
Abstract
This study examined the effects of a neck stretching exercise intervention on nurses’ primary headaches. Using a pretest and posttest two-group design, a total of 60 female staff nurses employed by a medical center in Taiwan were selected by convenience sampling. Participants in the experimental group (N = 30) practiced neck stretching exercises while experiencing headaches. The participants in the control group (N = 30) managed their headaches as usual. A structured questionnaire was used to collect data on headache intensity at baseline, and at 30 minutes and 1 hour after intervention. Decrease in headache intensity of the experimental group was significantly larger than that of the control group. Neck stretching exercises is an effective method for treating primary headaches.
Researchers suggest that nurses suffer from significant work-related stress (Dollard, LaMontagne, Caulfield, Blewett, & Shaw, 2007; Salilih & Abajobir, 2014). Occupational stress has often been found to cause nurses’ headaches (Hsieh, Chiu, Wang, & Chen, 2011; K. C. Lin, Huang, & Wu, 2007). Researchers have found a high prevalence of primary headaches (i.e., 44%-49%) among nursing staff (Hsieh et al., 2011; K. C. Lin et al., 2007). The impact of headaches includes impaired quality of life and socioeconomic costs (International Headache Society, n.d.; Takele, Haimanot, & Martelletti, 2008). Nurses’ headaches may also affect patient care via work interruptions, disputes with patients, work neglect, increased errors, and poor quality work. These problems can also increase economic costs (Hsu, Lee, Chien, Kuo, & Lin, 2010). Therefore, this study was designed to explore the effect of neck stretching exercises, a natural convenient, non-invasive intervention to reduce nurses’ headaches.
Literature Review
Headaches are classified as primary and secondary. Secondary headaches are caused by disease. Primary headaches are not associated with demonstrable organic diseases or structural neurologic abnormalities (International Headache Society, n.d.; Kunkel, 2010). More than 90% of headaches are classified as primary, including migraine, tension, and cluster headaches. These headaches are episodic and recurrent (International Headache Society, n.d.; Kunkel, 2010).
Static stretching involves slowly stretching muscles beyond their normal length and maintaining the stretch for a few seconds, increasing the length of the muscle, muscle flexibility and range of motion, inhibiting muscle spasms, decreasing muscle tension, and enhancing muscle strength, which, in turn, relieves pain (M. M. Chen, Lee, Chuang, & Chen, 2008; da Costa & Vieira, 2008; Marques, Vasconcelos, Cabral, & Sacco, 2009). Neck static stretching is a gentle, low intensity, safe, slow stretch (C. H. Chen & Chen, 2007). The exercises can be performed without equipment and only take a few minutes, including during breaks at work, to minimize tightness and decrease the potential for tension headaches (Behar, 2013).
Some studies show that stretching exercises can prevent or reduce pain, prevent sports-related injuries (da Costa & Vieira, 2008), and reduce lower back pain and chronic disability (M. M. Chen et al., 2008). Stretching exercises also can reduce neck pain, related disability, and headaches (Kay et al., 2012; Ylinen, Kautiainen, Wirén, & Häkkinen, 2007). Ylinen et al. (2007) compared the effects of a 4-week manual therapy and a stretching exercise program on neck pain, disability, and headache. They found a significant decrease in neck pain, disability, and headache in both groups after 4 weeks.
Ylinen, Nikander, Nykänen, Kautiainen, and Häkkinen (2010) examined the effect of neck exercises on cervicogenic headache during a 12-month training program and later monitoring. They found that headaches and pain in the neck and upper extremities in the strength-training group decreased significantly compared with baseline values. Thus, strong support exists for stretching exercises to be recommended as an appropriate intervention to relieve pain (Ylinen et al., 2010).
In the previous literature, stretching exercises were performed by holding the stretched position for 5 seconds to 30 seconds (Behar, 2013; da Costa & Vieira, 2008; Zakas, 2005). Zakas (2005) examined the effects of static stretching duration. The first stretching protocol was performed once for 30 seconds, the second was performed twice for 15 seconds, and the third was performed six times for 5 seconds. The results indicated a significant improvement in flexibility after all stretching exercise protocols (Zakas, 2005). Because few studies have explored the effect of neck stretching exercises on nurses’ primary headaches, this study was designed to explore this effect.
