
Abstract
The promotion of self-care and the prevention of burnout among nurses is a public health priority. Evidence supports the efficacy of yoga to improve physical and mental health outcomes, but few studies have examined the influence of yoga on nurse-specific outcomes. The purpose of this pilot-level randomized controlled trial was to examine the efficacy of yoga to improve self-care and reduce burnout among nurses. Compared with controls (n = 20), yoga participants (n = 20) reported significantly higher self-care as well as less emotional exhaustion and depersonalization upon completion of an 8-week yoga intervention. Although the control group demonstrated no change throughout the course of the study, the yoga group showed a significant improvement in scores from pre- to post-intervention for self-care (p < .001), mindfulness (p = .028), emotional exhaustion (p = .008), and depersonalization (p = .007) outcomes. Implications for practice are discussed.
A growing awareness of the stress and burnout experienced by nurses in a variety of clinical settings is evident worldwide (Ribeiro et al., 2014; Sermeus et al., 2011). Researchers have examined the negative consequences of burnout, which range from job dissatisfaction and anxiety to patient dissatisfaction with care, lower nurse-rated quality of care, and high risk of negative patient outcomes (McHugh, Kutney-Lee, Cimiotti, Sloane, & Aiken, 2011; Poghosyan, Clarke, Finlayson, & Aiken, 2010; Vahey, Aiken, Sloane, Clarke, & Vargas, 2004). Recent research has documented the correlation between nurse burnout and health care-associated infections, patient falls, medication errors, and other patient adverse events (Cimiotti, Aiken, Sloane, & Wu, 2012; Van Bogaert, Dilles, Wouters, & Van Rompaey, 2014). Based on the findings of landmark studies, it is clear that working conditions for nurses (including nurse-patient ratio, shift hours, and role strain/overload) must be improved to effectively prevent burnout (Aiken, Clarke, Sloane, Sochalski, & Silber, 2002; Li, Early, Mahrer, Klaristenfeld, & Gold, 2014; McHugh et al., 2011; Spence Laschinger & Fida, 2014; Van Bogaert et al., 2014).
In addition to policies that support positive changes in nurses’ work environments, health systems must provide occupational health resources to individual nurses that foster self-care and resilience in the practice setting. Nurses skilled in exercising self-reflection, self-care, and self-discovery are well-equipped to manage complex clinical dilemmas with emotional resilience, leading to higher quality care for patients (Quinn, 2014). Focusing on self-care strategies to prevent burnout and enhance resilience is not new; conceptual models that emphasize self-care and health promotion models to prevent burnout can be found in the medical, nursing, and allied health literature (Christopher & Maris, 2010; Dunn, Iglewicz, & Moutier, 2008; Kearney, Weininger, Vachon, Harrison, & Mount, 2009; Kravits, McAllister-Black, Grant, & Kirk, 2010).
Mind-body practices are a clear strategy for nurses to manage stress and build emotional resilience, according to a recent critical review of the literature (Smith, 2014). Nurses in a variety of specialty areas have reported improved outcomes after implementing mind-body techniques over time. Medical-surgical nurses participating in a mindfulness training program reported less burnout and stress than their controls after a 10-week intervention; in addition, the experimental unit reported higher patient satisfaction than the control unit during the same time period (Horner, Piercy, Eure, & Woodard, 2014). In addition, nurses working on a pediatric intensive care unit and practicing a 5-minute mindfulness-based intervention on the job reported less stress and burnout over time (Gauthier, Meyer, Grefe, & Gold, 2014).
One specific mind-body intervention with demonstrated benefits for wellness, self-care, and health promotion is yoga (Chapman & Bredin, 2011; Kumar, 2013; Yang, 2007). A study of mental health counselors confirmed the value of yoga and other mind-body practices to increase self-care during counselor training (Christopher, Christopher, Dunnagan, & Schure, 2006). Although yoga studies among nurses are rare, one study reported the potential for yoga to improve nurse and patient outcomes (Raingruber & Robinson, 2007). In this study, a sample of nurses practicing at an academic medical center described increased self-awareness, as well as enhanced problem-solving and ability to focus on patient needs after participation in a 3-month self-care yoga-based intervention (Raingruber & Robinson, 2007).
