
Abstract
Introduction
Lung cancer patients and their caregivers are at risk for negative health behaviors and poor psychosocial functioning, but few interventions exist that target this population. To inform intervention development, we explored potential targets and interest and concordance in health promotion interventions among lung cancer patients and their caregivers.
Methods
Lung cancer patients (n = 18) with a smoking history and their caregivers (n = 15) participated in a cross-sectional, observational survey study (an average of 1 month postdiagnosis) to assess health behaviors, psychosocial functioning, and interest in health promotion interventions. Fisher’s exact and Wilcoxon rank-sum tests examined factors associated with intervention interest. McNemar’s test examined concordance in interest.
Results
Many caregivers (40%) reported providing care at least 4 days per week, and over half (53.3%) reported a smoking history. Patients reported high cancer self-blame (mean = 3.1, standard deviation = 0.9, range = 1–4). Patients (55.6%) and caregivers (60%) reported clinically significant depressive symptoms. There was high interest and concordance in interest in cancer education (patients, 77.8%; caregivers, 86.7%) and diet and exercise (patients, 66.7%; caregivers, 80%) interventions. Significantly more caregivers were interested in stress reduction (patients, 53.3%; caregivers, 73.3%; P = .05) and yoga (patients, 16.7%; caregivers, 50%; P = .03) than patients. Caregivers interested in stress reduction interventions had higher levels of distress than those not interested.
Discussion
Health promotion interventions are needed and of interest to lung cancer patients and caregivers. Shared interests in interventions suggest dyadic interventions may be appropriate, yet interventions should also address distinct patient and caregiver needs.
Introduction
Lung cancer is the second most common cancer and leading cause of cancer death among men and women in the United States. 1 Over 230,000 people will be diagnosed with lung cancer this year alone. 1 Given screening initiatives and treatment advances, the number of people living with lung cancer is expected to grow, yielding a substantial population with complex care needs. 2
Compared to patients with other solid tumors, lung cancer patients have more comorbidities, 3 poorer quality of life,4,5 more unmet supportive care needs, 6 and worse survival outcomes, 4 even when diagnosed in earlier stages of disease. The disproportionate burden experienced by lung cancer patients extends to their informal caregivers, who themselves experience high psychological distress7,8 and poor physical health. 9 Patients and caregivers may share similar experiences and behaviors that contribute to these outcomes, including experiencing stigma related to lung cancer, 10 underutilizing supportive care services,7,11 and engaging in unhealthy lifestyle behaviors. For example, approximately 20% of patients and caregivers continue to smoke after a lung cancer diagnosis;12,13 24% of patients may engage in moderate to heavy drinking, 13 and 75% of patients do not meet physical activity guidelines. 13 Over 60% of lung cancer patients’ family members may have 2 or more behavioral risk factors. 14 Together, these findings suggest that lung cancer patients and their caregivers are a vulnerable population that could benefit from interventions to foster emotional well-being and healthful lifestyle behaviors.
Despite the need, very few interventions have been developed for this population. Most have been designed to address psychosocial concerns for advanced disease stages,15,16 symptom management,17,18 or targeted patients only. 19 To facilitate participation, health promotion interventions should be targeted to meet the needs and interests of patients and caregivers, but the lung cancer literature is limited in this regard, particularly for caregivers. One study has described interest in mental health and integrative medicine among distressed caregivers; 7 2 studies have described interest in lifestyle interventions among family members of lung cancer patients, though their caregiver status for the affected lung cancer patient was not specified.14,20 No studies have examined concordance between patient and caregiver interest in interventions, though evidence suggests moderate concordance with family member interest. 14 This is a significant gap in the literature given likely concordance between patient and caregiver behaviors 14 and poor mental and physical health in both populations. Factors associated with caregiver interest are similarly under described, with only 1 study describing correlates of interest among a sample of distressed caregivers. 7
This exploratory study extends the literature by describing interest in health promotion interventions among caregivers of lung cancer patients with a history of smoking, concordance between patient and caregiver interest in interventions, and factors associated with caregiver interest. Lung cancer patients with a smoking history were targeted in this study for several reasons. First, although the majority of lung cancer patients who smoke at the time of diagnosis do make a quit attempt, 21 some smoking patients are not interested in smoking cessation programs. Engaging these patients with other health promotion interventions (eg, stress reduction, diet, and exercise classes) may improve their health while enhancing receptivity to smoking cessation services. 22 Second, concordance between patient and caregiver smoking status has implications for both caregiver and patient health. Behavior change in either the patient or caregiver is likely to influence behavior change in the other. 23 Further, discordance between patient and caregiver smoking status is associated with higher caregiver distress.12,24 Third, patient self-blame for lung cancer due to a smoking history and caregivers’ blame of the patient are a source of distress for many families 25 and may influence help-seeking behavior 26 and caregiving behavior. 24 Perceived blame for cancer may motivate positive health behavior changes, 27 but if patients or caregivers continue to smoke, guilt or concerns about provider stigma may discourage them from using services until they quit. 28 The effect of perceived stigma and self-blame have not been examined as correlates of caregiver interest in health promotions interventions, but are clearly an important consideration for designing sensitive and palatable interventions.