Method
Study Design/Sample Selection
A pretest–posttest two-group design was used in this randomized study. Nurses who met the inclusion (i.e., aged 20-60 years and self-reported primary headaches at least once in the previous 4 weeks) and exclusion criteria (i.e., headache diagnosed as a specific disorder or diagnosed pathological headache; possible secondary headache symptoms including neurological symptoms or signs, a suddenly occurring headache accompanied by rapid deterioration, original headache frequency, intensity, time history, and/or characteristic change [Dodick, 2003]; and cognitive disabilities or a history of mental illness) were recruited from a medical center in southern Taiwan (Figure 1). The sample size was predetermined by using power analysis based on the power of 0.8, an effect size of 0.30 (Ylinen et al., 2007), and a = 0.05; 30 participants in each group were determined to be adequate to test the study’s hypothesis. In total, 60 nurses consented to participate in this study. The 60 participants were assigned numbers and then randomly assigned to the experimental or control groups using a computerized process developed by the researcher. Participants in the experimental group received the neck stretching exercise intervention. Participants in the control group used their usual headache management methods. All participants completed the study.
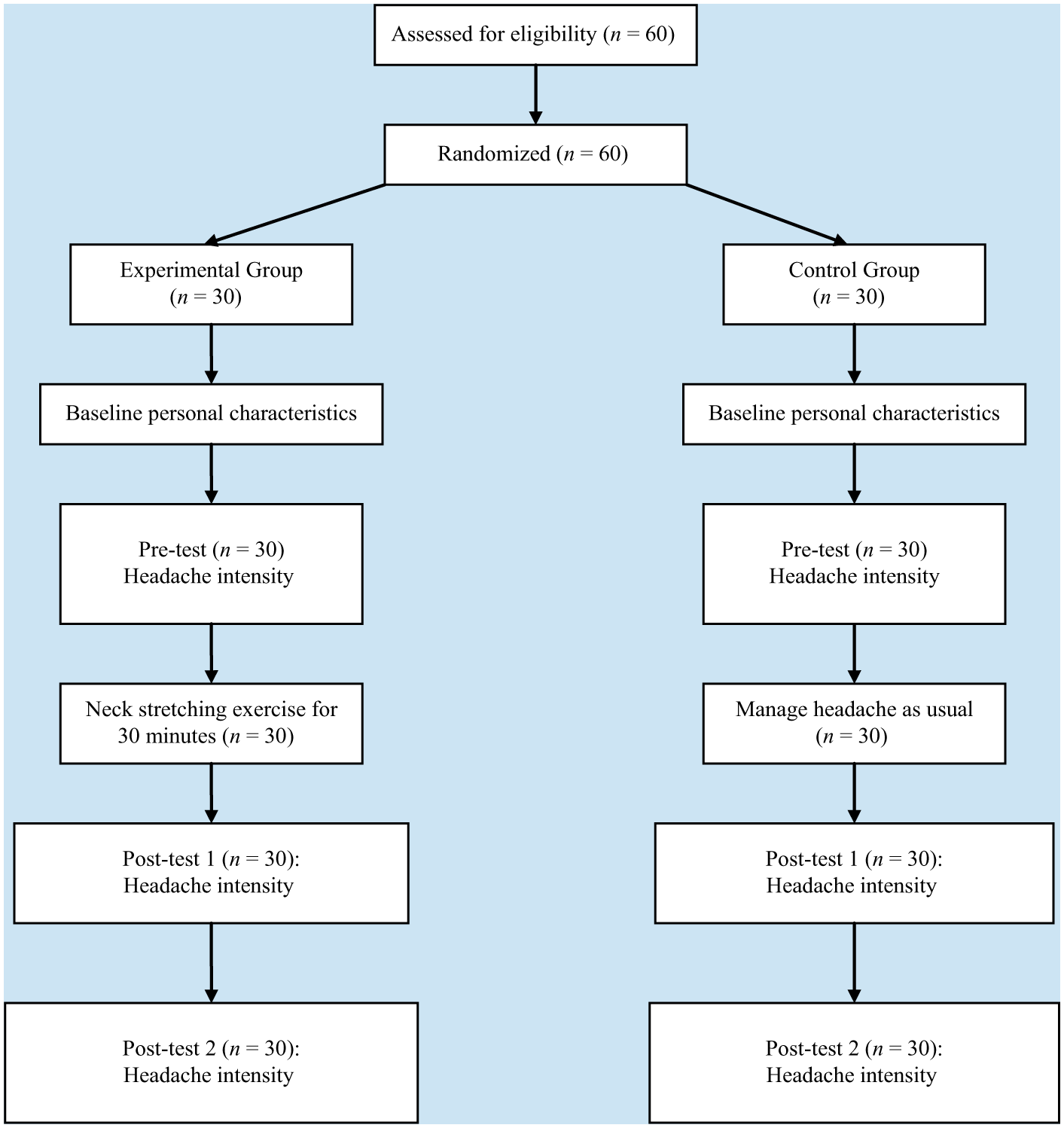
Flowchart of study participants.
