
Abstract
Breast milk is the ideal food for human infants, with benefits to mothers and babies. However, working mothers are more likely to choose not to breastfeed or to interrupt breastfeeding prematurely. This study assessed breastfeeding knowledge and attitudes among working mothers in South Jordan. Four hundred cross-sectional, self-administered Arabic surveys were distributed to working mothers at their workplaces. In addition to measuring mothers’ knowledge of and attitudes toward breastfeeding, barriers that prevented continuing breastfeeding beyond 6 months were also explored. Three hundred forty-four (80%) completed questionnaires were returned. The breastfeeding initiation rate was 72.4%, but only 20.9% were exclusively breastfeeding by 6 months. The participants showed satisfactory knowledge about breastfeeding and had positive attitudes toward breastfeeding. Most of the women who initiated breastfeeding reported ending breastfeeding prematurely. Approximately 30% of the mothers attributed premature cessation of breastfeeding to work. The results of this study could be useful for health care providers and policy makers when planning effective breastfeeding promotion programs and creating breastfeeding-friendly workplaces.
Keywords
Breast milk is the ideal food for human infants. Beyond the nutritional value, breastfeeding reduces infection susceptibility and neonatal mortality through active protection against infections (Renfrew et al., 2012). In addition, breastfeeding establishes a unique bond between mother and infant, which supports maternal role attainment (Ball, 2010; Labbok, Smith, & Taylor, 2008; Meyers, 2009). Women of childbearing age comprise a significant sector of the worldwide workforce. More than half of American, Canadian, and Australian mothers of children below the age of 3 years participate in the workforce (Baxter, 2008; Bureau of Labor Statistics, U.S. Department of Labor, 2006; Heymann & Kramer, 2009). In Jordan, women represent 48.5% of the population. Literacy rates are one of the highest in the region for both men and women, and among young adults. The higher education among women is responsible for higher employment rates among women (Majcher-Teleon & Slimène, 2009). However, because of non-supportive work environments and early return-to-work, working mothers around the world are less likely to breastfeed, or to stop breastfeeding prematurely (Centers for Disease Control and Prevention [CDC], 2008; Hendricks, Briefel, Novak, & Ziegler, 2006; Kimbro, 2006; Ryan, Zhou, & Arensberg, 2006).
Khassawneh, Khader, Amarin, and Alkafajei (2006) found that Jordanian employed mothers were less likely to fully breastfeed. Understanding work-related factors that lead to premature cessation of breastfeeding and then implementing breastfeeding-friendly policies in the workplace could significantly influence women’s abilities to successfully sustain breastfeeding. Supporting working mothers to continue breastfeeding has the potential to affect the health of mothers and children, employee retention and productivity, and cost savings to business and society (Bartick & Reinhold, 2010; Marinelli, Moren, Taylor, & The Academy of Breastfeeding Medicine, 2013). This study assessed working mothers’ breastfeeding knowledge and attitudes and explored barriers to continuing breastfeeding beyond 6 months, offering public health professionals information needed to promote breastfeeding in Jordan.
Method
The investigators randomly selected private and government organizations from all business sectors (e.g., health, banking, education) throughout the Al-Karak governorate. Facilities with similar work activities were selected randomly to participate. The investigators met mothers (those women who were unmarried or married without children were excluded from the study) at their workplaces.
An Arabic language questionnaire was developed by the researchers after reviewing multiple published questionnaires (Batal, Boulghourjian, Abdallah, & Afifi, 2006; Chaudhary, Shah, & Raja, 2011; Ekambaram, Vishnu Bhat, & Mohamed Asif Padiyath Ahamed, 2010; Saka, Musayeva, Ceylan, & Koeturk, 2005; Tarrant & Dodgson, 2007; Zhou, Younger, & Kearney, 2010). The first part of the questionnaire was a 14-item scale that measured breastfeeding knowledge. The questions were intended to assess mothers’ fundamental understanding of breastfeeding. Knowledge scores reflected correct and incorrect responses; the total number of correct responses was calculated and converted into a percentage score. The second part of the questionnaire was a 17-item scale to assess mothers’ attitudes toward breastfeeding. The arithmetic mean of the Likert-type scale (i.e., 5 = strongly agree, 4 = agree, 3 = I do not agree, 2 = strongly disagree, 1 = I do not know) was categorized as follows: ≥3.67 = high, 2.34-3.66 = medium, and ≤2.33 = low. For the purpose of calculating the percentage of responses, undetermined responses (i.e., I don’t know) were negligible (maximum of three responses) and considered disagree responses.
