke, Davis, De Moor, & Baranowski, 2001).
The self-efficacy measures did not reflect program duration (8 months) because participants were not asked to change their behavior over the duration of the study. Self-efficacy for exercise was assessed by asking, “How sure are you that you can exercise for 30 minutes at least 3 days per week over the next 12 months?” Likewise, self-efficacy for a healthier lifestyle was assessed by asking, “How sure are you that you can live a healthier lifestyle over the next 12 months?” Both items were scaled from 0 (completely unsure) to 10 (completely sure). Self-efficacy for a healthier diet was assessed with two items, “How sure are you that you can eat at least 3 servings of vegetables and fruit each day?” and “How sure are you that you can eat at least 5 servings of vegetables and fruit each day?” Items were scaled from 0 (very unsure) to 4 (very sure); an average score was calculated. Stress was assessed with two items, “How would you rate your overall stress level?” scaled 0 (no stress) to 4 (very high) and “During the past 30 days, how often did you have a lot of psychological distress?” scaled 0 (never) to 4 (often). In addition to descriptive statistics, paired t tests were computed to determine differences from baseline to post intervention for physical measures as well as questionnaire items. The α level was set at .05 for all comparisons.
Results
Of the 131 participants completing the 8-month program, ages ranged from 26 to 67 years. Average height and weight for the female participants was 164.8 ± 6.1 cm (64.6 ± 2.4 inches) and 82.3 ± 20.4 kg (181.1 ± 44.9 pounds), respectively; for the male participants 177.3 ± 8.9 cm (69.9 ± 3.5 inches) and 87.1 ± 14.8 kg (191.6 ± 32.5 pounds), respectively. Blood pressure and body mass index (BMI) did not significantly change between baseline and postintervention measures.
