
Abstract
The learning environment (LE) provides a context for many educational phenomena, of which wellness and burnout are particularly important. The LE can be thought of as consisting of a psychosocial dimension of personal, social, and organizational factors and a sociomaterial dimension that consists of spatial and technical factors. The interplay between elements of the LE and wellness of the participants is complex and only partially understood, requiring further research. Using this multidimensional model to describe and to plan to deliberately modify the learning environment can foster more rigorous and meaningful research evidence about the interaction of wellness and the LE. This article highlights four key considerations that scholars of wellness should consider when exploring the impact of the LE or designing interventions to modify the environment. These include 1) a thoughtful definition and theoretical conceptualization of the LE, 2) clarity about the study variables that are essential to the study question(s), 3) thoughtful and appropriate measurement of those variables, and 4) a study design that balances quality with feasibility. We provide a practical illustration of how these considerations can be applied in studies exploring the intersection of wellness and the LE.
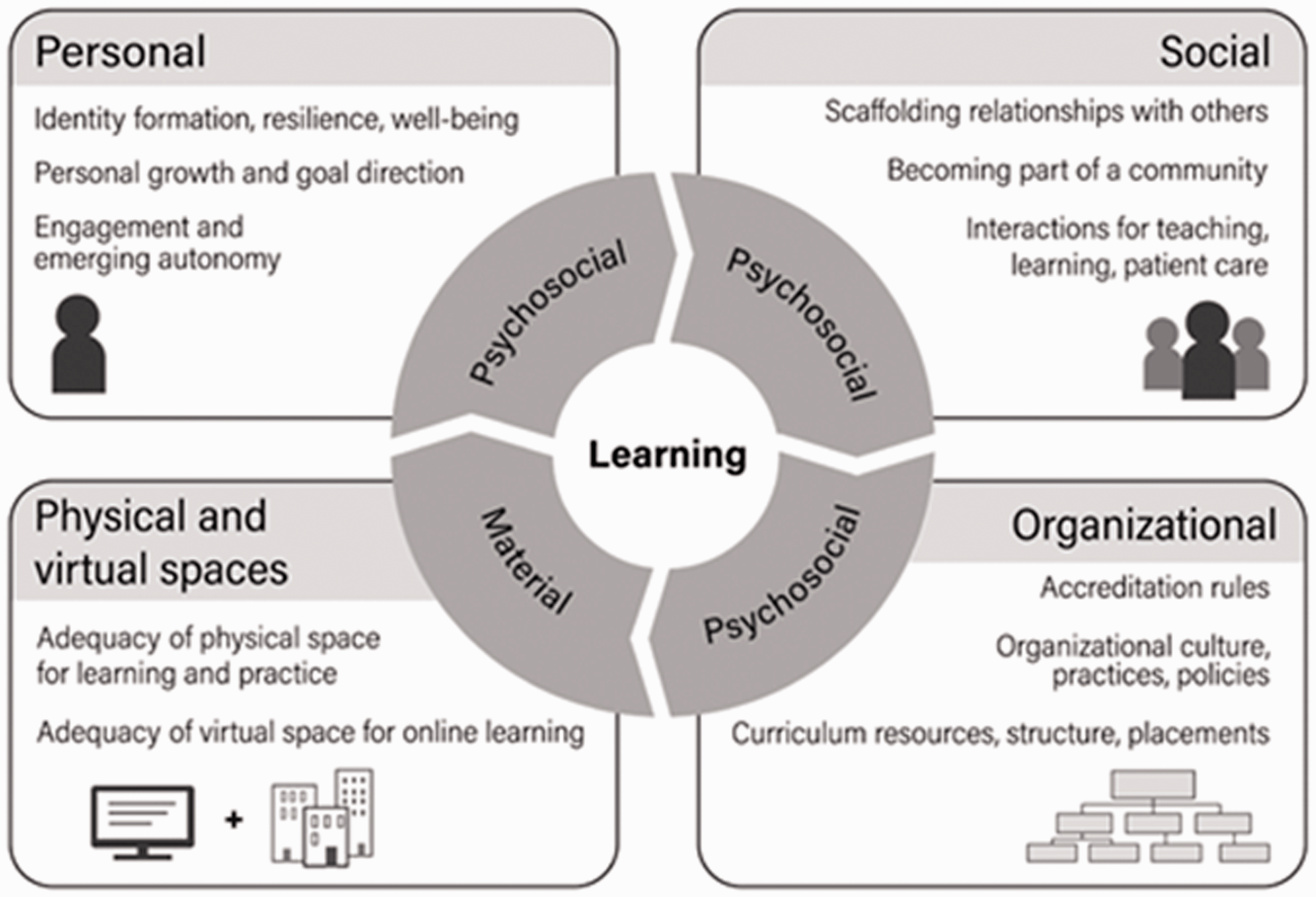
The LE can be defined as “… the social interactions, organizational culture and structures, and physical and virtual spaces that surround and shape the learners’ experiences, perceptions, and learning.” 1 Although there are relatively few theories or models of the Learning Environment (LE), they reflect a range of disciplines, including psychology, 2 higher education,3,4 and medical education. 5 A recent model (Figure 1) was commissioned by the Josiah Macy Jr Foundation for an invited conference on Improving the environment for learning in the health professions in 2018. 6 It was derived from a scoping review of the health professions literature to examine the theoretical frameworks used in research on the LE.
A Model of the Learning Environment. 1
This model has two primary dimensions: a psychosocial and a sociomaterial7–9 dimension. The psychosocial dimension encompasses the key human interactions that define most LEs. There are at least three levels in this dimension: the personal or individual characteristics that contribute to or respond to the LE, the social level encompassing interpersonal interactions of many kinds, and the organizational level of institutional policies, culture, and regulation. The sociomaterial dimension describes how learners interact with the physical and virtual world they learn in. It includes the physical spaces and attributes of buildings and classrooms, such as light, noise, seating arrangements, and temperature. It also includes virtual spaces consisting of information structures and networks, data systems, electronic health records, and learning management tools and technologies.10–12
