
Abstract
A 41-year-old male manufacturing engineer had a spinal cord injury after being thrown from the horse he was riding and landing on his neck. His injury was a C5 fracture with complete lower limb and trunk paralysis and partial upper limb paralysis. He was transported to the emergency department and eventually to rehabilitation. This article describes this employee’s return to work.
Keywords
E.B., a 41-year-old athletic male, worked as a manufacturing engineer in a consumer goods manufacturing facility. After work, he would often ride his horse on trails near his home. During one of his after-work rides, he started descending a rocky downhill section. On this particular day, the horse stumbled and then took off running. At the bottom of the hill, the horse suddenly stopped, throwing E.B. over the horse’s head onto his neck. He immediately was unable to move his arms or legs. He was taken by ambulance to a trauma center where he was diagnosed with a C5 fracture and anterior cord syndrome (ACS).
Five days after injury, his neurosurgeon performed anterior corpectomy stabilization. He remained in the hospital for several weeks before transfer to a step-down unit and eventually rehabilitation. During this time, he learned to feed himself, to brush his teeth, to comb his hair, and other activities of daily living. He progressed as expected through rehabilitation. Three months after surgery, E.B. was discharged and began a real life rehabilitation program at home. At home, rehabilitation consisted of assisted bathing and a bowel and bladder control program. Once he transitioned to life at home, bowel and bladder control was established. After he gained bowel and bladder control, a return-to-work plan was established.
After 5 months of medical leave, a job analysis was completed by his manager in preparation for return to work. E.B. worked in an office and on the manufacturing floor. He was responsible for organizing production meetings and discussing technical information. Essential functions of his job included use of the computer, data analysis, preparing presentations and spreadsheets, and answering the telephone. Much of the essential functions of his job were intellectual and knowledge based, compiling information and delegating work to staff. Physical requirements were minimal and non-essential to his job. A return-to-work team consisting of the employee, Occupational and Environmental Health Services, the physician, Human Resources, Safety and the employee’s manager was established internally to understand E.B.’s needs. The return-to-work team collaborated with E.B. and community providers to establish his return-to-work plan.
After the return-to-work plan was established, E.B. requested a practice run to work prior to his actual return-to-work date, allowing him and the return-to-work team to assess how his wheelchair would work in his office and how he would move around the manufacturing floor. This pilot return-to-work also informed E.B. and the team about the barriers and obstacles that needed to be addressed before he actually returned to work. Senior management was made aware of the practice run.
E.B. drove himself to work in a van outfitted for his electric wheelchair. He was provided a designated parking space. After completing the practice run, E.B. requested his office flooring be changed from carpet to tile as the wheelchair tires twisted and dislodged the carpet tiles. He also requested a shelving unit in the handicapped bathroom stall for placement of his catheter supplies. A fracture bedpan was available and an extra pair of pants was stored in the clinic. E.B. initially requested voice-activated computer software but decided he would try typing with two fingers as he had typed with two fingers prior to his injury. Plans for fire drills, alarms, and auto dysreflexia especially during an outside drill or building evacuation were discussed. Medications to assist with autonomic dysreflexia were also discussed. E.B. stated his stamina declined after half a day so he returned to work part-time for the first 2 weeks. He maintained a cheerful, thoughtful, and pleasant attitude about return to work. E.B. was back to work full-time 6 months after his accident.
Facts and Statistics
According to The University of Alabama National Spinal Cord Injury Statistical Center (2015), approximately 276,000 individuals with spinal cord injuries live in the United States. Spinal cord injuries occur mainly in men (80%) and the average age at injury in 2010 was 42 years. Although likely underreported, 12,500 new injuries are reported each year in the United States. Health-related expenses for an individual with tetraplegia in the initial year range from US$348,000 to over US$1 million. These expenses vary in each subsequent year according to the location of the injury but range from approximately $42,000 to US$180,000 or more. These expenses increase with higher cervical spine injuries.
In the United States, motor vehicle accidents are the primary cause of spinal cord injuries followed by falls, acts of violence (e.g., gunshot wounds), and sports-related injuries. According to The University of Alabama National Spinal Cord Injury Statistical Center (2013), more than 58.1% of these individuals are working at the time of the injury, but 1 year post injury, only 12% remain employed. One third of these individuals will be employed 20 years after a spinal cord injury.
