
Abstract
Low back pain (LBP) is a common health problem. Professions like physical therapy (PT), involving frequent lifting, bending, or standing, are at risk for developing LBP. The objective of this study was to determine the prevalence of work-related LBP and factors associated with and consequences of work-related LBP among physical therapists in Riyadh, Saudi Arabia. A self-administered online questionnaire (i.e., demographic data, history of LBP before and after working as a physical therapist, work setting, and effect on daily activities) was sent to 600 members of the Saudi PT association. Data were analyzed using the Pearson chi-square test and Mann-Whitney U test. Eighty-eight percent of potential respondents completed the questionnaire. Of these, 89.65% of the therapists reported LBP after beginning their PT practice, and 35.6% reported LBP at the time of this survey. Gender, PT specialty, and duration of contact with patients were all found to be related to LBP. The prevalence of work-related LBP among physical therapist in Riyadh was high, affecting patient care and daily activities of the therapists. Both primary and secondary prevention strategies (e.g., introduce ergonomics into PT curricula, reduce therapist stress, and promote teamwork) are needed to decrease LBP among therapists, so they can effectively care for patients.
Low back pain (LBP) is one of the most common health problems in the world (Hoy et al., 2012), the most frequently reported work-related musculoskeletal disorder (WMSD) associated with physical demands of various professions (Omokhodion & Sanya, 2003). Work-related LBP often leads to disability and impedes the performance of activities of daily living (ADLs; Andersson, 1999). Physical work requiring poor postures and frequent lifting, bending, or twisting are reported to be risk factors for LBP (Coenen et al., 2013).
Several studies have reported high incidence and prevalence of LBP among physical therapists (PT; Iqbal & Alghadir, 2015; Mierzejewski & Kumar, 1997; Molumphy, Unger, Jensen, & Lopopolo, 1985; Rugelj, 2003; Salik & Ozcan, 2004; Shehab, Al-Jarallah, Moussa, & Adham, 2003; West & Gardner, 2001). One study reported LBP to be the most prevalent form of work related musculoskeletal disorders (WRMD) among physical therapists (Cromie, Robertson, & Best, 2002); another similar study ranked PTs second among all health care professions in risk of developing work-related LBP (Hollingdale & Warin, 1997).
Data on the prevalence of WRMD in various professions provides the basis for formulating strategies to prevent or minimize the risk of developing this disorder (Sharma & Golchha, 2011). Although PTs are the largest category of staff working in Saudi rehabilitation services (Alghadir, Zafar, Iqbal, & Anwer, 2015), no previous study has reported on the incidence and prevalence of LBP among physical therapists. Thus, the authors investigated the prevalence of work-related LBP among PTs working in the Riyadh region of Saudi Arabia. In addition, they also identified factors (i.e., age, gender, sub-specialties, and work environment) which might be associated with LBP development and how LBP affects ADLs.
Material and Method
This research study used a survey based on a questionnaire previously published (Iqbal & Alghadir, 2015; Shehab et al., 2003); minor changes were made to the questionnaire due to differences in Saudi work culture. The survey link was sent along with an invitation to participate in the study to the 600 members of the Saudi Physical Therapy Association (SPTA) working in the Riyadh area. Posters explaining the study were displayed in hospitals and online via social networking sites to maximize response rate. Volunteers were also sent to different work settings to explain the study and encourage PTs to participate. A reminder email was sent 2 weeks after the initial invitation. To be eligible for the study, respondents had to be in direct patient contact for at least 1 hour each day and questionnaires had to be complete to be included in the analysis.
Instrument
The questionnaire included 30 items grouped in three domains: demographic and professional characteristics, general health history, and history of LBP before and after practicing physical therapy (PT). Specifically, questions were related to work settings, development of LBP, and the effect of LBP on therapists’ daily activities. Low back pain was defined as an unpleasant sensation in the lower back region below the scapulae and above the hip region, that may or may not radiate to the thighs and legs and which can be further classified into mild, moderate, or severe pain depending on the patient’s ability to perform daily work and non-work activities.
Data Analysis
Data were analyzed using SPSS (Version 19) for Windows (Statistical Package for Social Sciences, IBM Inc., Armonk, NY). Mann-Whitney U was used to test the difference in mean between two quantitative variables, and Pearson chi-square test was used to find the association between two categorical variables. Differences were considered significant if p < .05.
Results
Of the 600 PTs contacted, 502 (84%) completed the online questionnaire and met the inclusion criteria. Among these, 195 (39%) were females and 307 (61%) were males (Table 1). Three hundred sixty-eight (73%) respondents were of Saudi origin; however, no difference in prevalence of LBP based on nationality was observed.
