
Abstract
This article reports on a literature review of workplace interventions (i.e., creating healthy work environments and improving nurses’ quality of work life [QWL]) aimed at managing occupational stress and burnout for nurses. A literature search was conducted using the keywords nursing, nurses, stress, distress, stress management, burnout, and intervention. All the intervention studies included in this review reported on workplace intervention strategies, mainly individual stress management and burnout interventions. Recommendations are provided to improve nurses’ QWL in health care organizations through workplace health promotion programs so that nurses can be recruited and retained in rural and northern regions of Ontario. These regions have unique human resources needs due to the shortage of nurses working in primary care.
Occupational stress is due to work situations that place demands on workers; nurses’ inability to meet work demands can lead to illness or psychological distress (Edwards, 2003). Occupational stress is a major health problem for both employees and organizations, and can lead to burnout, illness, labor turnover, and absenteeism. Occupational stress can also be a barrier to recruiting and retaining workers (Bartram, Joiner, & Stanton, 2004).
Healthy work environments are vital to the retention and recruitment of health care professionals and the sustainability of health systems (Pino & Rossini, 2012). Health care organizations must control costs and increase productivity while responding to increasing demands from a growing aging population (Schalk, Bijl, Halfens, Hollands, & Cummings, 2010). A clear understanding of the nursing workforce is essential prior to developing recruitment and retention strategies.
According to the World Health Organization (2014), a global shortage of 7.2 million health care workers exists. This shortage is expected to increase to 12.9 million by 2035 (World Health Organization, 2014), and is especially pronounced for the nursing profession, which is the largest group of health care professionals in hospitals, one third of the Canadian health care workforce; approximately 6 in 10 Canadian nurses work in hospitals (Canadian Federation of Nurses Unions, 2013). Nurses’ work environments in Canada have received attention due to high absenteeism and staff shortages, augmented by dramatic cutbacks in funding and restructuring of health care services in the 1990s (Schalk et al., 2010). The Canadian Federation of Nurses Unions reported that 86% of nurses found their workplaces stressful and understaffed, 88% said they were under-resourced at work, and 91% experienced heavy workloads (Greenslade & Paddock, 2007).
In Canada, approximately 95% of the country’s land mass is rural and remote (Fierlbeck, 2011). Registered nurses (RNs) provide care to approximately 6.6 million (21.7% of Canadians) individuals living in rural and remote areas (Canadian Federation of Nurses Unions, 2013). However, the nature of nurses’ clinical practice in rural, remote, and northern regions of the country is poorly understood (Stewart et al., 2011). RNs are often overworked (Canadian Federation of Nurses Unions, 2013). Moreover, if the health needs of Canadians continue to change based on current trends, Canada will need an additional 60,000 full-time equivalent RNs by 2022 (Canadian Nurses Association, 2012). However, little is known about the determinants of a positive work environment in rural and northern settings (Penz, Stewart, D’Arcy, & Morgan, 2008).
Regrettably, the constant undersupply of RNs, recruitment challenges, and low retention rates limit northern and rural residents’ access to health services (Dotson et al., 2011). Access to services may even be eliminated in communities that do not have sufficient RNs to deliver health services, or residents may have to travel long distances to receive care (e.g., oncology services).
As the Canadian workforce ages, the overall health of nurses may decline, challenging the profession to adequately care for the health of the public. Today, Canadian nurses are often 30 years or older when they graduate from nursing programs and begin their nursing careers (Canadian Institute for Health Information, 2009). In 2009, most nurses practicing in Canada were 40 to 59 years old; nurses in this age group constitute 57.1% of the RN workforce in Canada (Canadian Institute for Health Information, 2009). In 2011, the average age of a Canadian RN was 46 years (Canadian Federation of Nurses Unions, 2013; Canadian Institute for Health Information, 2013).