The Spinal Cord
The spinal cord is housed within the rigid bones of the vertebrae making up the backbone. The spinal cord is composed of 31 pairs of spinal nerves aligning with each vertebrae of the back on the right and left sides of the body that carry messages from the brain to the body. Each of these nerves weaves its way into the muscles and tissues to all other body parts. The spinal cord and backbone are divided into five sections: cervical, thoracic, lumbar, sacral, and caudal equinis.
After a spinal cord injury, the individual’s movement depends on the location of the injury, type of injury, previous and current health status, and complications that may arise during treatment and rehabilitation.
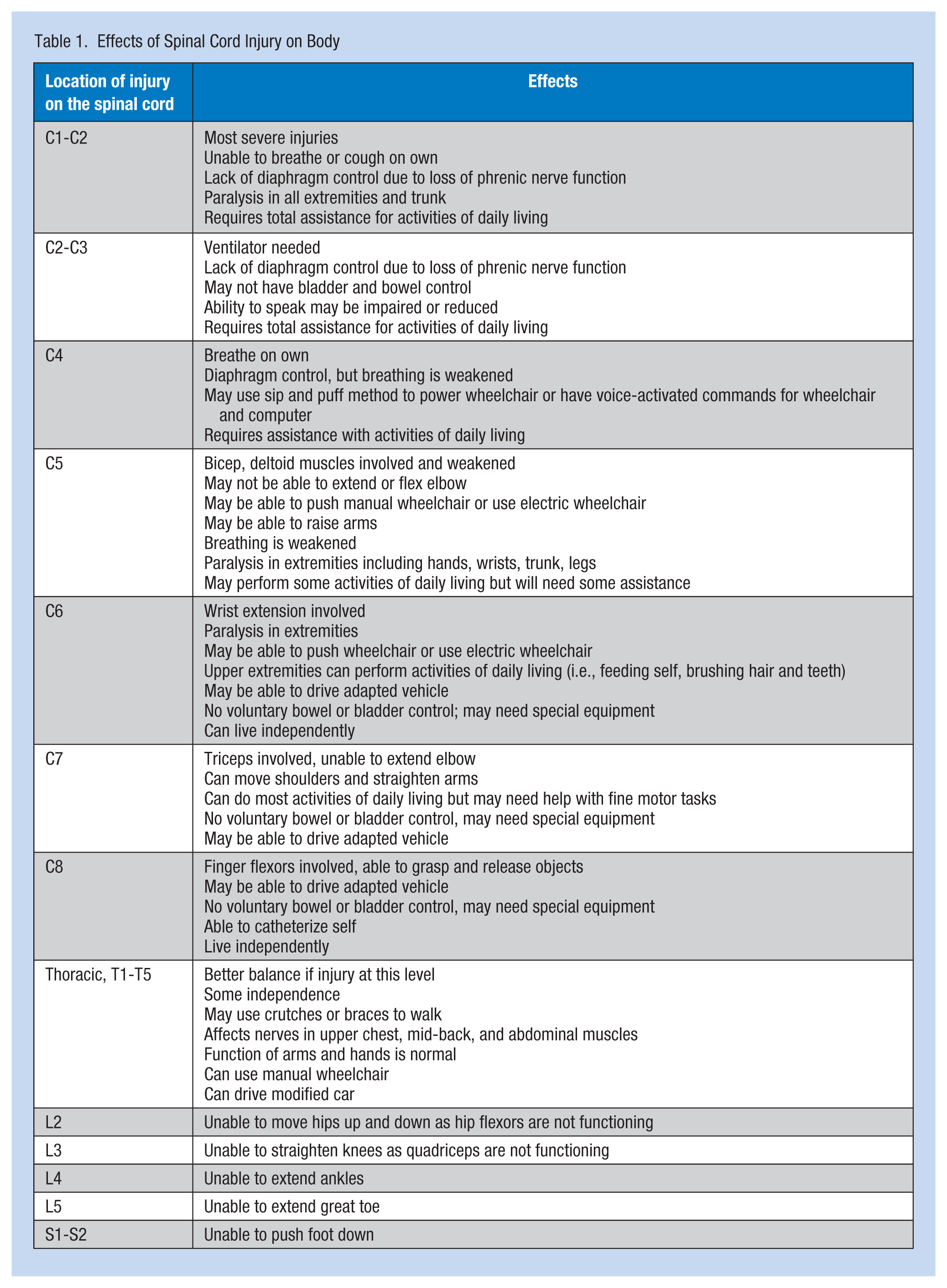
Below the level of the injury, some muscle control and sensory function may be present. Greater dysfunction is experienced when the injury is higher on the spinal cord. According to the Shepherd Center (2015) and The Rehabilitation Institute of Chicago (1990), some effects of spinal cord injury are listed in Table 1.
