
Abstract
Introduction: Diabetes mellitus type 2 (DM2), one of the four most important chronic diseases worldwide, is generally considered to be preventable. However, it is not yet sufficiently clear whether an aligned collaboration between different health professions could facilitate behavioral changes to be made by patients with DM2 regarding their eating and physical activity habits. Objective: To explore if and how far in current outpatient care for 3 health-care professions it is an objective to collaborate with each other supporting patients with DM2 in changing their eating and physical activity habits. Methods: We conducted 18 qualitative problem centered interviews with selected family physicians, nurses, dieticians working in outpatient setting and patients with DM2, transcribed verbatim, and analyzed with qualitative content analysis. Results: Issues identified ranged from description and reflection of current health-care practice, strategies, and hindrances to cope with changes of eating and physical activity behaviors as well as for health-care practice regarding interprofessional collaboration and patient-centered care up to considerations about collaboration and patient centricity (for health professionals and patients to achieve goals) and changes and ideas of “ideal care practice”. Discussion: The included professional groups work predominantly for themselves. Collaboration currently only takes place when individually triggered and neither structured nor organized.
Keywords
Introduction
Diabetes mellitus type 2 (DM2), 1 of the 4 most important chronic diseases worldwide, is generally considered to be preventable. Various studies have shown that weight reduction through changes in eating and physical activity habits can reduce cardiovascular risk factors, in other words help to prevent long-term major complications of DM2.1–3
However, it is not yet sufficiently clear whether an aligned collaboration between different health professions could facilitate behavioral changes to be made by patients with DM2 regarding their eating and physical activity habits. Although, the literature indicates slight differences that coordinated care planning (process and goal clarification) and collaboration between physicians and patients could help improving clinical outcomes, enhancing patient satisfaction, and promoting self-management skills. 4 Reeves et al. rated in their review on interprofessional practice and health-care outcomes the evidence to conclude on the effects of interprofessional collaboration as to low and not currently sufficient. 5
Referring to Borgermans et al. a “single handed practice and a problem-oriented care” are current problems in primary care which have to be overcome by leapfrogging strategies. The authors suggest opting for a move toward multidisciplinary care teams that are able to support effectively patients at different critical points of their chronic conditions such as the diagnosis, in an overarching way (global sense). These teams could actively contribute to changes in provider culture such as moving toward a goal-oriented care in order to meet challenges of lifestyle changes as a complex endeavor. According to them, these challenges can be tackled in a better coordinated way than it is today. 6
Issues and innovation processes enabling change improving the service provision/delivery especially through organizational development have been identified by Fitzgerald and McDermott. In general, for them one particular concern is a lack of coordinated and collaborative capacity of health-care organization. The authors suggest as one area of development, for example, that interprofessional collaboration should be supported through organizational development processes to enable to develop shared goals, cultures, and relationships across different professions up to different organizations. Therefore, much emphasis and support are needed and, for example, work process interventions such as structural interventions to improve the flow of information and as innervated by Gittell, also through expanded professional roles such as care coordinators for patients and for health professionals who could help to facilitate innovation and reduce wasted time and care. The authors suggest a focus on organizational dimensions to come to “good practices” in the process which would help aligning both care content and care organization. 7 We would like to add that their suggestions can be taken into account/applied on changes for both, in- and outpatient care organization.
When health professionals jointly work together with each other or are offering interprofessional care for patients, Reeves et al. propose to apply a so-called “contingency approach” to be flexible to adapt to meet particular needs of patients, remain adaptive to different contextual influences and to available resources. According to them, working as a team is only one form of working together. Other forms are collaboration, cooperation, and networking.8,9 The authors further have elaborated a framework for interprofessional teamwork in which they have integrated common elements of teamwork identified in the literature of more than 20 years and assigned to relational, processual, organizational, and contextual factors which, according to them, possibly affect the teamwork itself. These factors can be seen as possible sites for intervention to enhance or impair teamwork. 10
In their systematic review on experiences and shared meaning of teamwork and interprofessional collaboration among health-care professionals in primary care settings, Sangaleti et al. have listed as recommendations for health-care practice, referral and counter-referral arrangements and to know that goals shared with others serves to answer health-care needs of patients. 11 In their review on interprofessional collaboration in outpatient care, Supper et al. identified some similar factors such as Reeves et al. as main barriers. As main facilitators, the authors identified when different actors acknowledge the potential to ameliorate quality of care and extend their scope of duties. 12
In a patient engagement survey of the NEJM Catalyst Insights Council 13 on “what creates behaviour change may not sustain it,” only “in person social support” was identified to be an important factor as well when starting and even for maintaining behavior change. More education about preventable conditions according to them seems to be important only at the beginning, while a virtual social support, electronic reminder and personal technology devices become more important during maintenance of the behavior change process.