Neck Stretching Exercise Intervention
Study researchers developed the neck stretching intervention based on relevant literature (Behar, 2013; C. H. Chen & Chen, 2007; T. Y. Chen & Tu, 2001; Li, 1997; Zakas, 2005). Researchers consulted a physiatrist who suggested that the neck stretching intervention should be performed for about 20 min, holding each stretch for 10 seconds. To standardize the procedure and increase its fidelity, researchers also developed an instructional videotape for the experimental group. The experimental group then performed neck stretching exercises for 20 minutes instead of using their usual method of treating a headache. The researcher provided additional instruction as required to assure the accuracy of neck stretching.
Neck stretching included (a) sit or stand in a comfortable and relaxed position; (b) slowly turn the head and neck from side to side; (c) slowly stretch the neck in any direction (i.e., forward, right, backward, and left), especially stretching in the direction that is painful (i.e., stretch the muscle that is experiencing pain) with each stretch lasting 10 seconds; (d) repeat steps (b) and (c) for about 20 min. The experimental group was encouraged to perform neck stretching exercises according to their tolerance, slowly stretching until experiencing a slightly tight feeling and then holding the stretch at that point to avoid overstretching. The control group managed their headaches as usual and recorded whether or not they used analgesics. Interventions were used at break time in the workplace break room or after working hours.
Measurements
Self-reported structured questionnaires were used to collect data. Baseline personal characteristic data included age; education; marital status; headache frequency; highest, lowest, and average headache intensity in the past month; analgesic use for headache; non-medication methods of managing headaches; and the effects of those methods in the past month (i.e., 0 [no effect] to 10 [very effective] by self-report).
Headache intensity was measured at baseline (pretest), and at 30 minutes (Posttest 1) and 1 hour (Posttest 2) after intervention on a 0 (no pain) to 10 (unbearable pain) numeric rating scale (NRS). The NRS is a simple, valid method that has been used to measure acute and chronic pain intensity (Brunelli et al., 2010; L. Y. Lin & Wang, 2005). The test–retest reliability of NRS was .80 to .86, an acceptable range (Brunelli et al., 2010).
Data Collection
After receiving Institutional Review Board approval, the researcher explained to participants the research objectives, process, data collection procedure, and recruits’ right of refusal. Participants then consented to the study and completed the baseline demographic characteristics questionnaire. Both the experimental and control groups notified the researcher when they had headaches and had time to perform interventions such as rest or time off work. Participants recorded headache intensity on a questionnaire before the intervention. To prepare for the intervention, the researcher offered the experimental group a videotape about the neck stretching exercises and also described the process if required. The experimental group performed the neck stretching exercises for about 20 minutes. The control group managed their headaches as usual. The participants of the experimental and control groups recorded headache intensity at 30 minutes and 1 hour after beginning the intervention. These questionnaires were enclosed in envelopes by the experimental and control groups and were returned to the researcher.
Data Analysis
SPSS for Windows 18.0 software was used for statistical analysis. Descriptive statistics, including mean (M), standard deviation (SD), and frequencies, were calculated. Chi-square tests, independent t tests, and ANOVA were used to test the differences within groups, and ANCOVA was used to test the differences between the experimental and control groups. Repeated-measures ANOVA was used to test the effectiveness of the intervention.