The aims for this exploratory study were to (1) describe sociodemographic, and explore health behavior, and psychosocial characteristics, including depression, anxiety, perceived stigma, and self-blame for lung cancer among lung cancer patients and their family caregivers; (2) explore interest in health promotion interventions and examine concordance in interest among patients and caregivers; and (3) explore factors associated with caregivers’ interest in health promotion interventions.
Methods
Participants
Lung cancer patients presenting to a Southeastern Thoracic Oncology clinic within 6 months of their cancer diagnosis and their family caregivers were approached for participation in this study. If caregivers were not present when patients were approached, they were contacted by telephone to gauge their interest in study participation. Eligible patients were at least 18 years of age, diagnosed with lung cancer within the prior 6 months, smoked cigarettes 3 months prior to or after cancer diagnosis (as reported during screening), and were currently residing with a family member (ie, spouse, spouse-equivalent, or adult child). Patients were excluded if they were too ill to participate or had significant cognitive impairment (as judged by the referring physician), did not read or understand English, or did not have a caregiver who agreed to participate. Caregivers who were 18 years of age or older and a spouse, spouse-equivalent, or adult child of patient meeting study criteria were eligible. Caregivers who could not read or understand English were excluded. Written informed consent was obtained from each participant.
Procedure
This exploratory study used a cross-sectional design. Patient–caregiver combinations (dyads) completed a survey at the clinic or by mail to assess sociodemographic and caregiving characteristics, health behaviors, psychosocial functioning, and interest in health promotion interventions. Patient clinical data (American Joint Committee on Cancer [AJCC] stage and treatment type) were abstracted from the patients’ medical charts at participant enrollment. This study was approved by the local Institutional Review Board (00011626).
Measures
Sociodemographic and caregiving characteristics
Patients and caregivers reported their gender, age, race/ethnicity, education level, employment status, adequate financial resources (yes/no), marital status, relationship to patient, days per week of caregiving, and hours of daily care.
Health behaviors
Physical activity was assessed using an item from the CDC Behavioral Risk Factor Surveillance System (BRFSS) 29 : “During the past 30 days, other than your regular job, did you participate in any physical activities such as running, calisthenics, golf, gardening, or walking for exercise?.” Questions from BRFSS and the Minnesota Adult Tobacco Survey (MATS) 30 were used to assess history of smoking among patients and caregivers. Items from the Cancer Care Outcomes Research and Surveillance (CanCORS) caregivers study 31 were used to assess the number of days that the participant consumed an alcoholic beverage and the number of days engaged in binge drinking (5 or more drinks).
Psychosocial functioning
Stigma (I feel others think I am to blame for my lung cancer) and self-blame (I feel I am at least partially to blame for my lung cancer) were each assessed with 1 item developed for this study, based on a literature review to assess perceived lung cancer stigma and self-blame. Response options for stigma and self-blame items ranged from strongly disagree to strongly agree (range = 1–4). Caregivers completed an adapted version of this instrument to reflect perceptions about patient stigma (“I feel others think he/she is to blame for his/her lung cancer”) or blame (“I feel he/she is at least partially to blame for his/her lung cancer”). The 10-item short form of the Center for Epidemiological Studies Depression Scale (CESD-10)32 was used to assess depressive symptoms. CESD-10 scores range from 0 to 30, with a cutoff score of 10 or higher to indicate significant depressive symptoms. The 4-item Hopkins Symptom Checklist (HSCL) anxiety scale was used to assess current anxiety, 33 with scores ranging from 1 to 4.