Demographic Data Based on Gender
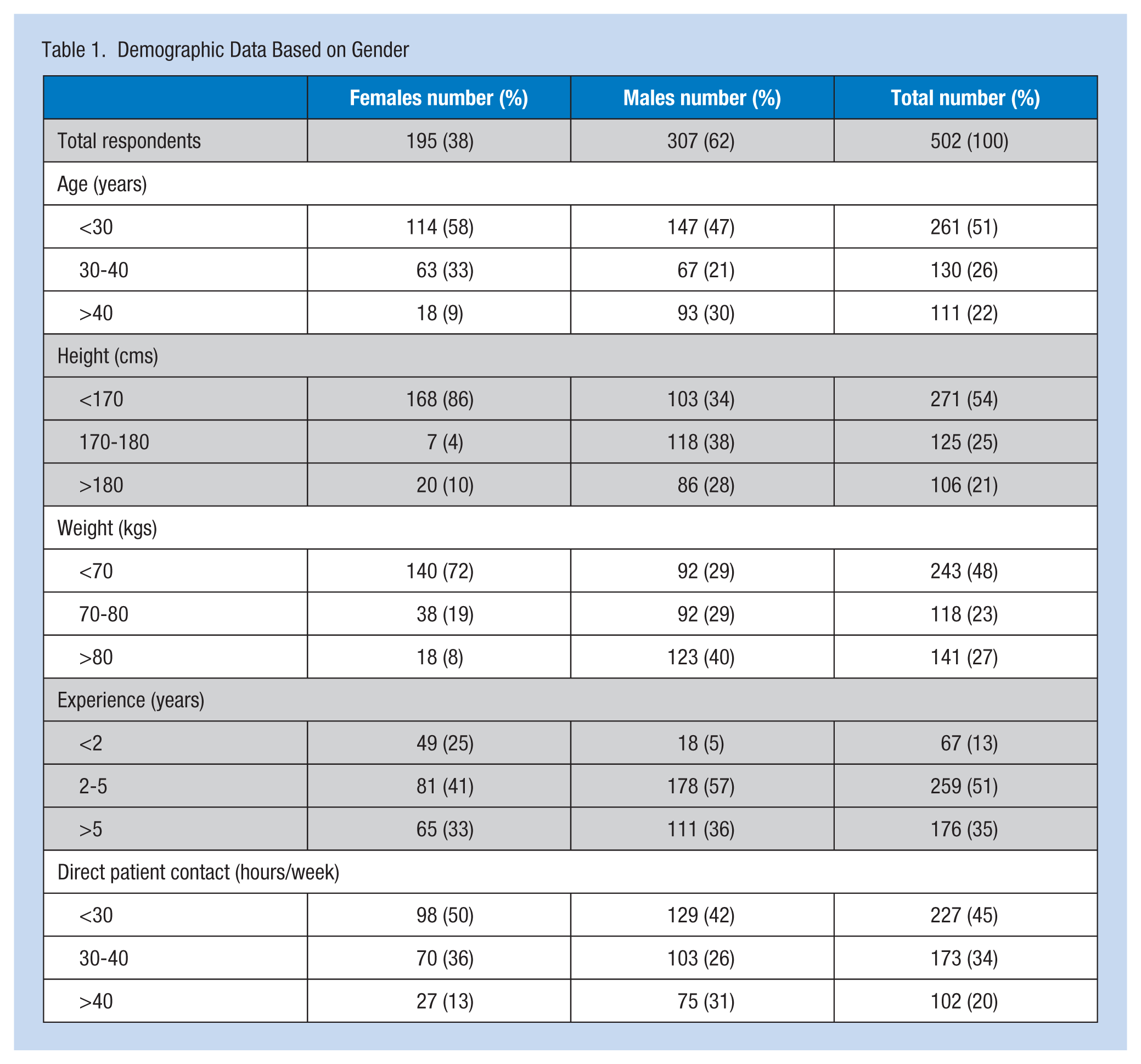
Of the 502 respondents, 281 (56%) of the PTs had earned bachelor’s degrees in PT; 131 (26%) and 55 (11%) had earned master’s and doctoral (PhD) degrees, respectively. The majority of the respondents (259; 52%) had work experience between 2 and 5 years, and 176 therapists (35%) reported experience between 5 and 10 years. Male participants were more experienced than females (Table 1). The distribution of respondents based on specialty is presented in Table 2.
