
Abstract
As frontline clinicians, occupational and environmental health nurses play an important role in educating workers and the public about the dangers and toxic effects of environmental contaminants. One of these contaminants is methylmercury, which enters the body through the consumption of contaminated fish and seafood. Methylmercury affects the central nervous system where it may cause psychiatric disturbances, ataxia, neuropathy, and visual and hearing loss. Because their central nervous systems are rapidly developing, the most vulnerable subgroups are infants in utero, babies, and young children. Pregnant women and nursing mothers can directly expose their infants because methylmercury passes through the placenta to the infant and is also present in breast milk. The purpose of this article is to provide an overview for occupational and environmental health nurses and other health care practitioners about the causes and consequences of methylmercury exposure in women of childbearing age and children so that they can better educate workers about this environmental contaminant.
Keywords
Imagine being an occupational health nurse for a seafood processing company that employs a large and diverse workforce in a coastal area. The volume of fish being processed by the company has decreased due to numerous fish kills in the area. At the same time, workers have presented to the occupational health clinic with a variety of symptoms including numbness, paresthesias of extremities, dysarthria, ataxia, and hearing and sight impairments. Young pregnant women are giving birth to babies with low birth weights and neurological problems. Could these environmental and health issues be related? Upon further investigation, the nurse learns that affected individuals appear to eat more fish than unaffected workers, and affected workers have elevated concentrations of methylmercury (MeHg) in their systems. These findings were true of Minamata Bay, Japan, after World War II (Harada, 1994, 1995), and they illustrate the severity of the problem—one that occupational, environmental, and public health nurses should be aware of today.
Mercury is a highly toxic element that occurs naturally in the earth’s crust and poses significant risks to human health. It can be found in three forms: (a) elemental, (b) organic, and (c) inorganic salts (Olson, 2013). Several products illustrate the beneficial uses of mercury including thermometers, switches, batteries, and light bulbs (Olson, 2013; U.S. Environmental Protection Agency [U.S. EPA], 2015). Due to the demand for these products, the amount of mercury cycling through the environment has increased over the past several decades (Krabbenhoft & Rickert, 2013). Organic MeHg is the most toxic of all forms and presents the greatest concern to the general public (Olson, 2013).
Methylmercury is primarily found in aquatic ecosystems and accumulates in fish. Consumption of contaminated fish is the main pathway of exposure to mercury by humans (Mergler, Anderson, Chan, & Mahaffey, 2007), making exposure an avoidable, behavioral decision. Individuals who consume fish should be aware of the hazards associated with eating contaminated fish, especially if they are frequent consumers.
Mercury primarily affects the central nervous system processes (Myers & Davidson, 1998). Women of childbearing age and parents of young children should be especially aware of MeHg toxicity so their dietary choices do not unduly expose their families to this toxic heavy metal. The worksite is an optimal venue to educate workers about MeHg toxicity and its impact on human health. Occupational and environmental health nurses can educate workers about the risks and consequences of MeHg as well as how to avoid exposures.
The purpose of this article is to provide an overview of the etiology, risks, and consequences of MeHg exposures, especially for women of childbearing age and children, so occupational health nurses can educate and empower workers to make appropriate dietary choices, reducing exposure to MeHg. Throughout this article, the term “fish” refers to freshwater fish, saltwater fish, and seafood.
Methylmercury
Methylmercury concentrates in aquatic systems when elemental and inorganic mercury, primarily from atmospheric sources, accumulates. Atmospheric mercury can be from either natural (e.g., volcanoes) or anthropogenic (e.g., burning fossil fuels) sources. Atmospheric mercury accumulates in the sediments of aquatic systems after it falls to earth in rain or snow. Mercury can also accumulate in sediment from industrial effluents (Harada, 1994). Once in sediment, bacteria convert mercury to organic MeHg (U.S. EPA, 2015).
Methylmercury enters the food chain when it is assimilated by plants and microscopic aquatic animals which are then consumed by larger animals and fish. Unlike other contaminants that bind to fatty tissues, MeHg binds to proteins and free amino acids in the muscles of fish and other aquatic animals where it remains bound and accumulates over time (Mergler et al., 2007). This process of bioaccumulation results in mercury concentrations being the highest in older and larger predator fish. Because MeHg concentrates in muscle, it is not removed by cleaning or cooking (Olson, 2013).
