
Abstract
Objective
To assess whether the Berlin Sleep Questionnaire and the Snoring, Tired, Observed, Pressure, Body mass, Age, Neck, and Gender questionnaire (STOP-BANG) might be suitable replacements for an overnight sleep pulse oximetry as screening tools for sleep disordered breathing in patients with fibromyalgia.
Introduction
Fibromyalgia (FM) is a chronic, centralized, pain sensitivity syndrome, characterized by diffuse musculoskeletal pain, accompanied by symptoms, such as insomnia, waking tired or unrefreshed, cognitive difficulties, fatigue, depression, and anxiety.1,2 It is estimated that 2% to 8% of people in the United States suffer from FM. For those diagnosed, 90% have sleep complaints,3,4 which include excessive daytime sleepiness, easily disturbed sleep, daytime tiredness, and fatigue. 5 Given the frequency in which these sleep-related symptoms are reported, the American College of Rheumatology has included “sleep complaints and waking tired or unrefreshed” as components of the composite Symptom Severity scale for the 2010 diagnostic criteria for FM. 6 The most common sleep-related breathing disorder is obstructive sleep apnea (OSA). In a previous study, the prevalence of OSA in the FM population was reported as 50%. 7 Moreover, many symptoms of FM overlap with OSA including waking unrefreshed, fatigue, tiredness, and insomnia.
Due to the noteworthy overlap between symptoms of FM and OSA, it is hypothesized that these conditions share similar risk factors. Previous studies observed a direct association between pain and poor sleeping, which included sleep duration, disturbance, and efficiency.8–10 It has also been noted that 88% of patients with chronic pain also suffer from insomnia. 11 The relationship between FM and poor sleep quality can directly affect activity levels, which in turn can increase the risk for obesity, leading to the possible formation of additional pain generators.
In addition to pain, weight gain is a risk factor for OSA. According to the National Sleep Foundation, 18 million Americans have OSA; the majority of which has concomitant obesity. 12 This association leads to the hypothesis that as an individual gains weight in their trunk and neck, their respiratory function becomes compromised. As the cycle continues, poor sleeping habits lead to daytime fatigue and less energy, which can affect the ability to exercise, engage in a healthy diet, and sustain a healthy lifestyle. One study evaluating obesity in FM patients observed that 50% of the study group was obese (body mass index [BMI] ≥ 30 kg/m2) and an additional 21% were overweight (BMI = 25–29.9 kg/m2). 13 Interestingly, BMI has also been observed to correlate directly with a heightened sensitivity of tender points in FM patients.13,14 Overall, the relationship between FM and sleep-related symptoms is important because sleep disturbances have been observed to be precursors and contributors to the severity of various FM-related symptoms.
Due to the prevalence of sleep disorders in the FM population, overnight sleep pulse oximetry is routinely ordered. This practice of ordering sleep pulse oximetry is present in many clinical settings, including our Fibromyalgia and Chronic Fatigue Clinic at Mayo Clinic (Rochester, Minnesota). Based on the data collected by the oximeter, a desaturation index (the number of independent desaturations from the baseline per hour of recording) is calculated, from which the potential presence and severity of OSA can be estimated. 15 The presence of oxygen desaturations during sleep could be an indication of an underlying sleep-disordered breathing, which can be further investigated via polysomnography or home sleep apnea testing. 16 A polysomnogram involves sleeping overnight in a sleep clinic, while a technologist continuously monitors heart rate, breathing patterns, blood oxygen level, and other measures to diagnose a variety of sleep disorders. 17 Home sleep apnea testing allows patients to bring similar diagnostic equipment home and wear the necessary sensors overnight. 18 These additional tests are costly and can provide a financial burden to many patients. Therefore, a practical, cost-efficient, screening tool for sleep apnea could be beneficial, especially in efforts to individualize additional testing. The Berlin Sleep Questionnaire (BSQ) and the Snoring, Tired, Observed, Pressure, Body, Age, Neck, and Gender questionnaire (STOP-BANG) are 2 validated and concise surveys, which are widely used in research and sleep medicine; these could potentially be used for screening of the likelihood of OSA and the potential need for a sleep pulse oximetry test. 19
Given the significant cost associated with nonselective testing in every FM patient, we sought to improve upon individualizing the diagnostic approach for sleep-related breathing disorders in patients with FM at Mayo Clinic. Thus, this study evaluated whether the STOP-BANG and the BSQ could be a discriminatory tool for OSA, aiding us in individualizing the need for overnight pulse oximetry testing in patients with FM.