To date, research has focused largely on occupational stress (Malik, 2011; Opie et al., 2010; Schonfeld & Farrell, 2010; Wu, Chi, Chen, Wang, & Jin, 2010), nurses’ health (Hayes, Douglas, & Bonner, 2013; Smith, Fritschi, Reid, & Mustard, 2013), burnout (Balevre, Cassells, & Buzaianu, 2012; Hanrahan, Aiken, McClaine, & Hanlon, 2010; Jourdain & Chênevert, 2010), work-related injuries (Witkoski & Dickson, 2010), and job satisfaction (Bourbonnais, Brisson, Malenfant, & Vezina, 2005; Eriksen, Tambs, & Knardahl, 2006; Marchand, 2007), issues affecting the nursing shortage. It is clear that nurses continually experience changes in their work roles and functions. A review of nurses’ quality of work life (QWL) should evaluate interventions to mitigate job stress, increase QWL and decrease work absenteeism.
The aim of this review was to evaluate workplace interventions, associated with work environments and QWL, targeting nurses’ occupational stress and burnout. An examination of the current literature focused on nurses’ occupational stress followed by a critical analysis of stress management interventions for nurses and their implications for nurses’ QWL. Similarly, the authors present an overview of the literature pertaining to nurses’ burnout, nurses’ work environments, and prevention interventions.
Method
Databases, PUBMED and CINAHL, were searched to examine workplace interventions, associated with work environments and QWL, targeting occupational stress and burnout for nurses. Primary search terms were “burnout,” “stress,” “nurses,” “QWL,” and “nursing.” To be considered relevant and included in the review, each study (a) evaluated an intervention to mitigate stress or burnout, or bolster QWL; (b) was published in English; (c) was published between 2002 and 2011; and (d) was conducted in a workplace.
Findings
Workplace Stress and Nursing
Occupational health risks, including the risk of musculoskeletal injuries, related to nursing can stem from both physical and mental stress. Furthermore, nurses experience stress related to shift work and irregular hours, unremitting exposure to disease and death, and for some, toxic chemicals and pharmacological compounds (Clegg, 2001; Nelson, Lloyd, Menzel, & Gross, 2003). Occupational stress involves the interaction of work and worker characteristics as well as personal stressors such as family responsibilities, lack of sleep, and personal resources (e.g., conflict-resolution management, health promotion practices) that influence nurses’ appraisal of and coping with workplace situations (Zeller & Levin, 2013).
Concern about potential population health risks and socioeconomic ramifications of a rural nursing shortage have led to investigations about nurses’ intent to leave their positions as an indicator of rural nursing workforce retention in the United States (Dotson et al., 2011); however, similar research in Canada is lacking except for two studies that have examined rural northern Canadian nurses collectively rather than investigating geographic differences (Penz et al., 2008; Stewart et al., 2011).
In a 2011 study, researchers examined factors leading to intent to leave a nursing position in rural remote Canada. Data collected as part of a national cross-sectional mail survey of RNs in rural and remote Canada showed that these nurses were more likely to plan to leave their nursing position within the next 12 months if they had higher self-reported occupational stress, did not have children or relatives, had diminished job satisfaction and less control over their work schedules, were required to be on call and make clinical decisions, worked in remote settings, were male, had higher levels of education, were employed by their primary agency for a shorter time, and had lower community satisfaction (Stewart et al., 2011). Such findings may guide health policy and provide organizations with strategies to augment recruitment and retention. Additional research is warranted because studies often do not consider the geographic differences across rural regions and a single definition of rurality has never been accepted.
Humphreys et al. (2009) developed a logic model for delivering primary health care in small rural remote communities (Daniels, VanLeit, Skipper, Sanders, & Rhyne, 2007). This model emphasized that workforce retention is related to leadership, continuing education and professional development, interdisciplinary teamwork, career opportunities and advancement, effective recruitment, workforce succession planning, and adequate infrastructure (Daniels et al., 2007).