As part of the National Health and Nutrition Examination Survey from 2003 to 2006, total blood mercury concentrations were measured for more than 16,000 people aged 1 year to more than 70 years (Caldwell, Mortensen, Jones, Caudill, & Osterloh, 2009). Children from ages 1 to 5 had the lowest mercury levels at approximately 0.3 µg/l. Levels increased with age to the 40s and 50s, and then declined (U.S. EPA, 2013a). Across all age groups, males and females had similar total blood mercury levels (i.e., 0.839 and 0.822 µg/l, respectively).
Among women of childbearing age (16 to 49 years), total mercury in blood was highly correlated with MeHg in blood, and both were consistently low. Geometric mean levels ranged from 1.39 to 1.98 µg/l from 1999 to 2010 (U.S. EPA, 2013a). Annually, the proportion of women who exceeded the level of concern (5.8 µg/l) was low, ranging from 1.7% to 6.8% (Mahaffey, Clickner, & Jeffries, 2009). Significant positive dose-response relationship between three variables (i.e., frequency of fish consumed, amount of fish consumed per meal, and total mercury consumed) and blood mercury levels were documented (Schober et al., 2003; U.S. EPA, 2013a).
Ethnic differences in fish consumption also affected blood mercury levels (Caldwell et al., 2009; Mahaffey et al., 2009; U.S. EPA, 2013a). A group identified as “other” which included Asian, Pacific islanders, American Indians, and Alaskan natives ate fish more frequently than other groups and had higher blood mercury levels than Hispanics, non-Hispanic Whites, and non-Hispanic Blacks. Factors other than frequency of fish consumption that affected mercury levels were portion size and type of fish consumed. Caldwell et al. (2009) found that non-Hispanic Black women had higher total blood mercury (1.081 µg/l) than non-Hispanic White (0.85 µg/l) and Mexican American women (0.70 µg/l), but they attributed much of this to genetic differences which resulted in less elimination of mercury from the body. Although Mexican American women ate more fish per meal, they ate it less frequently resulting in lower mercury intake and lower levels in blood (U.S. EPA, 2013a).
In the United States, other factors related to blood mercury levels were region of the country and economic status (Mahaffey et al., 2009). Blood mercury concentrations were highest among individuals in the Northeast, followed by the South and West; the Midwest had the lowest concentration. In addition to these regional trends, blood mercury levels were the highest along coastal areas where upto 17% of women exceeded the level of concern (5.8 µg/l). Fish consumption and blood mercury levels also increased with household income (Mahaffey et al., 2009).
Etiology of Methylmercury
Although elemental and inorganic mercury enter the body primarily through vapor inhalation and absorption through the skin, MeHg enters the body only through ingestion (Olson, 2013). Once ingested, about 90% of MeHg is absorbed from the gut into the bloodstream where it is distributed throughout the body and readily crosses the blood-brain barrier, affecting the central nervous system (Clarkson, 1995; Myers & Davidson, 1998; Olson, 2013).