Basic Data and LBP Characteristics of Respondents Before Practicing Physical Therapy
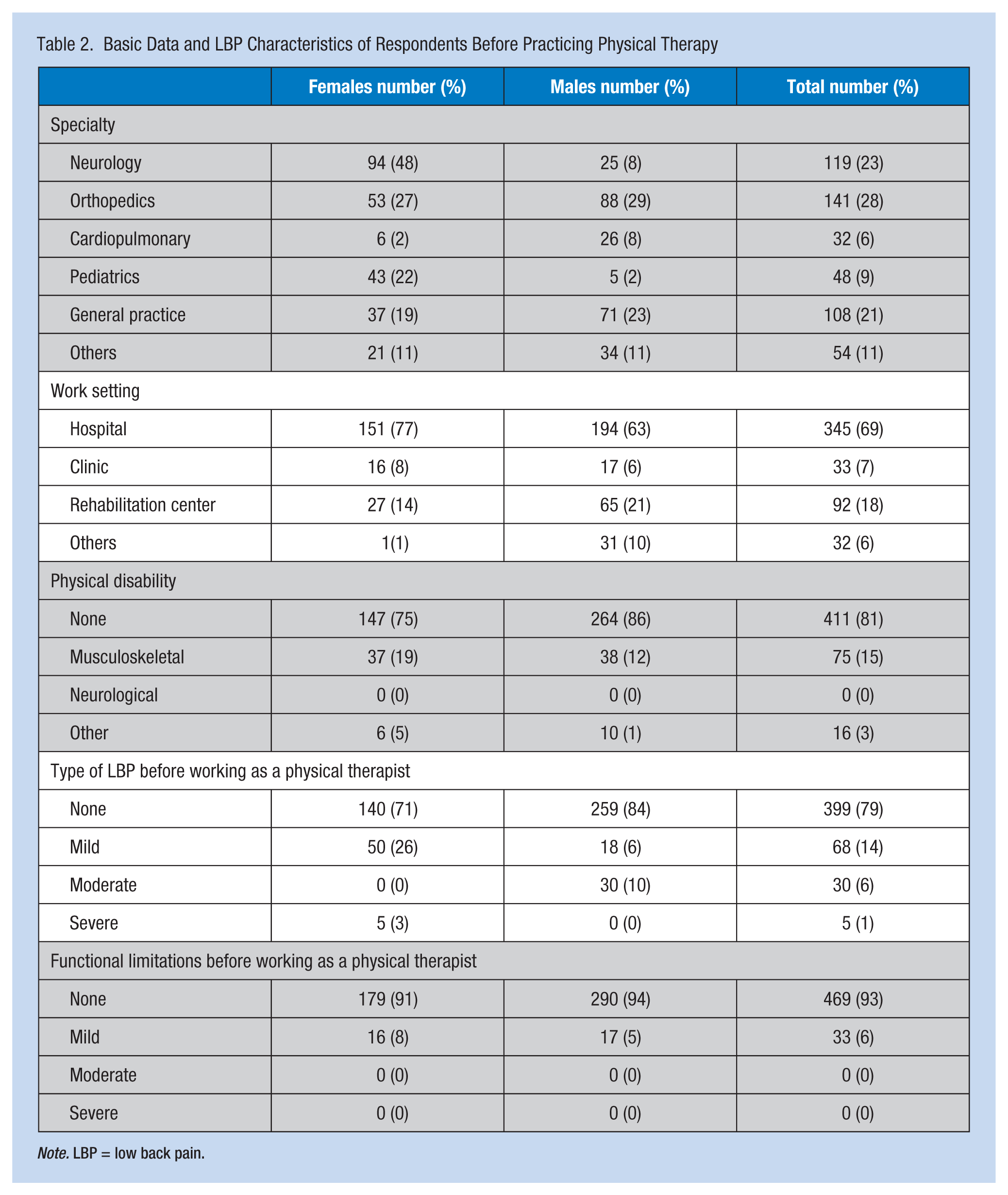
Note. LBP = low back pain.
Of the 502 respondents, 318 (63%) were working for the government; the remaining respondents reported working in the private sector. The majority of respondents (345; 68%) were employed in hospitals (Table 2).
Health History
More than 90% of the respondents (458 of 502) reported no history of illness (e.g., diabetes, arthritis, cardiopulmonary disease). Among remaining respondents, 20 (4%) reported hypothyroidism and 24 (5%) reported either asthma or hypertension. Only 103 (20%) of the 502 respondents reported LBP before working as PTs. Of these, the majority, 50 (26%) females and 18 (6%) males, reported mild LBP. Only five (3%) females reported severe LBP before practicing PT (Table 2). However, nearly 90% (450) reported developing LBP after joining the PT profession. Of these 450 respondents, 177 were females and 273 were males. Distribution of respondents based on gender and severity of pain is presented in Table 2. Thirty-nine percent of therapists reported their LBP was chronic.
Among all 450 respondents who reported LBP after joining the PT profession, 65 (14%), 135 (30%), and 250 (55%) of the therapists reported the average duration of their work-related LBP to be more than 4 weeks, between 2 and 4 weeks, and less than 1 week, respectively. At least 179 (40%) of these respondents, 74 (42%) females and 105 (38%) males, reported LBP at the time of the survey (Table 3).