Recruitment strategies and selection criteria are pivotal factors in subsequent retention because the better the match between workers and both their employing organization and worker role, the longer workers are likely to remain, independent of additional retention strategies (Thistlethwait et al., 2007). Arnetz (2006) proposed a theoretical description of the leadership–bottom line performance axis. In this model, leadership was identified as the essential factor in organizational health and employee well-being. Furthermore, resources, including employee skills, motivation, and energy, were found to be mediating variables.
Stress Management Interventions
Occupational stress is a serious threat to health care providers’ QWL and can cause hostility, aggression, absenteeism, and turnover and negatively affect productivity (Mosadeghrad, Ferlie, & Rosenberg, 2011). In a 2005 study, Shapiro and colleagues examined mindfulness-based stress reduction (MBSR) as an intervention for health care professionals. Thirty-eight health care professionals from the United States participated in this randomized control study (Shapiro, Astin, Bishop, & Cordova, 2005). Compared with controls, the intervention (MBSR) group demonstrated a significant mean reduction (27% vs. 7%, p = .04) in perceived stress and an increase in self-compassion (3% vs. 22%, p = .004; Shapiro et al., 2005). Eighty-eight percent of participants in the MBSR group showed improvement in their stress scores, and 90% demonstrated increases in self-compassion (Shapiro et al., 2005). Compared with controls, intervention participants reported greater satisfaction with life (19% vs. 0%, p = .06), less job burnout (4% vs. 10%, p = .21), and less distress (11% vs. 23%, p = .25; Shapiro et al., 2005). This satisfaction with life finding demonstrated potential benefits from a meditation-based intervention for health care professionals (Shapiro et al., 2005). Future studies should use a larger sample and also gather additional data at the 1- and 2-year marks to determine whether long-term benefits occurred. Moreover, future studies should incorporate measures of QWL and its relationship to occupational stress, as well as how social supports outside of the workplace influence work stress. Such undertakings should also better elucidate the relationships between factors outside of the workplace and their influences on workers’ job performance and competencies.
Burnout Intervention Studies
Questions about type and location of employment have prompted other researchers to examine job stress in rural and small urban settings (Pinikahana & Happell, 2004; Tyson, Pongruengphant, & Aggarwal, 2002). Some studies suggest that geography may be a mitigating factor for occupational stress and burnout (Pinikahana & Happell, 2004; Tyson et al., 2002). A cross-sectional study of a convenience sample of RNs (n = 136) working in two psychiatric hospitals in rural Australia revealed that the nurses experienced less burnout on the emotional exhaustion (EE), depersonalization (DP), and personal accomplishment (PA) subscales of the Maslach Burnout Inventory (Maslach, Jackson, & Leiter, 1996). Unlike nurses in urban hospitals and independent of burnout, the majority (66.1%) of rural psychiatric nurses stated they were satisfied with their jobs, particularly with their current work situations, aspects of support (e.g., support from management), and level of involvement in decision-making on their units (Pinikahana & Happell, 2004). These findings did not support the established relationship between high levels of stress and job satisfaction in nurses.
Several explanations for why this relationship was not observed in rural nursing could be hypothesized. Rural and northern residents are unique in culture, health needs, and health behaviors which may be both challenging and rewarding (Lightfoot, Strasser, Maar, & Jacklin, 2008). The cross-sectional design of the study only captured a snapshot of nurses’ views and may not accurately reflect their work environments and occupational stress levels. In addition, the cross-sectional, retrospective nature of the questionnaire could not demonstrate causation. Finally, given the cross-sectional design of the study and the non-rarity of outcomes, multivariate inferential statistical findings may overestimate the effect size compared with relative risk.