There is little doubt that stress, burnout, depression and other presentations of psycho-emotional distress are common experiences in medical education and practice. 13 Nor is there question about the adverse impacts of these distresses, such as dropping out, forced career change, substance abuse, suicide and depression, and many other phenomena. 14 The COVID pandemic is magnifying these stressors, adding new challenges including ambiguity, isolation-alienation, anxiety and atomization with loss of a sense of community. 15
Opposing these challenges is the concept of wellness, defined by the WHO, as the optimal state of health of individuals and groups. It focuses on both the realization of the fullest potential (life-satisfaction) of an individual physically, psychologically, socially, spiritually and economically and the fulfillment of these individual’s roles in family, workplace and community settings. 16 Some would use the term well-being for the above, emphasizing the more static description of an optimal state. Many prefer the term wellness as describing one’s awareness and active pursuit of activities, choices and healthy lifestyles to lead to a holistic concept of health, achieving one’s full potential. 17
Wellness is a concept that is multi-dimensional, dynamic and still evolving over time.
18
For the sake of our discussion, we have selected a multi-dimensional description of the concept (Figure 2) based on Hettler’s
19
original Hexagonal Model of Wellness:

Overview of the 8 Dimensions of Wellness. 20
Wellness is influenced by and itself influences many other phenomena, such as resilience 22 or interpersonal interactions, e.g., mentoring,23,24 or institutional culture. 25 Clearly, individuals in their pursuit of wellness or building resilience do so not in isolation but influenced by interactions with their social and cultural environments. Thus, one may need to place this active pursuit of wellness in a larger, multidimensional context, which we propose to consider in terms of the learning environment. We argue that the LE influences our learners’ chance to achieve wellness in this domain of their life.
Though always present, the LE may at times be invisible. It lurks in the background and can be taken for granted during times of stability. However, the LE may take front stage when an educational problem or crisis emerges, such as a suicide, learner unrest, or citation by a regulatory agency for a toxic educational culture. Consider how dramatically COVID is rewriting the learning landscape for trainees and educators alike.