Effects of Spinal Cord Injury on Body
ACS
Beck (1952) and Schneider (1959) initially described ACS. Weerakkody (2015) explained that ACS, also known as Beck’s syndrome, is caused by ischemic injury and occlusion to the anterior spinal artery and injury to the anterior portion of the spinal cord. The cause of this trauma includes atherosclerosis, aortic pathology (i.e., aneurysm, thrombosis, dissection, or surgical causes), external compression from herniated disc, neoplastic mass, posterior osteophyte, and kyphoscoliosis (Weerakkody, 2015). McKinley (2007) noted that ACS has the worst prognosis and a high mortality rate with poor functional outcomes because recovery of muscle movement and muscle coordination is hampered by the injury.
Complications of Tetraplegia
A number of complications accompany tetraplegia; the occupational health nurse must be aware of these complications in anticipation of the employee returning to work. The Mayo Clinic (2015) lists the following as potential complications for tetraplegia employees.
Bladder Control
The risk of urinary tract infections, kidney infections, kidney stones, or bladder stones is greater for the tetraplegia because the brain no longer communicates the need to empty the bladder so urine is stored. Proper techniques for emptying the bladder are taught during rehabilitation. In the workplace, the employee may need a clean surface such as a shelf in the bathroom for supplies.
Bowel Control
Employees will also learn bowel control in the rehabilitation phase of recovery. The gastrointestinal tract functions as it did prior to the injury. Diets high in fiber help to regulate bowel movements. The occupational health nurse can educate the employee on a high fiber diet. To be prepared for the tetraplegia employee, a fracture bedpan and extra pants should be stored in the clinic.
Skin Sensation
The employee with tetraplegia has a greater chance of developing pressure sores because the skin no longer receives messages from the brain and has lost sensation. The employee may not be able to sense changes in hot, cold, or pressure. In rehabilitation, the employee will be taught to change positions frequently to prevent pressure sores.
Circulatory System
The employee will be taught how to prevent circulatory complications while in rehabilitation. It is necessary for the occupational health nurse to be aware of both orthostatic hypotension (low blood pressure from swelling of the legs) and autonomic dysreflexia (a life-threatening rise in blood pressure) as complications for the employee with tetraplegia. Another circulatory problem may be formation of blood clots due to lack of muscle tone.
Respiratory System
The diaphragm, chest, and abdominal muscles may be affected after a spinal cord injury causing dyspnea or coughing. Higher level injuries, in the cervical and thoracic spine, can increase the employee’s risk for pneumonia and other lung problems.
Muscle Tone
The employee’s legs and arms may spasm at times or become flaccid. This response is caused by the uncontrolled tightening of muscle groups. The muscles may also become flaccid at times due to the inability to control them.
Fitness and Wellness
The employee with tetraplegia is more at risk for cardiac disease, obesity, and diabetes due to sedentary lifestyle and limited mobility. The occupational health nurse can work with the employee and external providers to develop an exercise program suitable for the employee’s abilities and needs.
Sexual Health
Due to the level of injury, many aspects of sexual function may be limited or impaired. The occupational health nurse can educate and support employees as they work through this issue.
Pain
Some employees with tetraplegia may experience pain whereas others may not be able to sense pain. The inability to sense pain becomes especially significant when gastrointestinal disturbances or other organs within the abdominal cavity are inflamed and the employee cannot sense the pain level.