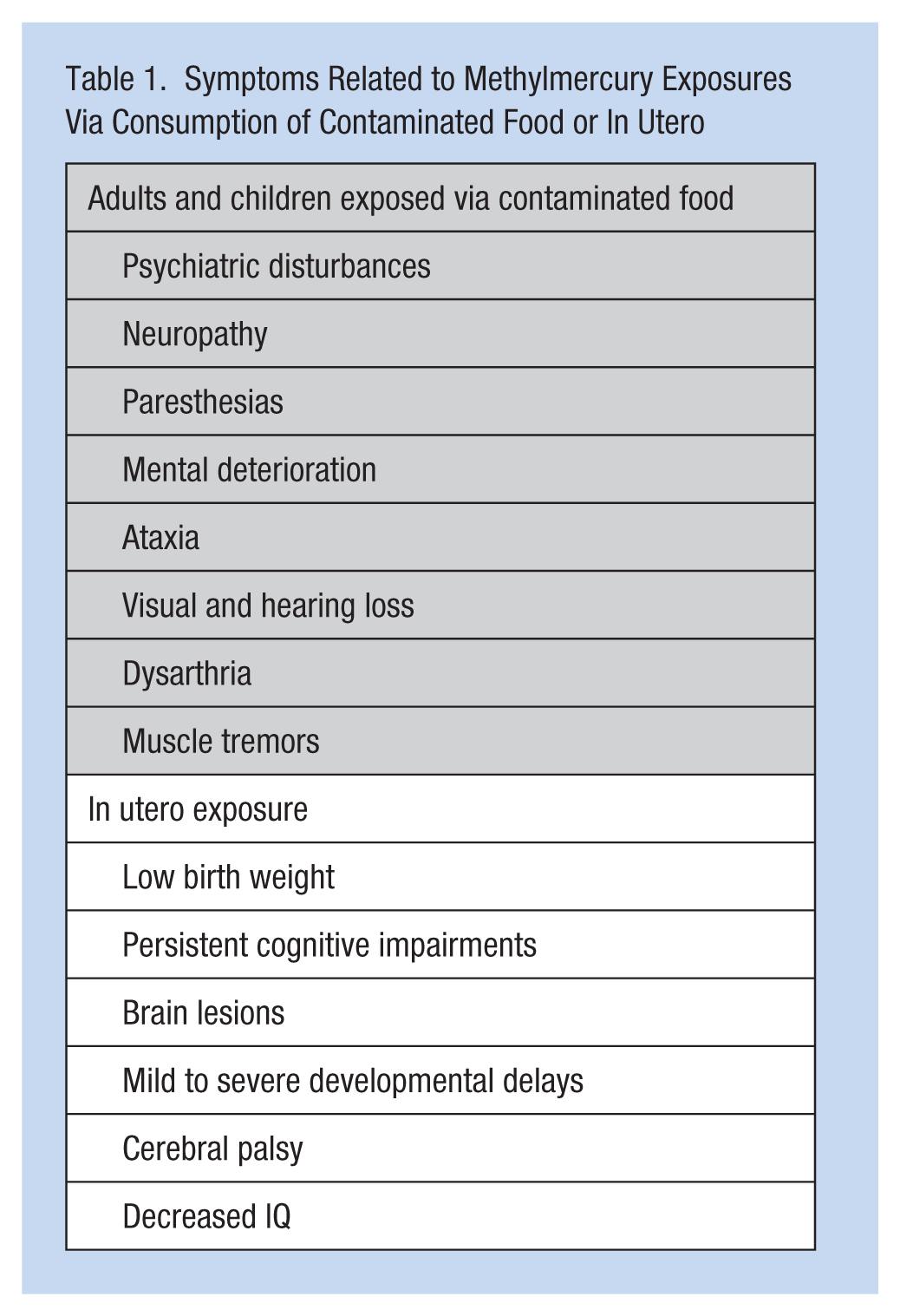
In adults and children, MeHg toxicity can cause psychiatric disturbances, ataxia, neuropathy, and visual and hearing loss. Additional symptoms may be paresthesias, dysarthria, mental deterioration, and muscle tremors. Extreme exposures may cause paralysis or death. None of these physical symptoms are pathognomonic for MeHg, and nurses who encounter workers exhibiting these symptoms should question them about symptoms and dietary choices such as fish consumption and frequency (Clarkson, 1995; Myers & Davidson, 1998; Olson, 2013).
The fetal brain is more susceptible to MeHg than the adult brain (Olson, 2013). Methylmercury in the mother’s blood readily crosses the placenta and enters the fetal blood, where it has a high affinity for hemoglobin. Levels of MeHg in fetal blood have been found to be higher than in mother’s blood (Myers & Davidson, 1998), causing diffuse and widespread neuronal atrophy, disruption of processes such as neuronal migration, and organization of gray matter. Results of these disruptions in utero can include teratogenic effects in the embryo, intrauterine hypoxia, premature death, and abortion (Olson, 2013).