The dietary questions showed that most participants increased servings of green salad, fruits, and vegetables (Table 2). Interestingly, self-efficacy for consuming three servings of fruits and vegetables a day increased significantly but not for consuming five servings. For the physical activity questions, no change in total physical activity or in the work, sport, or leisure-time indexes was found. However, a significant increase in participants’ response to the question “During leisure time I walk” (Table 2) was documented. Self-efficacy did not improve for living a healthier lifestyle or participating in physical activity three times a week.
Changes in Physical Characteristics, Self-Efficacy, and Dietary and Physical Activity Behavior (n = 131)
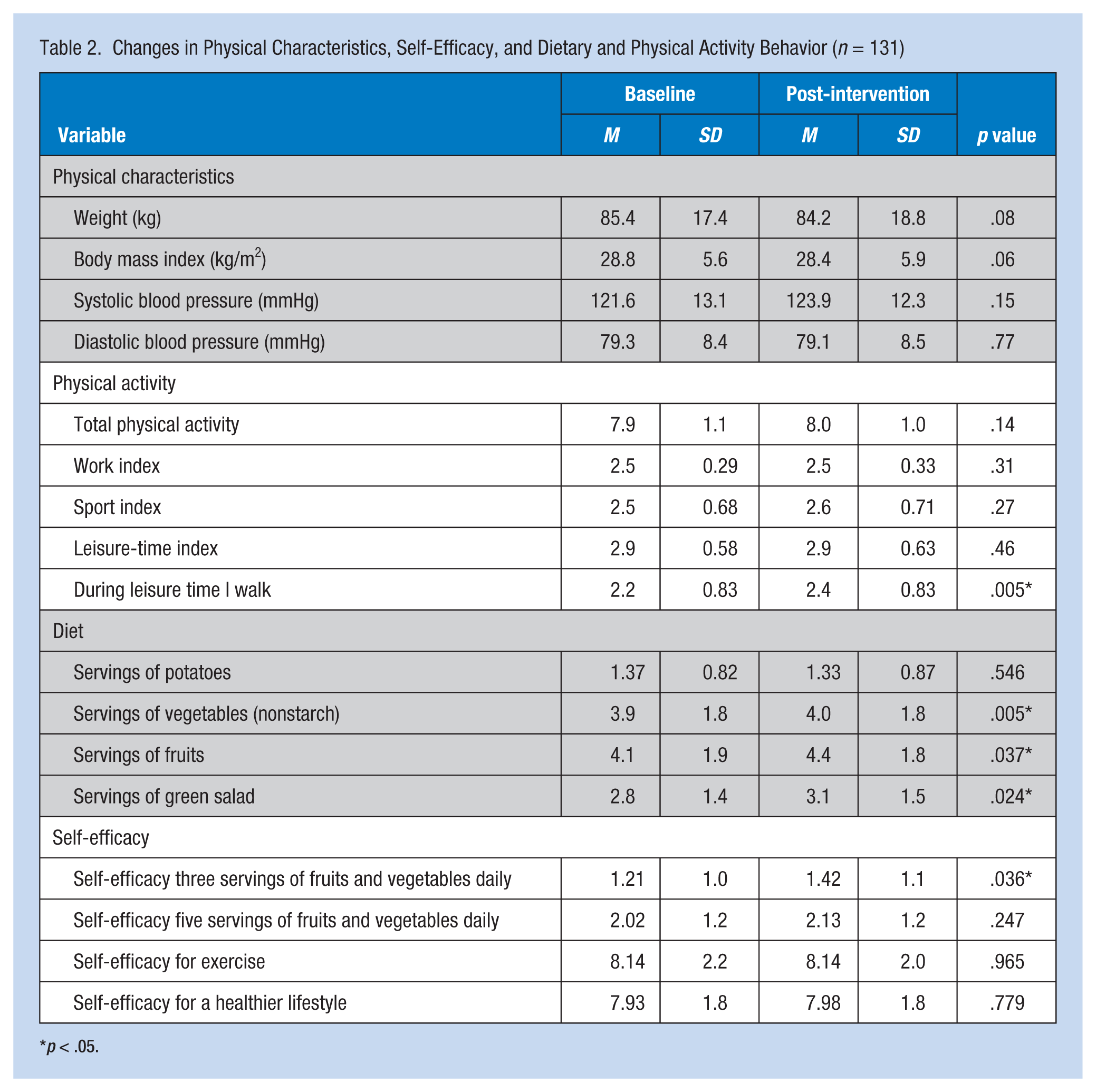
p < .05.
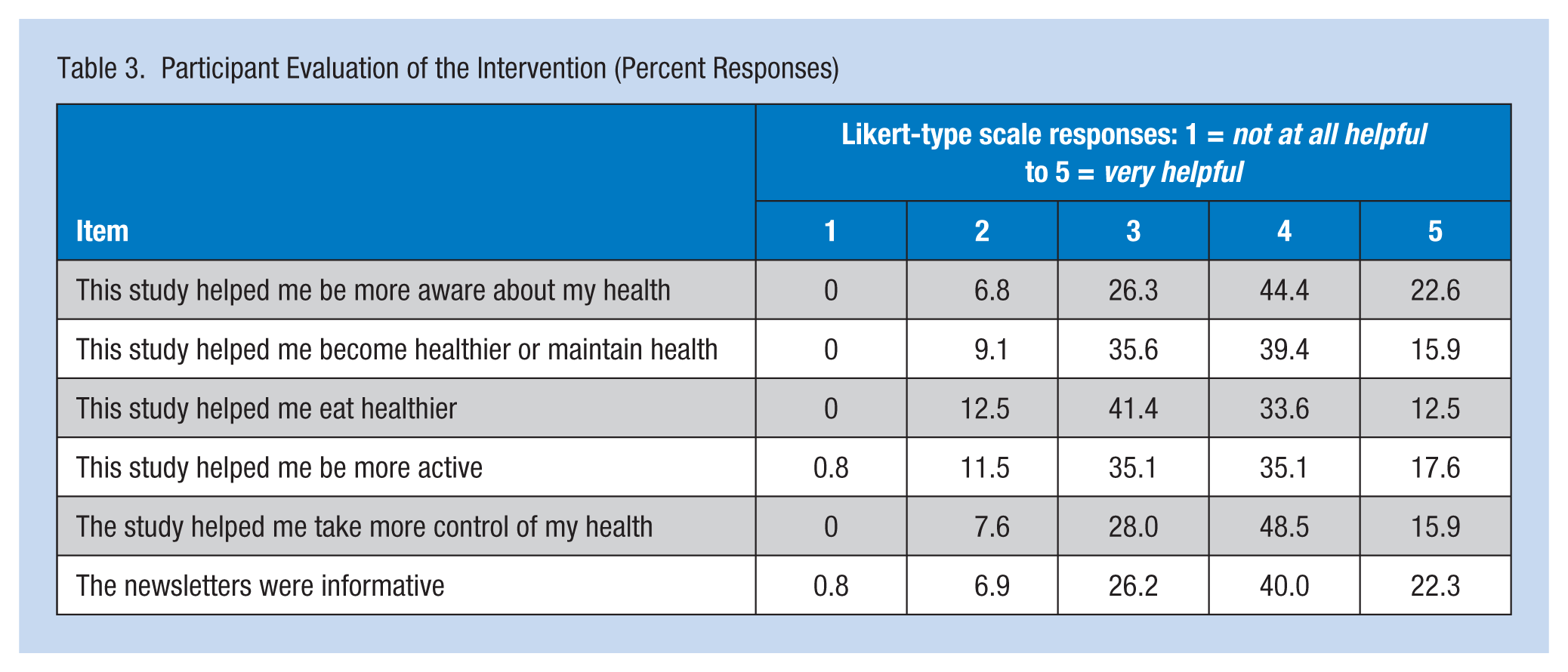
A key goal of the pilot project was to determine the feasibility of developing and delivering a minimal contact intervention which was clearly established. Table 3 shows that 67% of the participants thought the program was helpful or very helpful in making them more aware of their health, 55.3 % indicated that the program was helpful or very helpful in helping them become healthier or maintain health, and 64% responded that this study helped them take control of their health. For the diet and physical activity questions, 46.1% indicated that the program was helpful or very helpful in helping them eat healthier and 52.7% responded that the program was helpful or very helpful in participants becoming more active. A high percentage of participants indicated that the email newsletters were informative (62.3%).
Participant Evaluation of the Intervention (Percent Responses)
Discussion