Characteristics of Work-Related LBP Among Responding Physical Therapists
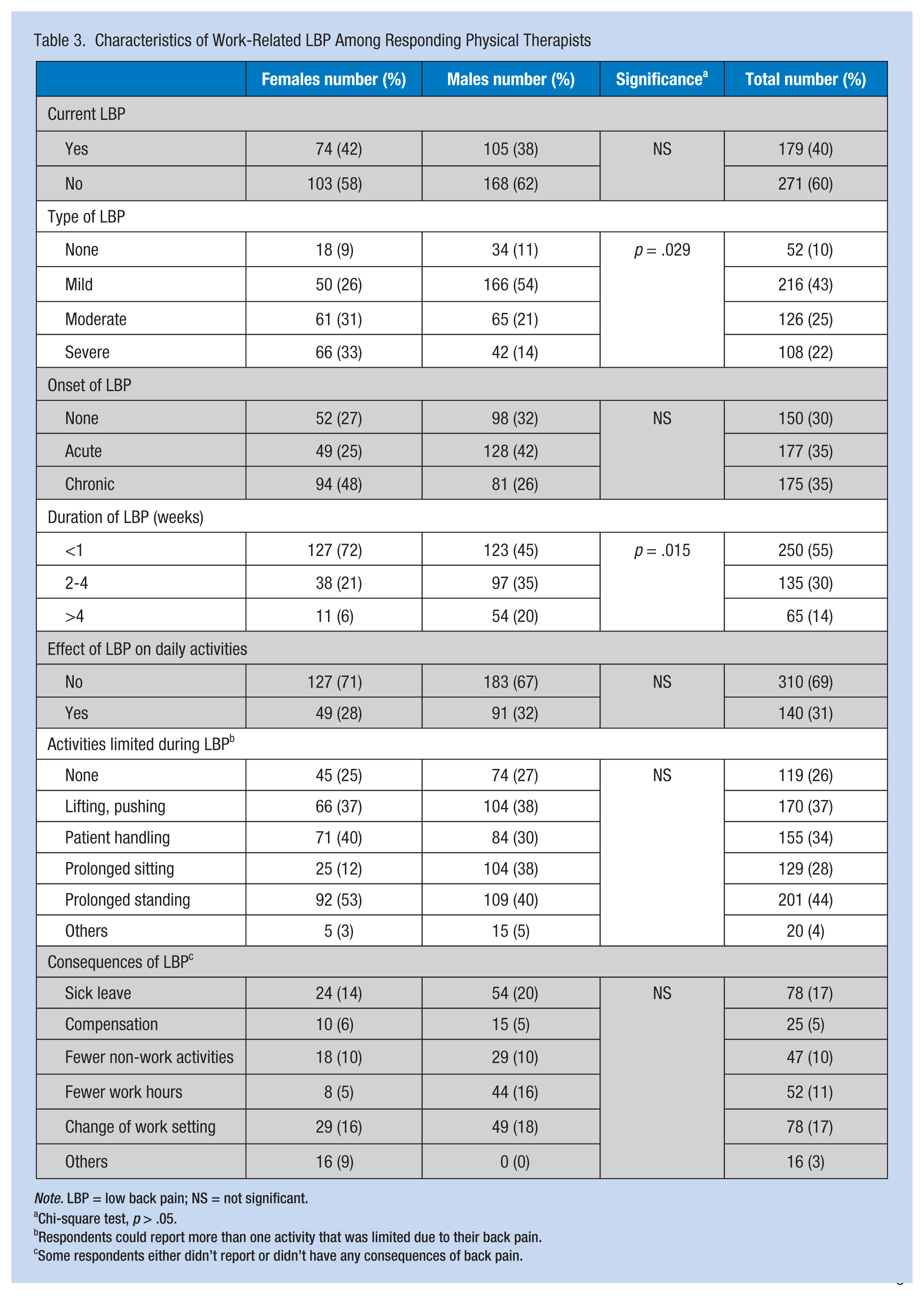
Note. LBP = low back pain; NS = not significant.
Chi-square test, p > .05.
Respondents could report more than one activity that was limited due to their back pain.
Some respondents either didn’t report or didn’t have any consequences of back pain.
On the Visual Analog Scale (VAS), between 0 and 10, 200 (44%) of the PTs reported their worst-ever LBP to be less than a 3, 129 (28%) reported their worst-ever LBP to be between 3 and 5, and 121 (26%) reported their worst-ever LBP to be greater than 5. Reported exact location of LBP is displayed in Table 4. Of 450 respondents who reported LBP, 142 (32%) reported pain in the lower back region and 159 (35%) reported pain in both the lower back and buttock regions (p < .05).
Location of Work-Related LBP Among Responding Physical Therapists
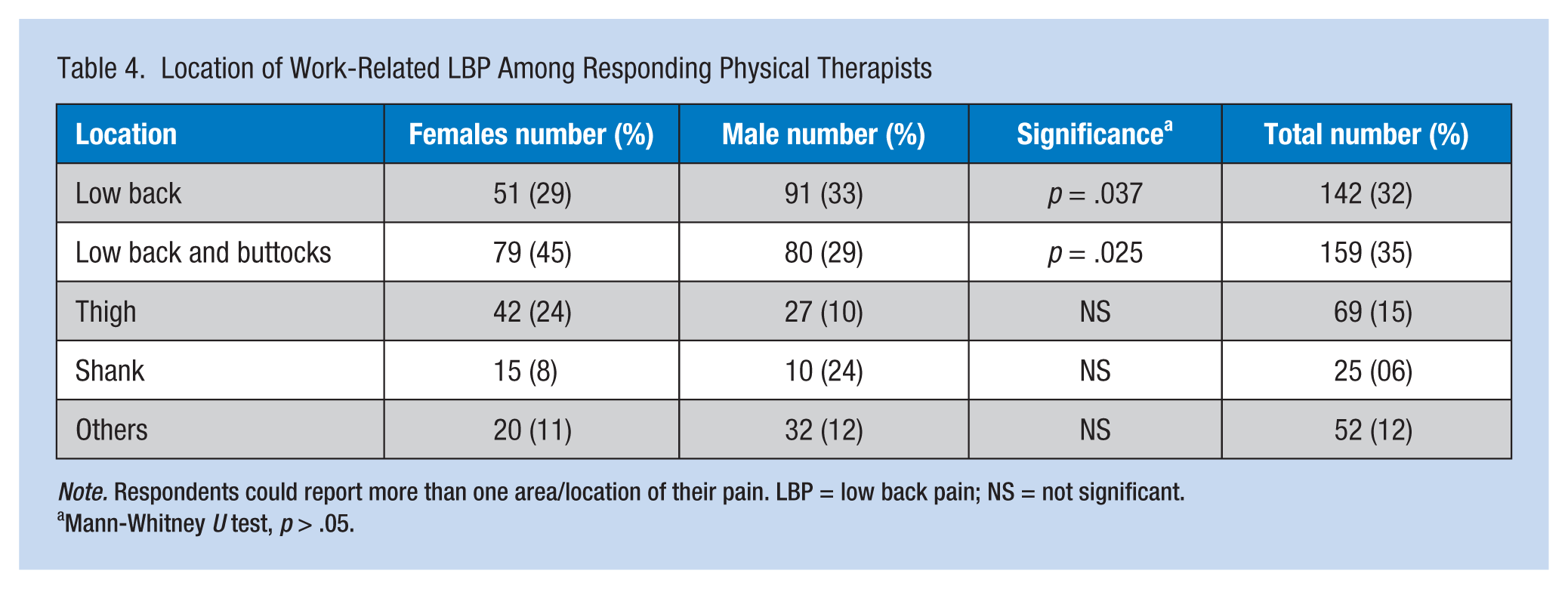
Note. Respondents could report more than one area/location of their pain. LBP = low back pain; NS = not significant.