Methods
Participant Population and Selection
Participants included patients who actively attended Mayo Clinic’s Fibromyalgia Treatment Program from June 8, 2018 through July 25, 2018. The Mayo Clinic Institutional Review Board approved the study (#17-011117). The target population was 50 patients, who received a formal diagnosis of FM using the 1990 and/or 2010 American College of Rheumatology Fibromyalgia Classification Criteria. The 1990 American College of Rheumatology classification criteria includes chronic widespread pain (defined as pain above and below the waist, involving the right and left side of the body) and the presence of at least 11 out of 18 specified tender points, upon palpation. However, the updated 2010 criterion is defined as chronic widespread pain associated with somatic symptoms, which are rated on the Widespread Pain Index scale and the Symptom Severity scale. The participants also had to have completed an overnight pulse oximetry test. Participants orally consented, signed a Health Insurance Portability and Accountability Act waiver, completed the BSQ and STOP-BANG questionnaires, and had their height, weight, and neck circumference measured. Neck circumference was taken as this is a known risk factor for OSA; it is documented that excess weight around the neck can cause narrowing of the airway when lying down.
Study Design
This study was designed as a prospective comparative study with a retrospective chart review component, for pulse oximetry test results. The participants’ age, sex, blood pressure, overnight pulse oximetry test results, and OSA diagnosis status were abstracted from their medical records. Participants were asked to complete the 2 surveys related to the risk of having OSA: the BSQ and STOP-BANG. The BSQ consists of 10 questions that are divided into 3 groupings: snoring, day time fatigue, and BMI/hypertension. If 2 or more groupings are positive, he/she is considered to be at high risk for sleep apnea, otherwise he/she is considered to be at low risk for sleep apnea.17–19 The STOP-BANG questionnaire consists of 8 questions that divide participants into 3 categories: high risk, intermediate risk, and low risk for sleep apnea. The STOP-BANG also includes questions regarding BMI, age, neck circumference, and sex. A score of 0 to 2 indicates low risk, a score of 3 to 4 indicates intermediate risk, and a score of 5 to 8 indicates high risk. After both surveys were completed, height, weight, and neck circumference measurements were taken and recorded. This information was used to calculate BMI and to verify responses provided on the STOP-BANG questionnaire.
Data Collection
Participants were each assigned a unique study identification and their status was tracked in a research participant tracking software, PTrax (Darlogix, Inc., Williamsville, New York). Study participants’ survey responses, overnight oximetry test results, and OSA diagnosis status were collected and stored using the Research Electronic Data Capture (REDCap) software hosted by Mayo Clinic Center for Clinical and Translational Science. 20
Data recorded from the overnight pulse oximetry included date, start time, duration, pulse data, and total event data (total events, average event duration, oxygen desaturation index, percent artifact, adjusted index). Peripheral capillary oxygen saturation percent (SpO2) data (basal SpO2, time <89%, events < 89%, maximum single time < 89%, minimum SpO2 and time, maximum SpO2 and time, average low SpO2, average low SpO2 < 89%) as well as an interpretation and impression from the physician were also recorded.
Statistical Analysis
Continuous variables are described using mean ± standard deviation and categorical variables are described using frequency and percentage. Sleep apnea categories and oximetry results were analyzed for association using Fisher’s exact test with significance set at (P ≤ .05).
Results
This study had a total of 50 participants, consisting of 46 (92%) women and 4 (8%) men. The average age of this population was 42.5 ± 14.46 (range, 19–71) years, with a mean BMI was 31.1 kg/m2. In addition, the average neck circumference was 37.48 ± 3.92 cm. At presentation, 6 (12%) participants had been diagnosed with OSA and 13 (26%) had hypertension.
BSQ and STOP-BANG Results
The BSQ results demonstrated that out of the 14 participants who were categorized as high risk, 12 (85.7%) had an abnormal oximetry test result. In contrast, out of the 36 participants who were categorized as low risk, 30 (83.3%) had normal oximetry results (Table 2).
The STOP-BANG survey responses are divided into 3 categories: high, intermediate, and low risk (Table 1). Out of the 50 participants, 7 (14%; 5 women and 2 men) were categorized as high risk, with 6 (85.7%) having an abnormal pulse oximetry test result. The results for the STOP-BANG also indicated that 30 participants were categorized as low risk and 26 (86.6%) had a normal pulse oximetry test result.
Characteristics of Fibromyalgia Patients and Risk Levels for OSA as Indicated by the BSQ and STOP-BANG.