When comparing the posttest scores of the two groups, the variables associated with the posttest score were treated as covariates (control variables), including the pretest score (Owen & Froman, 1998). After that, the posttest scores adjusted by pretest score and other control variables were compared (Owen & Froman, 1998). Analysis of Covariance was used to test the differences between the means of the experimental and control groups controlling for pretest scores.
Results
Demographic Characteristics of Participants
As shown in Table 1, age, education, marital status, experience of headache frequency, and headache management methods in the two groups at baseline did not significantly differ. The experience of the highest and lowest headache intensity was not significantly different between the two groups. However, the experience of average headache intensity in the past month in the experimental group was significantly higher than that in the control group. Randomization can avoid selection bias and interference factors, but still have the possibility of different distributions in baseline characteristics of the groups. Thus when comparing the groups, researchers must show the results of the adjusted analysis (Owen & Froman, 1998). Therefore, headache intensity at pretest was added to the covariates to adjust posttest headache intensity when comparing the posttest headache intensity between the experimental and control groups after the intervention.
Comparison of Demographic Characteristics Between Groups (N = 60)
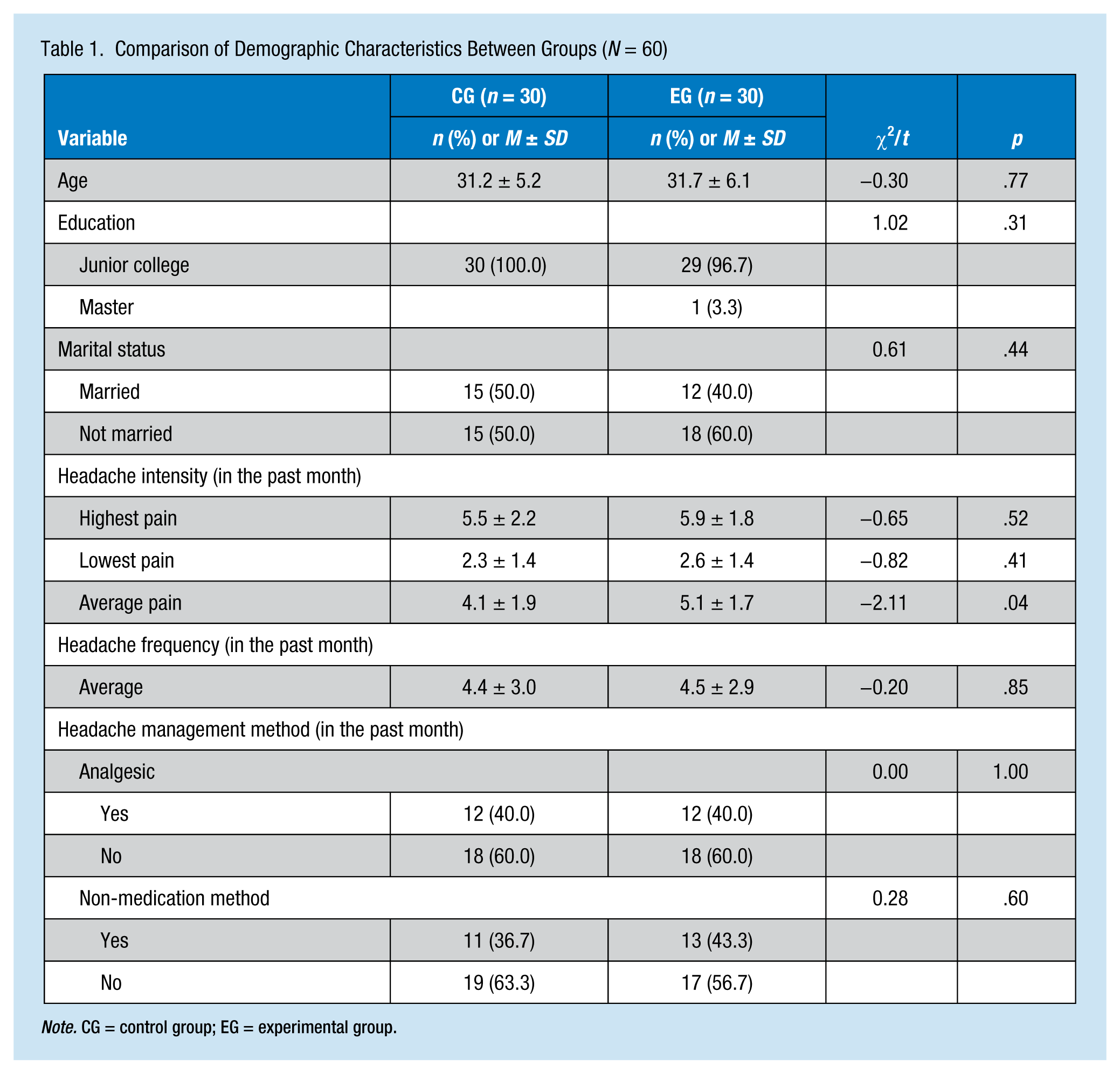
Note. CG = control group; EG = experimental group.