Further research is necessary to support the benefits of yoga, both for patients and nurses, who represent the nation’s largest health care profession (U.S. Department of Health and Human Services, Health Resources and Services Administration, 2010). Strong theoretical support for the value of self-care in promoting emotional resilience and an enhanced capacity for stress management and clinical decision making merits the investigation of yoga and other mind-body practices as an avenue for health promotion among nurses and other health care professionals. The purpose of the present study is to examine the efficacy of yoga to improve self-care and reduce burnout among nurses practicing at an urban, tax-supported health care network.
Method
To achieve the study purpose, the research team adopted an experimental study design; a randomized controlled trial consisted of 8 weeks of supervised yoga instruction for the intervention group and usual care for the control group. The Institutional Review Board (IRB) at the affiliated university approved the study. Written informed consent was secured from participants prior to study enrollment.
Institutional Support
An urban 560-bed teaching hospital was contacted to host this yoga research study. This hospital employs about 1,750 nurses practicing in a wide variety of settings—inpatient, outpatient, case management, and nurse informatics among other areas. Nursing administration and the Human Resources (HR) departments were contacted to initiate this possible collaboration, recruiting nurses, securing space, and obtaining approval from the hospital IRB for the research study. Support from nursing administration was important because the target population for the study was nurses. The chief nursing officer was very supportive of the study, and a nurse representative from nursing administration served as the main contact and liaison between the hospital and the university. The responsibility of this nurse representative was to communicate with the nurses, recruit participants, facilitate the IRB approval process, and arrange rooms for the yoga sessions.
As a key stakeholder in the development of the study protocol, the HR department recognized the importance of employee health and wellness. HR leadership welcomed the research study as a means of exploring the receptivity of staff nurses to yoga practice as a wellness initiative for the future. In particular, HR staff expressed interest in applying the findings of the study and participant recommendations to the organization’s wellness program for all hospital employees.
Another key stakeholder was the Environmental Services department. The liaison from Nursing Administration contacted the Environmental Services staff to allocate a space large enough to accommodate 20 participants for the yoga group. Environmental Services also committed to a weekly schedule for cleaning and preparation of the space.
Recruitment
Recruitment focused on nurses within the partner hospital system. Primary recruitment strategies included distribution of email advertisements to all health care provider staff, as well as flyer distribution to work and break areas. Advertising for the study was also conducted through the company intranet and employee portals. The partnership with administration was integral to recruitment. Hospital administration met with managers and supervisors of eligible units to provide information about the study and to encourage managers to share information with employees at regularly scheduled staff meetings.
Contact information for research personnel was provided on the recruitment flyers and all electronic communication. Interested individuals were encouraged to contact research personnel to complete a short online screening survey consisting of questions about job title and job duties, demonstrate willingness to complete eight weekly sessions of yoga, and provide contact information for monitoring. After ensuring the potential participant met the initial eligibility criteria of being a nurse within the partner hospital system, a member of the research team made contact via phone. Over the phone, the research personnel screened potential participants to assess additional inclusion criteria: no prior experience with yoga practice, willingness to complete eight weekly sessions and homework exercises, and willingness to be randomly assigned to the research or control group. In addition, the investigators screened for exclusion criteria: serious illness or major orthopedic diagnoses of the neck, back, pelvis, or lower extremities that could interfere with completion of the yoga intervention protocol.
Target recruitment and enrollment was 50 participants, with 25 in each group. This recruitment goal allowed for 10% attrition, with the expectation that 40 participants would complete the study. This assumption was based on a power analysis in g*Power 3.1.7 indicating that for a repeated measures analysis of variance (ANOVA) with interaction effects, a minimum sample of 40 was needed to find significance with a moderate effect size (Cohen’s f = .25), alpha = .05, power = .80, and an estimated correlation among repeated measures of .40 (Faul, Erdfelder, Lang, & Buchner, 2007). Recruitment strategies yielded more than 100 responses, including many hospital employees who were not nurses. Respondents cited a variety of advertising methods that informed them of the study, with email being the most commonly cited method. The initial screening tool yielded 71 nurses within the hospital system. Those possible participants were contacted by phone for further screening to confirm inclusion/exclusion criteria. The phone-based screening identified 49 eligible participants. The recruitment period was intentionally compact to be within a time frame when staff members already knew their schedules, but the scheduling of sessions and conflicting work schedules were a significant challenge for recruiting nurses to participate in this 8-week study.