Interest in health behavior interventions
Patients and caregivers answered questions to assess interest level in health promotion interventions (not interested, somewhat interested, very interested) including stress reduction, diet and exercise, yoga, educational classes about lung cancer and its treatment, and programs to help with smoking cessation or maintenance of smoking cessation for current or former smokers. As a follow-up to the smoking cessation question, participants also indicated their interest in participating by phone, mail, in person, or by computer/Internet. Participants also indicated whether they had daily access to a computer that is connected to the Internet at home.
Data Analysis
Descriptive statistics (means and standard deviations for continuous variables and frequencies for categorical variables) were used to summarize sociodemographic and clinical factors, caregiving characteristics, health behaviors, psychosocial functioning, interest in health promotion interventions, and delivery preferences for smoking cessation interventions. For interest in health promotion interventions, 95% exact binomial confidence intervals were constructed. Frequencies were also used to summarize the percentage of caregivers with clinically meaningful depressive symptoms on the CESD-10 (≥10).
We used McNemar’s tests to examine concordance in interest in health promotion interventions (stress reduction; diet and exercise; yoga; and educational classes about lung cancer and its treatment) for patients and caregivers. Fisher’s exact tests were used to examine the relationship between categorical characteristics (gender, education, relationship to patient) and the proportion of caregivers who reported being very/somewhat interested versus not interested in each type of health promotion intervention. Wilcoxon rank-sum tests were used to examine relationships between interest (very/somewhat interested versus not interested) in each intervention and continuous characteristics (age, time since patient’s cancer diagnosis, CESD-10, 4-item HSCL anxiety scale, stigma, and self-blame). Because only a subset of the caregiver sample had a smoking history, we excluded smoking cessation program interest from these analyses. All analyses were conducted in SAS (v.9.4, Cary, NC) with a 2-sided alpha level of .05 used to indicate statistical significance.
Results
Sample Characteristics
Out of 133 screened patients, 54 were eligible to participate (Figure 1). Of the eligible participants, 20 patients and 18 of their caregivers agreed to participate. We received surveys from 18 patients and 15 caregivers. Patients were 59 years of age (standard deviation [SD] = 10.0), on average, and predominantly non-Hispanic, white (88.9%), and male (55.6%) (Table 1). Although we had broad eligibility criteria in regard to disease stage, all patients who participated were considered stages I to III, with the majority (61.1%) of patients having AJCC stage III cancer. Family caregivers were younger than patients (mean = 47, SD = 11.6) and predominantly non-Hispanic, white (86.7%), and female (80%). Many caregivers (46.7%) were a spouse or partner to the patient and provided care ≥4 days/week (40%).