In summary, a move toward an active involvement of patients in the care process will have consequences on service delivery itself and an aligned collaboration between different professions in the health-care sector is one of the requirements. All these abovementioned proposes of change could or should be pulled together and before interventions are being activated, they should be carefully planned and adapted to local context.
Therefore, the aims of this study were to explore as follows: (a) In current outpatient care of family physicians, nurses, and dieticians is it an objective to communicate/collaborate with each other? (b) How far do the involved health professions (HP) collaborate with each other to give patients with DM2 support in changes to be performed by them in eating and physical activity habits? (c) How are the attitudes of patients with DM2 to cope with these behavior changes? (d) To what extend for patients collaboration between HP is central?
As there does not exist an agreed definition of “alignment” in the literature, we refer to it as how current service delivery in outpatient health care should be adapted and changed to warrant a more patient centred care, with better distributed (human) resources and reduced rate of errors.
Methods
Study Design
We conducted qualitative problem-centered interviews according to Witzel 14 with single providers or executives of the included health-care professions (HCPs) and with patients with DM2. We wanted to explore contextual factors and experienced strong- or weaknesses of the current organization of communication/collaboration with DM2 patients and among the health professions in the outpatient care setting.
Setting
The study took place in a bilingual (German/Italian) province in northern Italy in which a population of slightly more than half a million inhabitants is served by 1 health trust comprising 20 community health districts (outpatient care) and 7 hospitals, distributed on 4 health districts. Outpatient nurses and dieticians are working as employees of the health trust. Family physicians are working as freelancer in the different health districts, considered according to the Italian health-care system as gate keepers for secondary and tertiary care. In current regional health plans,15,16 the outpatient/primary health care is under reform and will be strengthened and care pathways for chronic diseases such as DM2 are being introduced.
Criteria for Selection of the Sampling
The interviewed health professions had to be key people in Diabetes care or be key informants about applications of the current health-care reorganization and had to work in the outpatient health-care setting.
Sampling of Participants
Eligible HCPs were family physicians (general practitioners, GPs), nurses, dieticians as well as patients with DM2. General criteria for selecting interview partners of all 3 health professions where being female or male, located in urban or rural area, length of working experience in the setting. The first family physician was approached randomly in an informal meeting of the setting, and next physicians were selected accordingly to general criteria plus working alone or in a group practice of GPs. Nurses were approached through an executive in the outpatient care setting with the function of a door opener. Dieticians were approached directly by the first author, as she was formerly coordinating the bachelor’s degree (education) of dieticians. Patients were approached through the interviewed family physicians.
Data Collection
Purposeful sampling according to Palinkas et al. 17 was adopted in the following manner: A first phone call with a potential interview partner of all included professions was conducted to give general information about the study, find out about the willingness to be interviewed and in a positive case a date at the location of the interviewee for the interview itself was agreed. Before the interview was sent by email a written information sheet about the study itself to every participant and confirmed the accorded date. Before starting an interview at the location of the professionals, every interviewee had to sign a prepared written and orally explained informed consent sheet/form, with which was also agreed the digital audio recording of the interview. The first author conducted all interviews using a semistructured interview guide according to Witzel. 14 . In the interview guide were addressed the main areas of interest such as how and if current practice of health care is centered on patient’s needs. We wanted to know whether and how interprofessional collaboration is practiced to target changes in eating and physical activity habits by the different health professions involved. The interview guide was adopted after new insights and personalized to fit the different health professional’s roles in diabetes care. For interviews with patients, the participating family physicians had to contact a person with DM2 and to agree with them about being interviewed. After this essential step, the first author had the permission to contact the person directly to according the date of the interview at patient homes.
After every interview, the first author made field notes as a possibility for self-reflection and about the general impression and conduction of the interview. All audio recordings were reheard by the first author to gather themes (and direction) to question in further interviews. After 18 interviews no new concepts (stories) emerged and it was deemed to have collected enough information and that was interpreted to have reached data saturation. All interviews were conducted between March and August 2018, where audio recorded, transcribed verbatim and had an average duration of 45 minutes, ranging from 21 to 92 minutes.