Following the phone screening, all eligible individuals were asked to complete another online survey which included the consent form, a demographic questionnaire, and core study questionnaires. After individuals completed consent forms and baseline assessments, they were enrolled in the study and randomized to the intervention (yoga) or usual care control group. A total of 54 individuals completed screening; of those, 40 met eligibility criteria and completed the enrollment process, including consent and baseline questionnaires.
Intervention
The yoga intervention was led by an experienced yoga instructor, who is an osteopathic physician in the local community. For more than 27 years, the instructor has provided health promotion services and yoga instruction in the Kundalini tradition through a wellness-based community practice.
The emphasis of the yoga intervention was to provide participants with self-care tools to manage and reduce stress. One of these tools is enhanced self-awareness, helping individuals become more aware of the simple, unconscious, daily activities, and functions that have a cumulative impact on health and well-being. Throughout the day, most individuals’ awareness is focused on activities outside the body while little attention is given to internal sensations and thoughts. Consequently, most bodily functions, such as breathing, are done unconsciously. Conscious awareness of the way in which one sits, stands, breathes, and thinks is crucial to improving the response to mental and physical stress. By teaching individuals how to observe themselves, many bodily and mental functions improve without strenuous or time-consuming exercise or activities (Mehling et al., 2011; Vago & Silbersweig, 2012).
In early yoga sessions, participants learned to become conscious of their breathing. Breathing is both a conscious and unconscious process and therefore gives conscious access to the autonomic nervous system. Inhalation stimulates the sympathetic nervous system, while exhalation stimulates the parasympathetic nervous system. When one inhales, heart rate increases and when one exhales, heart rate decreases. Practicing mindful breathing allows individuals to calm the body and mind immediately, thereby decreasing stress or energizing the nervous system if one feels fatigued or depressed (Burg & Michalak, 2011; Mason et al., 2013).
Throughout the intervention, the instructor taught participants the basics of postural alignment, deep breathing, and monitoring the mind with simple meditations. Each session concluded with deep relaxation. Each participant received handouts for each session to provide further information and a visual reminder of the exercises, the basis for cultivating a home practice. As the series progressed, additional exercises, breathing practices, and meditations were added to expose participants to the wide range of movements that can work not only the skeletal muscles but also other body systems such as the internal organs, nervous system, circulation, and emotions.
Data Collection
Participants completed assessments twice during the study: at baseline and at the end of the 8-week intervention period. For each assessment, participants completed study questionnaires online using the secure Qualtrics survey system. For the baseline assessment, participants completed a demographic questionnaire, the Health Promoting Lifestyle Profile II (HPLP II; Walker & Hill-Polerecky, 1996), the Freiburg Mindfulness Inventory (FMI), and the Maslach Burnout Inventory (MBI; Maslach, Jackson, & Leiter, 1986).
The HPLP II consists of 52 items that measure the frequency of multiple health-promoting behaviors, ranging from physical activity and nutrition to psychosocial health and sleep hygiene. The HPLP II has a test–retest reliability of 0.89 and well-established validity (Walker & Hill-Polerecky, 1996). The FMI is a 14-item scale that measures perceptions of mental openness, acceptance, and curiosity. The measure demonstrates construct validity and good internal consistency with a Cronbach alpha of .86 (Walach, Buchheld, Buttenmüller, Kleinknecht, & Schmidt, 2006).
The MBI consists of 22 items that measure professional burnout across three domains: (a) emotional exhaustion related to work demands, (b) depersonalization when interacting with patients, and (c) personal accomplishment related to attainment of professional goals (Maslach et al., 1986). A meta-analysis of 84 research studies yielded mean alpha estimates ranging from .70 to .80 for each of the three domains (Wheeler, Vassar, Worley, & Barnes, 2011). Considerable evidence supports use of the MBI as a valid measure to assess burnout among nurses (Pisanti, Lombardo, Lucidi, Violani, & Lazzari, 2013; Poghosyan, Aiken, & Sloane, 2009).