Patient and caregiver recruitment into study.
Sociodemographic, Clinical, and Caregiving Characteristics.
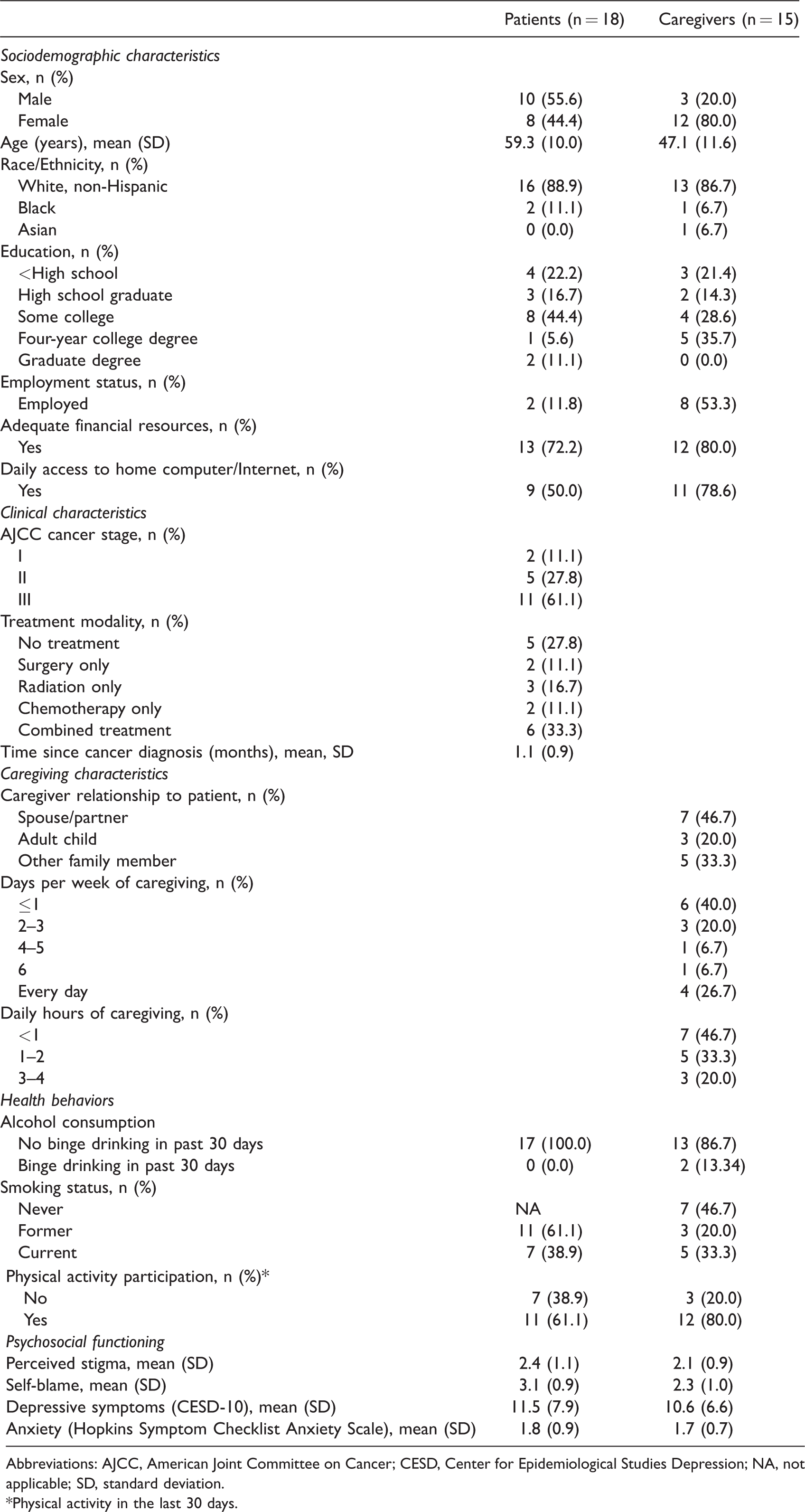
Abbreviations: AJCC, American Joint Committee on Cancer; CESD, Center for Epidemiological Studies Depression; NA, not applicable; SD, standard deviation.*Physical activity in the last 30 days.
Health Behaviors and Psychosocial Functioning
Among this sample of patients with a smoking history, many patients (38.9%) and caregivers (33.3%) reported current smoking (Table 1). All patients and the majority of caregivers (86.7%) reported no binge drinking in the prior 30 days. In addition, the majority of patients (61.1%) and caregivers (80%) reported participation in physical activity within the prior 30 days. Patients reported high self-blame for their cancer (mean = 3.1, SD = 0.9), whereas caregivers did not (mean = 2.3, SD = 1.0). The majority of patients (55.6%) and caregivers (60%) reported clinically significant depressive symptoms (≥10 on CESD-10). Patients and caregivers did not perceive high cancer-related stigma or report high anxiety.
Interest and Concordance in Health Promotion Interventions Among Patients and Caregivers
Patients and caregivers were concordant in their interest in cancer education (P = .16) and diet and exercise (P = .18) interventions; however, significantly more caregivers were interested in stress reduction (P = .05) and yoga (P = .03) interventions compared to patients. The majority of patients (83.3%, 95% confidence interval [CI]: 58.6%, 96.4%) and caregivers (86.7%, 95% CI: 59.5%, 98.3%) reported interest in at least 1 type of intervention (Figure 2). Participants reported the most interest in cancer education interventions (patients, 77.8%, 95% CI: 52.4%, 93.6%; caregivers, 86.7%, 95% CI: 59.5%, 98.3%), followed by diet and exercise (patients, 66.7%, 95% CI: 41.0%, 86.7%; caregivers, 80%, 95% CI: 51.9%, 95.7%), stress reduction (patients, 53.3%, 95% CI: 26.6%, 78.7%; caregivers, 73.3%, 95% CI: 44.9%, 92.2%), and yoga interventions (patients, 16.7%, 95% CI: 3.6%, 41.4%; caregivers, 50%, 95% CI: 21.1%, 78.9%). Among those with a smoking history, 50% of patients (95% CI: 26.0%, 74.0%) and 75% of caregivers (95% CI: 34.9%, 96.8%) were interested. Patients were mostly interested in participating in a smoking cessation intervention in person (77.8%), whereas caregivers preferred the Internet (66.7%) (Figure 3). Half of patients and less than a quarter (21.4%) of caregivers indicated that they did not have access to a computer connected to the Internet in their home.

