
Abstract
Background
Chronic stress plays a role in the development of health disparities. However, the relationship between neighborhood stressors and stress-related health problems and behaviors is unknown. In the city of Boston, Massachusetts, 3 neighborhoods, while within a 3 mile radius, have widely divergent life expectancies. This work aims to investigate and compare perceived neighborhood-level stressors, stress-related negative behaviors, and stress-related health problems in these neighborhoods.
Methods
Three hundred twenty-six participants were surveyed from the neighborhoods. Participants were asked to rate (1) 27 neighborhood stressors, (2) 16 stress-related negative behaviors, and (3) 13 stress-related health problems using a 1 to 5 Likert-type scale. Differences in responses between neighborhoods were analyzed using Kruskal–Wallis and χ2 tests.
Results
The highest neighborhood stressors overall were related to finance, unequal treatment, and unsafe bike/pedestrian access. The highest stress-related health problems were related to substance abuse and obesity, and the largest stress-related behaviors were related to poor diet, intolerance, and aggressive driving. There were significant differences across neighborhoods (P < .05) for 18 of the 27 neighborhood stressors, 8 of the 10 stress-related health problems, and 12 of the 15 stress-related behaviors.
Conclusions
There is marked contrast in stress landscapes between the 3 neighborhoods in Boston despite their geographical proximity. This finding potentially serves as an explanation for the drastic differences in health outcomes, even though these neighborhoods are equidistant from academic medical centers. Strategies for improving the health of individuals should incorporate the unique stressors at the neighborhood level. Further research is needed to investigate how specifically neighborhood stressors influence the health of residents, thereby informing what policy interventions might be useful.
Keywords
Introduction
Stress plays an important role in an individual person’s biology as well as health outcomes. Studies have shown that stressed individuals engage in less healthy behaviors such as exercising less, eating more, smoking more, and sleeping poorly. 