In another study, Psychosocial Intervention Training (PSI) was evaluated in terms of its effect on the knowledge, attitudes, and levels of clinical burnout in a group of forensic mental health nurses. The researchers found that nurses in the experimental group significantly gained knowledge and changed attitudes about serious mental illness and significantly decreased burnout (Ewers, Bradshaw, McGovern, & Ewers, 2002). Furthermore, 2 weeks after the intervention, scores between the experimental and control groups showed statistically significant differences on all three Maslach Burnout Inventory subscales (i.e., emotional exhaustion, depersonalization, personal achievement; Maslach et al., 1996). This study suggests such interventions can affect nursing care delivery, nurses’ health, and nurses’ QWL.
In another study, researchers examined the outcomes of a psychosocial intervention for licensed and unlicensed nursing staff working in a low-security mental health unit in the United States (Redhead, Bradshaw, Braynion, & Doyle, 2011). Forty-two nurses (21 nurses in each group) were randomly assigned to experimental and control groups. Knowledge, attitudes, and burnout were assessed before and after the intervention. Furthermore, a random sample of 44 care plans written by the nurses was audited before and after the intervention to examine the effect of the intervention on psychosocial intention in clinical practice. The results demonstrated that licensed and unlicensed nurses in the experimental group showed significant gains in knowledge and changes in attitudes compared with nurses in the control group. Similarly, care plans showed a significant increase in the implementation of psychosocial interventions. The only significant change in burnout was a reduction in depersonalization for licensed nurses in the experimental group. Table 1 summarizes all the study findings.
Summary of Study Findings
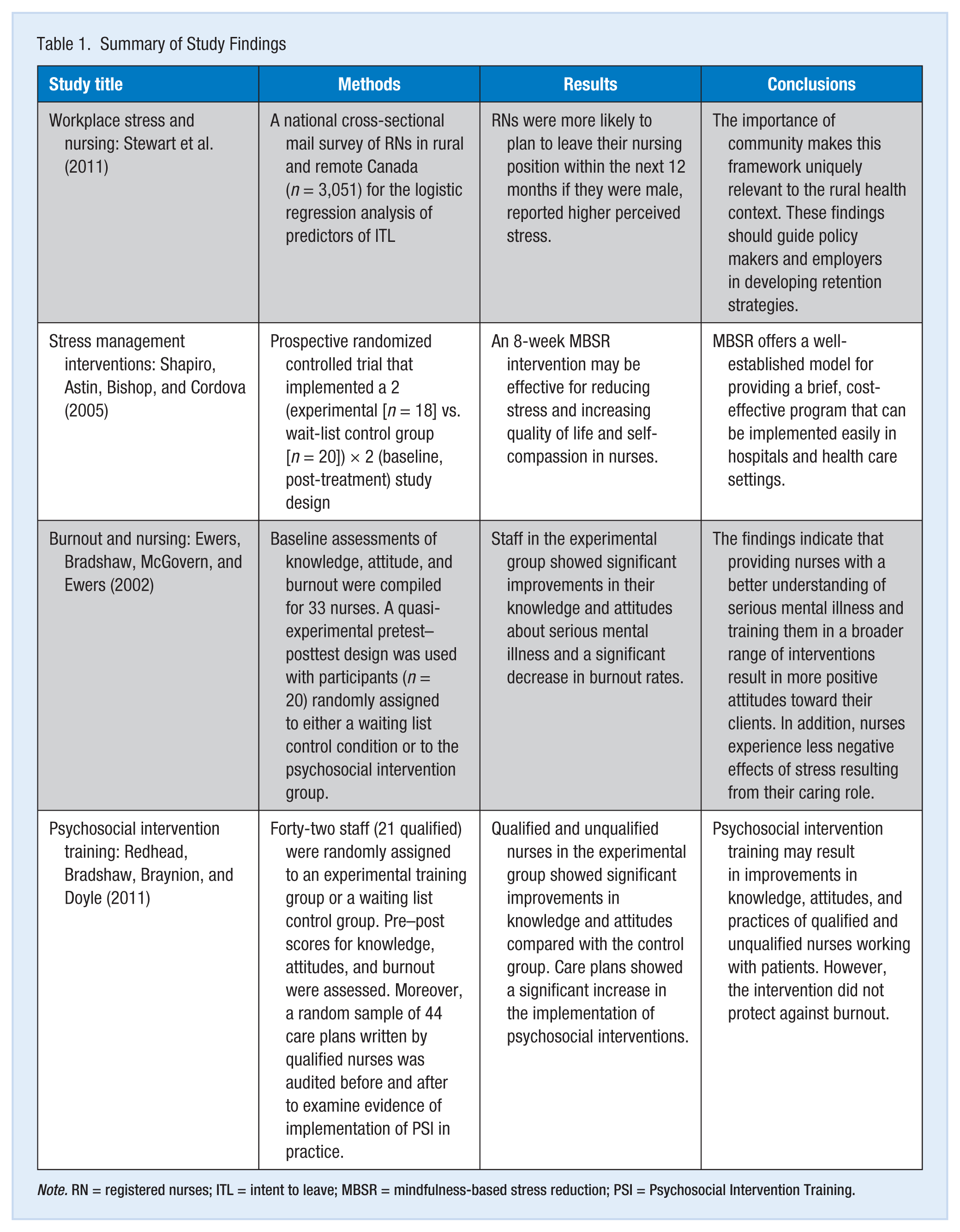
Note. RN = registered nurses; ITL = intent to leave; MBSR = mindfulness-based stress reduction; PSI = Psychosocial Intervention Training.
Discussion
The studies included in this review were all based in workplaces and focused mainly on individual strategies. Occupational stress research often lacks a comprehensive theoretical framework and standardized measurement tools (Webster, Beehr, & Love, 2011), which focus simultaneously on individual and organizational factors (Carson & Kuipers, 1998; Pino & Rossini, 2012).