The Ethical Committee of the Faculty of Medicine at Mutah University approved the study. The mothers received written information about research aims and study methodology; those who agreed to participate in the study were given a questionnaire. Unlimited time was given to complete the questionnaire. Participants were allowed to take the questionnaire home and return it the next day; the research team was available to answer any questions. Returning completed questionnaires indicated that mothers consented to the information being used for study purposes. All research data were anonymous, encrypted, and saved, with limited access by the research team only.
Data were analyzed using the Statistical Package for Social Sciences, Version 17 (IBM, Armonk, NY, USA). Data are presented as the mean ± standard deviation (SD). Descriptive statistics were used to characterize the demographic data and knowledge and attitude scores. The descriptive data are presented as the proportion of respondents or the mean ± SD. Student’s t-test for independent groups (i.e., two-tailed) were used to compare the attitude scores of participants by education and previous breastfeeding experience. Statistical significance was set at p < .05.
Results
Four hundred questionnaires were distributed, and 344 questionnaires (80%) were completed and returned. Most of the study participants were 30 years old or younger (73.5%), college graduates (72.4%), and had three or fewer children (64%). Two hundred forty-five (71.2%) participants reported that they had attempted breastfeeding, but only 51 (20.9%) had exclusively breastfed during the first 6 months. Details of the sociodemographic characteristics of the participants are shown in Table 1.
Sociodemographic Characteristics of Participants (n = 344)
