
Abstract
Background
Pharmaceutical care (PC) practice in Ethiopia is not well developed and is at its infant stage. As a result, very little is known about the level of involvement of pharmacy professionals in PC activities.
Objective
The aim of this study was to assess PC practice at drug retail outlets (DROs) of Gondar town and to identify factors associated with it.
Method
A cross-sectional study was conducted on 150 pharmacy professionals working in 55 DROs located in Gondar town, Northwest Ethiopia. Data on sociodemographic characteristics of respondents, their involvement in PC activities, handling of drug-related problems (DRPs), and consultation with colleagues and other health-care providers were collected and analyzed using statistical package for social sciences (SPSS) version 21.
Results
Majority of study participants were degree holders in pharmacy (68.7%) and work in community DROs (78%). Over half of the respondents (56.5%) were found to practice good PC, asking at least 3 of their last 5 patients what the goal of their drug therapy was. Nearly a quarter (24%) of pharmacy professionals did not document the desired therapeutic objectives for all the 5 patients they served. Handling of DRPs is poor for majority (76%) of the pharmacy professionals. Respondents working in the community DROs and diploma holders are poorly involved in PC activities. Age < 30 years, male sex, and working in the community DROs are significantly associated with poorer relation with colleague and other health-care providers.
Conclusions
Pharmacy professionals working in DROs of Gondar town have little involvement in the provision of PC. Especially, their handling of DRPs is very poor. The level of involvement of pharmacy professionals on some types of PC services was significantly associated with their sex, age, working site, and level of education.
Introduction
Health-care professionals play major role in striving for health in a population. The effort of each member of a multidisciplinary health-care team is essential for achieving therapeutic goals in disease manegement.1,2 Pharmacy professionals, as a member of health-care team, play a vital role in the health-care system through the medicine and information they provide. 3 Recently, the role of pharmacists is expanding globally from mere dispensing of medication to playing a key role in disease state management, patient monitoring, and resolving drug-related problems (DRPs). 4 An increase in health demand with a complex range of chronic medicines and poor adherence to prescribed medications forces the pharmacy profession to continue to move toward a patient-centered practice.5,6
The paradigm shift for pharmacy practice took turn in 1990, when Hepler and Strand introduced the term “pharmaceutical care,” which shows the patient as a focus of pharmacy practice.7,8 Pharmaceutical care (PC) is the responsible provision of drug therapy for the purpose of achieving definite outcomes that improve patient’s quality of life which represents growth in the profession beyond medication preparation and dispensing.7,9 It blends a caring orientation for the purpose of ensuring optimal outcomes which are cure of a disease; elimination or reduction of a patient’s symptom: arresting or slowing of a disease progress; or preventing a disease or symptom. It involves the process through which a pharmacist cooperates with a patient and other health-care professionals to prevent, identify, and resolve DRPs. 8 So the principal expected task of the modern pharmacy professional is to identify, resolve, and prevent DRPs.
This new and expanded role of pharmacists which evolves over the past 4 decades globally is introduced in Ethiopia very recently. Ethiopia has gone through various efforts to launch this role in Ethiopian health-care system. This starts with harmonization and implementation of the new clinical-oriented undergraduate pharmacy curriculum in 2009 followed by the endorsement of different standards and national guidelines such as the Ethiopian Hospital Reform Implementation Guideline which allows the practice of patient-oriented pharmacy service within the nation’s health-care system by indicating direct cooperation between physicians and pharmacists.10–12 However, what is written in the reform guidelines is hardly seen on the actual practice due to the fact that direct patient care in Ethiopia is still exclusively in the hands of physicians which makes pharmacists’ input in managing drug therapy ultimately dependent on physicians’ receptiveness to pharmacists’ role. Moreover, the perception of the general public regarding this role of pharmacists is weak. 13 So PC practice in Ethiopia is not fully implemented, not well developed, and is at its infant stage. As a result, very little is known about the level of involvement of pharmacy professionals in PC services. Studies conducted in the area are also rare. The aim of this study is to assess pharmacy professionals’ involvement in PC activities, handling of DRPs, and consultation with colleagues and other health-care providers and to identify factors associated with these PC services. The result of this study will provide baseline information to policy makers, public health agencies, and researchers to understand the status of this new role of pharmacy professionals in Ethiopia.
Methods
Study Area and Period
The study was conducted in Gondar town which is found 727 km North West of Addis Ababa, the capital city of Ethiopia. Gondar is the fourth largest city in Ethiopia. The total population of the town in 2017 was estimated to be 358 257. The town has 1 referral hospital affiliated to one of the main health science colleges in the country, 2 privet hospitals, 5 health centers, 20 pharmacies, and 35 drug stores. Most of the pharmacies and drug stores have at least 2 pharmacy professionals as a full-time staff. The study was undertaken from March 20 to May 30, 2018.
Study Design
Cross-sectional survey was conducted using a structured self-administered questionnaire distributed to pharmacy professionals working in community and institutional drug retail outlets (DROs) found in Gondar town.
Study Subjects
Pharmacy professionals working in Gondar town who were at least diploma holders in pharmacy education and willing to participate in the study were included as study subjects. Those who were not available at work site on data collection day were excluded from the study. A total of 160 pharmacy professionals gave consent to participate in the study. One hundred fifty of them filled and returned the questionnaire.
Operational Definitions
Institutional DROs: pharmacies and drug stores located in hospitals and community health centers.
PC: a patient-centered, outcomes oriented pharmacy practice that requires the pharmacist to work in concert with the patient and the patient’s other health-care providers to promote health; to prevent disease; and to assess, monitor, initiate, and modify medication use to assure that drug therapy regimens are safe and effective.
Pharmacy professional: experts on drug therapy and the primary health professionals who optimize the use of medication for the benefit of the patients.
Poor provision of PC: providing PC during dispensing of prescription and proper handling of DRPs for at most 2 patients out of last 5 patients and consulting with colleagues and other health-care providers in “not at all,” “almost never” and “sometimes” manner.
Good provision of PC: providing PC during dispensing of prescription and proper handling of DRP for at least 3 patients out of last 5 patients and consulting with colleagues and other health-care providers in an “often” and “very often manner.”
Data Collection Instrument
The data collection instrument was a structured self-administered questionnaire which was developed based on review of the relevant literature.14–16 It consists of 2 parts which comprised 11 questions to address the sociodemographic characteristics and 27 closed-ended questions to measure PC practice. The second section is divided in to 3 subsections each addressing the different aspects of PC service. The first subsection is about the level of involvement of pharmacy professionals in PC activities during dispensing of new or refill prescriptions; the second is about handling of DRPs. The last part is about pharmacy professionals relation with colleagues and other health-care providers in matters related to PC which was measured using 5-point Likert-type scale responses (0 = not at all, 1 = almost never, 2 = sometimes, 3 = often, and 4 = very often). Each study participant was requested in the questionnaire to think about the last 5 patients or customers who presented a prescription, the last 5 patients or customers who he/she discovered were experiencing DRPs and all the patients he/she saw in the past 2 weeks before the study period to respond to questions in the first, second, and third subsections of the second part of the questionnaire, respectively.
Data Quality Assurance
The questionnaire was assessed and approved for face validity by the study authors then pretested on 8 pharmacy professionals (4 from institutional pharmacy and 4 from the community pharmacies and drug stores) and after a thorough and deep review of inputs obtained during the pretest some modifications were done before distributing the questionnaire for data collection.
Data Analysis
The filled-in forms were checked for completeness of data, cleaned prior to data entry and entered into the computer, and analyzed by using the Statistical Package for Social Sciences (SPSS) version 21.0 for windows (SPSS Inc., Chicago, IL). The results were described using descriptive statistics in terms of frequencies and percentages values. In exploring the association of variables, the 5- or 6-point scale was recoded into “poor” and “good.” Binary logistic regression was performed to show possible associations between the dependent and independent variables, and the odds ratios were estimated at 95% confidence intervals. In all tests, the association was declared significant at P < .05.
Ethical Considerations
An ethical clearance was taken from the Ethical Review Committee of School of Pharmacy, University of Gondar, and all respondents were asked for their consent before participation in the study and each pharmacy professionals was informed about the objective of the study and confidentiality was assured. Thus, name and address of the pharmacy professionals were not recorded in the data collection instrument (questioner), and the collected data were used only for the purpose of the study and only aggregates of data were reported.
Result
Description of Respondents
One hundred sixty pharmacists and druggists working in a community and institutional DROs located in Gondar town gave their consent to participate in the study. One hundred fifty completed and returned the questionnaire making a response rate of 93.75%. The mean age of respondents was around 31 years with the majority being male (54.0%). More than three-fourth (78%) of the professionals are working in a community pharmacy setting. Nearly one-third (31.3%) were diploma holders in pharmacy education, and the rest had bachelor of pharmacy degree. Most of them (51.3%) had work experience of ≤4 years. The average number of working hours per day and the average number of working days per week were found to be 8.45 hours and 6.17 days, respectively. Relevant information on sociodemographic characteristics of the survey participants is summarized in Table 1
Demographic Characteristics of the Respondents (N = 150).

Abbreviation: BPharm, bachelor of pharmacy.
PC Practice in Drug Retail Outlets of Gondar Town, Ethiopia
The provision of PC for the last 5 patients who visited the DRO with new or refill prescription is indicated in Table 2. Nearly two-third of the professionals verified the understanding of at least 3 of the 5 patients for whom they presented the information by asking for feedback. More than half of the respondents (56.5%) had a good trend of asking at least 3 of the 5 patients about what they wanted to achieve from the drug therapy. However, 79.3% and 61.3% of them documented the information about medical condition and current medication for a maximum of only 2 of the 5 patients they served, respectively. Nearly, a quarter (24%) of pharmacy professionals documented the desired therapeutic objectives for none of the patients they served. Only 5 (3.3%) professionals asked all the last 5 patients with refill prescriptions whether DRP was experienced.
Pharmaceutical Care Activities Provided for the Last 5 Patients With New and Refill Prescriptions.

As shown in Table 3, more than half of the pharmacy professionals documented DRPs and interventions they made for a maximum of 2 of the 5 patients. Only 44% of the professionals implemented a strategy to resolve or prevent the DRP for at least 3 of the last 5 patients. Nearly two-third of the respondents carried out the follow-up plans established for the patient’s progress toward the patient’s drug therapy objectives for maximum of 2 patients of the last 5 patients they served.
Activities Done to Properly Handle Drug-Related Problems for the Last 5 Patients Served by the Pharmacy Professionals.

The results for consultation with colleagues and other health-care providers were reported as not at all (0), almost never (1), sometimes (2), often (3), and “very often” (4). As indicated in Table 4, many pharmacy professionals (64.1%) had a poor (not at all, almost never, or sometimes) discussion with physicians whenever one of their patient was having drug therapy problem. More than half (52%) of the professionals did not provide written copies of patient information to professional colleagues authorized to have such information in an often or very often manner. Nineteen (12.7%) respondents reported that up on referral they did not provide physicians a written summary of the patient’s medication history and any related problems at all.
Pharmacy Professionals’ Consultation With Colleagues and Other Health-Care Providers.

When dichotomized as poor and good, among the 3 PC service domains, handling of DRPs is poor for majority of the pharmacy professionals working in DROs of Gondar town (76%). Less than half (47.3%) of pharmacy professionals had good practice for consultation with colleagues and other health-care providers.
Factors Associated With PC Practice
Working site and academic qualification have significant association with involvement in PC activities. Those respondents who are working in the community DROs were found to have poor involvement than those who are working in institutional DROs and those who have diploma in pharmacy had poor involvement than degree holders in rendering PC for patients with new or refill prescriptions. A group difference was also found with regard to the activities that are carried out to solve or prevent DRPs based on sex and marital status. Male pharmacy professionals had significantly poor handling of DRPs than females. Singles were found to have good DRP handling than married pharmacy professionals. Sex, marital status, working site, and age significantly affected respondents’ relation with other pharmacy professionals and health-care providers. Respondents aged < 30 years, married, males, and those working in the community DROs had poorer relation with colleagues and other health-care providers than the respondents aged ≥ 40 years, singles, females, and working in institutional DROs, respectively. The detail of factors associated with PC practice is shown in Table 5.
Factors Associated With PC Practice.
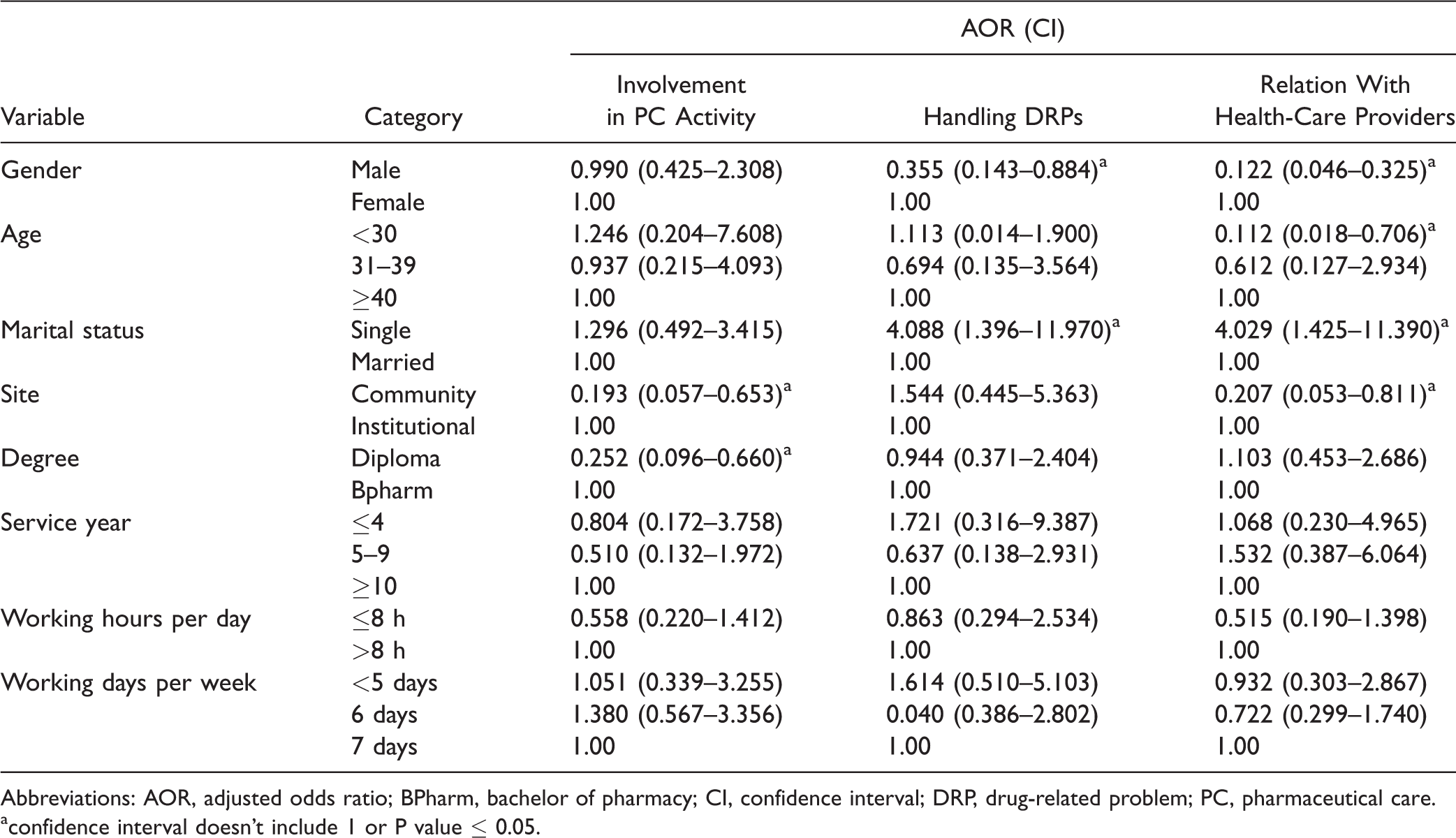
Abbreviations: AOR, adjusted odds ratio; BPharm, bachelor of pharmacy; CI, confidence interval; DRP, drug-related problem; PC, pharmaceutical care.
confidence interval doesn't include 1 or P value ≤ 0.05.
Discussion
PC has been viewed as one of the most important roles of the pharmacy professionals and, when appropriately implemented, has been shown to have a positive clinical, economic, and humanistic outcomes.8,17 This study assessed the level of provision of PC by pharmacy professionals across DROs of Gondar town. Three dimensions of PC practice were described in this study: (i) involvement in PC activities for new and refill prescriptions, (ii) handling of DRPs, and (iii) relation with colleagues and other health-care professionals.
