
Abstract
Research suggests that workplace discrimination plays a role in absenteeism, productivity, and turnover. A link among workplace discrimination, mental health, and health disparities may also exist. The purpose of this study was to determine whether self-reported workplace discrimination is associated with alcohol abuse among hospital workers. Cross-sectional analysis of baseline data collected from a prospective cohort study of workers in two healthcare institutions (n = 664) was conducted. Workplace discrimination in the previous 12 months was reported by 14% (n = 91) of participants who were four times more likely to score higher on likely alcohol abuse than their peers. White participants who reported any discrimination were more likely to score higher on likely alcohol abuse than racial/ethnic minority participants who reported any discrimination. Given a diversifying workforce, further research is needed on how workplace discrimination contributes to stress and maladaptive coping, and ultimately health disparities.
Unfair treatment in the workplace is one of the most common types of discrimination reported by Americans (Kessler, Mickelson, & Williams, 1999) and more likely to be reported by racial/ethnic minorities than Whites (Pavalko, Mossakowski, & Hamilton, 2003; Rospenda, Richman, & Shannon, 2009; Wadsworth et al., 2007). Workplace discrimination is defined as treating an individual less favorably in hiring, firing, pay, job assignments, promotions, layoff, training, fringe benefits, and any other term or condition of employment because of individual characteristics such as age, race/color, and sex (U.S. Equal Opportunity Employment Commission, 2008). Such experiences affect absenteeism, productivity, and employee turnover (Bond et al., 2007).
Beyond its job-related consequences, workplace discrimination may also be associated with racial/ethnic health disparities. Workplace discrimination can be considered a stressor distinct from occupational stressors such as job strain (high psychological work demands coupled with low control in meeting those demands) and generalized stress that is unrelated to individual characteristics such as race/ethnicity, gender, or social class (Bond et al., 2007).
Racial/ethnic minorities consistently report more stressors and higher levels of stress than Whites (Sternthal, Slopen, & Williams, 2011; Turner, Wheaton, & Lloyd, 1995). Conceptual models of the relationship between social stressors and health suggest that behavioral, psychological, and physiological responses to stressors accumulate over time to produce poor health outcomes (Clark, Anderson, Clark, & Williams, 1999; Geronimus, 1992; Krieger, 2005; McEwen & Seeman, 1999). Differential exposure and vulnerability to stress over a lifetime are thus potential drivers of racial/ethnic health disparities (Geronimus, Hicken, Keene, & Bound, 2006; Pearlin, Schieman, Fazio, & Meersman, 2005; Thoits, 2010). Workplace discrimination adds to that disparate burden of stress.
The mental health consequences of workplace discrimination include diminished psychological well-being, increased risk for psychological distress, and pronounced depressive symptoms (Roberts, Swanson, & Murphy, 2004; Rospenda, Fujishiro, Shannon, & Richman, 2008; Wadsworth et al., 2007). The sequelae of psychological distress include maladaptive coping strategies such as alcohol abuse. Racial/ethnic differences have been found in self-reported alcohol use, abuse (defined as a pattern of drinking that results in harm to one’s health, interpersonal relationships, or ability to work; Centers for Disease Control and Prevention, 2014), and associated problems (health and social harms directly or indirectly attributed to alcohol use; Rehm, 2011). Blacks initiate drinking at an older age, have lower rates of alcohol use, and lower levels of alcohol use compared with Whites but experience more severe consequences related to use (Zapolski, Pedersen, McCarthy, & Smith, 2014). Pooled data from three surveys of U.S. adults (n = 22,500) between 2000 and 2010 show that American Indian/Alaskan Native and U.S.-born Latinos consume the most alcohol and experience a greater prevalence of associated harms (Greenfield et al., 2015). Other national studies find that Whites and American Indians/Native Americans are at greater risk of alcohol use disorders than other racial/ethnic groups (Chartier & Caetano, 2010).