Patient and caregiver interest in health promotion interventions. *Smoking cessation results include those with a smoking history (current or former smokers; patients, n = 18; caregivers, n = 8).

Patient and caregiver preferences for smoking cessation delivery among those with a smoking history. Results reflect preferences reported by participants with a smoking history (current or former smokers; patients, n = 18; caregivers, n = 8).
Factors Associated With Caregivers’ Interest in Health Promotion Interventions
Caregivers who reported interest in stress reduction interventions had higher levels of distress than those who were not interested (depressive symptoms, P = .03; anxiety, P = .02; Table 2). Caregiver sociodemographic characteristics (age, gender, education), relationship to patient, and other psychosocial characteristics (stigma and self-blame) were not associated with caregivers’ interest in health promotion interventions. Furthermore, no patient characteristics were associated with caregivers’ interest in health promotion interventions.
Associations Between Lung Cancer Caregivers’ Interest in Health Promotion Interventions and Demographic and Psychosocial Factors.
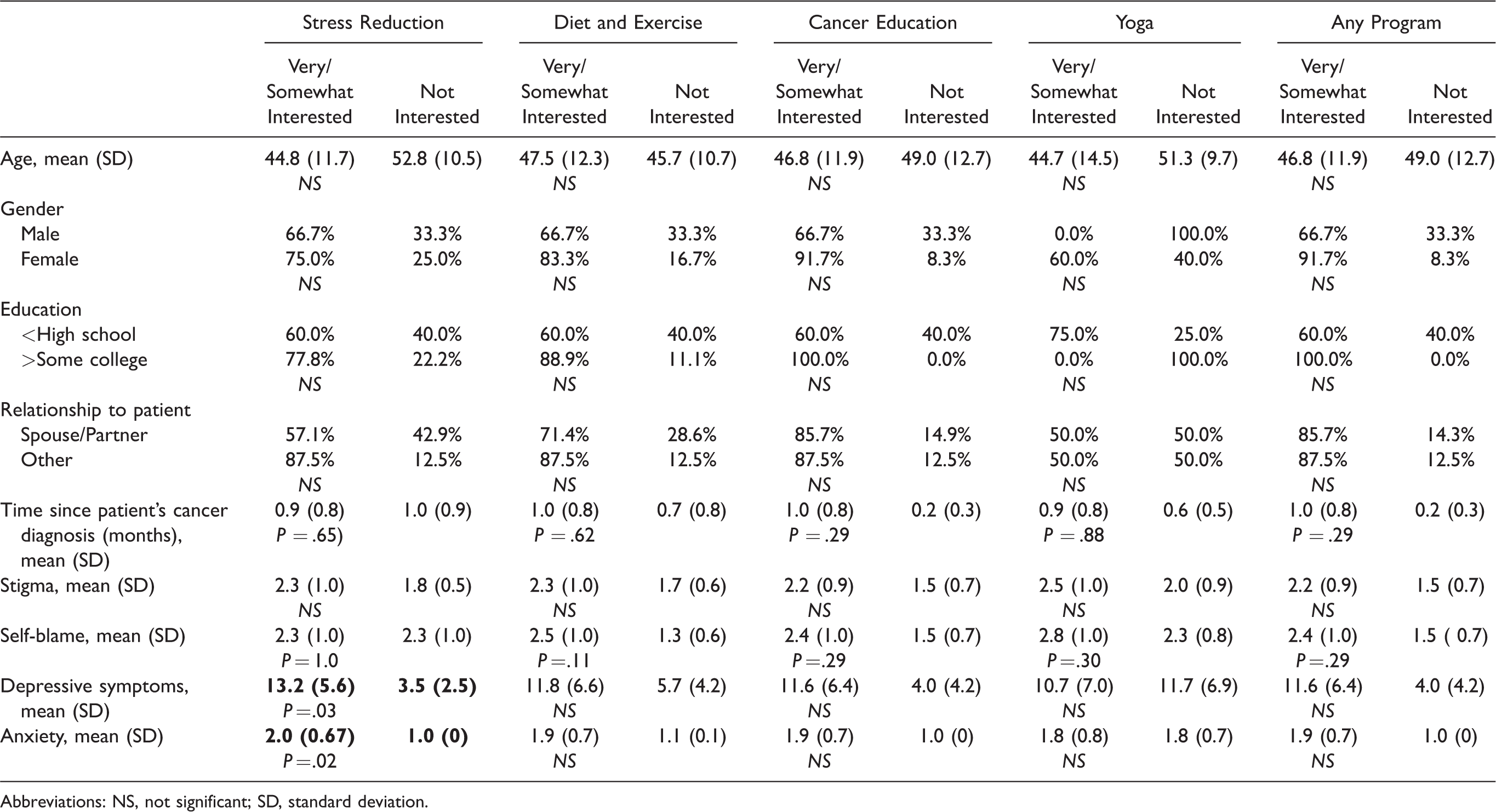
Abbreviations: NS, not significant; SD, standard deviation.