Mann-Whitney U test, p > .05.
Effect of LBP
Of the 450 respondents who reported developing LBP after joining the PT profession, 140 (31%) PTs reported they were unable to accomplish daily activities involving bending, twisting, or stooping. Another 47 (10%) therapists reported they had to limit non-work activities like shopping and household chores due to pain.
Work activities reported to be most affected by LBP included prolonged standing (201; 44%), lifting and pushing (170; 37%), patient handling (155; 34%), and prolonged sitting (129; 28 %; Table 3). The severity of LBP forced 52 (11%) PTs to decrease their work hours and 156 (34%) PTs to either change work settings or to take sick leave. At least 25 (5%) PTs claimed compensation due to LBP (Table 3).
Factors Associated With LBP
Specialty of the therapist was found to be significantly related to LBP severity and location (p < .05). Of 141 orthopedic specialists, only 43 (30%) reported severe LBP; of 119 neurology specialists, 84 (71%) reported severe LBP. Specialists in orthopedics complained of pain only in the lower back region, but specialists in neurology also reported pain in the buttocks, thighs, and legs as well as the lower back region (Tables 5 and 6).
Patient Contact Per Week and Location of Work-Related LBP Among Responding Physical Therapists
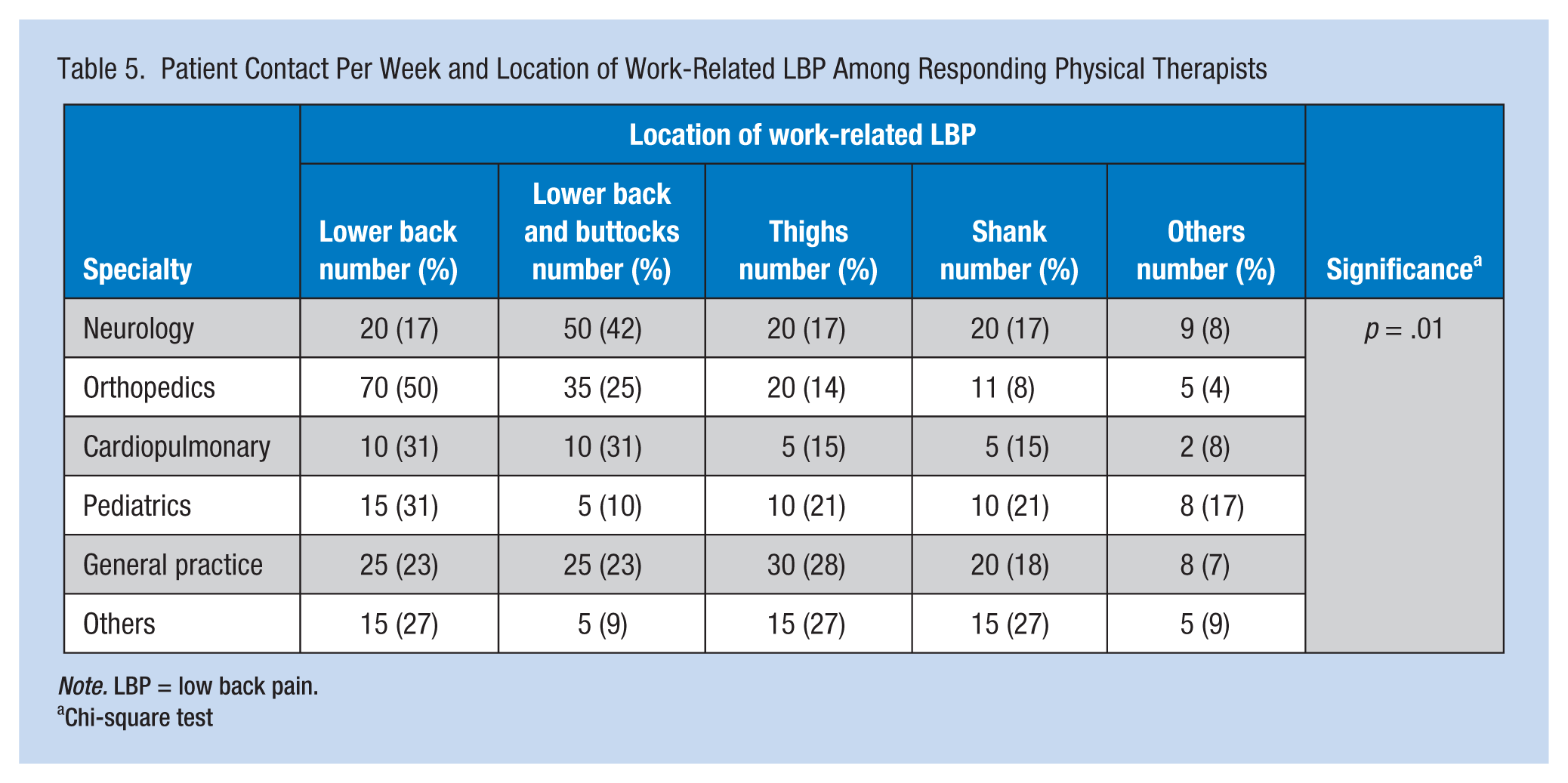
Note. LBP = low back pain.