In this paper we argue that, in order to better study wellness-related problems, it is necessary to recognize the subtle, but influential role of the LE. In summary, it would be hard, if not impossible to isolate studying an individual’s or group’s issues from the environment in which it happens. Thus, the complex and contextual nature of the LE poses both challenges and benefits to researchers when planning research on wellness and its related topics, such as resilience, stress, or burnout. We pose four considerations one should think about in any study linking wellness and the learning environment (Table 1).
Four Key Questions for Conducting Research on Wellness and the Learning Environment.

What Is Your Theoretical Perspective? What Do You Want to Understand or Change?
Research that makes a difference requires a theoretical foundation.26–29 Theory is critical for making sense of complex phenomena, for defining constructs and terms, and for explaining or predicting relationships among constructs and variables. It provides context for interpreting empirical data and guides research studies. However, it is important to recognize that every theory is limited, a simplification of reality. As attributed to statistician George E. P. Box, “All models are wrong, some are useful.”
We have introduced potential theoretical frameworks for both the LE and for wellness, above. The LE model emphasizes the importance of human characteristics and interactions, which are also clearly reflected in the social and emotional dimensions of the wellness model in Figure 2. Thus, the two models support each other. Similarly, the sociomateriality dimension of the LE model includes the physical, which maps onto the environment dimension of the wellness model. However, the wellness model does not specifically call out virtual spaces or technology as a component of wellness. This might suggest that there is a connection between wellness and the LE that is worth pursuing. Similarly, there are several additional dimensions of wellness (e.g., financial, spiritual, professional) that may fit this in the psychosocial dimension of the LE or may require an expansion of the model to accommodate them.
Of course, using alternative models for key constructs will also allow one to shift focus to somewhat different manifestations of wellness. For example, using multiple tenets in their Wheel of Wellness model, Witmer, Sweeney et al. 30 incorporated coping, self-worth, cultural identity, spirituality but also nutrition, self-care, and stress management into their model. Spirituality as a central energy force to engage in the pursuit of wellness is a theme in several holistic modules.31,32 Investigating the relationship of spirituality and the LE may require a modification of the LE framework to better address the nature of sacred and meditative environments.
Many tenets in these models overlap, but as their emphasis may be on different aspects within the framework, the rich variety of models allows the researcher to select one best fitting their explicit focus of research interest. By deciding on the primary focus of one’s interest, it allows for selecting the appropriate theoretical frame for measuring the changes due to the proposed intervention.
Identify Your Research Question
Identifying the research question depends somewhat on the research methodology. With qualitative methods, the question may focus on the description or exploration of selected phenomena, concepts, or experiences. With quantitative methods, the research question may be more in the form of a hypothesis that is to be tested. Mixed methods may state questions in more complex ways that combine both forms.
The key variables in a study are defined by one’s research question. A well-stated, clear, and comprehensive research question will help identify both independent and dependent variables as well as potential confounding variables that need to be taken into consideration. The learning environment itself can be both a dependent variable and an independent variable. As a dependent variable, LE may be influenced and altered by an initiative or intervention, such as a new learner wellness program. As an independent variable, it would be considered as an influence on an educational outcome, such as whether different institutional cultures and values require different kinds of wellness programs. Often, the LE is a confounding (background) variable that needs to be considered but is not among the dependent and independent variables (e.g., the LE alters the ways faculty engage in a wellness program).
However, it may be that one’s research question is more exploratory than hypothesis-testing. In such cases, qualitative studies may be more appropriate and the distinction among different kinds of variables less clear. In exploratory studies, the emphasis may be more on discovering variables that may be relevant, rather than testing them. Because the LE is multi-dimensional, recognizing and proposing new interactions between some of its components and the wellness dimensions is in itself a valuable task for qualitative studies.
Often, a research question can be answered with either qualitative or quantitative methods. For example, the problem of resident work hours and their impact on resident wellness is a phenomenon that can be examined through both theoretical frameworks to identify specific ideas or possibilities. If investigators wanted to examine the quality of the physical work site on resident wellness, they could identify emotional aspects of wellness in connection with the crowding and lack of privacy in the physical learning environment through interviews with the residents in that setting. The interviews could be analyzed to identify influences and dynamics in the relationship of emotional wellness and spatial crowding. These findings could lead to a quantitative study that sought to measure the magnitude of these relationships and perhaps develop an intervention to minimize the impact of the LE on wellness.