Management style, incentives and career structures, educational opportunities, salary scales, and recruitment and retention practices were some of the organizational factors that can influence the geographic distribution of health resources (Dussault & Franceschini, 2006; Golubic, Milosevic, Knezevic, & Mustajbegovic, 2009; Simon, Müller, & Hasselhorn, 2010). Any retention strategy should be linked to health service providers’ structures and functions to take advantage of existing partnerships and increase efficiencies. For example, health policy should be directed at upgrading rural health facilities and improving the work environment as part of a national health facility expansion plan (McLean, 2013). This approach provides funding to support the infrastructure that rural northern practitioners require to provide quality clinical care. Conversely, a plan to expand publically or privately funded health services in urban areas may work against new strategies for attracting health care providers to rural areas. Recruitment and retention of nurses may be more successful when hospital administration has an understanding of the perceptions of nurses in northern rural regions.
Recommendations
In Western countries, it is clear that occupational stress can have serious health implications for nurses (Kroenke et al., 2007; Mitchell et al., 2009; Simon et al., 2008). By industry, stress levels are highest in education, health care, and social services sectors (Jackson, 2009). Women are more likely than men to report high stress levels (Jackson, 2009), and because nursing is a female-dominated profession, this finding is of concern. Therefore, properly planned intervention programs that include aspects of both person-directed and organization-directed prevention measures are expected to prevent burnout and improve workers’ mental health. Positive effects can be extended by refresher courses at appropriate intervals after the end of the initial program (Awa, Plaumann, & Walter, 2010).
Future studies should use better designed and evaluated randomized controlled trials, with comparable participants, appropriate baseline data, and at least two post-intervention measurements points (Awa et al., 2010). Many of the studies analyzed in this review had small samples, low retention rates, and short intervention and monitoring durations. Furthermore, they often focused on nurses in larger urban centers and in one nursing specialty. It would be beneficial to examine intervention strategies across nursing specialties and in both urban and rural practice settings.
The authors hope this review fosters future studies that incorporate random assignment to treatment and control groups and report the results of all outcomes. Furthermore, statistically significant findings should be translated into nursing practice. In addition, the continued use of meta-analytic techniques to synthesize research findings should be pursued. As more primary studies are conducted, systematic reviews should be updated to reassess results.