Depression
Tetraplegia is a major life-altering event and depression may follow. The employee assistance program counselor can provide therapy sessions and refer to providers for medications. The occupational health nurse can also play a role in building rapport and assessing employees for mental health concerns.
Heat and Cold
Because a tetraplegic body cannot send messages to the brain about heat or cold, the employee may not be able to discern temperature. The occupational health nurse should initiate a plan for the tetraplegia employee during building evacuations. Fire drills requiring evacuation of the building on a hot summer day can cause the employee with tetraplegia to overheat quickly. The nurse can assign a safety team member as a buddy for the employee with tetraplegia and use an umbrella to shade the worker, put a wet towel over the tetraplegia employee’s head and neck to encourage evaporation, or shelter in place until the ambulance arrives. During the winter months, the employee with tetraplegia should shelter in place at an entrance until ambulance personnel can move the employee to a safe location.
The occupational health nurse can also assist the employee with tetraplegia in the grieving process. Grieving is a natural part of injury recovery and new life process. By providing on-site counseling and community referral, the employee can continue a healthy journey of recovery.
Autonomic Dysreflexia (Hyperdysreflexia)
Autonomic dysreflexia is a life-threatening condition that only affects individuals with spinal cord injuries. Workers with a T6 fracture and above are the most vulnerable to this condition, but rarely, lower thoracic injuries can also contribute to this condition. Autonomic dysreflexia occurs after the nerve pathways have been destroyed and the body no longer communicates sensations or irritations (Sci-Info-pages, 2002-2015). Some examples of sensations or irritations that can cause the autonomic dysreflexia response are a full bladder, restrictive clothing, keys in a pocket pushing on a hip, sunburn, fecal impaction, or abdominal pain.
The body’s normal response to an irritation is to send a signal to the brain communicating what is wrong. With destroyed nerve pathways, this communication cannot take place and the information is blocked. The body reacts to the irritation or the sensation by constricting blood vessels causing blood pressure to rise. When the body is signaled that the blood pressure is too high, the body slows the heart rate and then dilates the blood vessels to increase blood flow; the brain stops constriction of the leg blood vessels and abdomen. If the situation is not corrected, the blood pressure will continue to rise causing seizure, stroke, and death.