In the month prior to the study, the average headache score of participants was 4.6 ± 1.9 (range = 1-8), and the average headache frequency was 4.4 ± 3.0 (range = 1-15). Most participants (60%) did not report taking analgesics to manage their headaches in the past month. Twenty-four participants did take analgesics: acetaminophen (19, 31.7%), ibuprofen (3, 5.0%), mefenamic acid (1, 1.7%), and diclofenac (1, 1.7%). Most participants (60%) did not use a non-medication method to manage their headaches. Twenty-four participants (40%) did use non-medication methods to manage their headache, including sleep (15, 25.0%), massage (8, 13.3%), coffee (4, 6.7%), watching TV (3, 5.0%), and listening to music (2, 3.3%). Other non-medication methods (e.g., exercising, taking a shower, drinking plenty of water, drinking hot milk, using peppermint essential oil aromatherapy, defusing stress, breathing fresh air, and rubbing ointment on affected areas) were used by only one participant. The average effectiveness of the non-medication methods was 6.8 ± 3.0 (range = 1 [no effect] to 10 [very effective]) for sleep, 4.1 ± 2.7 (range = 1-8) for massage, 7.8 ± 1.5 (range = 7-10) for coffee, 4.0 ± 2.6 (range = 2-7) for watching TV, and 4.0 ± 0.0 for listening to music.
Comparisons of Headache Intensity Between and Within Groups
Headache intensity was compared between and within groups. As shown in Table 2, the pretest headache intensity was 5.07 (±1.76) for the experimental group and 4.57 (±2.01) for the control group. Headache intensity did not significantly differ between the two groups at pretest.
Comparisons of Headache Intensity at Pretest, Posttest-1, Posttest-2 Between and Within Groups (N = 60)
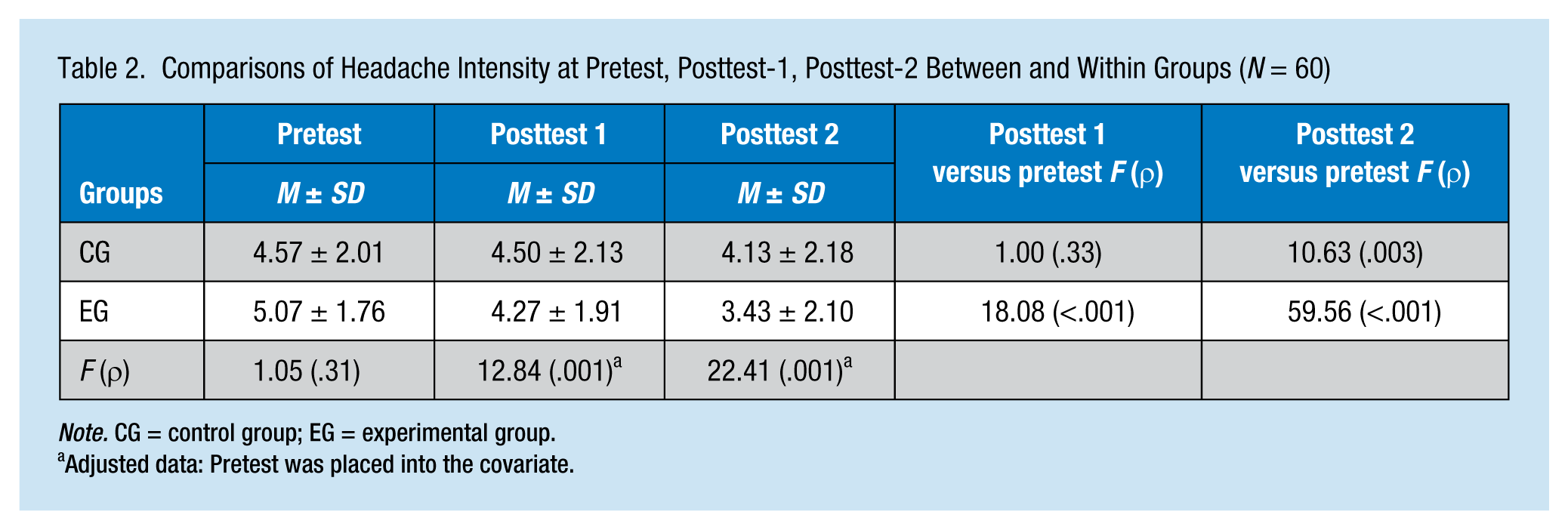
Note. CG = control group; EG = experimental group.