This study demonstrated that it is feasible to deliver a minimal contact nutrition and physical activity intervention program for white-collar workers at the worksite and can achieve significant improvements in physical activity and dietary behavior. Significant improvements in both fruit-and-vegetable intake and leisure-time walking were documented, although no changes in blood pressure or BMI were recorded. However, because the study did not incorporate a randomized design and only 41% of initial participants completed the study (primarily due to company layoffs), more definite conclusions must await further research.
Block, Block, Wakimoto, and Block (2004) evaluated an email intervention in a corporate setting to improve dietary habits. Their 12-week intervention used a tailored approach; using baseline data, individuals were placed into one of seven “lifestyle paths” depending on how much the participant cooked or ate in restaurants. Separate weekly email messages were then sent to each category of individuals. Their findings were similar to the present study with increased consumption of fruits and vegetables. The advantages of tailored interventions have been clearly demonstrated when promoting behavior change (Pignone et al., 2003; Rosal et al., 2001). However, tailoring adds expense and complexity, and if cost and simplicity are essential to providing a worksite health promotion program, tailoring may reduce feasibility. Each newsletter developed for the study intervention had its own theme and was based on self-efficacy, but provided many different strategies for improving particular health behaviors. Because the study population was white-collar workers, each with their own computer at work (and presumably at home), it was assumed that these individuals were experienced in “surfing the net” and browsing through large databases, pausing to focus on topics or ideas the individual found useful. This approach is in effect a form of “self-tailoring” because individuals are free to causally peruse the newsletter looking for information they find helpful.