These consequences could be particularly relevant for the healthcare industry. Increased reporting over time of workplace discrimination is partially attributed to growing racial/ethnic diversity in the American workforce (Rospenda et al., 2008; U.S. Equal Opportunity Employment Commission, 2008). The Joint Center for Political and Economic Studies (Frogner & Spetz, 2013) conservatively estimates that at least one third of the future workforce will be employees of color. Furthermore, the 2010 Patient Protection and Affordable Care Act (P.L. 111-148) includes a number of provisions to address workforce diversity issues.
Previous studies suggest that workplace discrimination is associated with alcohol abuse (Rospenda et al., 2009; Yen, Ragland, Greiner, & Fisher, 1999), but the phenomenon has not been examined in healthcare settings. Therefore, the current study examined the association between self-reported workplace discrimination attributed to multiple demographic characteristics and alcohol abuse among an ethnically diverse hospital staff. The study hypothesis was that racial/ethnic minority hospital staff would be more likely to report both workplace discrimination and alcohol abuse than White staff. This article adds to the literature by examining the independent effect of workplace discrimination on alcohol abuse by including other measures of psychosocial stress and explicitly hypothesizing an interaction effect between minority status and reports of workplace discrimination.
Method
Data Source
The Gradients in Occupational Health in Hospital Workers (GROW) Study was a longitudinal case–control study of injuries among hospital workers. Baseline data were collected between July 2002 and November 2004; detailed study methods have been described elsewhere (Rugulies et al., 2004). The 664 participants (166 cases and 498 controls) were recruited from approximately 6,000 hospital workers employed by two healthcare institutions in northern California. Cases were recruited at the occupational health clinic when employees sought care for a work-related injury. Work-related injuries were defined as a new presentation of an acute or cumulative work-related musculoskeletal injury that was evaluated at the site’s hospital-based employee health clinic and determined to be work related. Physicians were excluded from the study because they did not go to the same employee health clinic as other hospital staff when suffering a work-related injury. Cases were matched with controls by job group, shift length, or at random (within a hospital), yielding a 3:1 ratio to cases. The present study analyzed data from baseline data collection.
Measures
Workplace discrimination
To assess exposure to workplace discrimination, participants were asked, “During the past year, have you been treated unfairly by coworkers or supervisors because of your race or ethnicity, nationality, sex, sexual orientation, or age” (1 = yes, 0 = no); data from this item were used in the main analyses. For those who reported any workplace discrimination in the past year, additional questions were asked about the type and frequency of such experiences. These items were adapted from a measure that included workplace harassment, unfair treatment, and psychological abuse designed specifically for physicians during their intern training (Richman, Flaherty, & Rospenda, 1996). The GROW study expanded the unfair treatment section of the Richman measure to include a variety of bases for unfair treatment (e.g., the original scale asked only about unfair treatment based on gender) and workplace circumstances during which unfair treatment might occur. In addition, the GROW study asked participants to rate the stressfulness of these experiences using the Experiences of Discrimination measure (Krieger, Smith, Naishadham, Hartman, & Barbeau, 2005) as a model.
Alcohol abuse
The CAGE (Cut down on drinking, Annoyances with criticisms about drinking, Guilt about drinking, and using alcohol as an Eye Opener) questionnaire is an alcohol abuse screener developed for use in healthcare settings (Ewing, 1984). A score of 1 is evidence of risk of alcohol abuse, 2 is evidence of a current problem, and 3 is evidence of dependence. Participants were grouped in the “likely alcohol abuse” category if they scored a 2 or 3.
Demographic information
Data were collected on self-identified race/ethnicity (White, Asian/Pacific Islander, Black, Latino, or Other/Mixed), age in years, gender, educational attainment (i.e., high school graduate or less, some college, associate degree, baccalaureate degree, or more), and annual household income (i.e., less than US$40,000, US$40,000-US$79,999, US$80,000-US$119,999, US$120,000 or more).