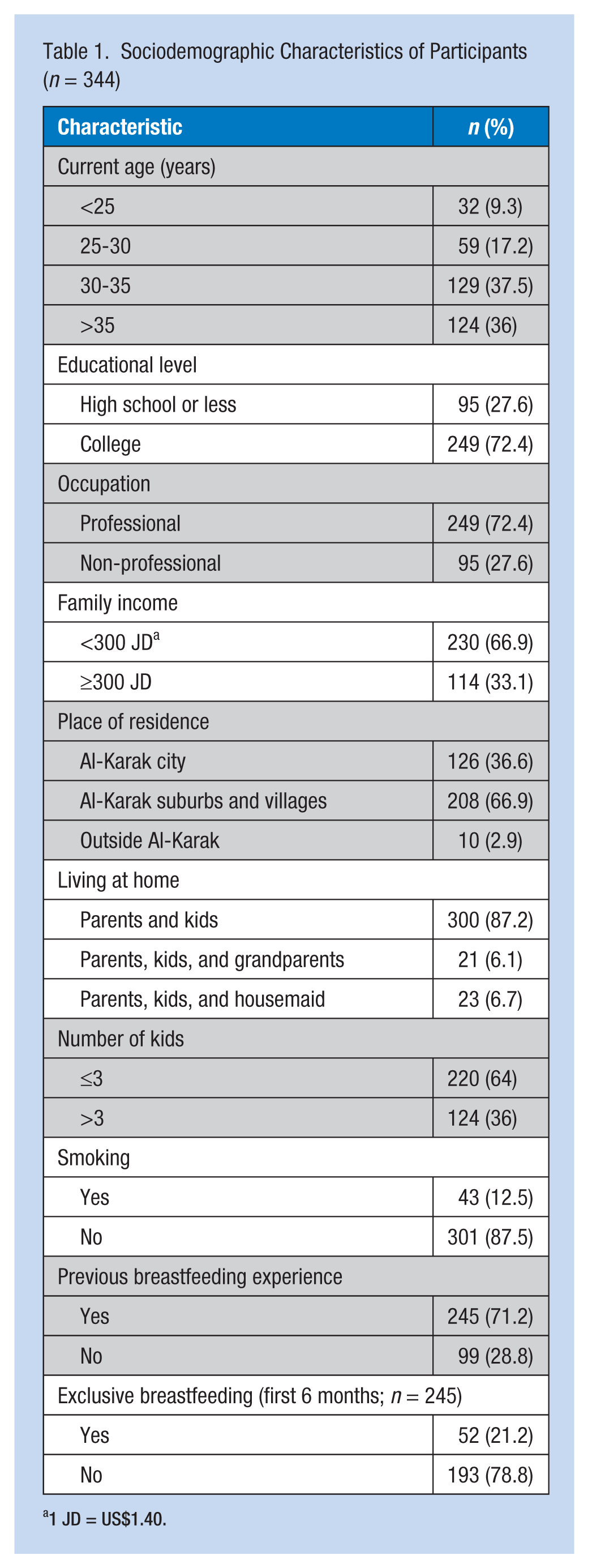
1 JD = US$1.40.
Working Mothers’ Breastfeeding Knowledge
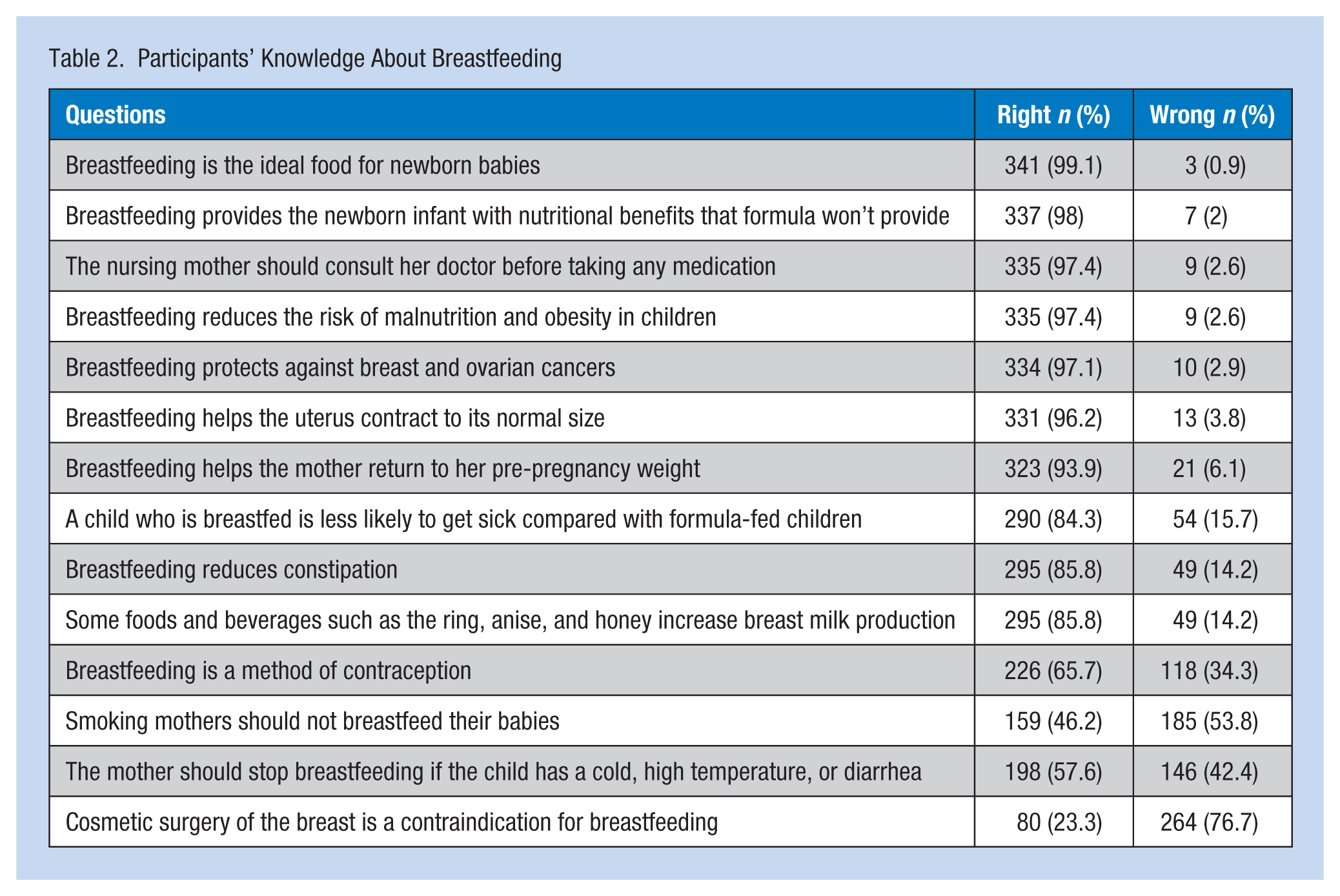
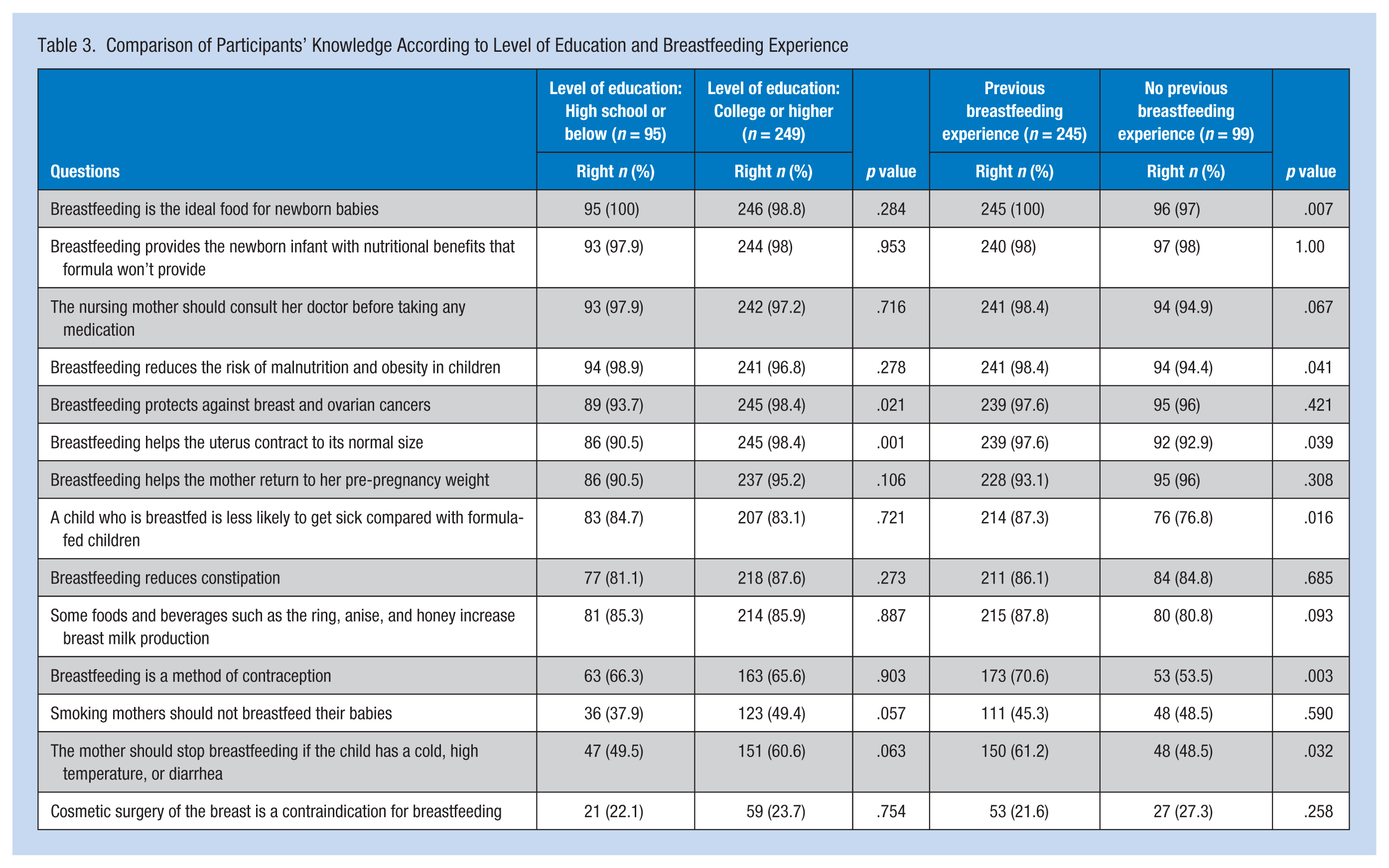
Most of the women in the study were knowledgeable about breastfeeding. Almost all the mothers (n = 341, 99.3%) knew that “breastfeeding is the ideal food for a newborn.” However, only 80 (23%) mothers responded to the statement “Cosmetic surgery of the breast is a contraindication for breastfeeding” correctly. College graduates and mothers with breastfeeding experience demonstrated more knowledge. “Breastfeeding helps the uterus contract to its normal size” was the only statement with statistical significance (p = .001 and p = .039, respectively). Table 2 shows the participants’ knowledge about breastfeeding. Table 3 compares mothers’ breastfeeding knowledge by mothers’ education and previous breastfeeding experience.