A respondent and content validation was obtained through 1 group session and other 2 individual consultation sessions with the single members of the research support team. The latter was composed of all professions and patients with the function as a guarantor for context knowledge and had to ensure to adopt a realistic perspective of the field. 18
Data Analysis
The audio recorded interviews were transcribed verbatim. Transcripts were pseudonymised and read carefully by the first author and afterwards uploaded together with the audio files in MAXQDA software (analytics pro12) for qualitative content analysis according to Kuckartz et al. 19 A first step in data analysis was the immersion into the data with a focus to reflect and search for central parts of each interview to respond the research questions and to summarize the relating essential findings. In this step, we paid attention not to focus too quickly only on these central parts, but to look at the whole text and what of that was important to better understand the context of the setting. In a next step, these parts of the interviews were labeled with few words (coding) which described best the content of the paragraph concerning. Afterward, the focus was creating categories that connected more codes under a sort of umbrella. Specifically, as suggested by Green et al. 20 in a further step of the analysis, we were mainly concentrated on finding themes.
In our study, accordingly to the above-cited authors as a first analytic step, we explored the sights and perspectives of the single health professions and patients to gather/capture possible patterns and themes specific for and to them. In a second step, we looked for similarities and differences between the single perspectives and focused to link them to context and process of work in this setting/field.
Research Ethic Committee and Data Oversight
The ethical committee of the South Tyrolean health trust gave positive approval of the study (no 08/2018). Participation was voluntary and informed consent was signed before every interview.
Results
The encoding of the interviews led to nearly 600 codes. From these, the following categories/themes were then created: The issues were ranging from “description of and reflections about current practice” (Tasks/activities/responsibilities of professional groups/services/patients -what and how could it be done?). In addition, further issues were assembled to “strategies” or “hindrances” to cope with changes of eating and physical activity behaviors, (both for health-care practice regarding interprofessional collaboration and patient-centered care). Other topics were labeled as “considerations about collaboration and patient centricity” (likewise for health professions and patients to achieve goals) and changes and ideas of “ideal care practice” the latter could only be assigned to HCPs (Figure 1).

Overview of Characteristics of the Study Sample.
In the following section, we display the obtained results according to how the single HCPs and patients described themselves regarding their role and tasks in current health-care practice according to some of the abovementioned categories/themes.
Family physicians described themselves to be the first contact point for diagnosis of DM2 which they verified through the prescription of blood glucose testing. Their role was seen to monitor these afterwards in control visits. How regularly these visits had to be were described to be dependent on patients’ clinical outcomes and depending on patient’s integration in the referring specific diabetes center situated in a hospital. Often in the interviews was described an implicit indirect but concerted contact with the diabetes center situated in the hospital and we had by and large the impression of competences between them being quite clear.
Nurses, working in outpatient health care currently seemed not to be integrated in the caring process for Patients with DM2 without any complications. They were normally rarely involved, only, for example, blood sampling, wound care for ambulatory patients, and so on.
Dieticians in outpatient care reported that for them it is very important that patients could come regularly to them and not only once. They said that their task is to do a nutritional and a general physical activity anamnesis and for them seemed to be very important that patients do communicate even about their critical situations with them.
Patients interviewed described themselves as being differently able to cope with their symptoms of DM2, all had the disease since at least 6 up to 16 years. All of them stated to regularly take the prescribed medications, to have a good relationship with their general practitioner and to furthermore be under good “control” of the diabetes center in the hospital. They had contact with a dietician at most only when being diagnosed.
In Table 1, we present meaningful statements of the different interviewees according to the most frequent categories/themes assigned.
Tasks/Activities/Responsibilities of Interviewees assigned to Themselves.