Occupational category
Originally, 13 occupational categories were created based on status in the organization, education/licensing, frequency and type of patient contact, and frequency and type of physical labor. The categories then were collapsed into six groups: administrator and professional, nursing, other clinical (e.g., mental health, nursing assistants, rehabilitation), clerical, technical, and support positions.
Stress
The four-item short version of the Perceived Stress Scale (Cohen, Kamarck, & Mermelstein, 1983) was used to assess general social stress unrelated to occupational demands or discrimination, which is known to contribute to poor health outcomes (McEwen & Seeman, 1999). Participant appraisal of general stressors such as difficulty controlling important things in one’s life were measured on a 4-point scale (0 = never, to 3 = very often). The items were summed to produce a stress score (range = 0-12).
Job strain
The 14-item version of the Job Content Questionnaire (Karasek et al., 1998), which includes five items on psychological demands and nine items on job control, was used to assess job strain, which has been associated with poor psychological and physical outcomes (Netterstrøm et al., 2008). Participant responses were measured on a 4-point scale (0 = strongly disagree, to 3 = strongly agree). A summary score was calculated by taking the ratio of the psychological demands subscale to the job control subscale; higher ratio scores indicate greater job strain.
Statistical Analyses
Chi-square analyses were conducted to describe differences in reports of workplace discrimination and alcohol abuse by sample characteristics. Logistic regression analyses were then conducted to examine the association between workplace discrimination and alcohol abuse independent of socio-demographic characteristics, perceived stress, and job strain. A regression model tested the interaction effect of discrimination and minority status on alcohol abuse. SAS Version 9.2 (Cary, North Carolina) was used for all analyses.