Participants’ Knowledge About Breastfeeding
Comparison of Participants’ Knowledge According to Level of Education and Breastfeeding Experience
Working Mothers’ Attitudes Toward Breastfeeding
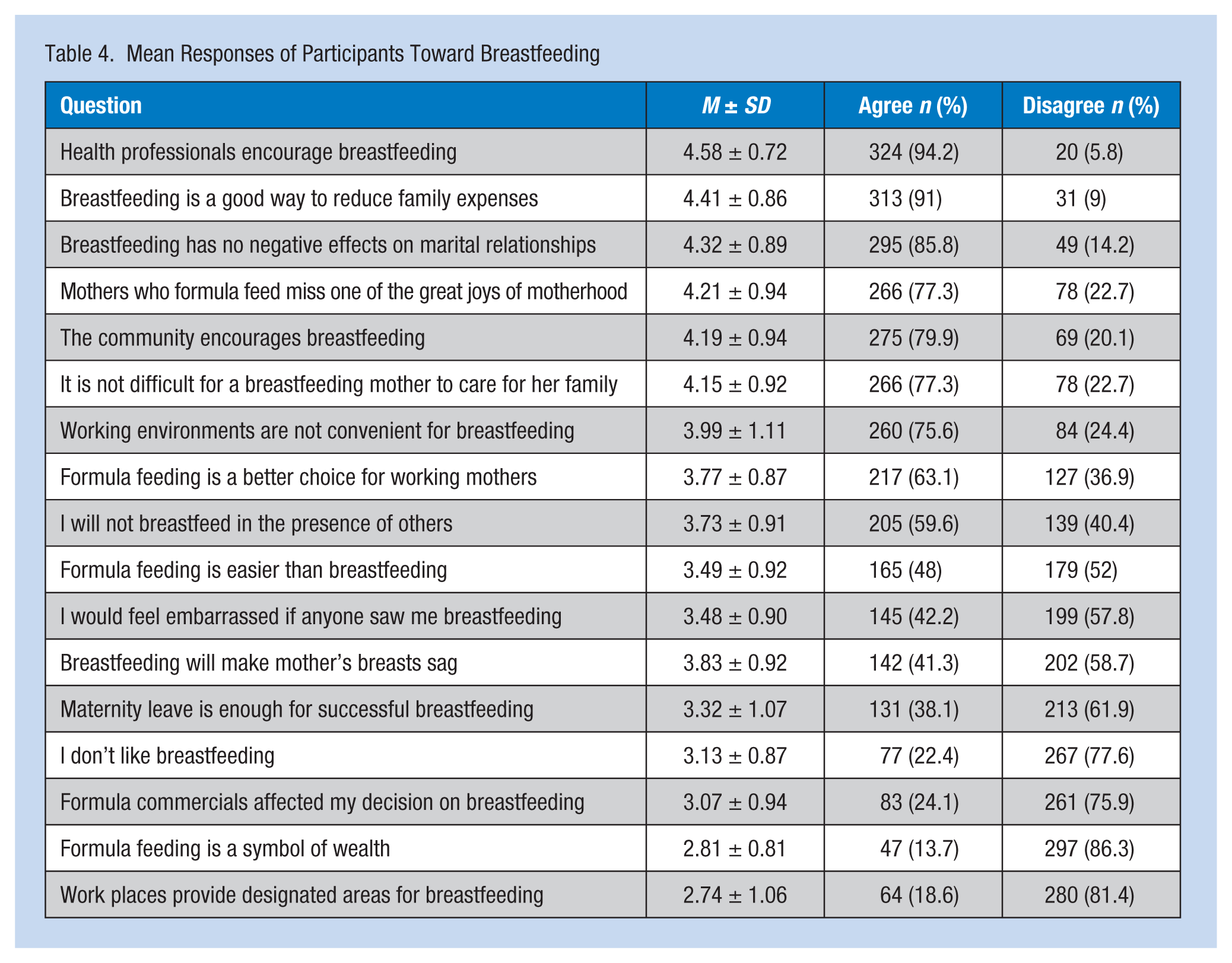
Working mother respondents demonstrated positive attitudes toward breastfeeding. The statement, “Health professionals encourage breastfeeding” had the highest agreement score (4.58 ± 0.72); the statement, “Workplaces provide designated areas for breastfeeding” had the lowest score (2.74 ± 1.06).
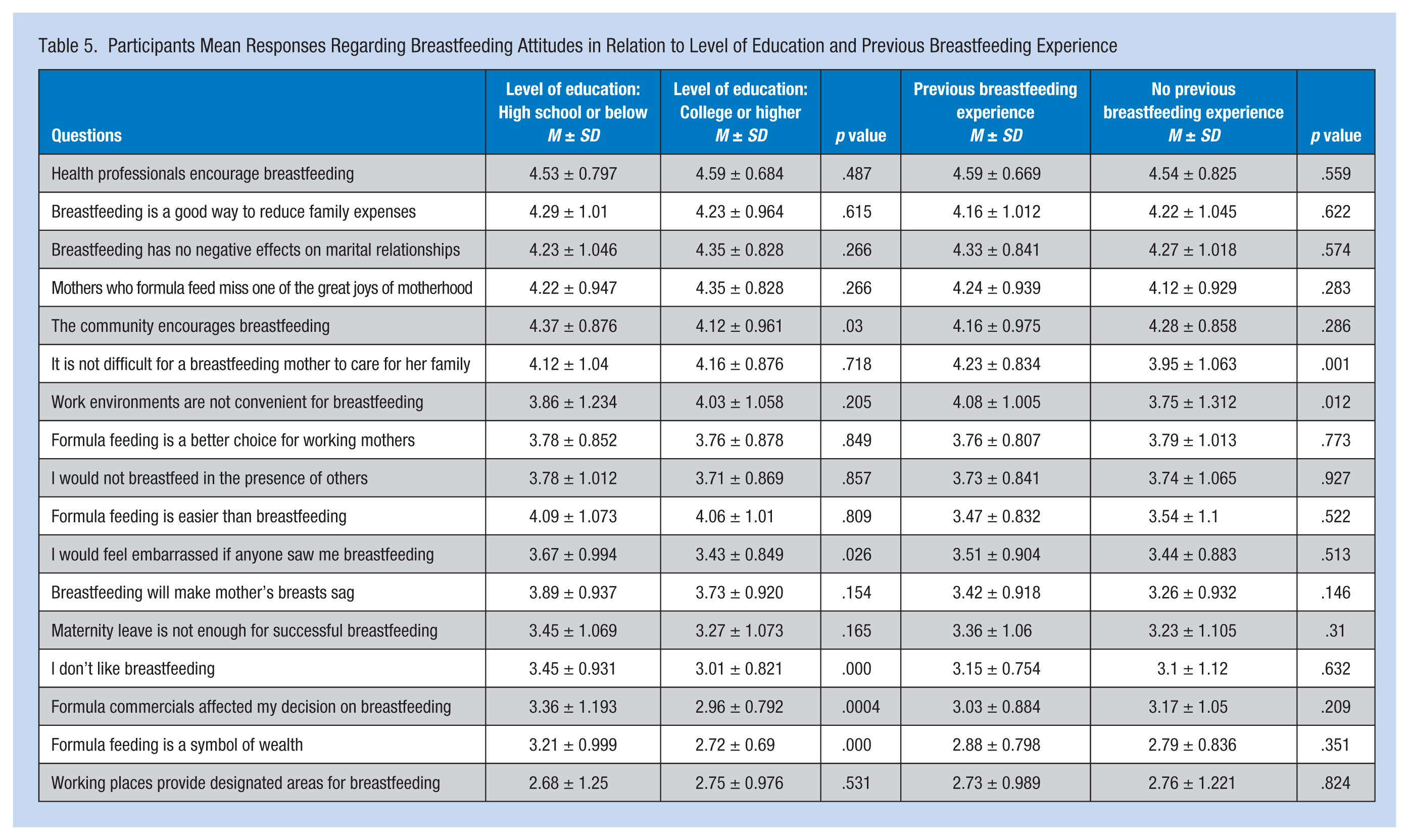
Mothers with less education believed that formula feeding was a symbol of wealth, were more affected by formula commercials, and even stated that they did not like breastfeeding. These results were statistically significant. However, mothers with previous breastfeeding experience reported that it was not difficult for breastfeeding mothers to care for their families, and they disagreed with inexperienced mothers who thought that work environments were not convenient for breastfeeding (p = .012). Table 4 shows the mean participant responses toward breastfeeding. Table 5 compares average responses by education and previous breastfeeding experience.
Mean Responses of Participants Toward Breastfeeding
Participants Mean Responses Regarding Breastfeeding Attitudes in Relation to Level of Education and Previous Breastfeeding Experience
Breastfeeding Barriers
Barriers to breastfeeding were defined in relation to maternal perception (e.g., forced to end breastfeeding although mother was still willing to breastfeed). Two hundred twenty-eight mothers reported they had ended breastfeeding prematurely. Approximately, one third of these mothers (n = 72, 31.6%) attributed early breastfeeding cessation to work issues (Figure 1). Only 64 (18.6%) respondents stated they had a designated area for breastfeeding at their workplaces (Table 4). In addition, 213 (61.9%) respondents believed that maternity leave alone was not long enough to establish successful breastfeeding (Table 4).