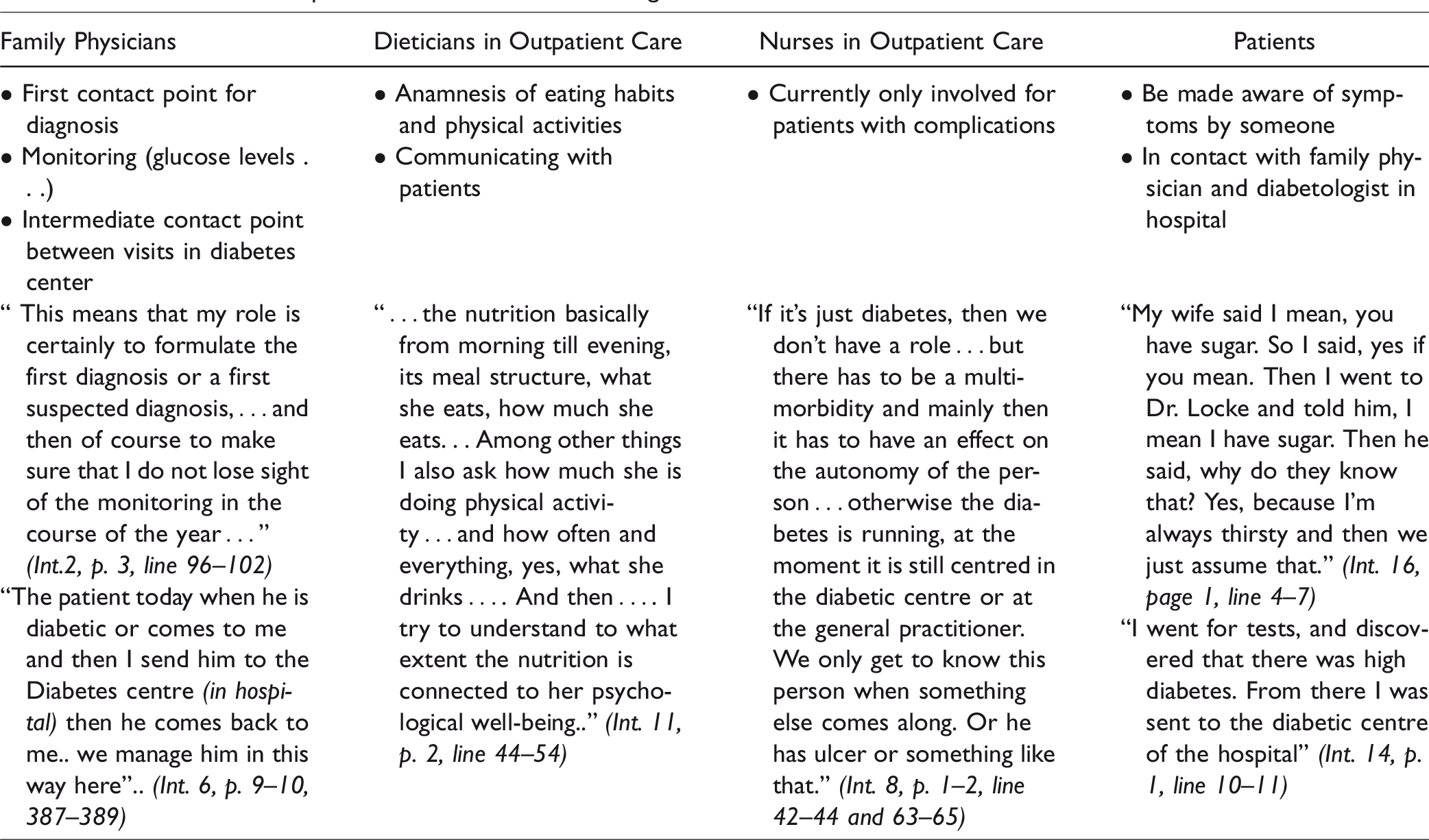
Table 2 describes some of the emerged meaningful ideas the different interviewees had on what and how current health-care practice should be changed.
What and How Tasks/Activities/Responsibilities Could/Should be Performed.

In the following, we present themes discussed/explored during the interviews by the different HCP referring to challenges in their current health-care practice. For them, hindrances were more in the foreground as is depicted trough the statements below.