Results
Workplace discrimination was reported by 14% of participants (n = 91), and 9% of participants (n = 60) scored 2 or 3 on the CAGE screener. In unadjusted analyses, workplace discrimination was associated with race/ethnicity (with Blacks and Whites being most likely to report these experiences), annual household income (with those earning US$40,000-US$79,999 most likely to report these experiences), and more job strain. Alcohol abuse was associated with being male and White, and reporting more perceived stress. Table 1 presents descriptive statistics for the sample stratified by report of any workplace discrimination in the past year and alcohol abuse.
Sample Characteristics Stratified by Report of Workplace Discrimination and Self-Reported Alcohol Abuse (N = 664)
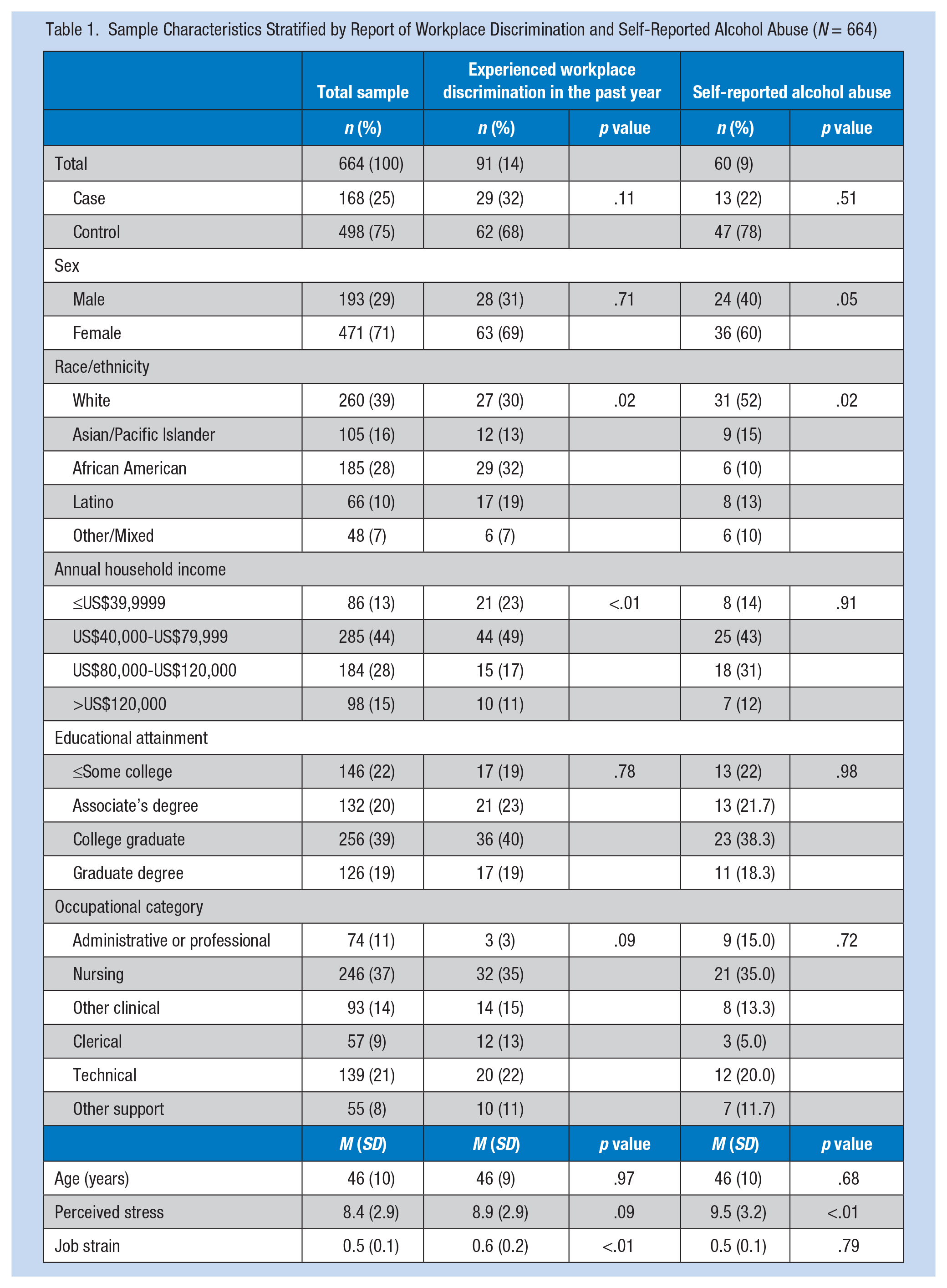
Workplace discrimination in the past year was most commonly attributed to race/ethnicity (63%, n = 57), nationality (47%, n = 42), and age (44%, n = 40). Of those who reported unfair treatment attributed to race/ethnicity, 37% were Black, 23% were Latino, 18% were Asian or Pacific Islander, 14% were White, and 9% were Other or Mixed Race (p ≤ .01). Of those who reported unfair treatment attributed to nationality, 48% were Black, 21% were Latino, 12% were Asian or Pacific Islander, 10% were White, and 10% were Other or Mixed Race (p ≤ .01). No significant difference was found by race/ethnicity of those who reported unfair treatment attributed to age: 38% were White, 30% were Black, 18% were Latino, 10% were Asian or Pacific Islanders, and 5% were Other or Mixed Race (p = .69).