How Will You Measure Relevant Variables?
Every key variable in the study will need to be measured or accounted for in some way. Some variables will be simple categories (gender, intervention vs control group, geographic region) whereas others may be measured with multi-question instruments (such as resilience instruments, or burnout questionnaires). Measuring variables may be qualitative (e.g., observing learner interactions in various spatial classroom environments) or quantitative (e.g. improved stress scores as a result of an innovation). Some key variables may not be directly observable or measurable, but surrogates can be used. Residents’ level of fatigue may approximate their increase in medical errors in the acute setting or may correlate with burnout if chronically present. 33 Measuring LE variables is one of the greatest challenges for research in this domain because of the complexity and contextual nature of LE studies. These often entail that there are many variables that could be considered relevant, but resources, sample sizes, and measurement tools are seldom adequate to address them all.
Thus, planning a study of the learning environment and wellness will require careful, reflective modeling of the LE, recognition and prioritization of measurable variables, and data that are expected to be most useful for answering the research question. It might be beneficial to consider upfront a list of recognizable LE components potentially at play and sort them into independent and dependent variables of importance to the primary outcomes. There are also likely to be confounding variables that need to be measured (e.g., learner anxiety, classroom noise, teaching faculty OR schedules, or post-call fatigue.
One significant challenge to research on the LE is that the most common way to measure the LE is through questionnaires given to individual learners. 34 These instruments ask individuals about their perceptions of or preferences for various aspects of the LE and combine items into various scales that presumably measure different components of the LE. There have been several reviews and critiques of these learner-focused questionnaires.5,35 The problem with this state of affairs is that the measurement of the LE is heavily weighted toward the Personal level of the LE model (Figure 1). The questions may address interpersonal and institutional and spatial and technological characteristics of the environment, but all these measures are built on learner perceptions. As important as learner perceptions are, they are subjective and far from the complete story of how the LE and phenomena like wellness are connected.
Measuring LE variables at the social level of the LE model is much less developed, but there are some tools for assessing team performance that hold promise for use in studying the LE. 34 Even more challenging is measuring LE variables at the organizational level. There may be some institutional attributes that are quite straightforward (e.g., level of research funding, number of faculty, urban vs suburban vs rural location), but measuring organizational variables like culture or trustworthiness is much more challenging.
Spatial environments may be measured by square footage, light levels, density of seats or lab benches or beds, availability of small to large meeting rooms, and many others. Virtual environments may require fewer tangible measures, such as the brand and version of a learning management system, the number of computers/learner, support staffing levels, upgrade cycles, and user perceptions of functionality. Yet a new variable during the COVID-19 pandemic is just emerging – fluctuating degrees of access to on-line spaces – illustrating the ever-changing nature and layers of the LE. Illustrating the still evolving nature of wellness, one may now think of individual or group wellness influenced by internet bandwidth. Professional, emotional, social and even spiritual dimensions of wellness are all recognizable in the on-line space during quarantining.
A key lesson about measuring the LE is that the field needs to liberate itself from a reliance on learner perceptions as the primary operational definition of the learning environment and develop objective measures that emphasize behaviors and changes in the performance of individuals, groups, and institutions.
What Is Your Study Design?
The complexity of the LE also limits the range of common study designs36–38 used in LE research. The complex interaction of personal, social, institutional, and physical factors makes the strategies of randomization, careful controls, adequate statistical power, and equivalent comparison groups virtually impossible. As a result, many of the published studies of the LE use simple single-group observational designs for qualitative descriptive or quantitative correlational studies. Also, fairly common are comparisons among naturally occurring groups (e.g., institutions, curricula.) Quite uncommon, but essential to providing high-quality research evidence are pre- and post-intervention designs, control-vs-intervention comparisons, or complex statistical modelling designs. The emphasis of these designs is on an intentional, usually prospective intervention. However, the more sophisticated the design, the more complex (and expensive) it becomes to implement. Nonetheless, studies designed to probe the LE and wellness should aspire and work towards the best, most rigorous study design that is feasible in that situation.