Chi-square test
Specialty and Severity of Work-Related LBP Among Responding Physical Therapists
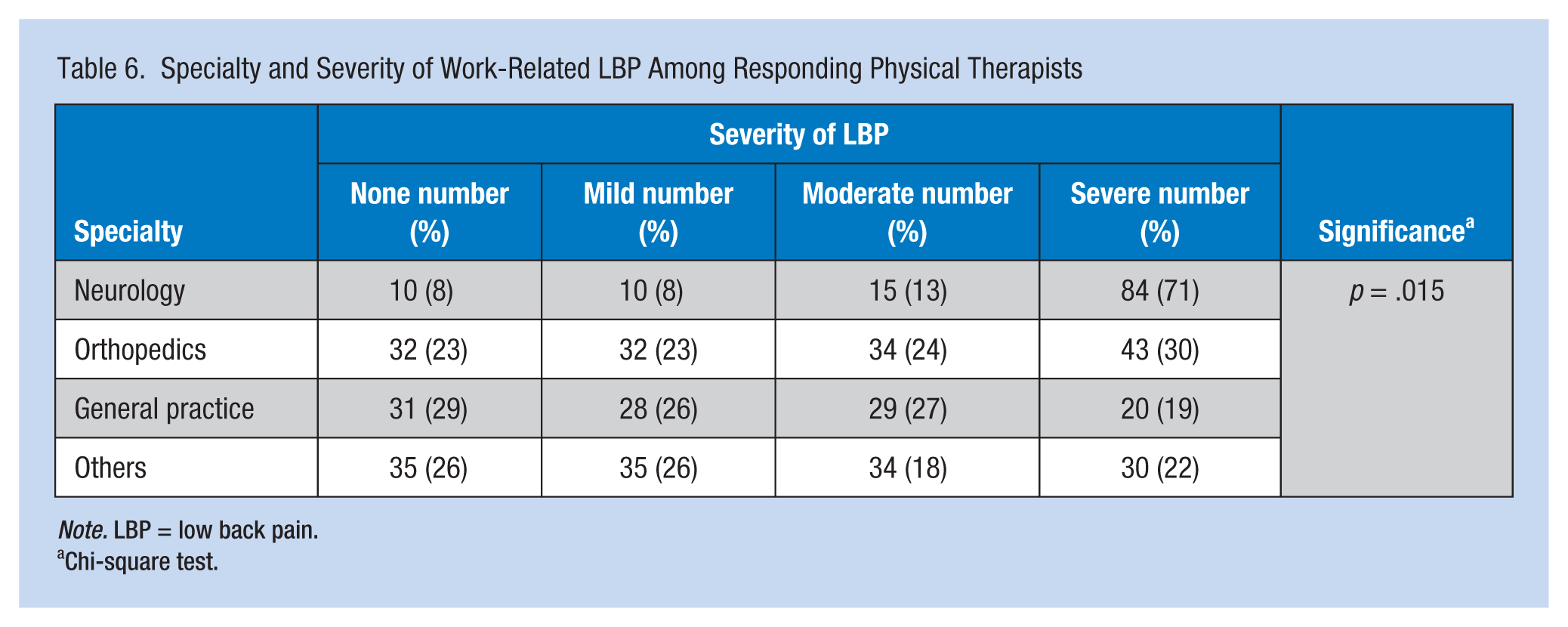
Note. LBP = low back pain.
Chi-square test.
Severity, location, and duration of LBP were related to the gender of the therapist (p < .05). Among 108 PTs who reported severe LBP, 65 (37%) were females and 43 (16%) were males. Compared with females, males reported longer duration of LBP. The majority of males complained of pain only in the lower back region, but females had pain in both the low back and the buttock region (Tables 3 and 4).