1 In addition, chronic stress is associated with persistent low-level inflammation, suboptimal cardiovascular health, impairments in memory and learning, and higher rates of numerous morbidities, including obesity.2–4 It is estimated that stress-related ailments cost the US$300 billion annually in medical bills and lost productivity. 5 According to the American Psychological Association, the average reported stress level of Americans has increased overall, with greater percentages of adults reporting “extreme stress” compared to previous years. 6
In recent years, research into stress landscapes has expanded beyond individual sources of stress to the structural and social determinants of neighborhoods. While many associations between individual stressors and health outcomes are known, 7 the effects of neighborhood-level stressors have on health outcomes are less clear. Recent studies have shed light on how neighborhood-specific factors (eg, access to sidewalks, perceived walkability, density of stores selling affordable healthy foods, recreational facilities) are associated with better cardiovascular health. 8 In addition, 1 important dimension of neighborhood effect is social connectedness. One meta-analysis demonstrated that the quality and quantity of one’s social relationships have been linked to mental health and numerous other morbidities.9,10
Neighborhood effects are particularly interesting in the city of Boston, Massachusetts. Despite its density of academic health centers, social services, and expanded access to care for low-income residents, 11 Boston has striking geographic health disparities. 12 Even with all of Boston’s vast health-care resources, there remains a persistence of geographically based disparities, demonstrating barriers that are embedded within the social and physical environments of the neighborhoods. Situated within a 3 mile radius, the Boston neighborhoods of Roxbury, Jamaica Plain, and Back Bay (Figure 1) vary by average annual income, percentage of residents with high school diplomas, and eligible voter registration. 12 While these 3 neighborhoods are equidistant to primary, secondary, tertiary, and quaternary care, the neighborhoods have unexpectedly large differences in life expectancy (59, 78, and 89 for Roxbury, Jamaica Plain, and Back Bay, respectively). 12
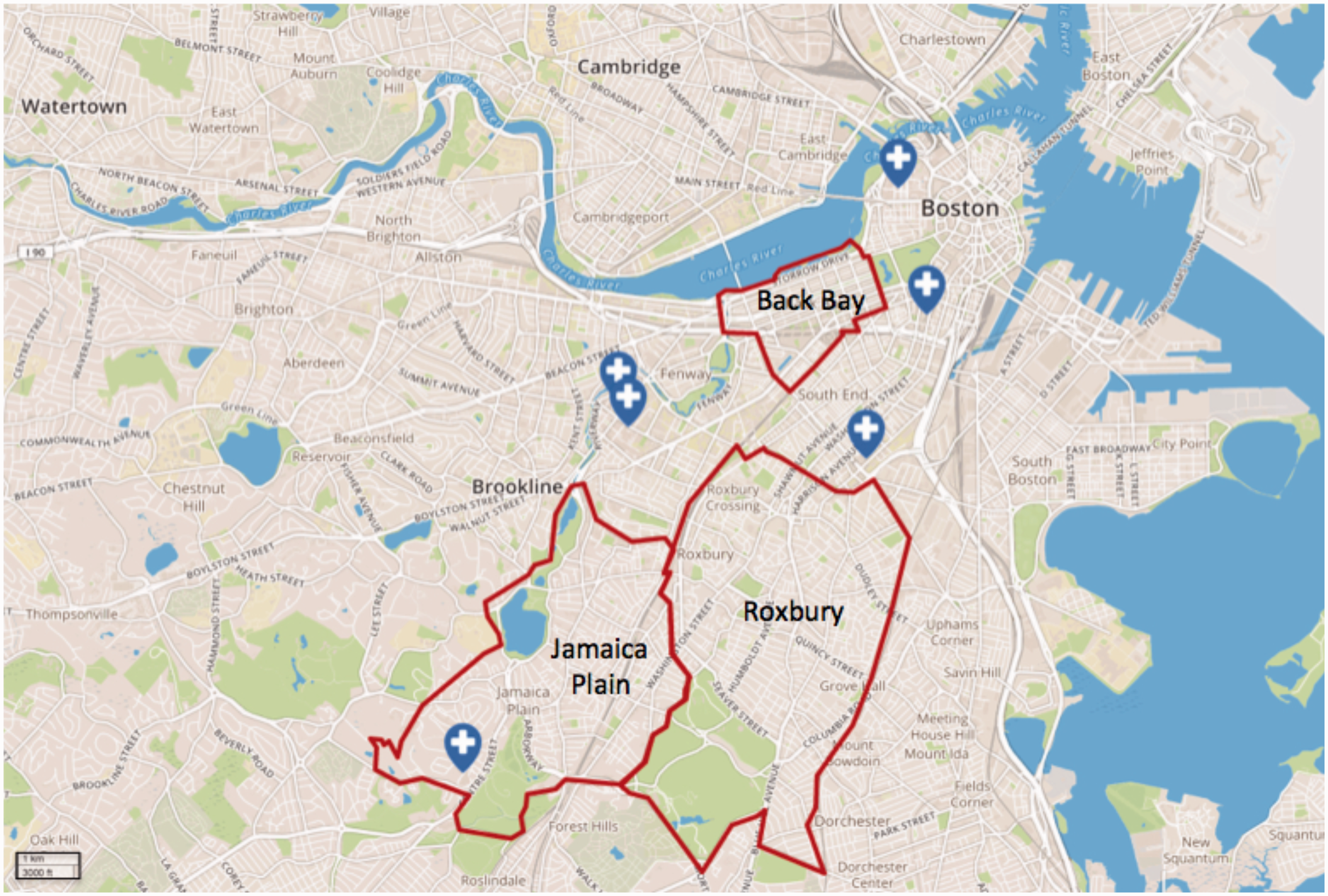
Map of Boston With Neighborhoods of Roxbury, Jamaica Plain, and Back Bay. Major tertiary care hospitals depicted with label.