In addition to symptoms also exhibited by adults, babies and young children exposed to MeHg in utero may experience low birth weight, mild to severe developmental delays, persistent cognitive impairments, cerebral palsy, brain lesions, and decreased IQ (Association of Reproductive Health Professionals [ARHP], 2008, 2010; Caldwell et al., 2009; Myers & Davidson, 1998; Olson, 2013). The severity and persistence of symptoms when individuals were exposed to MeHg in utero have been variable. Some studies found only slight or no developmental delays in children who were exposed in utero (Myers & Davidson, 1998). Conversely, the ARHP (2008) and Murata, Weihe, Budtz-Jorgensen, and Grandjean (2004) found prenatal exposure could cause health outcomes that persist into adolescence. Frequently, these outcomes include subtle deficiencies in motor skills. Spontaneous abortion or intellectual disability can occur in rare cases, even when mothers exhibit no symptoms of MeHg toxicity (Olson, 2013).
Risk Assessment
Risk assessment is used to determine the probability of a health risk associated with a toxicant exposure (Sy & Long-Marin, 2012). One component of risk assessment is to determine how a toxicant enters the body and how much of it enters from contaminated sources. Because the primary entry of MeHg is ingestion of fish, risk assessment has been used to establish reference doses (RfD) and fish consumption advisories throughout the United States. These advisories are based on the concentrations of MeHg found in various fish species as determined from periodic sampling and monitoring. The U.S. EPA (2015) has established a daily exposure limit or RfD that is unlikely to cause harmful effects throughout a lifetime. For humans, the RfD is based upon the amount of mercury an infant in utero can be exposed to because this is the life stage that is most vulnerable to the toxic effects of MeHg. Determining an RfD is a stepwise process of calculating a benchmark dose ascertained from existing studies and applying uncertainties based on professional toxicologic or epidemiologic judgment. These uncertainties include individual variability, duration of studies that were used, extrapolation errors, and database quality, all of which result in a conservative determination of the RfD. With this approach, Rice, Swartout, Mahaffey, and Schoeny (2000) calculated an RfD for humans to be 0.1 µg of mercury consumed per kilogram of body weight per day (µg/kg per day). This value was reexamined and confirmed by the U.S. EPA (2012) after more studies were completed and included in the analysis.
The RfD was used by the National Research Council to recommend minimum fetal blood mercury levels (Mahaffey et al., 2009; Schober et al., 2003; U.S. EPA, 2013a) and establish levels for risk assessment. The RfD of 0.1 µg/kg per day corresponds to mercury levels of 3.5 µg/l and 5.8 µg/l in pregnant mothers and fetal blood, respectively. Therefore, MeHg levels of 3.5 µg/l and 5.8 µg/l have frequently been used as index levels of concern for maternal and fetal blood, with 5.8 µg/l as the level of concern for children and other adults.
The U.S. Food and Drug Administration (FDA) in conjunction with U.S. EPA and appropriate state departments of conservation, natural resources, and health are the main entities that collaborate to develop and publish fish consumption advisories. Using the U.S. EPA’s recommended RfD and the MeHg concentrations found in each fish species, the amount of fish that can safely be consumed over a given time (e.g., do not consume, one meal per week, one meal per month) is calculated. Consumption advisories may vary by region or even water body; therefore, guidelines for specific waters should be checked to see which species are safe and which ones are listed under advisories (Bahnick, Sauer, Butterworth, & Kuehl, 1994).
Although virtually no level of fish consumption is without risk for MeHg exposure, definite health benefits of eating fish can exceed potential risks (Johnston & Snow, 2007). Fish are low in saturated fat and high in omega-3 fatty acids, which are important for brain development. They are also high in vitamins A, B, and D as well as some minerals. Pregnant women should consider fish in their diets because of the benefits provided during gestation (ARHP, 2008). Ginsberg and Toal (2009) quantified the risks of MeHg exposure versus the benefits of omega-3 fatty acids when including fish in the diet. They developed a sliding scale of relative risk by calculating risk-benefit based on MeHg and omega-3 fatty acid concentrations for each species. Risks exceeded benefits for species that were extremely high in MeHg, even though some were also high in omega-3 (e.g., shark and swordfish). However, benefits greatly exceeded risks in some fish such as trout, herring, and Atlantic salmon (American Academy of Pediatrics [AAP], 2012; Oken et al., 2012).