Data Analysis
Investigators used the Statistical Package for the Social Sciences (SPSS; Version 20) to calculate descriptive and inferential statistics (IBM, 2014). Initial analyses focused on an exploration of the relationships among demographic variables and baseline measures. Based on the preliminary analyses, a repeated measures multivariate analysis of variance (MANOVA) was conducted. In addition, univariate ANOVAs were used as post hoc tests to interpret significant interactions.
Results
Categorical demographic variable frequencies and percentages as well as means and standard deviations of the continuous demographics are shown in Table 1. Preliminary analyses were conducted to test for significant relationships among demographic variables and for demographic differences between participants in the control and experimental groups. For these analyses, married participants were compared with unmarried participants, and those with children were compared with those without children due to small group sizes within the original variable coding. A series of cross-tabulations with chi-square, Pearson’s correlation, and independent samples t test revealed no significant relationships among the demographic variables. In addition, no significant differences in demographics were found between the control and experimental groups, suggesting that the two groups were similar in demographic makeup and the research team did not need to control for demographic characteristics in the primary analyses. In addition, the demographic variables were tested in relation to the outcome variables at baseline, and no significant relationships were found.
Descriptive Statistics
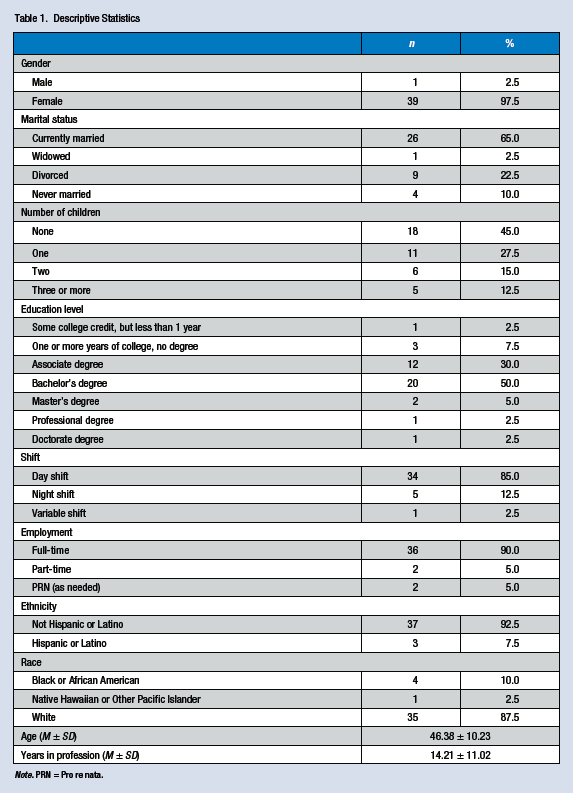
Note. PRN = Pro re nata.
Preliminary analyses did reveal a pattern of significant relationships among the outcomes of interest at baseline (Table 2), suggesting that MANOVA be used to account for the increase in Type 1 error associated with correlated outcomes. Thus, a repeated measures MANOVA (time: within-subjects effect; group: between-subjects effect) was conducted on the outcomes of interest (self-care, mindfulness, and the three burnout subscales, measuring emotional exhaustion, depersonalization, and personal achievement). The results revealed a significant multivariate main effect of time, F(5, 34) = 5.57, p < .001, η2 = .450, and a significant multivariate interaction effect of time by group, F(5, 34) = 2.57, p = .045, η2 = .274, but no significant multivariate main effect of group, p = .270 (Table 3).
Pearson’s Correlation Coefficients Among Scales at Baseline
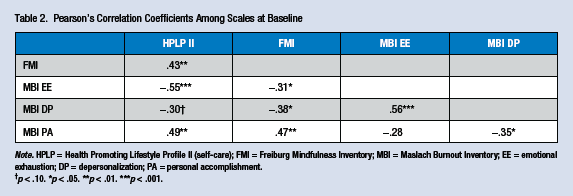
Note. HPLP = Health Promoting Lifestyle Profile II (self-care); FMI = Freiburg Mindfulness Inventory; MBI = Maslach Burnout Inventory; EE = emotional exhaustion; DP = depersonalization; PA = personal accomplishment.
p < .10. *p < .05. **p < .01. ***p < .001.