To our knowledge, there have been no studies that have examined the relationship between neighborhood characteristics and residents’ health in Boston. Our study investigates 2 main research questions. First, what neighborhood-level characteristics are perceived as stressors by residents of these neighborhoods? And second, what stress-related negative behaviors and stress-related health problems do each neighborhoods’ residents report?
Data and Methods
Neighborhood Selection and Focus Groups
This study involved focus groups and survey administration in the Boston neighborhoods of Roxbury, Jamaica Plain, and Back Bay. The study protocol was approved by the institutional review board at Harvard Medical School, and participants gave informed consent. From November to December 2016, 15 focus groups of adults over the age of 18 years were conducted with residents of these neighborhoods. Five focus groups were conducted in each neighborhood, consisting of 5 to 8 participants. Informed consent was obtained from all participants, and a disclosure of complete anonymity was given prior to initiating any study procedures. To ensure consistent facilitation, a single moderator was used and focus group sessions followed a standard outline of (1) introduction of the study and explanation of “neighborhood-level stressors” (2) identification of neighborhood characteristics that were personally stressful, and (3) specification of positive and negative characteristics within the participant’s neighborhood. After creating a list of neighborhood stressors, participants were asked to identify unifying themes among individual neighborhood characteristics. In addition, participants were asked about stress-related health problems and stress-related behaviors that occur in their neighborhood. Discussions typically lasted approximately 1 hour.
Survey Development
Insights from the focus groups were used in combination with local epidemiologic health data to develop a survey with the goal of assessing the magnitude of (1) perceived neighborhood-level stressors, (2) self-reported stress-related health, and (3) perceived stress-related negative behaviors. To assess perceived neighborhood-level stressors, 20 of the 27 stressors were derived from participant responses from focus groups. The additional 7 stressors were taken from previously described community sources of stress.13,14 Survey participants were asked what they perceived to be the largest “problems” which cause the most stress to people in your neighborhood. They were asked how much they agree/disagree with how much of a stress source each of the 27 neighborhood characteristics were in their neighborhood; ranking was between 1 and 5, with 1 = not a stress source and 5 = very strong stress source. To assess self-reported stress-related health problems, survey participants were presented with a list of stress-related health problems that are associated with chronic and neighborhood stress.15–17 Survey participants were instructed to identify the stress-related health problems that they currently have and then rate how large of a problem it is to them (1= minimal problem, 2= moderate problem, 3= large problem). Lastly, to assess stress-related negative behaviors, survey participants were instructed to identify the stress-related negative behaviors that have the greatest impact on overall community health in their neighborhood. They were allowed to check a maximum of 5 behaviors from a list of 16 behaviors that were compiled from focus group sessions and previously described stress-related negative behaviors. 18
Survey Administration
In the Boston neighborhoods of Roxbury, Jamaica Plain, and Back Bay, 326 residents were surveyed. Surveys were administered in person in all 3 neighborhoods. A single research team member was present at the time of all survey administrations. In Roxbury and Jamaica Plain, participants were selected from local community health centers as well as a park in the community. Back Bay participants were selected from local primary care centers and a local park. Address of residence was verified in all participants to ensure they lived in the respective neighborhoods being studied.
Statistical Analysis
Demographic characteristics of survey participants included sex, ethnicity, and highest level of education completed. Comparisons between neighborhoods were made using χ2 tests. Mean age was compared using analysis of variance with pairwise comparisons based on Fisher’s least significant difference. Comparisons across neighborhoods were performed using Kruskal–Wallis (K–W) tests for Likert-type scale variables (neighborhood stressors and stress-related health problems) and χ2 tests to compare percentage of respondents endorsing stress-related negative behaviors with the greatest impact. For analysis of neighborhood stressors, we selected categories that had a mean of 2 or higher in at least 1 location. For analysis of negative stress-related behaviors, we selected behaviors that had a minimum of 20% of survey respondents identifying the behavior as negatively impacting community health in at least 1 of the 3 neighborhoods for analyses. All analyses were performed using SAS Statistical Software (SAS Institute, Cary, NC). Statistical significance was determined based on α = .05.