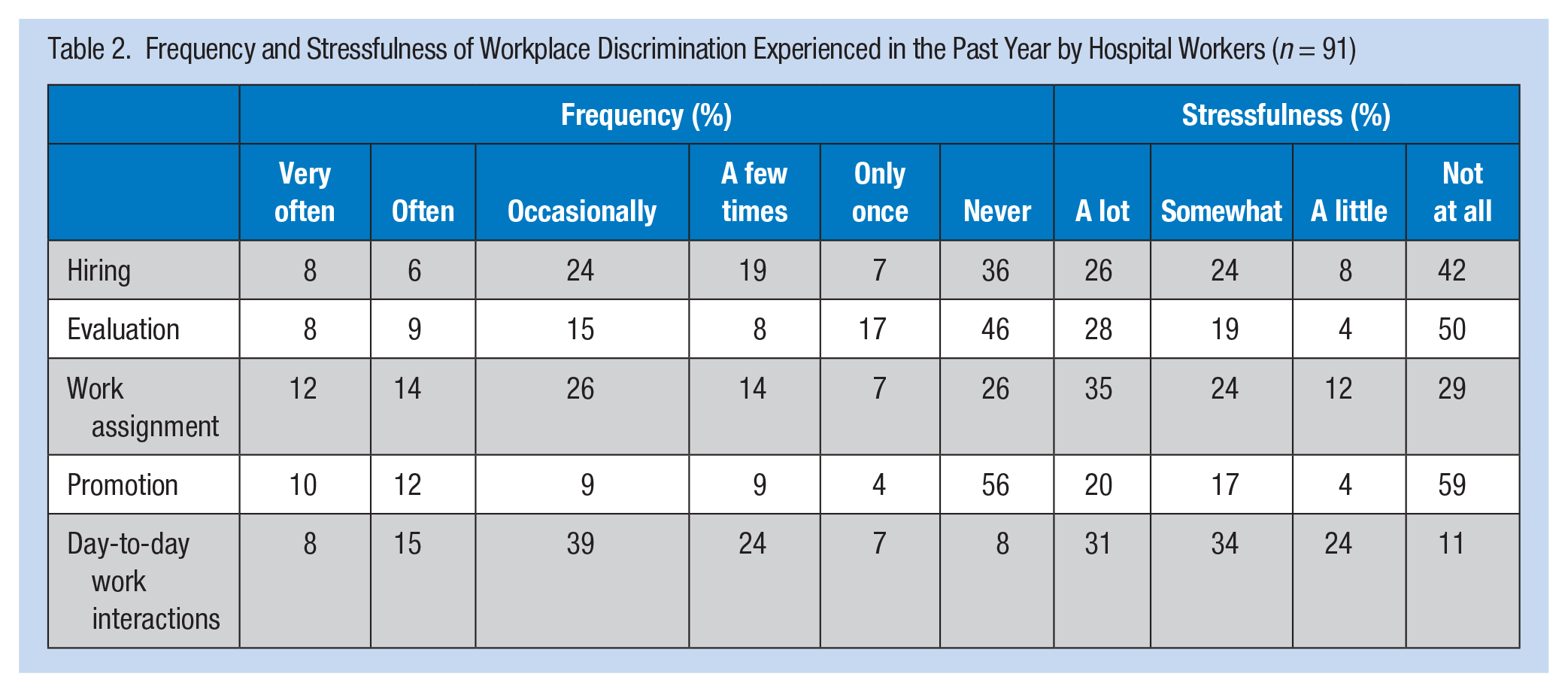
Of those reporting any discrimination in the past year (Table 2), day-to-day interactions was the most common issue (92% experienced at least one discriminatory day-to-day interaction in the past year and 89% considered the experience at least a little stressful). Discrimination in promotion was the least commonly reported issue (44% experienced this type of discrimination in the past year and 41% considered the experience at least a little stressful). No differences in stressfulness ratings were found by race/ethnicity.
Frequency and Stressfulness of Workplace Discrimination Experienced in the Past Year by Hospital Workers (n = 91)
For the moderation analysis, minority status was used in place of racial/ethnic categorization due to small sample sizes. The interaction between minority status and workplace discrimination was significant for alcohol abuse, that is, the odds of alcohol abuse (scoring 2 or 3 on the CAGE screener) was lower for minorities who reported workplace discrimination in the past year than for Whites. Table 3 presents the multivariate model of the association between workplace discrimination and alcohol abuse.