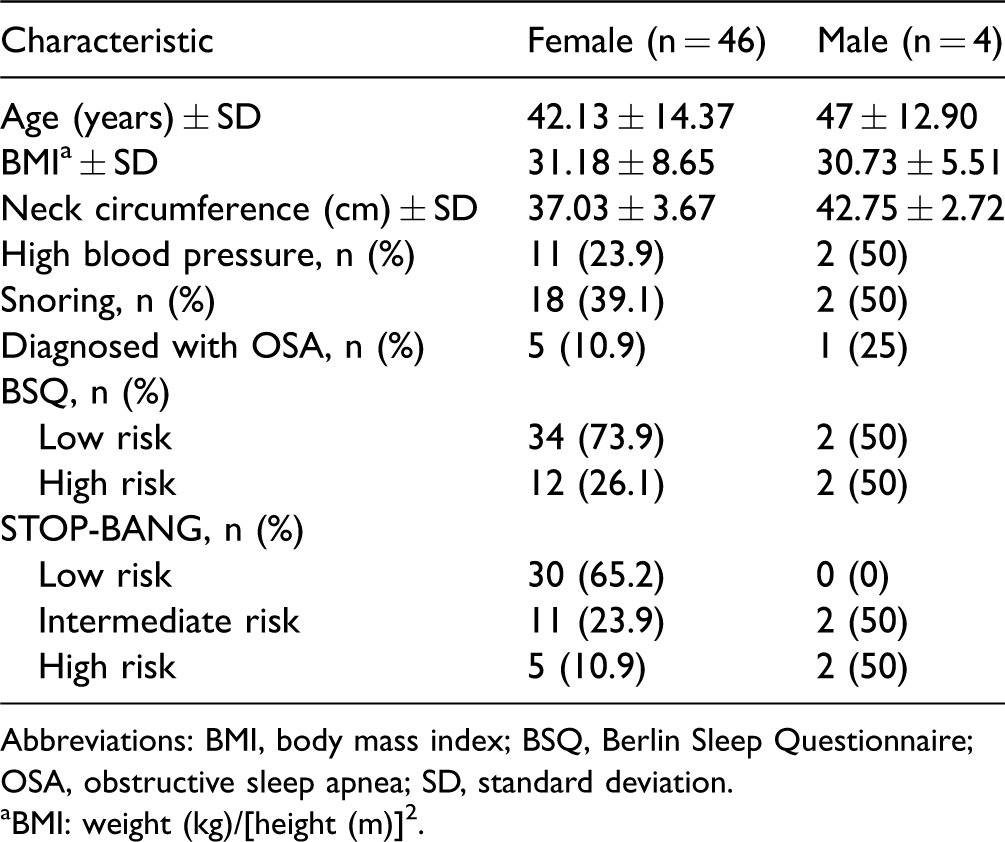
Abbreviations: BMI, body mass index; BSQ, Berlin Sleep Questionnaire; OSA, obstructive sleep apnea; SD, standard deviation.
aBMI: weight (kg)/[height (m)]2.
Fisher’s Exact Test for STOP-BANG and Berlin Sleep Questionnaire.

Assisted breathing devices used by participants in this study included continuous positive airway pressure and bilevel positive airway pressure devices. Percentages are calculated from the total of participants who scored in each category.
aAs determined by a physician at Mayo Clinic.
bIncludes assisted breathing device users who have been diagnosed with obstructive sleep apnea. Assisted breathing devices used by participants in this study, included continuous positive airway pressure and bilevel positive airway pressure devices.
Pulse Oximetry Results
The overnight pulse oximetry data were abnormal for 18 (36%) of the 50 participants. Five out of the 18 with abnormal readings had normal impressions due to the use of continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BiPAP) devices during testing. CPAP and BiPAP machines are used to treat OSA, so it is assumed that these participants would have had an abnormal oximetry result without the use of these assisted breathing devices. 21 Upon medical record review, all 5 of these participants had a formal diagnosis of OSA and therefore have been analyzed as having abnormal oximetry test results in Tables 2 and 3.
Pulse Oximetry Test Results as They Correlate to Scores of BSQ and STOP-BANG.

Abbreviations: BSQ, Berlin Sleep Questionnaire; OSA, obstructive sleep apnea; STOP-BANG, Snoring, Tired, Observed, Pressure, Body mass, Age, Neck, and Gender questionnaire.
aNone of the participants in this study scored both low on the BSQ and high on the STOP-BANG.
bAs determined by a physician at Mayo Clinic.
cScore of high on both BSQ and STOP-BANG.
dIncludes assisted breathing device users that have been diagnosed with obstructive sleep apnea. Assisted breathing devices used by patients in this study included continuous positive airway pressure and bilevel positive airway pressure devices.
eScore of high on BSQ and intermediate on STOP-BANG.
fScore of low on BSQ and intermediate on STOP-BANG.
gScore of low on both BSQ and STOP-BANG.
hScore of high on BSQ and low on STOP-BANG.