Although infants can consume MeHg through their mothers’ breast milk, the benefits of breastfeeding can also exceed the risks (Grandjean, Weihe, & White, 1995). Breastfeeding imparts a definite health advantage to infants over those who are formula-fed. The protective effects of breastfeeding include lower rates of respiratory and gastrointestinal infections (AAP, 2012). The maternal consumption of one to two portions (4-8 ounces) of fish (i.e., salmon, canned light tuna, or herring) per week benefits neurological and cognitive development of fetuses and neonates (AAP, 2012; Oken et al., 2012; Perinatal Nutrition Working Group [PNWG], 2012). The fish contain docosahexaenoic acid (DHA), an essential nutrient promoting cognitive development and normal birth weight and gestational length (PNWG, 2012).
Occupational and environmental health nurses may suspect MeHg toxicity in workers who exhibit symptoms previously listed (Table 1). Because no physical symptoms are pathognomonic for MeHg toxicity, further evaluations should be used to confirm the diagnoses. If MeHg is suspected, workers should be questioned about potential contacts with mercury to identify possible causes (e.g., occupational, accidental, or dietary choices). A definitive diagnosis requires blood, urine, and tissue analysis for the presence of mercury (Olson, 2013).
Symptoms Related to Methylmercury Exposures Via Consumption of Contaminated Food or In Utero
Nursing Implications
Occupational and environmental nurses play an important role in educating workers about the dangers of MeHg toxicity, particularly educating women who are pregnant or planning to become pregnant, and parents of young children. The process of educating these workers about the risks, benefits, and healthy choices of fish consumption is called risk communication (Sy & Long-Marin, 2012). Although the goal of effective risk communication is to provide workers with necessary information to empower them to make healthy choices, the process essentially has two steps: (a) educating the educators (e.g., occupational health and environmental health nurses and other clinicians) and (b) educating women workers of childbearing age and working parents. Because the second step cannot be achieved without accomplishing the first step, it is essential that occupational health nurses are prepared to share accurate MeHg information with workers (e.g., Anderko, 2009; Callejo & Geer, 2012; Olson, 2013).
Educating the Educators
Educating the educators about MeHg levels in fish and associated consumption advisories is only one part of this phase. Understanding factors such as risk-benefit, regional trends of fish consumption, ethnic differences, and individual lifestyle choices can determine which workers are at highest risk of adverse effects. Although eating fish is a behavioral choice, many factors influence that choice, including economics (e.g., subsistence anglers), culture, availability of fish, and health benefits. Knowing why workers “choose” to consume fish can inform behavioral strategies to reduce risks of MeHg exposure. In addition, nurses should learn to access resources that provide current information to professionals (e.g., state and local agency consumption advisories) and offer informational materials to workers (e.g., brochures, videos). Anderko (2009) developed an educational module for nurses consisting of four short videos and a workbook covering a variety of topics related to risk communication and other aspects of MeHg toxicity, particularly for vulnerable subgroups. The ARHP (2008, 2010) offered online workbooks with information that nurses can use to counsel and educate vulnerable subgroups concerning MeHg exposure and lifestyle choices that can minimize exposures.
Educating the Public
Educating the public encourages occupational and environmental health nurses to provide both worksite and public education either through individual, routine health care services, or worksite programs. Individual interactions could include determining whether workers (or their families) consume fish or are likely to consume fish. The next steps could be determining whether workers are aware of the risks associated with consuming fish high in MeHg and providing information about these risks and how to avoid them. For example, Anderko (2009) developed a diet survey to identify the frequency, quantity, and types of fish consumed. This approach enables nurses and workers to determine how to best reduce exposures.
Worksite and community-based programs can disseminate information, reaching larger, more diverse groups. Environmental health nurses working with public health units are likely to develop and implement these programs. Callejo and Geer (2012) identified four ways through which communities can be made aware of in utero MeHg exposure: (a) clinical integration (e.g., providers communicate the message in routine care), (b) community integration (e.g., organizations promote the message to the public), (c) media coverage and dissemination, and (d) message persistence (e.g., continuous exposure via media outlets). Delivering the message involves the collaboration of many constituents within the community including health care providers, applicable government agencies, community leaders, and media outlets. Examples of how community-based programs might be designed and implemented are reported by Callejo and Geer (2012) for Brooklyn, New York, and by Derrick, Miller, and Andrews (2008) for subsistence anglers in a Georgia community.