Perceived “hindrances” for Interprofessional Collaboration in Current Health-Care Practice by Different Health Professions
For family physicians seemed to be a challenge to see the potential of collaboration only in extreme situations as it is described through the statement of a female doctor working in group practice in a rural area. It is then also sometimes, if really overweight people,. . where they (the patients) also then say themselves, … it has been really long that I try to lose weight and I have already tried this diet, then it is also difficult for me (as a doctor), because then I notice it is already a certain frustration there arose with the patient … therefore I must also say that I send her to a diet consultation also. I really have to say that I already sent some then, actually, with the professional support when I really see it is a really severe obesity. (Int. 3, p. 6, line 226–234)
While a dietician working in an urban community district stated that a great problem is that different HCPs give different information (no concerted action). . . it's just important, very important, I'd like to emphasize that, . .that the team doesn't give different information, that the doctor doesn't say, you have to leave out the carbohydrates because that happens with the family doctors because some diabetics are very likely only cared for by family doctors or at least once as a first step and there are many family doctors who unfortunately at the moment when diabetes is diagnosed recommend to leave out the carbohydrates, so all carbohydrates pasta, rice, bread and so on and that's, that's a big problem. This is a very big problem and it is even bigger if it happens in the same house, … so if it happens in the hospital. If in a diabetological service the doctor says this and the dietician says the opposite, that cannot be. That must not be at all. (Int.1, p. 9, line 367–371)
A female nursing leader responsible of an urban part of a health district pointed out that currently every service in and outside of health care for patients with DM2 is working against the other. So according to her, there is too little trust between the different stakeholders and therefor networking is not possible. this is the next island, you know? And I don't think that's possible. Because we nearly go into competition then. You know I've experienced when (we introduced) Evviva … (Self-management), were some from the Diabetikerbund (patient association) and how they negatively (reacted) on the health offers … , then I think, then I do not help the diabetic … who does go in there … Then I take away the trust in the system. … Because he (the patient) falls into the system again and again. And I think that's what's important, that we manage that. (Int.8, p. 20, line 836–842)
“Strategies” or “hindrances” of Patients to Cope With Changes of Eating and Physical Activity behaviors
Some patients seemed to have no problem to change their habits, while others described themselves as resistant. Now I had it once … I don't know what it was. There I had had it again at 200, once at noon. Then I got dressed and left. So, I thought to myself, because if I go and I go almost every day, if it is somehow possible, I go every day into the forest or so and then it goes down again. (Int. 17, p. 4, line 166–170) Because if they tell me to come and collect this, collect that, I'll go even if there is to walk half a day. But walking like this with your hands in your hand, just to say walk, seems to me an absurd thing. (Int. 15, p. 7, line 259–261)
As an example, we report in the following statement of a family physician how intricately/entangled change in HC-practice will be. Physical activity at which I recommend, to move a little more, but I repeat, in my opinion it is there that we should work much more as a whole outpatient area, as doctors, nurses, etc … but you cannot do it in a traditional surgery. (Int.6, p. 4, line 157–159)
To sum up, all health professionals interviewed, considered changing eating and exercise behavior of patients with DM2 as their responsibility. All claimed that these would be part of their field of activity. At the same time, it seemed that in current practice in outpatient health care, however, it is not an issue/theme/task for the health professions to give support when patients have to change their eating and exercise behaviors. This is not true for dieticians, because they are explicitly responsible for it.
Discussion
As we explored above through the description of the obtained results, the current collaboration between the 3 included professional groups is poorly developed as can be expected because of the health-care structure. The health professions work predominantly for themselves. Interprofessional collaboration according to the Canadian Def. 2012, in which several (health and social) professions meet on a regular basis to ensure optimal care, drawing on the competence/expertise of the other professions certainly cannot be spoken of. For example, family physicians did not transfer to other services or professions. Some of them knew about other programs such as EVVIVA D (self-management courses for and ideally with patients with DM2 according to Stanford Patient Education Research Center), but described that as being impossible or for them not actively promotable. This could be the NIH (not invented here)-syndrome. 21
GPs are the only health professions who in current Italian outpatient health-care system continuously/regularly have contact with the patients. They could therefore play a key role in the "allocation/assignment" of patients to other health professions because of their long-term role in care. This can be for both, changing eating and exercise behavior and for collaboration between the professional groups if they would recognize their professional limits/boundaries. However, this behavior can only be seen in rare cases, their priority is to monitor clinical parameters and medication adherence (medication intake).
In our findings, health professions in the outpatient health care of patients with DM2 seemed to life in separate worlds. The patient is the one transferring the communication between their separate “islands.” However, due to an overall work pressure, health professionals do not see to need to change the situation.