Multivariate Regression Model Examining the Association Between Workplace Discrimination and Self-Reported Alcohol Abuse by Hospital Workers (n = 664)
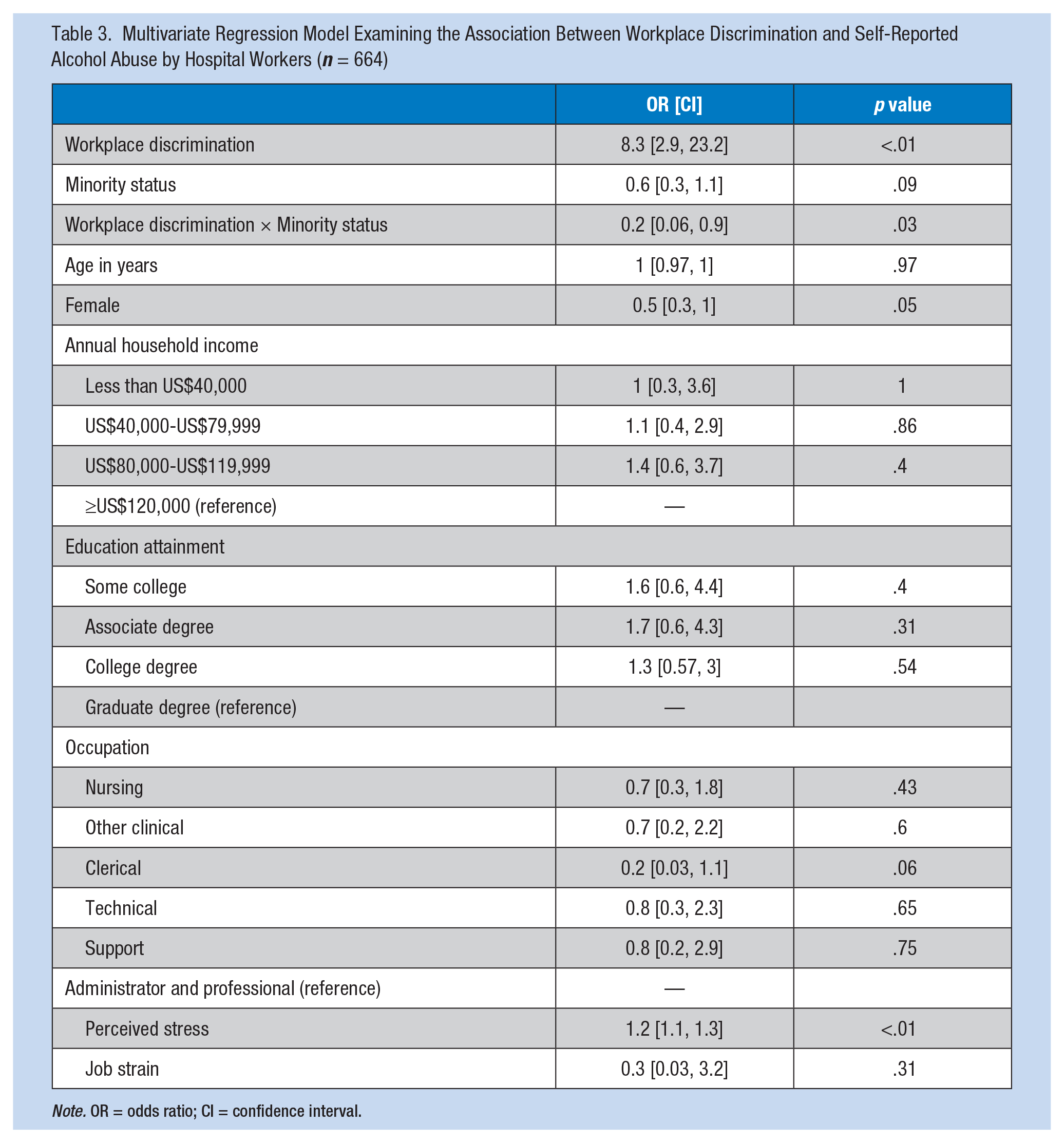
Note. OR = odds ratio; CI = confidence interval.