Although tailoring was not used in the development of the newsletters for this project, tailoring did play a role in health screening which was part of the intervention. The screening included height, weight, blood pressure, dietary habits and physical activity. Immediately following the health screening, participants received a short 15-minute, nurse-led counseling session tailored to screening outcomes. A survey by Hewitt Associates in 2015 showed 72% of 1,000 employer survey respondents reported having some form of health initiative (Hewitt, 2015). Increasingly, evidence supporting the cost-effectiveness of such programs is compelling. Because screening is already common in the workplace, screenings can provide a baseline and a context to support individual behavior change, especially since this brief intervention can be delivered quickly and easily through email. Because the project began with personal contact and tailored behavior change counseling, the monthly newsletters associated with the project did not appear as random health education messages appearing in their mail boxes and were therefore more relevant to participants.
A number of studies have used pedometers to increase physical activity, but not through a worksite intervention (Croteau, 2004a, 2004b; Dinger et al., 2007). Dinger, Heesch, and McClary (2005) recruited community participants for a minimal contact study; participants were given a pedometer, 6 weeks’ worth of step log sheets, self-addressed envelopes, and some brochures describing strategies for increasing physical activity as well as risks and benefits of physical activity. Each week the participants received email messages targeted toward increased activity based on the Transtheoretical Model. After the 6-week intervention, participants showed a significant increase in minutes spent walking and improvement in many of the Transtheoretical Model constructs. Although this study was minimal contact, it did impose a greater burden on participants as well as on those conducting the study who had to analyze the log sheets and deliver the email messages. The present study used several low cost strategies (i.e., health screening followed by a tailored health counseling session by a nurse, pedometers, and monthly newsletters) and found a significant increase in leisure-time walking, significant changes in dietary and physical activity behaviors, and self-efficacy for changing dietary and physical activity behavior. This approach may be promising in other worksite settings, especially those in which resources are limited.
Although the worksite offers unique opportunities to develop health promotion interventions, these efforts are not without challenges related to advancing the health of the population while protecting individual workers’ rights to privacy and freedom of choice. Health promotion is focused on preventing disease, increasing longevity, and improving quality of life, with additional benefits from the employers’ perspective of improved productivity and fewer health care costs. However, differences in individuals’ beliefs and values about health and the role of government and employers do exist (Buchanan, 2006). Because of these conflicts, occupational health promotion efforts may be viewed by employees as paternalistic or intrusive. When company resources are limited, as they clearly were during the course of this investigation as evidenced by the large number of layoffs, employees may harbor negative feelings about the use of these resources for health promotion at the workplace. Workers may believe that capital would be better spent on employee pay and benefits or workplace improvements for enhanced safety and comfort (Strasser, Gates, & Brehm, 2010).
Given the wide diversity of workplace settings, it is beneficial to also have a wide variety of options when designing worksite health promotion programs. The minimal contact program presented is low in cost, but still showed improvements in worker health-related behaviors, and the participants found the information helpful.
This study was not a randomized controlled trial and therefore the results must be viewed with caution. The purpose of the study was to test, in a real-world situation, the feasibility of the delivery method and the participation of and acceptability to a company and its employees. Application of a randomized design would not have served this purpose, nor did the available funding and time frame permit it. However, the dose-response relationship suggests a real effect. The 41% response rate for the final evaluation is also a limitation, due to the “real-life setting” and rapid changes in the workplace, especially in the auto industry.
Applying Research to Practice
This study demonstrated the feasibility of delivering a minimal contact nutrition and physical activity intervention program in a white-collar worksite and achieving significant improvements in physical activity and dietary behavior. Significant improvements in both fruit-and-vegetable intake as well as leisure-time walking were documented. Because screening is common in the workplace, it can be used to provide baseline data and a context for individual behavior change, especially since this brief intervention can be delivered quickly and easily through email, and provide information for improving health including technological and electronic advancements in the health promotion arena.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Blue Cross Blue Shield of Michigan Foundation.
Author Biographies
Kimberlee A. Gretebeck conducts physical activity and diet interventions with adults and older adults aimed at developing and maintaining a healthy lifestyle.
Tatiana Bailey is Director of the University of Colorado–Colorado Springs Economic Forum in the College of Business. She is an expert on health economics, policy and urban economic development.
Randall J. Gretebeck investigates the role of diet and exercise on energy and macronutrient metabolism in relation to chronic disease prevention. He is also involved in developing noninvasive community-based methods for detecting and monitoring the development of chronic diseases.