Results
There were 326 participants in this study of which 53% were men, and the mean age was 67 years. Demographic information of survey participants by neighborhood is shown in Table 1. Survey participants differed across the 3 neighborhoods in level of education, mean age, and race/ethnicity. The most stressful neighborhood characteristics were related to finances, safety, unequal treatment, diet, sleep, and exercise. By neighborhood, the highest stressors were as follows: (a) Roxbury—cost of living, “high drug, pill, and alcohol usage,” and discrimination (mean strength of stressor: 4.1, 3.8, and 3.0, respectively); (b) Jamaica Plain—housing costs, “high drug, pill, and alcohol usage,” and unsafe pedestrian/bike access (mean: 3.1, 2.8, and 2.0, respectively); and (c) Back Bay—unsafe pedestrian/bike access, lack of affordable fitness facilities, and noise pollution (mean: 3.2, 2.9, and 2.4, respectively).
Demographic Information of Participants Surveyed in the Boston Neighborhoods of Roxbury, Jamaica Plain and Back Bay.

Categories that are statistically significant across neighborhoods are depicted with an asterisk.
There were significant differences (P < .05) in neighborhood-level stressors across neighborhoods for 18 of the 27 questions (K–W test, P < .05) (Figure 2): stressors that were significantly different were high cost of living; unaffordable housing; high cost and/or poor access to parking; high cost and/or poor access to public transportation; high drug, alcohol, or pill usage; poor police presence; overly aggressive or unequal policing; discrimination; segregation; perceived safety; lack of suitable jobs; lack of access to affordable healthy food; lack of access to affordable fitness facilities; noise pollution; traffic congestion; unpleasant walking environment; unsafe pedestrian and bicycle access; and difficulty accessing social services (eg, childcare, health care, temporary job offices, etc.). The greatest perceived stress-related health problems by neighborhood were (Figure 3) as follows: (a) Roxbury—substance abuse, obesity, and