The method of delivery is an important consideration in worksite and community-based programs. For instance, Burger et al. (2003) found that a classroom presentation was more effective than simply using a brochure, and Connelly and Knuth (1998) found that using a persuasive tone when presenting information on fish advisories was more effective than using a commanding tone. Also, presenting actual contaminant levels in fish and using clear, understandable terminology about advisories lead to better understanding and compliance in California (Tan, Ujihara, Kent, & Hendrickson, 2011). These examples illustrate that knowing the target audience is necessary when developing effective worksite and community-based programs, and can also direct occupational and environmental health nurses when they provide routine care for workers.
Fish that are generally high in MeHg and should only be consumed once per month or should be avoided by pregnant women, women who expect to become pregnant, and children include king mackerel, several species of sharks, swordfish, Gulf of Mexico tilefish, and albacore tuna (ARHP, 2008, 2010; U.S. EPA, 2013b). Some examples of fish low in MeHg include shrimp, canned light tuna, catfish, salmon, several sunfish species, and tilapia (ARHP, 2008). Even though these species may have no consumption restrictions, pregnant women, women who plan to become pregnant, and young children should limit consumption to two three-ounce meals per week (U.S. EPA, 2004).
Summary
The health of workers and community members is predicated on reliable information and guidance about the safe consumption of fish. Occupational and environmental health nurses can promote the health and safety of workers by disseminating this information through health and wellness programs. These programs should focus on causes, risks, and effects of excessive intake of MeHg, especially among women who are pregnant or of childbearing age, and young children. Prevention of MeHg toxicity primarily targets dietary fish choices; therefore, education should be the main component of a primary prevention program. Occupational and environmental health nurses can also provide education about the necessary average daily intake of omega-3 polyunsaturated fatty acids (DHA) in nursing mothers’ diets. In addition, counseling should be provided to women of childbearing age about the recommended fish species to eat (e.g., salmon, shrimp, or catfish) and the avoidance of MeHg-laden fish (e.g., swordfish, marlin, mackerel, or tilefish). Nurses can play a significant role in advocating for legislation to reduce or eliminate sources of MeHg contaminants in fish. The PNWG (2012) has developed nutritional recommendations for seafood consumption by breastfeeding, pregnant, and childbearing age women.
Ongoing research into the risks and benefits of seafood consumption for breastfeeding, pregnant, or childbearing age women should be a priority. The nurse can participate in interprofessional collaborative research on MeHg exposures and health effects. Furthermore, educating nurses about the health benefits and risks associated with fish consumption, particularly in relation to MeHg toxicity, should be a priority.
In Summary
Methylmercury is a highly toxic heavy metal that enters the body through the consumption of contaminated fish and seafood.
Unborn and young children are especially vulnerable.
Occupational and environmental nurses play an important role by educating workers and the public about the hazards of methylmercury and how to avoid it.
However, many nurses need to first be educated about methylmercury because they are not familiar enough with the issue to properly counsel workers.
Pregnant women, women who plan to become pregnant, and parents of young children should be primary recipients of educational programs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
N. Elizabeth Colvin has an MS in fisheries biology from the University of Arkansas at Pine Bluff and a BSN in nursing from Armstrong State University, Savannah, Georgia. She is currently employed as a registered nurse at Memorial University Medical Center in Savannah, Georgia, and is working towards a DNP degree from Augusta State University.
Pamela Lynn Mahan, PhD, RN, is an associate professor of nursing at Armstrong State University School of Nursing. She has more than 25 years’ experience in higher education with educating and mentoring undergraduate and graduate nursing students in the classroom and clinical environment. Her teaching expertise encompasses epidemiology, public and community health, health promotion, and nursing theory.
Jeffrey Harris, MSN, RN, CNS, is a senior lecturer at the School of Nursing, Armstrong State University.