This study overall result revealed that pharmacy professionals working in Gondar town had a poor documentation, patient counseling, and drug monitoring activities, which is consistent with other studies, which concluded that the number of patients receiving PC service was relatively low and only implemented to a limited extent.18–20 In Cuba, which has almost comparable health-care system with those of developing countries, the PC practice has not yet been developed by pharmacists in their daily practice. 21 Although the concept of PC is sweeping over the pharmaceutical world, not much of it has been implemented. Previous studies conducted in Ethiopia also revealed that community and hospital pharmacists involvement in public health services are poor.22,23
The level of involvement of pharmacy professionals in Gondar town on some types of PC services was influenced by their sociodemographic characteristics like sex, marital status, educational level, working site, and age. Male pharmacists were found to be significantly less involved than females in activities used to solve and prevent DRPs. They also have significantly poor relation with other pharmacists and health-care providers than females. These findings are consistent with the result from a previous study which reported that female pharmacists were significantly more involved than males in providing general health promotion services and significantly highly rated the quality of service they provided as compared to males. 24 Although this study assessed self-reported level of involvement of pharmacists and druggists, it seems that males were less involved in the activities that should be carried out to handle DRP and in cooperating with other health-care professionals. So we recommend further study to find out specific barriers unique to these groups. The possible explanation for single pharmacy professionals to have good practice in handling DRPs and good relation to other health professionals is that single pharmacy professionals may get more time to read and check updated guidelines, books and drug information websites than married ones which are expected to be busy with their family life. The more the person updates himself/herself with recent disease and drug-related information the more confidence he/she will have to addressing DRPs and interact with his colleagues and other professionals in matters related to the practice of his profession.
Diploma holders claimed to be significantly less involved in rendering PC service for both new and refill prescriptions than those who have degree in pharmacy. A previous study also revealed that community pharmacy professionals with a qualification of degree or above had a significantly higher level of public health service delivery than those having diploma. 22 In this study, pharmacy professionals who are working in the community DROs were significantly less involved in rendering PC during dispensing of prescription drugs and also had poor consultation with colleagues and other health-care professionals than pharmacy practitioners in the institutional setting. This may be because practitioners in the community DROs have limited access to patients’ clinical records with which to monitor drug therapy and confidently interact with physicians and nurses than do institutional pharmacists. This may also be due to the fact that a significantly larger proportion of institutional pharmacy professionals in our setting had degree in pharmacy than those working in community DROs and with this the level of education was found to have a significant relation with involvement in PC activities. Erku and Mersha emphasized that community pharmacy professionals’ involvement in PC in Ethiopia is severely limited such that they mostly involved in activities pertaining to the dispensing of medications and have less intense involvement in public health activities. 22 The same holds true for previous studies conducted outside Ethiopia which revealed that institutional pharmacy professionals more frequently monitor drug therapy than pharmacy professionals in the community setting.25,26
Relationship of pharmacy professional with other health-care provider, especially with physician, is one of the most important concerns in implementing PC in different countries. However, the majority of respondents were found to have poor communication and relation with colleagues and other health-care providers. Among all activities, the trend of referring patients to pharmacists and physicians was rated as good. However, pharmacy professionals were found to have poor discussion with physicians whenever their patients were having DRPs which is consistent with other studies which reported that majority of the pharmacy professionals never or rarely had interactions with physicians with regard to their patients’ medications and their collaboration with colleague pharmacists in preventing and resolving negative outcomes associated with medication problems was low.27,28
The interpretation of the result of this study should be done by taking the following limitations in to consideration; (i) it is a single center cross-sectional study so that the result may not be generalized to other settings. (ii) Data was collected through self-administered questionnaire so that its geniunity depends on the honesty of respondents and social desirability bias may be involved.
Conclusion
The finding of this study had implied that pharmacy professionals in Gondar town are less involved in the provision of PC. Especially, their practice of activities needed to properly handle DRPs is very poor. The level of involvement of pharmacy professionals on some types of PC service was significantly associated with sex, working site, educational level, and age of pharmacy professionals.
Footnotes
Acknowledgments
The authors are very grateful to our study participants for giving their time in filling the questionnaire.
Authors’ Contributions
MBA had participated in concept development, questionnaire design and write up of the final research and manuscript preparation and finalization. LS and SA had contributed in data analysis, interpretation, and write up of the research.
Consent to Publish
Participants consent was taken to publish this work.
Data Accessibility Statement
The data sets during and/or analyzed during the current study is available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Ethical Review Committee of School of Pharmacy, University of Gondar. The respondents were informed about the purpose of the study and their verbal consent to participate was obtained.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.