Adjusted data: Pretest was placed into the covariate.
When comparing posttest headache intensity between the two groups, the researcher compared the posttest scores of the two groups, adjusted by pretest score. As shown in Table 2, headache intensity of the experimental group was significantly lower than that of the control group at Posttest 1 and Posttest 2. The neck stretching exercise intervention had a statistically significant effect on decreasing headache intensity of the experimental group at Posttest 1 and Posttest 2 compared with the control group.
In terms of within-group differences, headache intensity of the experimental group at Posttest 1 and Posttest 2 were both significantly lower than that of the pretest. In the control group, no significant difference was found between Posttest 1 and the pretest. However, headache intensity at Posttest 2 was significantly lower than at pretest. Neck stretching exercises reduced headache intensity earlier than the control group. The experimental group could significantly lower headache intensity and maintain it through Posttest 2.
Comparison of the Two Groups’ Headache Intensities by Repeated Measures
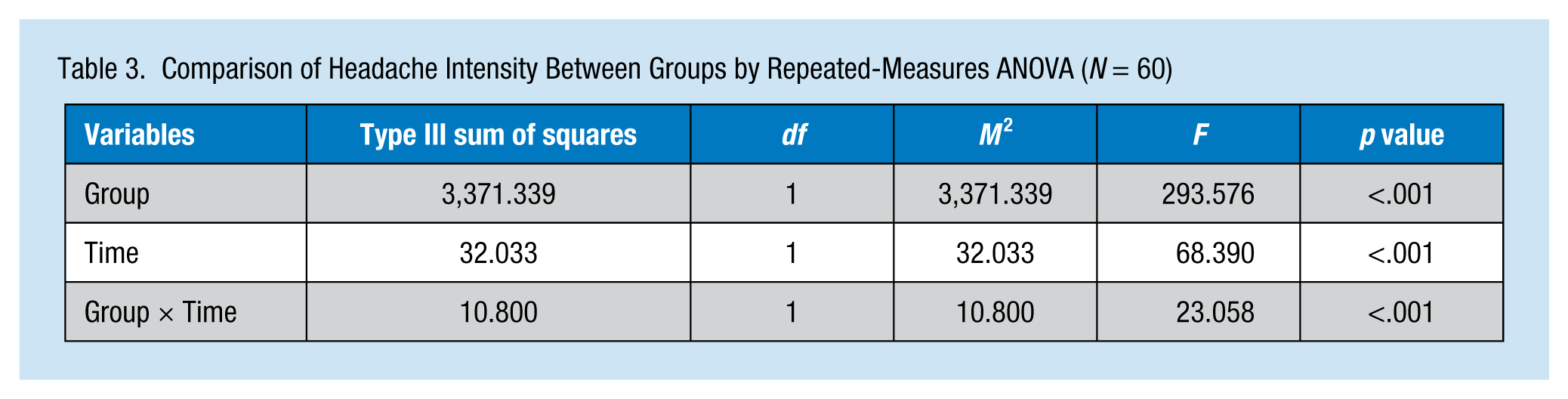
As shown in Table 3, the full model of the repeated-measures ANOVA revealed a statistically significant difference in headache intensity between the groups (F = 293.576, p < .001). In terms of time effect, a statistically significant difference in headache intensity between the pretest and posttest was found. Regarding the Group × Time interaction effect, the difference in headache intensity between the pretest and posttest in the experimental group was significantly greater than in the control group. The decrease in headache intensity of the experimental group was significantly larger than that of the control group.