Although complex study designs are not typical of qualitative research, these studies also have design considerations that parallel those of quantitative methodologies. An adequate sample of informants is necessary to generalize the findings. Research questions that focus on differences among groups will need intentional actions to define these groups explicitly and sample from them adequately. Whereas quantitative studies depend on measuring previously defined variables, qualitative studies may focus on identifying novel variables and influences. The study may go on to identify the structures of these variables for subsequent quantification.
Applying These Research Principles: An Illustration
As an example of how these four considerations can aid in developing a study of wellness within the learning environment, let us consider the topic of medical student career choice.
What Is Your Theoretical Perspective? What Do You Want to Understand or Change?
Taking career choice as the topic of research, the first step would be to select or define one’s theoretical perspective on this phenomenon. Complex questions such as this one can be considered from many perspectives, each of which bringing with it assumptions and priorities. One could approach this as a consumer choice issue, applying economic and rationality models that would focus on positive and negative attributes of a set of alternative outcomes, with weighted priorities given to each attribute. Alternatively, this problem could be considered one of professional identity formation, which would emphasize psychological growth and self-image in the context of the social meaning of a profession. There are many, many others.
For this illustration, mentoring and career advising programs are thought to be useful in guiding students towards well-fitting specialties. This road can be straight for some trainees but long and winding for others. One may have an interest in examining potential influences and influencers on medical students’ original vocational stances and how eventually they finalize a decision about their future medical specialty. What factors affect their views on a desired fit between their personal and professional priorities, values, and their ultimate choice?39,40
This topic aligns both with elements of the Learning Environment (Figure 1) and with dimensions of Wellness (Figure 2). One may look at this decision as a key factor determining future Professional Wellness, since a poor selection of one’s specialty can have significant consequences on the well-being of the learner later in career, as an attending. But such “mismatches” may go beyond individual Wellness, and have untoward effects on the health care system, if the result is a trainee switching to another specialty or even dropping out of medicine altogether.
One reported intervention with a beneficial impact on this conundrum is a medical student mentoring program with a focus on career guidance and informed decision making about specialty alternatives. This illustrative study will thus focus on how a well-designed mentoring program may or may not reach its goal of understanding specialties and choosing wisely.41,42
Identify Your Research Question
Figure 3 below is meant to serve as an inventory of possible factors in LE and Wellness that may factor in the above question. Its complexity illustrates the richness of factors possibly active in this study. Indeed, for any manageable study, elements of this framework will need to be ignored or set aside – but that is part of the benefit of theory; it guides you in those decisions.

An Example How the Learning Environment and Wellness Interface in a Clinical UME Environment to Influence Outcomes of Medical Students Selecting Their Future Specialty. The multifaceted learning environment (Brown Box with list of LE elements) effects the trainees’ UME experience in multiple ways creating stresses and rewards. On this background the program runs the mentoring program (White Box), but its efficiency is deeply intertwined with the particular LE of the program. As they progress through their clinical clerkships, medical students live through a wild array of experiences that stem partly from the LE surrounding them and is connectable to wellness outcomes (Blue Box in the middle) and the sum of these encounters may influence their eventual choice of specialty (Black Box). Once in residency (GME box), the LE continues to create experiences possibly affecting multiple wellness dimensions and post-GME a trainee’s final career path may have long-term outcomes on the practitioner’s wellness (Blue Box on the right). A researcher may initially choose to employ a dense matrix like this, for a comprehensive overview of the multitude of factors of possible interest but will later need to focus on a limited number of variables in the study proposal.
Using this illustration, one may decide to set the study’s main focus on positive (or negative) experiences aligning with later successful (or unsuccessful) career patterns, select the positive (or negative) wellness factor(s) of interest and choose to study it in the context of some selected elements of LE (exposure to the hidden curriculum, limits on weekly hours of work, issues of access to resources, level of fatigue among learners or mentors, collegiality versus competition etc.). Setting the focus on just a limited number of LE elements and only on a few dimensions of wellness are all essential to designing a realistic, manageable study. In summary, this model implies that studying wellness on a selected LE platform may offer a large number of new and exciting research questions.