Of the 502 respondents, 475 (94%) PTs reported working full time (>3 hours per day); only 27 (5%) therapists reported working part time (<3 hours per day). Two hundred twenty-seven (45%) therapists reported patient contact less than 30 hours per week (Table 1). Respondents with more patient contact were found to have significantly higher severity of LBP (p < .05; Table 7).
Specialty and Severity of Work-Related LBP Among Responding Physical Therapists
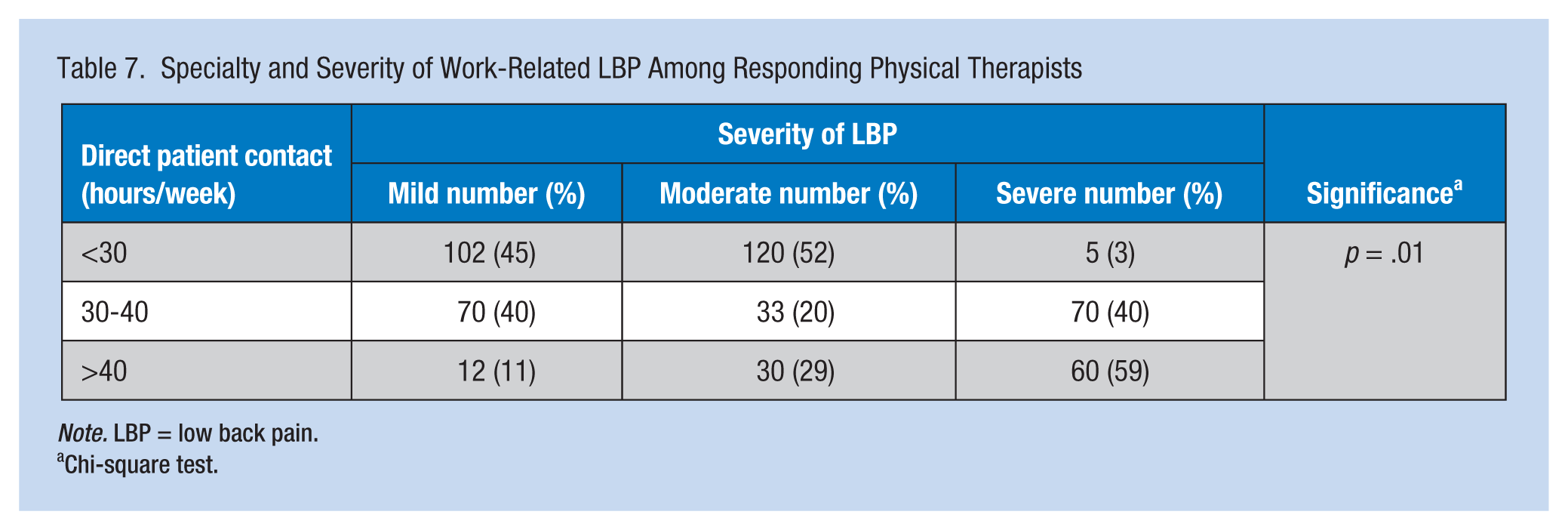
Note. LBP = low back pain.
Chi-square test.
Discussion
This study reported a prevalence of 89% for work-related LBP among PTs in the Riyadh region in Saudi Arabia. Among these, 39 % of PTs reported they were suffering from pain at the time of this survey. Study results show that gender, duration of contact with patients, and area of PT specialty were associated with LBP. Study findings are similar to other international surveys from New Delhi (Iqbal & Alghadir, 2015), Kuwait (Shehab et al., 2003), Great Britain (Scholey & Hair, 1989), Canada (Mierzejewski & Kumar, 1997), United States (Bork et al., 1996; Campo, Weiser, Koenig, & Nordin, 2008; Molumphy et al., 1985), Slovenia (Rugelj, 2003), and Turkey (Salik & Ozcan, 2004) that reported the incidence of work-related LBP among PTs between 29 % and 68 %.
Physical therapists are responsible for treating patients who have various types of pain; it is ironic to find that physical therapists suffer similar conditions. Higher prevalence of work-related LBP among PTs could be due to either extreme loads in the work setting or faulty musculoskeletal techniques used in treating patients (Poitras, Blais, Swaine, & Rossignol, 2005; Scholey & Hair, 1989). Physical therapists may overload their muscles and joints during treatment sessions (Iqbal & Alghadir, 2015) which increases the risk of developing disorders (Campo et al., 2008; Glover, McGregor, Sullivan, & Hague, 2005; Hoy, Brooks, Blyth, & Buchbinder, 2010; Poitras et al., 2005; Scholey & Hair, 1989; Shehab et al., 2003). Bent or twisted postures during patient transfers, and positioning and mobilization of joints are other factors reported to precipitate pain (Campo et al., 2008).
The majority of respondents in this study reported less than 5 years of work experience, and 85 % of respondents were less than 40 years of age (Table 1). This finding shows that respondents were newly qualified, just beginning their careers. From these study findings, it would appear that physical therapists are not following the principles of prevention and treatment of pain that they prescribe patients (Glover et al., 2005). Unfortunately, this problem can be expected to increase in the future as WMSDs are known to increase with age (Iqbal & Alghadir, 2015). Strategies must be developed to prevent WMSD in high-risk groups (Campo et al., 2008) such as physical therapists.