Means and Standard Deviations for Control and Treatment Scales and Baseline and Posttest With Main Effect and Interaction Statistics
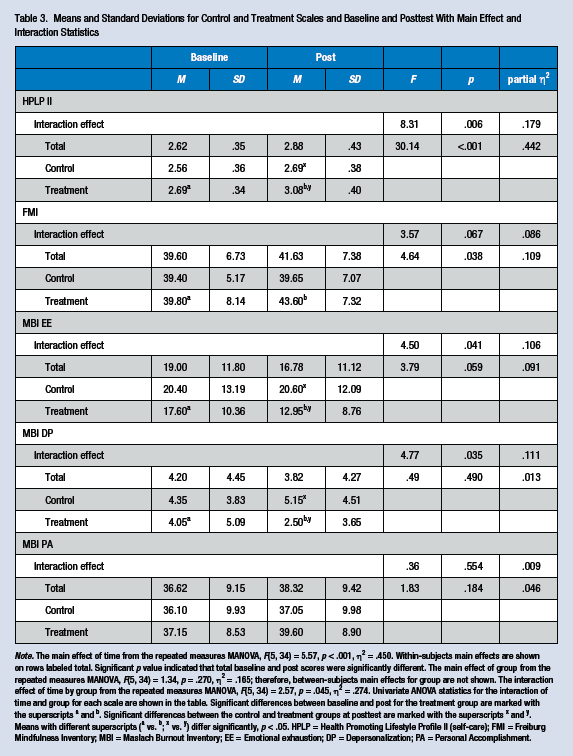
Note. The main effect of time from the repeated measures MANOVA, F(5, 34) = 5.57, p < .001, η2 = .450. Within-subjects main effects are shown on rows labeled total. Significant p value indicated that total baseline and post scores were significantly different. The main effect of group from the repeated measures MANOVA, F(5, 34) = 1.34, p = .270, η2 = .165; therefore, between-subjects main effects for group are not shown. The interaction effect of time by group from the repeated measures MANOVA, F(5, 34) = 2.57, p = .045, η2 = .274. Univariate ANOVA statistics for the interaction of time and group for each scale are shown in the table. Significant differences between baseline and post for the treatment group are marked with the superscripts a and b. Significant differences between the control and treatment groups at posttest are marked with the superscripts x and y. Means with different superscripts (a vs. b; x vs. y) differ significantly, p < .05. HPLP = Health Promoting Lifestyle Profile II (self-care); FMI = Freiburg Mindfulness Inventory; MBI = Maslach Burnout Inventory; EE = Emotional exhaustion; DP = Depersonalization; PA = Personal Accomplishment.
Further investigation of the univariate effects for time revealed that self-care and mindfulness showed a significant improvement from pre- to post- intervention, regardless of group (p < .05). Investigation of the univariate interaction effects revealed a significant time by group interaction for self-care (p = .006, partial η2 = .179), emotional exhaustion (p = .041, partial η2 = .106), and depersonalization (p = .035, partial η2 = .111) scales. In addition, the mindfulness measure showed a marginally significant interaction (p = .067) with a moderate effect size of partial η2 = .086. Figure 1 shows the pattern of relationships for these four outcomes. Analysis of the simple effects revealed that the yoga group showed a significant improvement in scores from pre- to post-intervention for self-care (p < .001), mindfulness (p = .028), emotional exhaustion (p = .008), and depersonalization (p = .007) outcomes. No significant improvement from pre- to post-intervention on any outcomes was found for the control group. Analysis of the simple effects also revealed that at posttest, the intervention group had significantly better scores than the control group for self-care (p = .003), emotional exhaustion (p = .028), and depersonalization (p = .048) scores. No significant differences between the intervention and control groups were found at baseline (p > .05). Tests of normality revealed slight deviations for the MBI depersonalization and personal achievement subscales (particularly in skewness); therefore, all analyses on these measures were confirmed with nonparametric analyses, and similar results were found in all cases.