A holistic care for DM2 patients not only monitoring the HbAa1c values but also actively working with them on behavior change is only provided by chance and not structurally supported by interprofessional collaboration. This is in line with Borgermans et al. 6 where envisioned opportunities are to upscale noncommunicable diseases in outpatient care. The study at hand wanted to better understand some of the existing local barriers for “multidisciplinary team-based outpatient care services, goal-oriented care” and to explore how coordinated and integrated the service delivery currently is. This is an important step before planning interventions and for adapting them to local context and was scope and focus in our study. In the topical Italian plan for chronic diseases, 22 it is acknowledged that treatment of pluripathologies requires the intervention of different professional figures, but there is a risk that the individual professions intervene in a disjointed way, focusing the intervention more on the treatment of the disease than on the management of the patient as a whole person. This sometimes leads to conflicting/contradictory solutions, with possible diagnostic and therapeutic duplications contributing to the increase in health expenditure. Referring to the ability to cope with permanent/stable changes in the national plan health professionals are described as equally challenged as patients are. According to Reeves et al., health professionals should realize when to work (act) as a team, or in a collaborative, or in a coordinated way with other professions from in or outside of their own working reality and when they should function as a network. For adapting and adopting to the “contingency approach” introduced by them, 8 it would be necessary to define individually, that mean for every patient, which form of collaboration between which health professions would be most appropriate and necessary in our case in the outpatient health care. Currently, competition between different health professions seems to be an obstacle to do so, we noted the attitude of “I can do that too, it's ‘only’ about healthy nutrition” from all professions interviewed.
The potentials of the other health professions are not seen and therefore cannot be exploited. This is in our point of view a contingency/conditionality issue: If family physicians do not consider diet and exercise as to be important/to be changed, they therefore will not refer to other health professions. Some recommendations Sangaleti et al. listed for health-care practice such as referral and counter-referral arrangements and to know that goals shared with others serves to answer health-care needs of patients 11 are lacking areas in our reality.
Considering the prerequisites for functioning collaboration identified by Reeves et al. 8 as a standard to achieve and main barriers and facilitators described by Supper et al. on interprofessional collaboration in primary care, there is still much to do for different actors acknowledgement of their potential to ameliorate quality of care. 12
At first glance in our study, there is no discernible need for aligned collaboration between the different professional groups. “It's temporally not possible” and the professions even do not think it makes sense for avoiding long-term complications. Patients do not demand it either. They are satisfied as it is—and patients do not know anything else. A problem that only dieticians perceived as was when health professions give different or even contradictory information. The patients here were in the role of whistle-blowers or deliverer, thus the professional groups may be informed about through them. This could be interpreted as a sign of working like in ancient times or as we would prefer to be a signal for change needed in health-care practice and approaching to tasks, responsibilities, but to be successful had to be applied in a concerted manner as suggested by Fitzgerald and McDermott. 23
Turning to the point of which ideas have been described by the different health professions as a change toward “ideal health care practice” it became evident that nobody criticized the own mode of working be it from the organizational or from the content standpoint. The ideas of family physicians to “train” their assistant to do routine activities or to have nurses at their hands or organizing sessions on specific topics for specific patient groups were formulated as hypothetical and not as goals for them. It seemed to us that our interviewees were furthermore/additionally frustrated by often announced and never “realised” local or national Health Care (HC) reforms/projects and that they had no voice in the change process itself. Their resistance could also be a sort of helplessness of not knowing how to adapt and be let alone (it does not matter if I change something, it is no use anyway.). Nurses seemed that they would like to take over tasks of family physicians and dieticians if they would be involved in the activity at stake. The “requests” seemed rather hypothetical assumptions, but what would be (how would they behave) if something would change in practice? “Changing the others” is always easier than changing oneself meant as the own way of working (referring to social support, and needed organizational support Gittell 24 ). A systematic review on how HCPs contribute to interprofessional collaboration 25 summarized the existing evidence, which the authors described as limited and fragmented. Nevertheless, the contribution of HCP was characterized to overcome different kind of gaps by managing intersections/duplications and by finding the time and place to overcome them. In line with Gittell et al., further emphasis to study these activities therefore would be needed in the everyday routine work of HCPs. 25
Strengths and Limitations
Through our study, we explored some details about the perspective and description of the real-world experience of 3 different HCPs and patients with DM2 in a local area of Northern Italy. We were interested in their point of view on 2 lacking/underserved areas/crucial points of current and future health-care practice for chronic patients, namely, focusing on lifestyle and disposition to change and analyzed the results across them. Although we have captured the problem we have not found a satisfying solution. The sample size in our qualitative study was small and the aim was the exploration and not generalizing of findings. Therefore, we would recommend for future research to build with quantitative data on it and focus at comparing with other realities.
Conclusions
Collaboration does not simply just happen. It currently takes place because individual professionals want to happen it and neither structured nor organized. At present, collaboration seemed inadequately supported organizationally and processual and the “system” is currently not demanding for a coordination or distribution of competences between the professional groups. Collaboration currently is not seen connected with the outcomes of patients by the involved health professions, they are living on their own island.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.