Of the 13 participants (26%; all women) who were prescribed narcotics or benzodiazepines, 9 had normal pulse oximetry test results. Out of the 4 who had abnormal pulse oximetry results, 2 were categorized as intermediate risk and 2 as high risk on the STOP-BANG, and all 4 were categorized as high risk on the BSQ. Of the 24 participants (48%) with a BMI greater than 30 kg/m2, 12 (50%) had abnormal pulse oximetry results. In addition, 9 participants (8%) had neck circumferences greater than 40 cm, and 6 (66.7%) of these individuals had abnormal pulse oximetry results. Of the 7 participants (14%) who had both a BMI greater than 30 kg/m2 and a neck circumference greater than 40 cm, 6 (85.7%) had an abnormal pulse oximetry test result.
Association of Sleep Apnea Surveys and Oximetry Results
Fisher’s exact test was utilized to assess for any significant association between the sleep apnea surveys (BSQ and STOP-BANG) and the overnight pulse oximetry results. Fisher’s exact test for STOP-BANG and BSQ were both highly significantly (P < .001) associated with the sleep pulse oximetry results, indicating that participants at high risk for sleep apnea, based on the sleep apnea surveys, have a greater prevalence of abnormal oximetry results than those at low risk for sleep apnea. Out of the 14 participants who were categorized as high risk on the BSQ, 12 (85.7%) were significantly associated (P < .001) with an abnormal oximetry result or assisted breathing device (Table 2). In addition, the 6 participants who were categorized as high risk and the 8 who were categorized as an intermediate risk on the STOP-BANG were significantly (P < .001) associated with abnormal oximetry results.
The participants who were categorized as high risk (14) on the BSQ, half of them (7) also were categorized as high risk on STOP-BANG. Six (85.7%) of a total of 7 participants who were categorized as high risk on both the BSQ and STOP-BANG had either an abnormal pulse oximetry test result or were already utilizing an assisted breathing device (Table 3). In contrast, of the 28 participants who were categorized as low risk on both surveys, only 3 (10.7%) had an abnormal oximetry result. Of the 8 participants who were categorized as low risk on the BSQ and intermediate risk on the STOP-BANG, 3 (37.5%) had an abnormal oximetry test result.
Discussion
Main Findings
This study evaluated the effectiveness and utility of the BSQ and STOP-BANG as discriminators of probable OSA in patients with FM, as compared to traditional overnight pulse oximetry. This was done in an effort to improve individualized diagnostic testing in the FM population, where the vast majority of patients have sleep complaints, while also trying to minimize the patient’s burden. The current solution to the high prevalence of sleep complaints in FM patients at Mayo Clinic and other institutions includes obtaining an overnight pulse oximetry testing for all patients seen for FM. However, in the literature, the test results have never been evaluated and analyzed to determine if the test was indicated based on the patient’s risk level for OSA or as a prerequisite screening tool. Based on the current results, this study suggests that participants at high or intermediate risk for sleep apnea, according to the BSQ and STOP-BANG, have a greater prevalence of abnormal oximetry results than those at low risk for sleep apnea. This group of FM patients would most likely benefit from an overnight pulse oximetry.
The BSQ predicted abnormal oximetry results in 85.7% of high-risk participants and normal oximetry results in 83.3% of low-risk participants. The STOP-BANG survey predicted abnormal oximetry in 85.7% of high-risk participants and normal oximetry in 86.7% of low-risk participants. When both surveys were utilized together to predict risk for OSA, the results were slightly more correlated (92.8%) with the results of the pulse oximetry test. As expected, those who were deemed as low risk on both surveys had the highest probability (89.3%) of having a normal oximetry result.
The one participant who scored high on both surveys, yet had a normal oximetry, has been encouraged by their rheumatologist to follow up with a sleep medicine clinic for further testing and possible treatment of what is believed to be undiagnosed OSA. This result indicates an instance where the participant’s risk level for OSA, as determined by the BSQ and STOP-BANG survey, may have been of more help diagnostically than their oximetry test result. In addition, the strong association between high BMI, large neck circumference, and abnormal pulse oximetry testing observed in this study, further suggests the discriminatory accuracy of these measures for patients at risk for OSA. Utilizing these validated questionnaires could considerably reduce the need for mandatory and non-individualized overnight pulse oximetry testing for FM patients and thus, substantially reduces health care–associated costs. The BSQ and STOP-BANG surveys together contain 18 straightforward questions, many of which are repeated between the 2 surveys, including snoring, tiredness, and high blood pressure. Measuring BMI is already part of the intake procedure, and measuring the neck circumference is easy and noninvasive. Together, the proposed additions to the intake procedure for FM patients are far less time-consuming, burdensome, and financially impacting than an overnight pulse oximetry test.