It was found that female therapists were at higher risk of developing LBP after joining the PT profession than male physical therapists. In addition, the majority of injured physical therapists reported specializing in neurology. Patients with neurological disorders are more dependent and require frequent lifting and transfers. Smaller body builds of females (heavier but shorter) compared to males (Table 1) is a disadvantage for women when lifting or transferring patients and using body force during treatment increasing spinal load leading to back pain (Bork et al., 1996; Shehab et al., 2003). Other health care professionals (e.g., nurses [Retsas & Pinikahana, 1999, 2000] and dentists [Alghadir, Zafar, & Iqbal, 2015; Shaik, Rao, Husain, & D’sa, 2011]) also reported LBP due to frequent patient handling, transfers and repositioning (Bork et al., 1996; Cromie, Robertson, & Best, 2000). The majority of patients admitted to hospitals are dependent and require significant care. Shortage of staff and patient load can increase workload and work-related stress (Kumar, 2007). Stress has also been associated with musculoskeletal pain (Fischer et al., 2015; Gil et al., 2004). About 24 % of the respondents have reported work-related injuries, the back being the most common site of injury. Another study by Glover et al. (2005) also reported low back injury to be the most common injury among PTs, forcing them to either seek treatment or reduce their daily physical activities.
As shown in previous studies, this study found that work-related LBP also affects non-work activities like shopping and household chores (Cromie et al., 2000; Cromie, Robertson, & Best, 2003; Vincent-Onabajo et al., 2016). This effect was more prevalent in those respondents who reported more patient contact each week. As a consequence, respondents were forced to seek sick leaves, decrease work hours and seek treatment from their colleagues. Unless and until therapists take care of themselves, they cannot care for patients (Iqbal & Alghadir, 2015). Distribution of workload according to individual capacity and personal health (Campo et al., 2008) could improve this situation.
Besides lower back, other parts of the body are also affected by work-related pain (Iqbal & Alghadir, 2015; Rossettini, Rondoni, Schiavetti, Tezza, & Testa, 2016; Salik & Ozcan, 2004); however, literature in this area is limited. Work-related pain can also be related to furniture in health care facilities (e.g., the use of revolving chairs and chairs without armrests). Height adjustable chairs with armrests and back support can prevent work-related pain (Rempel et al., 2006).
The next step is to devise primary as well as secondary prevention strategies to decrease the prevalence of work-related LBP, so that physical therapists can effectively care for their patients. Ergonomics including proper lifting techniques and the availability and convenience of using equipment should be emphasized. It has been previously proposed that ergonomics should be introduced as a separate course during physical therapists’ training (Iqbal & Alghadir, 2015) so that they can use their body force efficiently and effectively without putting any extra load on their bodies. Additional education should contribute to the prevention of work-related injuries as well as prevent consequent pain. Regular workshops and lectures on patient handling should be organized for physical therapists and other health care workers. Equipment such as slide boards, sit to stand frames, suspension frames, and height adjustable beds should be readily available for patient care. Facility administration must report LBP incidence rates (Al-Eisa & Al-Abbad, 2013) and then develop comprehensive safe patient handling and mobility programs to eliminate WMSD.
This study should be replicated in other parts of Saudi Arabia and among non-SPTA members. Also, a long-term study could investigate how therapists cope with chronic LBP. Other studies might avoid self-report questionnaires for which respondents may overestimate their experiences.
Conclusion
The prevalence of work-related LBP among physical therapists in the Riyadh region of Saudi Arabia affects patient care and therapists’ ADLs. Gender, PT specialty and duration of contact with patients were found to be associated with the development of work-related LBP. Clinicians should devise primary as well as secondary prevention strategies to treat therapists, so that they can effectively care for patients. Introducing ergonomics during the PT curriculum is essential so that therapists can learn to work efficiently and effectively. Also work-related stress reduction and teamwork could decrease the risk of WMSD.
Applying Research to Practice
Low back pain (LBP) is a common problem associated with health care professions. Studies on the prevalence of such work-related pain in various professions can provide a basis for formulating prevention strategies to prevent or minimize the risk of its development. Although physical therapists constitute the largest category of staff working in rehabilitation services in Saudi Arabia, no previous study has reported incidence and prevalence of such pain among them. The prevalence of work-related LBP among physical therapist in Riyadh was found to be high, affecting patient care and daily activities of the therapists. Clinicians must devise primary, as well as secondary, prevention strategies to minimize the risk of such development. Introducing ergonomics during the physical therapy curriculum, reduction of stress among therapists, and promotion of teamwork are essential so therapists can work efficiently and effectively.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was full financially supported by King Saud University, through Vice Deanship of Research Chairs, Rehabilitation Research Chair.
Author Biographies
Ahmad Alghadir is an associate professor and director of Rehabilitation Research Chair, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia.
Hamayun Zafar is an associate professor at Rehabilitation Research Chair, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia. He is also associated with Department of Odontology, Clinical Oral Physiology, Umea University, Umea, Sweden.
Zaheen A. Iqbal is a Researcher at Rehabilitation Research Chair, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia.
Einas Al-Eisa is an Associate Professor at Rehabilitation Research Chair, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia.