
Abstract
This article examines dialectical tensions in the health narratives of participants of the Employee Wellness Program (EWP) of a large public university in the southeastern United States. Semi-structured interviews (n = 12) with team leaders in the program indicated that health is a multifaceted concept characterized by three pairs of dialectical tensions: autonomy versus connection, private versus public, and control versus lack of control. These findings suggest that to better promote health and wellness in the workplace, EWP staff should consider employees’ unique experiences and beliefs about health when designing organization-wide programs and campaigns.
Today, many employers offer Employee Wellness Programs (EWPs) to manage their rising health care costs. Such programs are designed to increase work productivity and decrease absenteeism (Brown, 1996), boost employee morale and loyalty (Lewis, 1995), promote teamwork among coworkers (O’Donnell, 1994), and create a benevolent image for the employer. However, the actual outcomes of these programs remain mixed (Lewis, 1995; Parker & Spinda, 2007). For instance, a systematic review of 33 studies on the outcomes of EWPs published between 2000 and 2009 reported inconsistent results regarding the effectiveness of EWPs in reducing tobacco and alcohol use, and controlling health-related costs; this study also reported limited support for the effect of EWPs on absenteeism and mental health (Osilla et al., 2012). When implemented inappropriately, EWPs can lead to resentment and alienation among particular groups of employees (Zoller, 2004).
One possible explanation for these findings is that management and employees define health and wellness differently. For instance, the Farrell and Geist-Martin (2005) study of technology employees’ narratives about wellness revealed that although the EWP framed wellness in terms of physical and mental wellness, employees tended to talk about social wellness (i.e., the connections one has with colleagues and the community at large). Hence, the effective design and implementation of EWPs calls for a study of the subjective definition of health among program participants. Studying health narratives (i.e., personal tales and accounts about health) provides insights into these subjective understandings of health.
A health narrative is not completely coherent, but “a contested, open-ended text, fraught with competing rhetorics and systems of meaning” (Willard, 2005, p. 115). The dialectics approach offers a unique tool for unpacking the conflicts and contradictions in health narratives. Dialectical theory refers to a variety of conceptual approaches that rely on contradictions as a useful way to understand the world. Hegel (1969) and Bakhtin (1981) have been highly influential in developing theories of dialectics in the western world. Hegel defined dialectics as tensions that result from opposing ideas. A Hegelian dialectic consists of a thesis and antithesis, which eventually is synthesized to resolve the initial dialectic tension and become the foundation of a new round of dialectical tension. Bakhtin, on the contrary, argued that the tension between the two contradicting ideas might never be solved or reach a synthesis. The authors adopt the approach of Bakhtin and conceptualize dialectics as tensions between opposite ideas or values (Stohl & Cheney, 2001).
Dialectics are useful to the study of health narratives. Examining the dialectical tensions embedded in individual narratives and experiences about health provides insights into the creation and negotiation of meaning in the health care context and a baseline for more effective public health policies and campaigns (Villagran, Collins, & Garcia, 2008). Several existing studies have adopted the dialectical approach for the study of health discourses and narratives. Basu (2010) studied the narratives of sex workers in India as subalterns and found that sex workers conceptualized health as impossible by discursively engaging the dialectic of hope and hopelessness. Another study examined the discourse of a healthy diet among Asian Indians living in the United States and found that such discourse was based on the dialectical tension between homogeneity and heterogeneity (Koenig, Dutta, Kandula, & Palaniappan, 2012). This pair of dialectical tensions allowed Asian Indians to remain connected to their ethnic identity and manage individual dietary preferences at the same time. Golden (2010) examined the experiences of husbands and wives placing spouses with dementia in a residential care facility and found that they experienced a series of contradictions of autonomy and connection, change and continuity, and openness and closedness before, during, and after placement. Finally, Considine and Miller (2010) studied end-of-life communication between hospice workers and their patients and found that such communication was guided by the dialectical tension between “leading” and “following.” Most of the hospice workers either shifted between the two poles in communicating with patients or transcended the dialectic tensions, depending on the situation.
Hence, to understand how the idea of health is constructed by EWP participants, the researcher asked the following research question:
Method
The research was conducted with participants of an EWP at a large southeastern university. The wellness program was established in 2009 and consisted of a variety of free resources and events to increase employees’ sense of well-being and assist them in setting and attaining personal health and fitness goals. The signature offering was an annual health screening that measured height and weight; triglyceride, cholesterol, and glucose levels; blood pressure; and other biometrics. Employees were assigned to a category, depending on their biometric measurements. The next year, these employees had the opportunity to participate in the screening again and, if improved, could be assigned to a new category and eligible for cash rewards. A small cash reward was also given to initial participants.
Other program offerings included a US$5 fresh lunch on Fridays, weight loss groups, a team-based 5 km run/walk, meditation classes, diabetes education, tobacco cessation courses, exercise training, and Strive for Five, an ongoing program in which group members held each other accountable for reaching specific lifestyle goals. The wellness program was housed in its own office on campus, and support personnel consisted of a Director of Health and Wellness, paid staff, and staff and faculty volunteers called Ambassadors who promoted the program within their own professional or academic units on campus.
Participants
The participants for this study were 12 EWP Ambassadors, liaisons between the wellness program and their departments to increase membership and encourage participation among existing members of the program. The EWP director facilitated Ambassador participation through email. Strategic sampling was used to ensure Ambassadors were recruited for the study (Lindlof & Taylor, 2002).
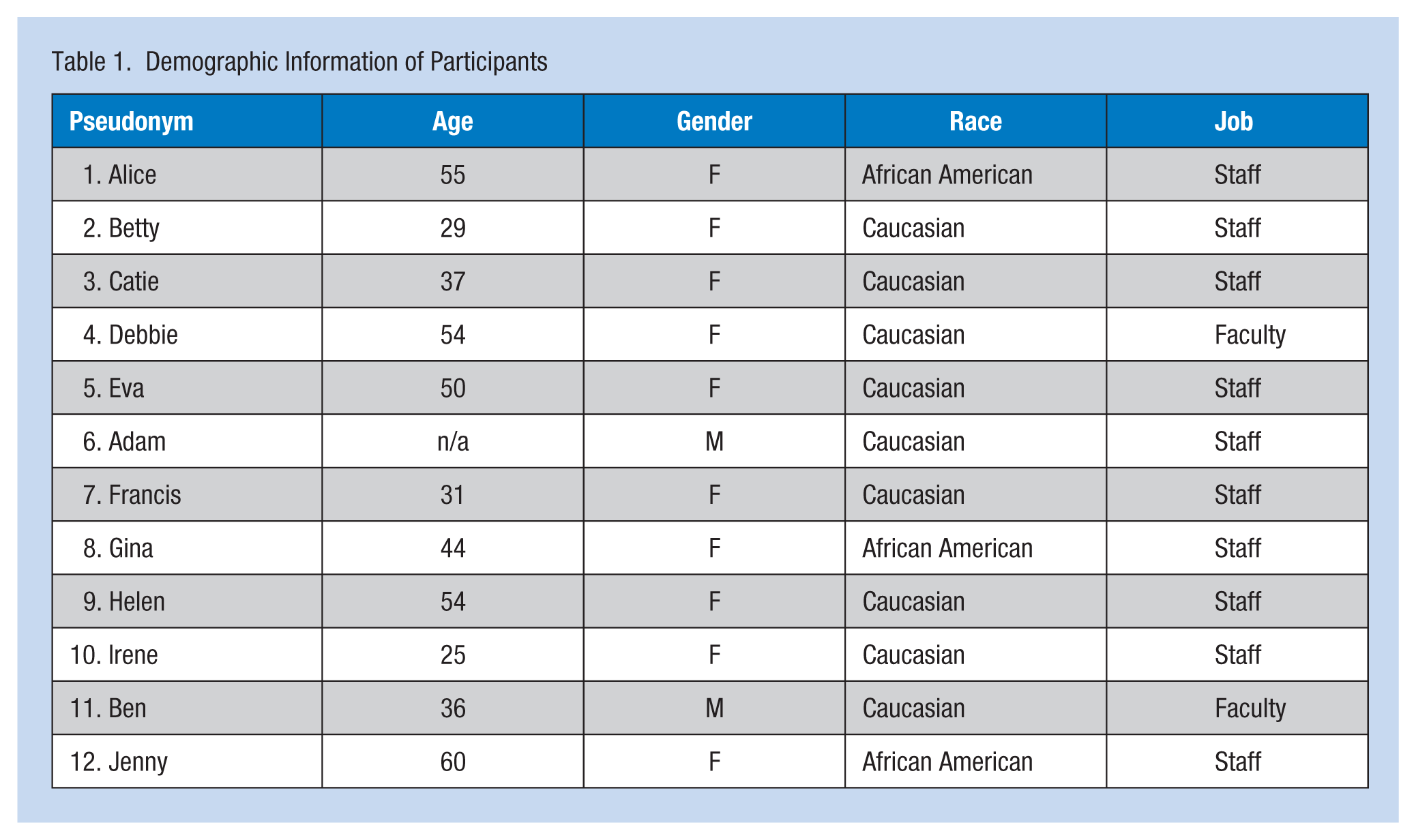
Participants represented a variety of departments (i.e., Department of Kinesiology, Department of Mathematics, Department of Art History, Office of Information Technology, College of Continuing Studies, Student Affairs, Study Abroad Office, School of Law, Housing, Recreation Center, Research and Assessment, and Payroll) on campus and included two faculty and 10 staff members. Nine were Caucasian and three were African American. The average age of the participants was 43.18 years (SD = 12.14; Table 1).
Demographic Information of Participants
Semi-Structured Interviews
The study was approved by the Internal Review Board of the authors’ institution. Semi-structured interviews were conducted using a series of prepared questions followed by allowed probing regarding incidents that were particularly relevant to the research goals. The questions were divided into three main sections. Questions in the first section were related to understanding participants’ backgrounds as employees and their wellness program goals. The second set asked participants specifically about their role as Ambassadors. These questions were designed to connect the Ambassador role to participation of others in the wellness program. The final set of questions addressed participants’ general attitudes and beliefs about health, and how they sought and shared health information. Although efforts were made to ensure that each question was addressed, the interviews were conducted as conversations, allowing for the discussion to take new directions if relevant.
At the interviews, participants were informed that their responses would be confidential, presented with a consent form to sign, and then asked whether they could be recorded. All the participants in the study were referred to by pseudonyms to protect their privacy. In all instances, participants agreed to be audio recorded. Interviews generally lasted between 30 minutes and 1 hour. Each participant was given a US$20 gift card for their time. All interviews were transcribed verbatim by a graduate student. In the end, a total of 178 single-spaced pages of transcripts were analyzed.
Data Analysis
This study applied a grounded theory approach and constant comparison method for analyzing the interview data. First, the researchers used open coding (Glaser & Strauss, 1985), which required reading the interview transcripts for the purpose of identifying recurring concepts and values. This process revealed the prominence of dialectical tensions in employees’ health narratives, although finding dialectical tensions was not the initial goal of the study. The three pairs of dialectics were autonomy versus connection, private versus public, and control versus lack of control.
Second, the researchers recoded the interviews based on the three pairs of dialectical tensions. Finally, the recoding revealed multiple overlapping tensions and tensions that branched off from primary tensions. Thus, the analysis turned to the constant comparison method to locate subthemes or more specific dialectical tensions within broader themes. In essence, these dialectical tensions explained how participation in the wellness program, personal beliefs about health, and relationships with other employees were connected within organizational and larger social and cultural contexts.
Results
The analysis of the interview transcripts led to the identification of a number of dialectical tensions in participants’ narratives about health: autonomy versus connection, public versus private, and control versus lack of control.
Autonomy Versus Connection
The tension between achieving health as an individual and striving for health within a community occurred frequently in participants’ discussions about their own health attitudes and behaviors. On one hand, participants often talked about health in terms of what they ate, how much they exercised, and how they felt. Individuals were expected to be responsible for their own health. Similarly, employees felt “judged” for not being healthy or not maintaining a healthy lifestyle (i.e., not working out and not eating nutritiously). For instance, when asked why some of their colleagues did not participate in the EWP, one participant answered half-jokingly, “Other than being lazy?” Comments like this indicated participants’ beliefs that individuals were responsible for their own health.
On the other hand, participants defined health as situated in one’s immediate and distant social networks, and many of them expressed the desire to achieve health in a community. Some even came to define health in relational terms. Many participants cited having “a sense of community,” as their motivation to strive for health, as if it was too lonely to do it on their own. This community was sometimes based on strong ties such as their families and close friends, but many times, a community was formed by weak ties such as colleagues and other EWP participants. Family was obviously the most important context for healthy behavior. Several participants commented that they liked the EWP because of its family focus. For instance, Betty said,
I think I like that it’s family-oriented. A lot of things seem to be like involved with, you know you and your family, kind of like they’re doing the 12 Days of Wellness. I saw that they had like an event where it was like come and get information, but it wasn’t just information that was just applicable to me, also it’s something that could be for my family. So I think that the fact that they considered your family, I think that kind of was a great aspect.
Some participants also stated that they were trying to strive for health as a family, instead of as individuals.
Other participants commented on the importance of striving for health within the communities of friends and colleagues. Such connections provided social support for individuals. Debbie commented,
I like the sense of community because that’s fun for me and I like to meet people across campus . . . and there are a lot of folks that I know so it’s really kind of, it’s just fun
Striving for health with a group of friends and colleagues also gave workers a sense of camaraderie. Jenny said,
Everybody’s in the same boat. And you think well, this is my problem with me, you can see, hey, I have a battle with weight, but it’s like we battle with the same thing. You may not be able to see mine, but that makes you feel better . . . makes you feel a lot better.
Public Versus Private
Another pair of dialectical tensions in participants’ health discourses was the tension of treating health as a private issue and viewing health as a public matter. Very often, health was considered to be something very private and personal, and as a result, people talked only to their close friends and family members about health or did so in any depth. Although participants did talk about health with their colleagues, these conversations often stopped at the very superficial discussion of weight or healthy diet. Even within the EWP, participants’ conversations about health concerns and challenges barely scratched the surface. Adam said, “We avoid conversations about specific markers like reducing weight, or getting a handle on your hypertension.” He went on to say, “To create a lifetime awareness and appreciation of wellness, you have to have those kinds of discussions about chronic disease . . . I don’t even think they happen in our program as well as they should.” In fact, some employees were very cautious talking about their health problems with the staff of the EWP because they were afraid that whatever information they disclosed might be used against them by their employer. Irene, who used to work for the EWP, commented,
And you know, just people are really sensitive about their health information. Especially if they have any problems and they don’t want their employer to know, because there’s just always that fear that, “Well what if I lose my job or, you know, what if it affects my performance at work?” Then maybe they don’t want the employer to be the first one that finds that out.
Furthermore, some employees tended to think of health as a private matter and resisted the EWP because they considered it to be a form of managerial control. Although none of the participants in this study explicitly claimed to hold this view, perhaps because they were all active participants and leaders in the program, they did often mention this situation anecdotally. For example, Eva talked about the story of a colleague who consciously chose to improve her health on her own instead of participating in the EWP. She said,
But [this colleague] told me, the reason she doesn’t want to participate in the programs is because she doesn’t want to go exercise because it’s an employer program. She wants to be exercising because she’s choosing to exercise and she’s choosing to do it on her own when she can and that type of thing. And that struck me because I’d never thought of it that way because, here I’m seeing it as a benefit, a gift that the university offers, and she would interpret that more as a mandate, an employer mandate instead of a benefit or a gift.
Although health was often considered a private matter, health also contributed to one’s public image and identity. Participants in the EWP often associated the identities of their colleagues and themselves with their health status. One of the interview questions asked, “To what extent is being healthy part of who you are?” Participants unanimously said health was a very important part of their identity. Furthermore, participants tended to evaluate their colleagues based on their health status. In this sense, health became one’s image, public and visible, for others to see.
Ben, whose job was somewhat related to health and wellness in the university, did not even consider his participation in the EWP in personal terms. Instead, he treated his participation as a public endorsement of the program that was consistent with his identity as an expert on physical exercise. He said,
For me it was more of just I think I ought to be doing this to . . . be supportive of another organization on campus that’s . . . trying to do something good . . . Because if people like me don’t help with it, what message is that sending . . . to people that maybe are contemplating, “I might ought to join this”?
For Ben, being healthy was part of his public persona instead of his private identity.
Control Versus the Lack of Control
Another pair of dialectical tensions in participants’ discourse about health was the tension between a sense of control and a sense of lack of control. On one hand, employees seemed to have high self-efficacy. They expressed the belief that if they did the right thing, they would be healthy. This idea very much resembled the discourse of healthism or lifestylism, which is based on the fundamental assumption that individuals are ultimately in charge of their own health (Crawford, 1980). Many participants believed they would achieve perfect health as long as they adopted a healthy lifestyle, which included but was not limited to healthy eating, drinking more water, exercising regularly, and not smoking. One question asked of participants was how they would rate their current health status on a scale from 1 to 10. Although most of the participants stated a number between six and eight, almost all of them expressed the belief that they could achieve a 10 if they would adopt a few more healthy behaviors, such as drinking less soda and more water or eating fewer snacks.
On the other hand, participants also expressed a sense of lack of control over their health, this feeling that they lacked control stemmed from familial, organizational, and larger social contexts. Many female participants mentioned that although they were concerned about their own health, they were not able to act on improving their health because of family responsibilities. They also cited family obligations as one of the causes of their colleagues’ unsatisfactory health and their failure to participate in the EWP.
Furthermore, this feeling of powerlessness came from work. The intensity and the sedentary nature of most participants’ work were cited as major obstacles to achieving health. For instance, Alice commented,
I sit a lot. And with bursitis if you’re not moving a lot it can bother you, and if you’re standing too much it bothers you so it takes some getting up and walking around and getting a little exercise. Sometimes you get pinned to your desk working on certain things and you’re not getting the physical exercise and it can become stressful at times, and by the end of the day you’re too exhausted to really do anything besides go home, cook, do whatever errands and go to sleep. So it’s kind of a little drawback on it.
On an organizational level, some participants in managerial positions also cited a lack of support from the university as an obstacle to health promotion. They cited the university’s lack of resources for health promotion, inflexible work schedules, and lack of involvement from upper administration as organizational constraints that rendered employees powerless in attaining health.
Finally, the larger social context also contributed to participants’ feelings that they lacked control over their own health. Jenny cited the social environment as a cause of her poor diet,
Being where I’m from, it’s a small town, everybody does what they need to do [sic], and with me if it’s fried it’s food. No meat, no meal. That was the idea I had, that was my Southern mindset, you know. And I came from a family of farmers. Chickens and pigs and cows. So we ate meat at every meal because we raised meat. But you know, Southern family. It’s everybody in the South.
Similarly, Francis commented on how American culture made it extremely difficult to cultivate a healthy body image among children. She said,
Body image is hard in our culture; it’s so hard. And I told several friends who have daughters, “I don’t know how you’re going to raise them. I know you’re doing a great job, but how do you raise—and boys too—boys are starting to show signs of body image issues and eating disorders and whatnot. And I know the culture can’t completely be blamed, but I really feel it’s doing a pretty horrible job of raising kids to, or influencing their thoughts about their bodies.
Discussion
Answering the call of Basu and Dutta (2009) to “foreground articulations of health by participants who are at the core of any health campaign” (p. 86), the current study examined the health narratives of EWP participants at a large public university using an interpretive perspective. Semi-structured interviews with participants of the EWP demonstrated that their health narratives were not coherent. Instead, three pairs of dialectical tensions were identified: autonomy versus connection, private versus public, and control versus lack of control. Participants tended to think of health as an individual endeavor, yet they also approached their endeavors within social networks of family, friends, and colleagues. Furthermore, most of the participants were experiencing the tension of treating health as a private matter and as a public issue. This tension was especially salient in the context of the EWP. On one hand, most of the participants kept their health a private matter, being very cautious communicating with others on health issues. On the other hand, health became a part of employees’ public identity at work. Finally, participants expressed ambivalence between a high level of perceived control over their health and a sense of lack of control.
Implications for Practice and Future Research
The dialectical tensions in EWP participants’ health narratives identified in this study indicated that health is a multifaceted concept that must be understood not only as an objective state but also a subjective experience. Furthermore, such subjective and personal conceptualizations of health will certainly affect individuals’ health behaviors (Reed, Rayens, Conley, Westneat, & Adkins, 2012). The findings offer several practical implications for the promotion of health and wellness in the workplace. First, practitioners must acknowledge the inherent contradictions in employees’ beliefs about what health is and how to achieve health. Allowing participants to define health in their own unique ways could contribute to their confidence and increase their identification with the program.
Second, EWPs should be designed to encourage internal diversity so that employees will not feel excluded or alienated. Pushing to achieve health and wellness goals defined by management or health professionals in a top-down manner is likely to discourage employees from participating and benefiting from EWPs as well as creating resistance and resentment in extreme cases. For instance, EWPs should provide programs that accommodate employees’ needs for both privacy and community support.
The current study only examined the health narratives of Ambassadors in the EWP, who are likely to be more devoted to health and wellness and more involved in the EWP than regular participants. Their understanding of health might also be more sophisticated and nuanced than regular EWP participants. The next step is to examine the health narratives of non-Ambassador participants in the program, to explore whether these groups of employees conceptualize health differently. This study will provide insights into how to increase participants’ involvement in and commitment to the program. Further research should also examine how those employees who chose not to participate in EWPs conceptualize health, as such a study will assist EWP administrators to better understand the reasons for such choices and modify programs to have wider appeal. In addition, because EWPs support employees improving their health in a group setting, it will be interesting to examine how the interactions among EWP participants might influence their understanding of health and wellness, and change their actual behaviors to improve their own health. The social network approach will be especially useful in this line of research (Tang, Mieskowski, Oliver, Eichorst, & Allen, 2015). Finally, since EWP participants have multiple identities (e.g. participants, employees, parents, siblings, and children), further research could adopt the bona fide group theory (Putnam & Stohl, 1990) to examine the overlap of these identities and whether their identity as health seekers in an EWP will influence their personal lives and those of their families and social circles encouraging positive health outcomes in a wider context.
Conclusion
By investigating EWP participants’ subjective understandings of health, the current research identified three pairs of dialectical tensions, autonomy versus connection, private versus public, and control versus lack of control, through an analysis of participants’ narratives. These findings highlight the importance of designing EWPs that recognize employees’ diverse, and sometimes contradictory, beliefs about health.
Applying Research to Practice
Employees often have different beliefs about what is health and how to achieve health. Employee Wellness Programs (EWPs) should be designed to allow for such internal diversity so that employees will not feel excluded or alienated. Pushing to achieve health and wellness goals defined by management or health professionals in a top-down manner is likely to discourage employees from participating in and benefiting from EWPs as well as create resistance and resentment in extreme cases.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The current study was partially supported by a RGC grant from the University of Alabama awarded to the first and second authors.
Author Biographies
Dr. Tang is an associate professor, Department of Communication Studies, University of Alabama. She conducts research on culture and health communication.
Dr. Baker is an assistant professor, Department of Communication Studies, University of Alabama. Her research interests lie in the areas of organizational diversity, group communication, dialectics, crisis management rhetoric, and negotiation.
Dr. Meadows is an assistant professor, School of Communication, East Carolina University.