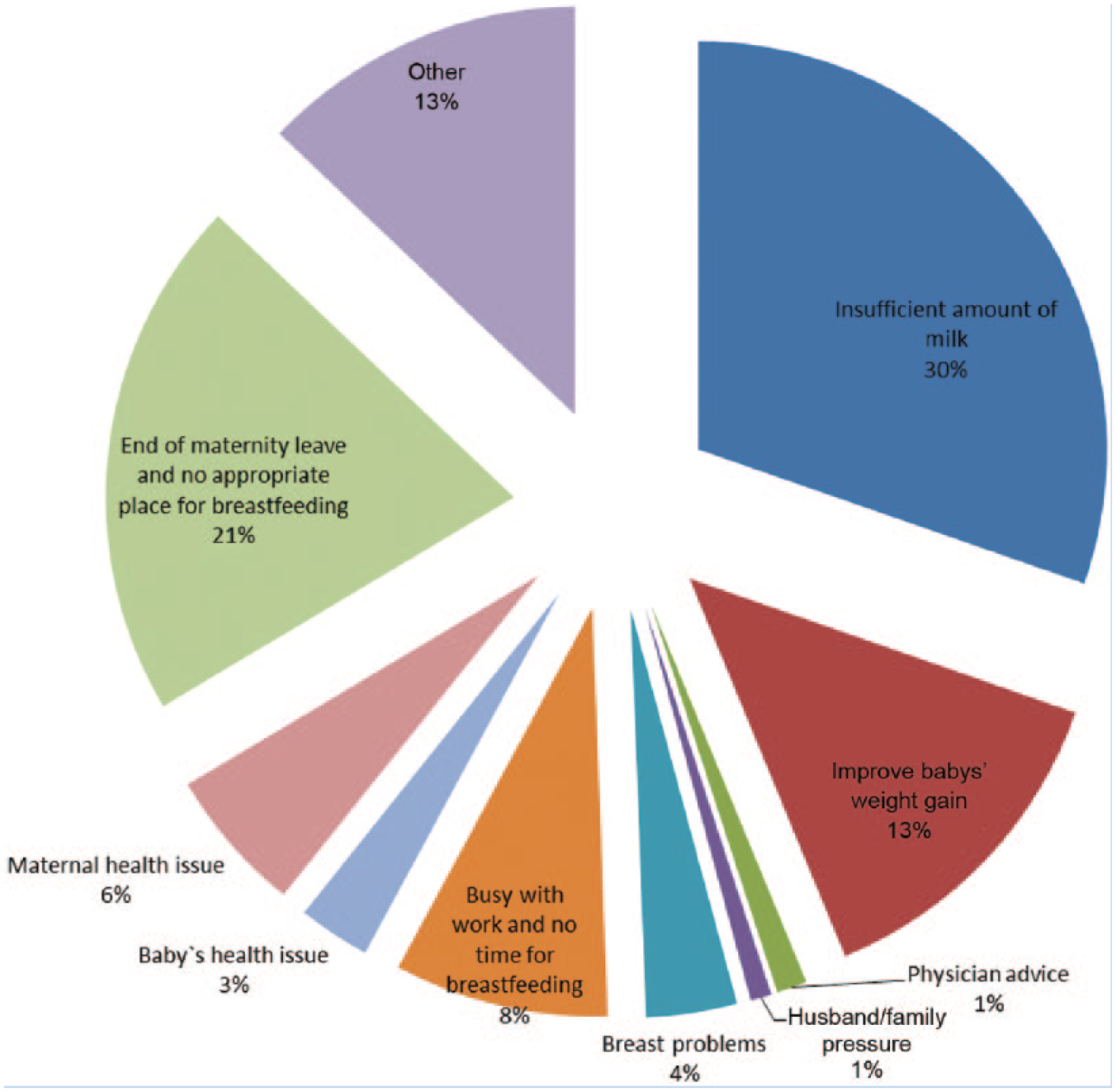
Causes of premature breastfeeding cessation (as perceived by the mothers).
Discussion
This study explored the knowledge of, attitudes toward, practices in relation to, and barriers to breastfeeding among working mothers in South Jordan. The study demonstrated that working mothers have satisfactory knowledge of and positive attitudes toward breastfeeding. However, only one fifth of breastfeeding working mothers breastfed exclusively for 6 months. For 30% of respondents, work-related factors were the cause of premature cessation. Mothers with previous breastfeeding experience were more likely to advise new mothers to breastfeed.
However, the study also identified knowledge deficits specifically related to breastfeeding contraindications. The mothers’ answers to questions about contraindications to breastfeeding showed that more than 40% of the respondents believed that mothers should stop breastfeeding when babies have colds, fevers, or diarrhea. Alternatively, more than 50% of the respondents thought that smoking and breast surgery were contraindications for breastfeeding. Therefore, accurate contraindications should be included in counseling about breastfeeding.
Although almost 80% of the respondents admitted that society encourages breastfeeding, approximately 60% of the respondents would not breastfeed in the presence of others and 42% would be embarrassed if they were seen breastfeeding. Embarrassment could be a cause of early breastfeeding cessation or to choose not to breastfeed at all. Jordanian culture discourages breastfeeding in public (Scott, Mostyn, & Greater Glasgow Breastfeeding Initiative Management Team, 2003; Tarrant, Dodgson, & Choi, 2004; Tarrant, Dodgson, & Tsang Fei, 2002). Therefore, providing a clean, private, and safe place for lactation (not a bathroom) with a handwashing facility in proximity to mothers’ work stations could improve breastfeeding adherence by encouraging mothers to pump as needed (Kimbro, 2006; Marinelli et al., 2013).