Discussion
In this exploratory study, we sought to describe sociodemographic, health behavior, and psychosocial characteristics in lung cancer patients with a history of smoking and their caregivers and to examine their interest, and concordance in interest, in health promotion interventions. To our knowledge, this study is the first to examine concordance in interest in interventions within lung cancer patient–caregiver dyads and both patient and caregiver factors associated with caregivers’ interest in interventions. The evaluation of factors associated with caregivers’ interest was important, as most studies have focused on factors associated with patient interest and not caregivers’. Overall, our results suggest that lung cancer patients and their caregivers have multiple risk factors for poor psychosocial functioning and physical health and a shared interest in cancer education and diet and exercise interventions. In addition, distressed caregivers were more interested in stress reduction interventions compared to caregivers who were not distressed.
In this study, patients and caregivers had a shared interest in cancer education and diet and exercise interventions, suggesting a dyadic approach may be beneficial in which patients and caregivers receive an intervention jointly. Dyadic interventions may be more efficient at improving patient and caregiver outcomes because patients and caregivers are targeted simultaneously, requiring less resources than interventions delivered separately to patients and caregivers. Furthermore, dyadic approaches may capitalize on the potential teachable moment of the patient’s cancer to motivate the caregiver to engage in a healthier lifestyle. Although dyadic approaches simultaneously deliver interventions, it is important to address unique concerns among patients and caregivers as individuals as well. For example, in this study, patients reported high self-blame for their cancer, whereas caregivers did not blame the patient. In some cases, an individual approach in which patients and caregivers are targeted separately may be needed. Our findings showed that significantly more caregivers were interested in stress reduction and yoga interventions and suggest that these types of interventions may be more suitable to be delivered individually. In addition, although patients and caregivers have a shared interest in cancer education and diet and exercise interventions, it is possible that dyad members may prefer to receive these types of interventions individually.
Overall, most patients and their caregivers were interested in interventions focused on cancer education, diet and exercise, and stress reduction. Half of caregivers were interested in yoga interventions but interest was less common among patients. A high proportion (ie, at least two-thirds) of patients and caregivers were interested in cancer education and diet and exercise interventions, which is consistent with broader literature suggesting that patients and caregivers desire information for how they can make positive changes to their health and improve their management of cancer.14,34 These interventions may be palatable approaches that can also serve as entry points for promoting other health behavior changes such as smoking cessation. 22
Smoking cessation interventions may also be appropriate for lung cancer patient–caregiver dyads. Although 75% of caregivers were interested in smoking cessation compared to 50% of patients, the prevalence of smoking among caregivers and concordance in smoking for cancer dyads 12 suggests the need for smoking cessation services for both patients and caregivers. Smoking cessation interventions often target individuals, but cessation may be more easily achieved when targeting both members of the dyad jointly. 35 When discussing smoking cessation, providers should be sensitive to patient and caregiver attributions of behavioral blame for cancer and lung cancer stigma, as they may be a deterrent to talking about smoking cessation. 28 Low levels of stigma reported in our sample may have been the result of our limited assessment of stigma in comparison to full stigma measures (eg, Cataldo et al. 36 ).