Implications
The outcomes of this study indicate the potential for further individualization of care for FM patients. The results suggest that the BSQ and STOP-BANG survey can be used as an effective prescreening tool, on a case-by-case basis, for patients with sleep-related symptoms, rather than having prerequisite overnight pulse oximetry testing performed for all FM patients. If an individual scored high on both surveys, the physician would then assume the overnight pulse oximetry results would be abnormal and could move directly to the next step in diagnosing OSA, polysomnography. The data suggest that individuals who scored low on both surveys would not need to complete an overnight pulse oximetry test unless otherwise indicated. Individuals who score high on the BSQ and either low or intermediate on the STOP-BANG, or low on the BSQ and either high or intermediate on the STOP-BANG, should still complete an overnight pulse oximetry test because the discriminatory accuracy of these score combinations was inconclusive in this study.
Individualized diagnostic testing decreases unnecessary health-care spending. One study, evaluating over testing in the United States, observed that 24.9% of diagnostic testing are unnecessary. 22 Over utilized diagnostic testing is widely considered to be an important contributing factor to the exorbitant health-care spending in the United States. Currently, every patient seen for FM at Mayo Clinic is required to complete an overnight pulse oximetry test. At approximately $180 per test, an estimated $450 000 per year is spent on pulse oximetry testing in this clinic alone. If the individual’s insurance does not cover the full price of the test, it potentially becomes an unnecessary out-of-pocket cost. Use of the BSQ and STOP-BANG survey to determine when/if pulse oximetry testing is indicated is an intervention that can both improve treatment outcomes and reduce health-care costs.
Limitations
The design of this study was essentially a retrospective chart review; a rigorous prospective study would have helped further our conclusions. Our study consisted of 50 total participants and this small sample size could have affected our results, due to random variation alone. Of the 50 FM participants included in this study, 12% had been diagnosed with OSA at the time of data collection. This finding indicates a decreased prevalence of OSA among FM patients treated at Mayo Clinic for FM in comparison with populations observed in previous studies. A study conducted in 2017 observed the presence of OSA in 50% of a sample size of 24 patients with FM. 7 The discrepancy in OSA rate among FM participants in this study may differ from what others have previously observed because many participants who had abnormal pulse oximetry testing had not yet completed a polysomnogram to get a formal diagnosis of OSA. Future research should investigate this limitation further with a more robust sample size.
Another limitation of our study is due to the possible confounding effects of factors, such as fatigue and unrefreshed sleep, which is very common in both the FM and sleep disorder patient populations. Both the BSQ and STOP-BANG included questions related to fatigue, which may not necessarily be indicative of higher risk for sleep apnea in the FM patient population, where fatigue and unrefreshing sleep are central components of the condition itself and the diagnostic criteria. 6 The BSQ includes one question related to nonrestorative sleep and another related to daytime fatigue. Both questions are included in the same category, in which 47 participants (94%) scored positively. The STOP-BANG survey includes 1 question on daytime fatigue that counts toward their overall risk for OSA. All 50 participants answered positively to this question. Due to the design of the BSQ and STOP-BANG questionnaires and the possible confounding effects of fatigue, it is relatively easy for patients with FM to have a high risk for OSA based on daytime fatigue alone, which may potentially contribute to an overestimation of risk and thus a lower predictive accuracy and validity in this patient population.
Conclusion
Our results indicate that the BSQ and STOP-BANG can be utilized to determine the need for overnight pulse oximetry testing in FM patients. This intervention is important because effective treatment of sleep-related symptoms can improve overall quality of life for FM patients and potentially decrease the severity of various symptoms. Utilization of the BSQ and STOP-BANG surveys in this population would not only save the individual the inconvenience of unnecessary testing but would also expedite the diagnostic process, leading to a faster diagnosis and treatment of OSA, which in turn could improve the overall patient experience.
Footnotes
Acknowledgments
The authors thank their colleagues in the Fibromyalgia and Chronic Fatigue Clinic at Mayo Clinic for allowing them to conduct this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.