Working mothers are more likely to end breastfeeding prematurely compared with non-working mothers (CDC, 2008; Hendricks et al., 2006; Kimbro, 2006; Ogbuanu, Glover, Probst, Hussey, & Liu, 2011; Ryan et al., 2006). In this study, 93% of mothers who initiated breastfeeding reported they had prematurely ended breastfeeding and this study’s findings revealed that working mothers are less likely to practice exclusive breastfeeding, consistent with previous research (Ogbuanu, Glover, Probst, Liu, & Hussey, 2011; Skafida, 2011). The rate of exclusive breastfeeding until 6 months in this cohort was 20.9%, which is slightly higher than the percentage reported in the United States by Jones, Kogan, Singh, Dee, and Grummer-Strawn (2011). Although it is expected that mothers with higher education may fill positions with more work responsibilities, in this study, a higher percentage of mothers with higher education practiced exclusive breastfeeding which may be explained by more accurate knowledge and understanding of the benefits of exclusive breastfeeding than mothers with less education. These results were consistent with previous reports that mothers in the highest categories of academic skills were more likely to initiate exclusive breastfeeding (Webb, Sellen, Ramakrishnan, & Martorell, 2009).
Adopting new policies to encourage exclusive breastfeeding is needed. Previous studies have shown that “breastfeeding friendly” work environments as well as part-time employment for breastfeeding mothers enable them to continue breastfeeding for longer periods of time (Ogbuanu, Glover, Probst, Liu, et al., 2011; Skafida, 2011). Laws to improve breastfeeding, including extended paid maternity leave, breastfeeding breaks, and onsite child care facilities, support working mothers. In Jordan, maternity leave by law is 10 weeks. The majority of study respondents (61%) reported that maternity leave should be longer, and only 18.6% had a daycare facility at their place of work.
Mothers who reported previous breastfeeding experience had more accurate knowledge about breastfeeding and were not as sensitive to breastfeeding barriers, which are consistent with previous reports (Uchendu, Ikefuna, & Emodi, 2009). These results highlight the need for working mothers with previous breastfeeding experience to advocate for breastfeeding. They can serve as role models for new mothers by sharing their stories, including the obstacles they encountered and how they achieved breastfeeding success.
More than 80% of working mothers returned completed questionnaires. This high response rate might be related to the education of participating mothers, working mothers’ desire to have their voices heard, or the researchers personally distributing and retrieving the questionnaires.
The main limitation of this study is that it was focused on South Jordan and the results cannot be generalized to the entire country. In South Jordan, most businesses are small to medium size. Labor laws ask businesses with 20 or more women employees to maintain a safe child care facility under the supervision of a qualified nursemaid for children less than 4 years of age, provided that there are 10 or more children. A limited number of facilities in this area fulfill these criteria.
In this study, the time between last delivery and answering the questionnaire was not recorded. However, the researchers know that this time interval differed among the respondents. Recall bias of the respondents should be addressed in a larger study.
Implications for Occupational Health Nurses
Occupational health nurses focus on promotion and restoration of health, prevention of illness and injury, and protection from work-related and environmental hazards (Explorehealthcareers.org, 2012). Non-initiation or early cessation of breastfeeding due to maternal work issues could be viewed as a health hazard. The effects of never breastfeeding or prematurely ending breastfeeding on maternal and child health and child cognitive development are now well established and include an increase in the incidence of illness and significant health-related costs (Bartick & Reinhold, 2010; Renfrew et al., 2012). This study provides evidence of the effect of maternal work on breastfeeding. Occupational health nurses can work with breastfeeding mothers to provide the best workplace environments for these workers.
Conclusion
This is the first study in South Jordan to assess the knowledge of, attitudes toward, and practices in regard to breastfeeding by working mothers. Breastfeeding knowledge among participants was adequate and their attitudes toward breastfeeding were positive in general. Work-related causes were responsible for premature cessation of breastfeeding in approximately 30% of participants. This study provided direction for health care professionals and policy makers for planning effective breastfeeding promotion programs and creating breastfeeding-friendly work environments.
Applying Research to Practice
The findings of this study suggest that further strategies should be implemented to improve rates of breastfeeding among working mothers. Longer paid maternity leaves and providing appropriate place for breastfeeding at the workplace will significantly improve breastfeeding rates. It is expected this will hugely affect the health of children, mothers, and communities.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Eyad Altamimi is a pediatric gastroenterologist and an associate professor of pediatrics. His research interest includes childhood nutrition and malnutrition prevention.
Reem Al Nsour is a graduate of Medical School at Mutah University. She is a senior radiology resident with interest in female medical imaging.
Duaa Al dalaen is an obstetrics and gynecology resident. She participates in campaigns promoting breastfeeding and maternal and child health.
Neyaf AlMajali is a senior general surgery resident. Her research interest focuses on research methodology and disease epidemiology.