Comparison of Headache Intensity Between Groups by Repeated-Measures ANOVA (N = 60)
Discussion
The findings showed that 20 minutes of neck stretching exercise was significantly better at decreasing the intensity of primary headaches in the experimental group than the usual methods used by the control group at 30 minutes and 1 hour after intervention. Also, the neck stretching exercises had an earlier effect on reducing headache intensity in the experimental group than the usual methods did in the control group. The effect of reducing headache is congruent to the findings of Ylinen et al. (2007), which found that neck muscle stretching programs could reduce neck pain and headache.
In this study, the stretching exercise consisted of repeatedly turning the head and neck in extended positions for a total of 20 minutes, with each stretch duration of 10 seconds. The neck stretching exercise had an immediate effect on reducing headache intensity. In the study of Ylinen et al. (2007), neck stretching was used five times a week, with each stretching exercise repeated three times while holding each movement for 30 seconds. However, those researchers examined the effects after 4 weeks.
Participants in the control group used their usual headache management methods except medication. Therefore, headache intensity of the control group at posttest 2 was also significantly lower than at pretest. However, the effect only appeared at 1 hour after beginning the intervention. Headache intensity of the experimental group was significantly reduced at 30 minutes and continued to 1 hour after intervention. The neck stretching exercise had an earlier effect on reducing headache intensity than the usual methods used by the control group. In this investigation, nurses managed their headaches using methods such as sleep, massage, and drinking coffee in the previous month. Further studies should compare the effects of neck stretching exercise and other specific methods on reducing headache intensity.
Several limitations were identified for this study. The samples were recruited from only one hospital. To increase generalizability, future studies should apply the intervention to diverse samples. This study was a one-time-only intervention study and did not explore the effect of neck stretching exercises on preventing reoccurrence of primary headache. Future studies should follow participants over a longer period to determine the incidence of primary headache and assess the long-term effects on reducing the intensity of primary headaches.
In clinical situations, nurses are challenged by patients’ health conditions and their potential alteration. Work stress and tension occur often. Nurses need to control the excessive tension that causes headaches. During rest periods at work, turning the head and stretching the neck can relieve tension in the neck muscles and reduce the intensity of headaches. Also neck stretching could allow nurses to return to work sooner than the usual methods used by the control group, thus supporting economic, nursing workforce, and patient benefits.
Implications for Practice
Headaches are a health concern for health care providers, which can also affect the quality of their work. This study found that neck stretching exercises are effective in reducing the intensity of primary headaches. In addition, neck stretching is cost-effective and easy to implement individually. Neck stretching can be considered one method to reduce primary headaches for nurses.
Applying Research to Practice
In clinical situations, nurses are challenged by patients’ health conditions and their potential alteration. Nurses need to control the excessive tension that causes primary headaches. Stretching the neck can reduce the intensity of headaches. In addition, neck stretching is easy to implement individually. Neck stretching can be considered one method to reduce primary headaches for nurses.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: We declare that all authors have read and approved submission of the manuscript, and the manuscript has not been published and is not being considered for publication elsewhere in whole or part in any language except as an abstract.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This funding was supported by the Kaohsiung Veterans General Hospital, Taiwan.
Author Biographies
Li-Ying Lin, RN, MSN, Doctoral Student, College of Nursing, Kaohsiung Medical University, and Department of Nursing, Veterans General Hospital, Kaohsiung City, Taiwan.
Ruey-Hsia Wang, RN, PhD, Professor, College of Nursing, Kaohsiung Medical University, Taiwan.