Given the high levels of depressive symptoms in our sample, it is encouraging that over half of patients and nearly three-quarters of caregivers were interested in stress reduction interventions. Patients were less receptive to yoga, though half of caregivers were interested. Our findings may reflect a gender difference, as the majority of the caregivers were female and patients male. These interventions have not been widely tested among lung cancer patient–caregiver dyads, though interventions incorporating aspects of stress reduction such as coping skills training have demonstrated feasibility among lung cancer caregivers.18,37 In terms of dyadic interventions, a mindfulness-based stress reduction intervention has demonstrated feasibility among lung cancer patient–caregiver dyads in the advanced disease setting, 38 as has a yoga intervention. 16 Other dyadic stress reduction interventions are being tested. 39 It is possible that in our sample, participants may have been more receptive to interventions described as “mind–body/relaxation” approaches rather than “yoga” interventions, though these are often the same or similar approaches.
Key challenges in designing and delivering interventions for lung cancer patients and their caregivers include identifying those in need of services and then ensuring that interventions offered are low burden to accommodate caregivers’ busy schedules but sufficiently dosed to have an effect. 40 Screening for caregiver distress is a logical next step to mirror patient distress screening initiatives and a recent pilot study suggests cancer caregiver distress screening is feasible in an ambulatory surgical center. 41 In our study, caregivers who reported interest in stress reduction interventions had higher levels of distress compared to caregivers who were not interested. This result echoes that from a sample of head and neck cancer caregivers, an underserved population with similar risk factors for poor psychosocial and health outcomes. 42 An additional challenge includes developing low-cost and easily accessible interventions to extend reach to caregivers with other vulnerable characteristics such as low income, poor health literacy, or residing rurally. A potential avenue for supporting lung cancer patients and caregivers is a multicomponent health promotion intervention offering cancer education, diet and exercise, and stress reduction components, with potential for dyadic participation. Such an intervention could be delivered through the use of educational web-based materials in a supported self-management format, in which participants are provided with self-directed educational materials to learn information and strategies to promote healthy behaviors and manage emotions.43,44 This approach would allow participants to access the website at their preferred time and location, potentially reducing participation burden. Furthermore, this type of intervention has the potential to be low cost for patients and caregivers and accessible to those residing rurally.
Limitations/Strengths
Limitations of this exploratory study included a small sample of lung cancer patients with a smoking history and their family caregivers who were recruited from one clinic. The majority of participants were non-Hispanic, white, had at least some college education, and reported adequate financial resources. Furthermore, caregivers in this study reported less time spent caregiving in a week compared to national statistics for cancer caregivers. 45 As such, these findings are not generalizable to all lung cancer patient–caregiver dyads and should be further examined in a larger, more diverse sample. In addition, we did not collect data on characteristics of those who declined to participate and therefore cannot assure that they are demographically or clinically similar to participants who consented. Given the paucity of information pertaining to lung cancer caregivers’ interest in health promotion interventions, we focused our analyses primarily on the caregiver and did not examine characteristics associated with patient interest. Although this study provides new information that can help guide development of health promotion interventions for lung cancer patients and caregivers, we did not collect data on intervention delivery preferences such as timing of delivery (eg, at diagnosis, during treatment), and preferences for a dyadic versus individually delivered approach. In addition, we only assessed preferences for mode of delivery (eg, in person, Internet-based) for smoking cessation interventions. Furthermore, this study was conducted prior to availability of well-validated lung cancer stigma assessments (eg, Cataldo et al. 36 and Ostroff et al. 46 ), and our assessment may have underestimated the experience of stigma in this population. In addition, although patients in this study reported high self-blame, it is possible that asking participants about self-blame incited self-blame or potentiated self-blame. Despite these limitations, this study provides key information to guide intervention development for lung cancer patients and caregivers.
Implications
Our findings suggest that health promotion interventions focused on stress reduction, diet and exercise, and cancer education should be offered to lung cancer patients and caregivers. In addition, yoga and smoking cessation interventions are also of interest to some lung cancer patients and caregivers. Further research should confirm these findings in a larger and more diverse sample and explore other potential correlates of caregiver interest (eg, additional sociodemographic, disease, treatment, and environmental factors), patient and caregiver delivery preferences for these intervention types, and preferences for and advantages of using individual or dyadic approaches. In addition, future research should explore how health promotion interventions for cancer caregivers or dyads may vary, depending upon cancer type.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Comprehensive Cancer Center of Wake Forest University (CCCWFU), with support from the Biostatistics Core of the CCCWFU (P30 CA012197). Chandylen Nightingale’s work on this manuscript was in part supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant KL2TR001421. Laurie Steffen’s work on this manuscript was supported by a Cancer Control Traineeship, National Cancer Institute/National Institute of Health (NCI R25CA122061).