Two issues are vital with respect to evaluating stress management and burnout interventions. First, common measurement approaches would permit investigators to compare studies nationally and internationally. Second, interventions should be more rigorously evaluated.
Effective health policy should incorporate health, cultural and social contexts of occupational stress, and its relationship to QWL. National recognition and support of factors related to job satisfaction and quality work environments may retain nurses working in both rural and urban settings. In particular, identifying occupational barriers that nurses working in rural and remote regions experience is essential. Given the limited number of employment opportunities in these regions, employers and employees must work together to create a positive workplace that fosters career advancement, supports job satisfaction, and increases nurses’ QWL. In terms of policy implications, the recruitment and retention of nurses to northern and rural areas is a serious undertaking for decision makers and planners. Building positive work environments is a crucial component of retaining health care professionals in the north and recruiting those from other regions to move to rural areas for lifestyle and career opportunities.
Policy and practice changes, such as strategies to increase the recruitment and retention of nurses, and organizational initiatives to reduce stress due to staffing and workload issues are needed to improve the quality of services that nurses provide. Canada has many rural remote areas in which nurses are the only professional health care providers. From an occupational health and safety perspective, it is crucial that administrators and health policy makers understand the realities of northern rural nursing practice and the quality of work environments for RNs. National recognition and support of factors related to job satisfaction, and safe quality work environments may retain those RNs working in northern rural communities.
Conclusion
The objective of this literature review was to evaluate workplace interventions associated with healthy work environments and QWL, targeting the management of occupational stress and burnout for nurses. Beyond a geographic lens, studies are needed to develop interventions that respond to social and political changes, new health policies, and economic factors, such as unemployment. The viability of the nursing workforce depends on addressing human resources issues associated with workplace stress and job satisfaction (Stewart et al., 2011). The literature demonstrates that the challenges of rural northern practice, which initially attracts nurses, become a source of occupational stress, job dissatisfaction, lower work ability scores, and absenteeism (Nowrouzi et al., 2014). From a recruitment and retention perspective, it is crucial that administrators and health policy makers foster environments that appreciate the realities of northern and rural nursing practice and uniquely affect the quality of work environments for nurses.
Understanding and evaluating workplace interventions that target the management of stress in the workplace is of importance to nurses’ quality of work life (QWL). Moreover, occupational stress affects not only job satisfaction, but also satisfaction in other life domains including: leisure, family, financial well-being, health, housing, friendships, education attainment, community engagement, neighborhood interactions, spiritual well-being, the environment, and cultural and social status. Additional research is needed to further examine the relationship between QWL and occupational stressors, particularly in rural and northern regions of Ontario, Canada. These may ultimately lead to the development and implementation of QWL programs that are tailored to meet the needs of employees and employers.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Behdin Nowrouzi is a postdoctoral fellow and occupational therapist in the Centre for Research in Occupational Safety and Health, Laurentian University, Sudbury, Ontario, Canada.
Nancy Lightfoot is an epidemiologist in the School of Rural and Northern Health and in the Centre for Research in Occupational Safety and Health, Laurentian University, Sudbury, Ontario, Canada.
Michael Larivière is a clinical psychologist, associate professor in the School of Human Kinetics and in the Centre for Research in Occupational Safety and Health, Laurentian University, Sudbury, Ontario, Canada.
Lorraine Carter is an associate professor in the School of Nursing at Nipissing University, North Bay, Ontario, Canada.
Ellen Rukholm is a senior research fellow at the Centre for Research in Rural and Northern Health, Laurentian University, Sudbury, Ontario, Canada.
Robert Schinke is a professor in the School of Human Kinetics, Laurentian University, Sudbury, Ontario, Canada.
Diane Belanger-Gardner is the former (retired) administrative director of the Family and Child Program at Health Sciences North, Sudbury, Ontario, Canada.