How Will You Measure Relevant Variables?
Typical variables differ for qualitative and quantitative studies. Often in a qualitative study, one relies on observed or self-reported values, whereas quantitative studies may lead one to analyze or compare data in rubrics, look at curricular or policy documents, teaching structures etc. Some variables are directly measurable while others are not. Surrogate markers – if validated in the literature – can be useful proxies for both qualitative and quantitative studies.
In this illustrative study, work-life balance may be hard to measure directly, but asking interviewees about their access to child-care, desire of flexible hours, or seeking part-time positions is more tangible. 43 Also, access to measurable surrogate data varies widely – some of the institutional aspects of the LE (policies, promotion criteria, passing scores) may be relatively easy to retrieve, the workload of teaching clinical faculty can be approximated (through productivity targets measured as mandated RVUs), time obstacles, expectations (stated and hidden), lifestyle of trainees can be estimated by inquiring about their typical clinical schedules.
A quantitative study may compare wellness scores of trainees on different clerkship rotations (UME) or in residencies in a number of specialties (GME), as it relates to their hours of rest, daily case load or using a self-reported work-life balance questionnaire to measure scores on a depression or burnout scale.
Based on these considerations, an illustrative study interested in how the learning environment shaped student wellness and influenced the outcome of mentoring, may use the frame in Figure 3, and select some of the following measurables:
In essence, we are linking the independent variables of the Social, Institutional and Sociomaterial LE to short-term wellness outcomes in hopes of studying their effect on the intervention (mentoring) as it determines one’s specialty choice.
What Is Your Study Design?
If setting off to identify factors in the LE with an influence on vocational wellness, the ideal design might be a qualitative study collecting comments from trainees on their personal experiences or observing how they navigate the clerkship environment encountering both positive and negative (and hidden) elements of the curriculum. A qualitative wellness study would be ideal to generate some hypotheses for a later interventional study and help define the key measurable variables for it. Once such data are available, a quantitative wellness/LE study may compare the success of an intervention on pre-selected outcomes (stability or change in satisfaction, modified aspects of social, emotional, physical, financial, or other wellness in this illustrative example). One may decide to compare these to pre-interventional outcome parameters or contrast them with those in other programs that lack an effort to optimize their LE.
Using the LE model reflectively (Figure 1), might prompt the researcher to focus on particular components of the LE, such as the
Finally, there is the challenge of measuring these critical variables. As noted earlier, reliance on individual self-report and preference data in many studies of wellness and the LE is decidedly subjective. To some extent, this appropriately reflects the fact that wellness is an individual phenomenon and that people respond to the same LE in different ways. Authors should be mindful of limitations and biases of self-reported data and – prior to concluding the need of significant changes in one’s system – the purely qualitative data should well be supplemented with other methods for measurement. In the mentoring example, it would be appropriate to measure the effectiveness of the mentoring relationship from the perspectives of both learner and mentor, as well as against more external metrics like rates of mentor reassignment or learner drop-out from the program. LEs in the residency years might be measured by published questionnaires35,44 but also by residency program characteristics like urban vs suburban locations, program size, faculty characteristics, and specialty training.
Conclusions
The relationship between wellness and the learning environment is complex and not well understood. The need for research into this relationship is strong, but the quality of the research is too often weak. In this article, we have sought to emphasize the characteristics of higher quality research that is driven by meaningful and important questions, uses the best study designs feasible, clearly defines key variables, and measures them appropriately. This rigor and transparency will foster the ability to compare studies and situations, as well as clarify the interpretation of results.
There is a growing awareness of the need to consider the learning environment in the context of burnout, stress, and wellness. There are also a number of interventions that are designed to improve the learning environment in the hopes of enhancing wellness. Both of these developments will be most fruitful, if they follow these considerations for conducting research in the learning environment and wellness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.