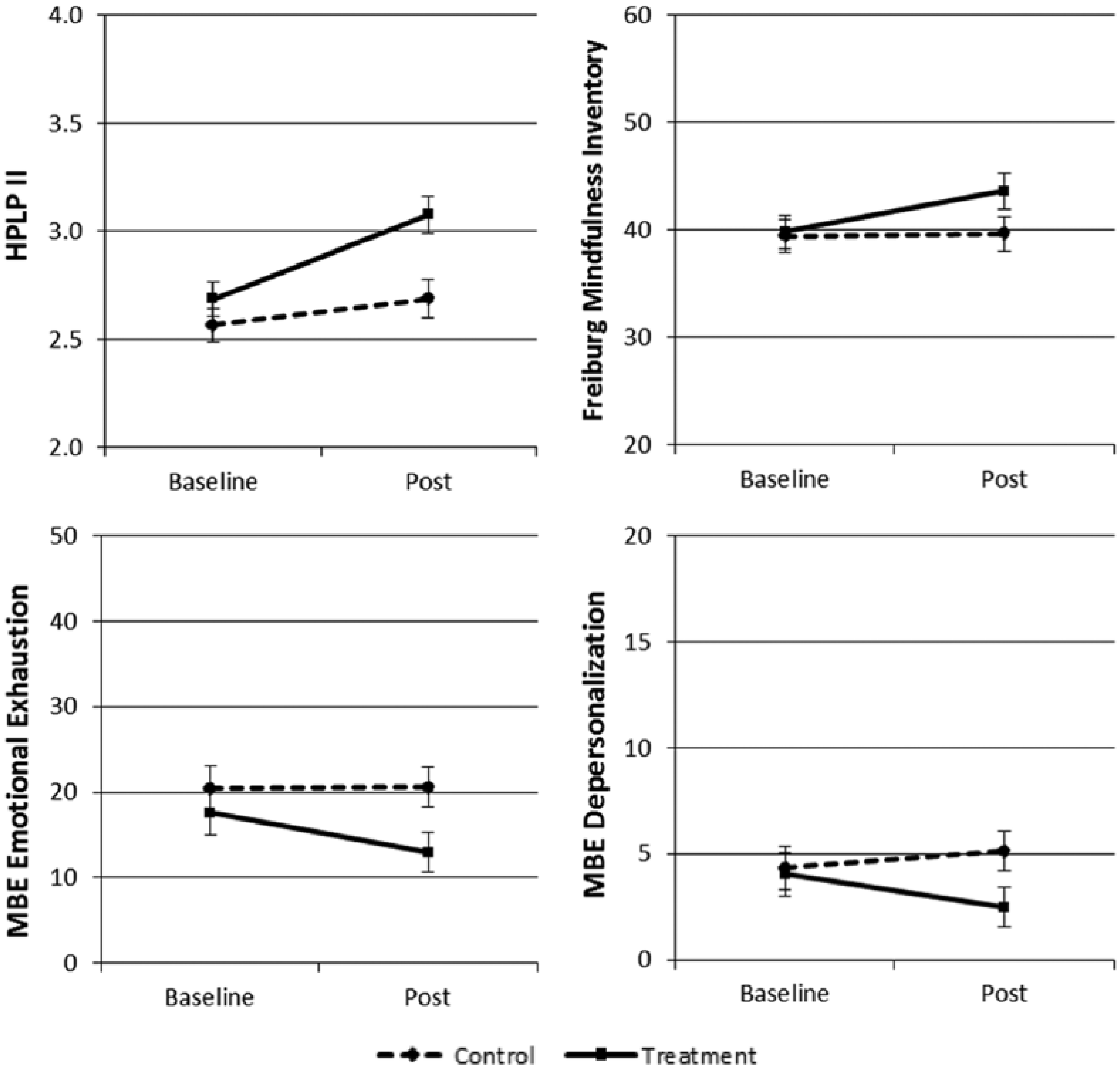
Baseline and post means with standard error bars for treatment and control groups.