Discussion
Unfair treatment in the workplace is one of the most common types of discrimination reported by Americans and thus a potential contributor to racial/ethnic health disparities. Racial/ethnic minority hospital staff reported more discrimination than White hospital staff, consistent with other studies, but no differences in ratings of stressfulness of such experiences were found. Little is known about racial/ethnic differences in appraisals of discrimination stress as measures used in previous research often lacked that component (Thrasher, Clay, Ford, & Stewart, 2012). One explanation for the lack of racial/ethnic differences in appraisal of discrimination stressfulness may lie in differences in life-long experiences of discrimination and consequent adaptation. Racial/ethnic minorities’ familiarity with discrimination (i.e., discrimination that one has experienced, witnessed, heard about from family and friends) may result not only in adaptive coping with discrimination but also in less severe appraisal of associated stress. Ursin (2009), in discussing the cognitive activation theory of stress (CATS), explains the definition of stress in four terms, stress stimuli, stress experience, non-specific, and general stress response, and the body’s physiological response to stress. When a stress stimulus (discrimination in the current study) is presented, the individual evaluates the threat level of that stimulus based on prior experiences and expectations of outcome and responds accordingly (Meurs & Perrewé, 2011; Ursin, 2009). The racial/ethnic minority participants in the current study reported more discrimination in their current work situations than their White counterparts, which endowed them with greater present-time prior experience with each encounter. According to CATS (Meurs & Perrewé, 2011; Ursin, 2009), greater prior experience may result in different, likely lower, outcome expectancies and adaptive coping. Part of adaptive coping may include viewing and rating one’s experience of stress (discrimination) as less severe. In addition, the statistically significant frequency of discrimination experienced by minority participants is not likely to have been limited to the time of the study; they may have had more past-prior experience with discrimination. It is important to note that physiological response is a separate category of stress response from general stress response (Ursin, 2009); responding to stress is normative, but sustained arousal (which is likely the more frequent stress [discrimination] experienced) has been correlated with illness and disease (Clark et al., 1999; Sternthal et al., 2011; Ursin, 2009)
The positive, independent association between workplace discrimination and alcohol abuse is also consistent with existing research in both workplace and general perceived discrimination (Borrell et al., 2007; Rospenda et al., 2009; Yen et al., 1999). No previous study of workplace discrimination, however, has explicitly considered the potential moderating effect of minority status on alcohol abuse. Contrary to the study hypothesis, White hospital staff members who reported workplace discrimination were more likely to score in the “likely alcohol abuse” category than racial/ethnic minority staff who reported workplace discrimination. Another study using data from the 2005 National Alcohol Survey found that Whites who reported experiencing unfair treatment (discrimination) often or very often had greater odds of problem drinking, after controlling for psychological distress (Mulia, Ye, Zemore, & Greenfield, 2008). This study used a measure specific to workplace discrimination and a lower threshold for any discrimination experienced in the past year, which suggests a robust finding. National studies show Whites and Native Americans at greater risk of alcohol use disorders than other racial/ethnic groups (Chartier & Caetano, 2010). These racial/ethnic differences might be due, in part, to group differences in cultural norms and attitudes related to drinking. Specifically, Blacks tend to have more conservative alcohol norms and attitudes than Whites, which is evidenced by comparatively higher abstention rates among Blacks (Caetano & Clark, 1999). In the current study, drinking may be more culturally permissible for White employees as a way to cope with workplace discrimination.