gastrointestinal dysfunction (mean magnitude of health problem: 1.5, 1.4, and 1.0, respectively); (b) Jamaica Plain—substance abuse, insomnia, and obesity (mean: 1.4, 1.0, and 0.6, respectively); and (c) Back Bay—chronic pain, anxiety, and insomnia (mean: 1.2, 1.1, 1.1, respectively). There were significant differences in 8 of the 10 self-reported, stress-related health problems across the 3 neighborhoods (K–W test, P < .05): Significant neighborhood differences were observed in anxiety, chronic pain, addiction, obesity, irritability, insomnia, fatigue, and digestive problems, while depression and respiratory dysfunction were not different across neighborhoods.
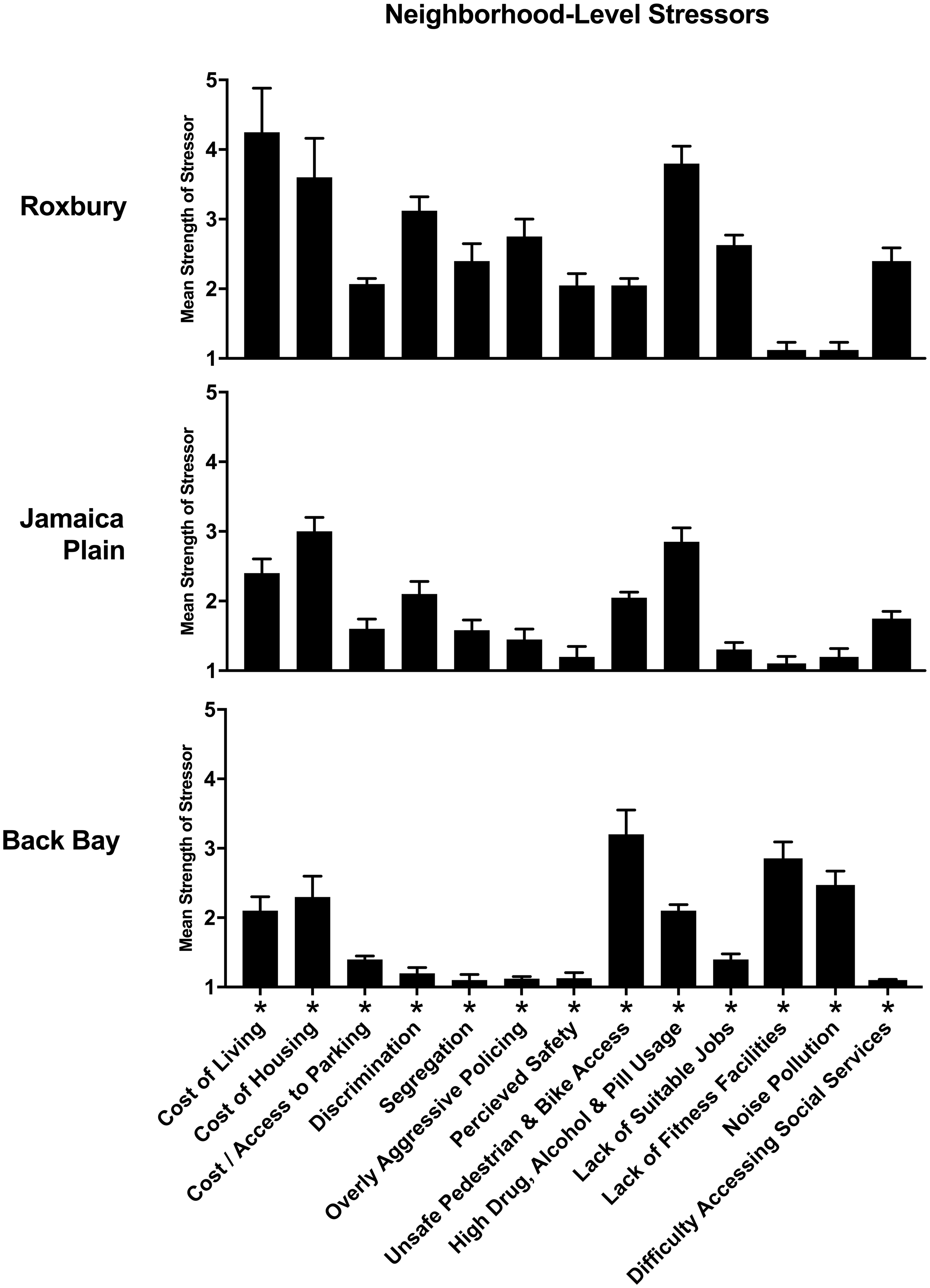
Self-reported Neighborhood-Level Stress Sources. Participants were asked to rate the neighborhood characteristics between 1 and 5—1 = “not stressful,” 5= “very strong stress source.” The mean strength of the stressor is shown on the y-axis. Standard deviations depicted. Only stressors with a mean of greater than or equal to 2 in at least one of the neighborhoods are depicted. Neighborhoods characteristics that are statistically significant across neighborhoods are depicted with an asterisk.

Self-reported Stress-Related Health Problems by Neighborhood. Participants were asked to identifying which stress-related health problem they have personally and to quantify how large of a problem it is—between 1 and 3—1 = “mild problem,” 2 = “moderate problem,” 3 = “large problem.” The mean strength of the stressor is on the y-axis. Standard deviations depicted. Health problems that are statistically significant across neighborhoods are depicted with an asterisk.
Stress-related negative behaviors also had unique imprints across the neighborhoods. The percentage of participants that identified a specific behavior as having the greatest impact on overall community health were significantly different in 12 of the 15 negative behaviors (χ2 tests, P < .05). Only domestic violence, sexual assault, and unfriendliness were not significantly different across neighborhoods (Figure 4).