Discussion
Findings from this exploratory study provide early, pilot-level evidence of the efficacy of yoga to improve self-care and mindfulness while reducing burnout among nurses practicing at an urban, tax-supported health network. Compared with controls, the yoga participants reported significantly higher self-care as well as less emotional exhaustion and depersonalization upon completion of an 8-week yoga intervention.
Findings from previous studies (Kravits et al., 2010; Raingruber & Robinson, 2007) support those of the current study, corroborating the premise that yoga practice may be an effective strategy for health promotion among nurses and may lead to a reduction in experiences of burnout.
The limitations of the present study included the small sample size, lack of an active control group, and reliance on self-report measures. To address these limitations in future studies, investigators recommend a targeted recruitment strategy that aligns with the efforts of HR and administration, to secure even greater collaboration and support, yielding a larger pool of staff nurses able and willing to participate. In addition, the use of a comparison group or an active control group would strengthen the study design and determine the impact of yoga, relative to other promising interventions. Objective measures of psychosocial phenomena such as stress or burnout could strengthen the intervention design. For example, previous studies have included measures of cortisol and other biomarkers that correlate with stress and burnout (Galantino, Baime, Maguire, Szapary, & Farrar, 2005; Grossi, Perski, Evengård, Blomkvist, & Orth-Gomér, 2003).
Implications for Occupational Health Nursing Practice
Based on the reported effect size, this yoga-based intervention is promising, but further research is necessary to confirm the findings. Given the potential benefits and the limited risk of offering a gentle yoga program, health care agencies and networks may find a return on investment in terms of employee-level outcomes, including self-care and mental health, and potentially patient outcomes, including safety-related indicators as well as perceived quality of care.
The role of the occupational health nurse is to promote informed decision making among workers, with a focus on occupational hazard prevention and health promotion (American Association of Occupational Health Nurses, Inc, 2012). Occupational health nurses who practice in health care settings can apply the findings from this pilot study when engaging with nurses and other health care professionals, all of whom are at risk of stress and burnout in their practice environments. By emphasizing the potential value of yoga to improve self-care and reduce burnout, occupational health nurses are able to advocate for a noninvasive, nonpharmacological approach to prevention among an at-risk population in the workforce.
Additional research examining the efficacy of yoga practice to influence health outcomes among nurses and other health care professionals could clarify and quantify specific gains from a yoga-based intervention for employee wellness. Future studies may include a design that could support the exploration of a dose-response effect for yoga practice on health and job-related outcomes. In addition, studies with a longitudinal design could enable investigators to examine any long-term benefits of yoga practice in terms of burnout, resilience, and self-care capacity among nurses and other health care professionals.
Applying Research to Practice
A sample of 20 nurses who practiced yoga as part of an 8-week intervention reported greater self-care and mindfulness at the end of the study compared with 20 controls. In addition, yoga participants reported less emotional exhaustion and depersonalization, two chief components of burnout. Although more research is necessary to confirm these findings, the potential value of yoga for the occupational health and wellness of nurses is clear.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Research and Creative Activities Fund of Texas Christian University.
Author Biographies
Gina K. Alexander is an assistant professor in the TCU Harris College of Nursing and Health Sciences, with a teaching focus on public health nursing. Her research interests include the investigation of complementary and integrative therapies for health promotion.
Kari Rollins, DO, is the director of The Wellness Center in Fort Worth Texas, an integrative health center for the promotion of health and prevention of illness. In her practice she combines the wisdom of ancient medicine with cutting edge technology. She has been teaching yoga as part of her medical practice since 1981.
Danielle Walker is a lecturer in the TCU Harris College of Nursing and Health Sciences. Her research interests include nursing education and intervention based research.
Lily Wong is a nursing director at JPS Health Network, a public teaching hospital. She is responsible for nursing practice, ensuring clinical practices are in compliance with state and all regulatory agencies rules and guidelines. She collaborates with other disciplines/departments to achieve quality patient care.
Jacquelyn Pennings is a statistician at Elite Research. She plans and conducts statistical analysis for many research and grant projects.