The results of this study must be considered in light of its limitations and strengths. First, the cross-sectional design cannot establish the direction of effect between experiences of workplace discrimination and alcohol abuse. Second, the sample was drawn from two hospitals in northern California and may not generalize to other geographic or workplace settings. Third, a single item was used to measure workplace discrimination, which assesses exposure to this stressor but not the specific aspects of workplace discrimination that may influence health outcomes. The authors also were not able to assess the effects of each individual’s ability to cope with experiences of workplace discrimination using personal resilience and social support, which could directly influence alcohol abuse rates and may vary by racial/ethnic minority status. Strengths of the current study include the racial/ethnic, socioeconomic, and occupational diversity of the sample and use of a workplace discrimination measure that allowed for attribution to one or more personal characteristics (e.g., race/ethnicity, gender, age). Furthermore, only one previous study with a multiethnic sample also included other measures of stress to establish an independent effect of workplace discrimination on health (Rospenda et al., 2009). No identified research to date has tested the potential interaction effect of minority status and reports of workplace discrimination.
Conclusion
Study findings suggest that, independent of other general and job-related sources of stress, experiences of discrimination in a hospital setting are related to alcohol abuse, particularly among White staff members. The rise in discrimination claims with a diversifying workforce (U.S. Equal Opportunity Employment Commission, 2008) as well as new federal initiatives addressing healthcare workforce diversity issues underscores the need for further research on how experiences of workplace discrimination may contribute to stress, maladaptive coping, and poor health among healthcare workers. Prospective designs should identify trajectories of self-reported discrimination among workers who abuse alcohol and trajectories of alcohol use among workers who report discrimination. Most importantly, future studies should assess stress levels from workplace discrimination over time and its relationship to increasing alcohol use, transition to alcohol abuse, and development of alcohol-related problems by race/ethnicity.
Applying Research to Practice
This study of ethnically diverse hospital staff investigated a potential relationship between alcohol abuse and reports of workplace discrimination, which is known to contribute to absenteeism, productivity, and employee turnover. Increased alcohol intake may be one type of maladaptive coping behaviors used by workers experiencing discrimination on top of other sources of job stress. These findings suggest that healthcare leaders should consider how experiences of discrimination and other negative aspects of the work environment may be undermining their efforts to address the Affordable Care Act charge to increase workforce diversity. Furthermore, the findings can inform workplace wellness or employee support programs by highlighting possible cultural differences in responses to perceived unfair treatment at work.
Footnotes
Acknowledgements
The authors thank Genevieve Ames, PhD, and anonymous reviewers for their helpful comments on previous versions of this manuscript as well as Rachel Clad, MPH, for manuscript preparation assistance.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute for Arthritis and Musculoskeletal and Skin Diseases (Grant R01AR47798) and the National Institute on Aging (Grants P30AG015272-14S1; P30AG015272-14S3).
Author Biographies
Angela D. Thrasher is an assistant professor of Health Behavior at the University of North Carolina Gillings School of Global Public Health. At the time of the study she was a research associate with the Center for Aging in Diverse Communities at the University of California at San Francisco School of Medicine. Dr. Thrasher’s research interests include the health effects of discrimination experienced over the life course and the development, selection, and adaptation of measures used in research with diverse populations.
Anita M. Wells is an assistant professor of psychology at Morgan State University, where she leads the graduate program in psychometrics. Dr. Wells studies social psychological factors associated with academic performance, particularly trauma and violence, as well as psychosocial sustainability among military veterans and their families.
S. Melinda Spencer is an associate professor of Health Promotion, Education, and Behavior at the University of South Carolina Arnold School of Public Health. Dr. Spencer also holds an appointment with the USC Institute for Southern Studies. She is a social gerontologist whose research interests include the health of American Indian and African American elders, older adults living in rural communities, as well as sexual minority aging.
Leslie Cofie is a doctor candidate in the Department of Health Behavior at the University of North Carolina Gillings School of Global Public Health. His research interests include global health and African immigrant health.
Irene H. Yen is an associate professor of Medicine at the University of California at San Francisco School of Medicine. She also serves as research director of the Alameda County Medical Center. Dr. Yen’s research interests include the social determinants of health, the built environment, and survey tool development.