The employee may have medications to alleviate the hypertension. Medications may be used for autonomic dysreflexia if the condition persists after removal of the irritant (Table 2).
Medications to Reduce Blood Pressure After Automonic Dysreflexia
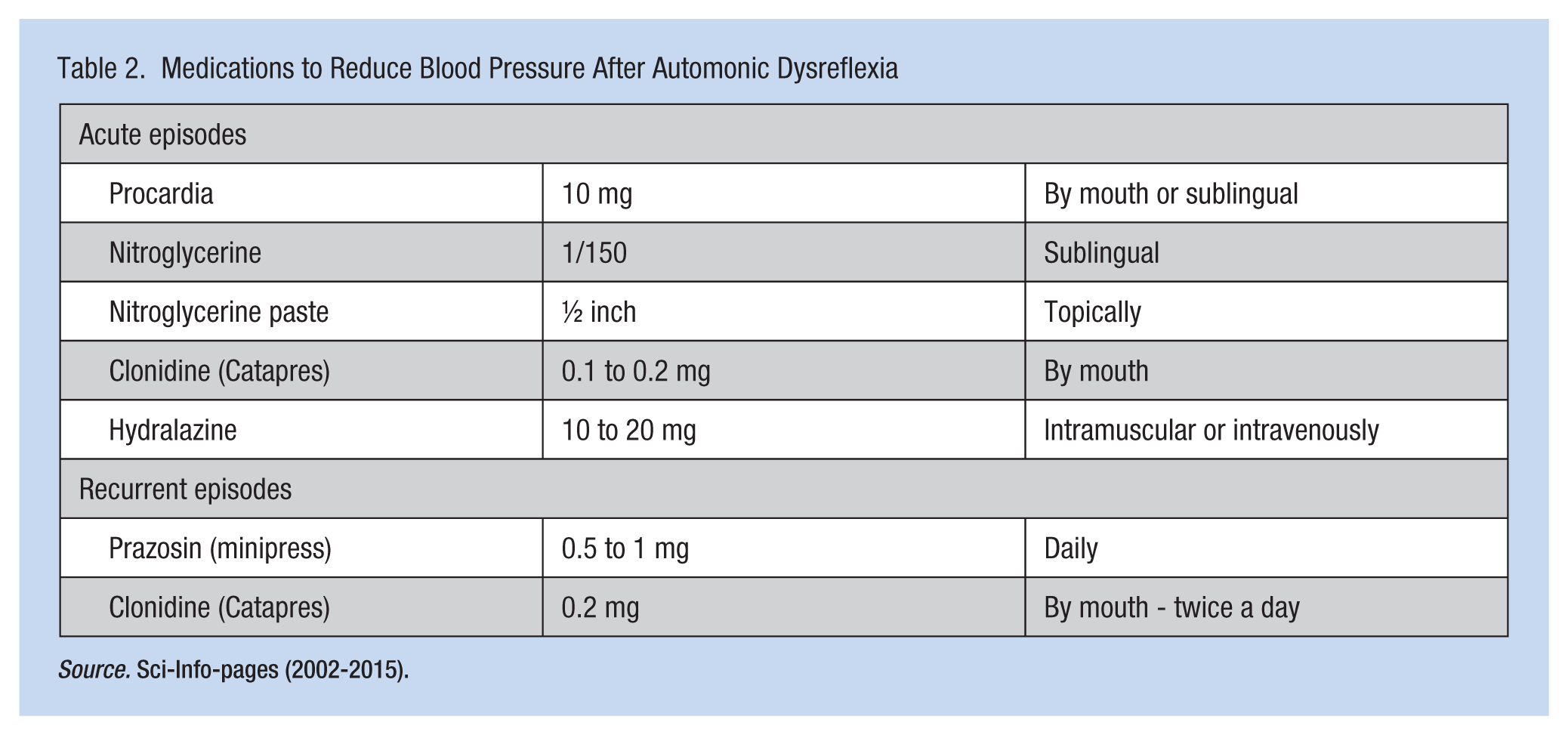
Source. Sci-Info-pages (2002-2015).
Implications for Practice
Occupational health nurses must understand the etiology and complications of spinal cord injury. Complications may present symptoms that warrant a quick assessment by the nurse to determine whether a life-threatening condition exists.
The occupational health nurse must also actively listen to the employee’s suggestions so reasonable accommodations can be implemented in the workplace. The occupational health nurse can assist the worker in making accommodations and can educate the worker about accommodation options. But most importantly, the occupational health nurse can assist the employee with tetraplegia feel comfortable and accepted in the workplace.
Conclusion
An employee with a spinal cord injury such as tetraplegia returning to work requires thoughtful consideration regarding the employee’s and the employer’s needs. Building rapport with the employee throughout the entire hospitalization and rehabilitation process supports an easier transition back to work. E.B. found taking charge of a “practice run” to the workplace helped him identify obstacles that could interfere with productivity and comfort. Obstacles addressed were changing the floor material in his office, placing a shelf in the bathroom, purchasing an appropriate bedpan, discussing expectations during fire drills, and understanding the potential for autonomic dysreflexia during building evacuations. E.B. decided against using a computer voice-activated system and instead typed with two fingers, adapted to existing processes within the computer programs he had used prior to the accident. Accommodations were addressed and E.B. was welcomed to return to full-time employment.
Resources:
Job Accommodation Network
National Spinal Cord Injury Association
Paralyzed Veterans of America
SCI-Info-Pages
The National Spinal Cord Injury Association
National Institute on Disability and Rehabilitation Research (NIDRR)
www2.ed.gov/about/offices/list/osers/nidrr/about.html
The University of Alabama National Spinal Cord Injury Statistical Center
Footnotes
Acknowledgements
The author thanks Corranda Kosciolek, FNP-BC, PhD-c.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Letha Smith is an occupational health nurse in Irving, Texas, and is a member of the North Texas Association of Occupational Health Nurses.