Self-reported Stress-Related Negative Behaviors. Participants were asked to identify which stress-related behaviors were present in their neighborhood and have the greatest impact on overall community health. The percentage of survey participants that identified each stressor is shown on the y-axis. Only stressors with at least a 20% response rate in at least one neighborhood are shown. Behaviors that are statistically significant across neighborhoods are depicted with an asterisk.
Discussion
We believe that this is the first study to examine neighborhood stressors and stress-related behaviors and health outcomes across city neighborhoods. We found important differences across neighborhoods in how residents perceive neighborhood stressors as well as self-identified stress-related health problems and negative behaviors. These data reveal unique stress landscapes for these 3 geographically proximate neighborhoods. This is a particularly interesting finding given the striking nature of health disparities between neighborhoods that are equidistant to well-regarded academic medical centers; in addition, residents have equal access to health care due to long-standing policies such as the Massachusetts public health insurance program for low- to medium-income residents, MassHealth.19,20 If that is the case, then what other factors are serving as barriers to optimal health in Boston?
Our work suggests that the day-to-day stressors faced by the residents of Boston are strongly influenced by their geographic place of residence. This may partially explain some of the health disparities between these neighborhoods. In previous work, many of the neighborhood stressors that differ in the 3 neighborhoods of our study such as perceived discrimination, educational access, socioeconomic status, and environmental stress have been shown to have a negative impact on stress-related health disparities such as rates of asthma, hypertension, substance abuse, diabetes, obesity, and depression.21–26 However, our results are unique in that health insurance coverage mandates dating back to 2006 have achieved near-universal coverage and access for the residents in Massachusetts. 27 This suggests that the striking disparities across neighborhoods in Boston may be arising from other mechanisms such as the physical and social environment of neighborhoods, rather than more traditionally accepted explanations such as health access and cost.
Boston is a city that over the years has developed a true “culture of neighborhoods.” This is likely in part due to its history of segregation along racial, ethnic, and religious lines. Despite the neighborhoods of this study being less than 3 miles apart, each neighborhood has developed its own identity. It is plausible that this identity contributes to many different axes such as social capital, educational opportunities, values and priorities, social interactions, law enforcement, and the surrounding physical environment they experience. These factors likely influence residents’ interaction with the health-care system.
Our data demonstrate that residents of Boston experience these characteristics differently depending on their place of residence. A number of these findings predictably reflected economic disparities across the neighborhoods, with the more resource-limited neighborhood (Roxbury) listing high cost of living as its largest stressor, and the most affluent neighborhood in Boston (Back Bay) listing unsafe pedestrian and bike access. We also observed a potentially important dissonance between what residents perceived as stressors and what they perceive to be the stress-related health problems and negative behaviors in their neighborhood. Residents of Roxbury and Jamaica Plain rated health problems related to sleep, diet, and exercise among the largest problem affecting the health of their community. One would imagine that they would also describe neighborhood stressors that act as a barrier to good sleep hygiene, healthy diet, and exercisability. However, neighborhood characteristics related to sleep, diet, and exercise were among the lowest stressors reported in these neighborhoods. This dissonance in perceived stressors and health problems affecting community health suggests a blind spot in the pathway to disease manifestation. A possible explanation of this observation is that neighborhoods with higher rates of unmet social needs, such as Roxbury and Jamaica Plain, may be less likely to perceive stressors that are unrelated to basic necessity.28,29 If residents are unable to perceive stressors that may be influencing health problems in their community, there is little hope in affecting these potential upstream pathways. It is essential to further illuminate the relationship between neighborhood stressors and the resultant stress-related health problems and behaviors if we hope to empower residents to make meaningful changes that influence their health.
Our study has several limitations to consider. Most notably, our study was not randomized. About 70% of the survey participants were selected from community health centers in Roxbury and Jamaica Plain or from primary care offices in Back Bay. Differences in patient populations at community health centers and primary care offices could potentially confound some of the differences seen in the stress landscapes between the neighborhoods. In addition, we chose to have survey participants self-identify their stress-related health problems from a list of conditions, and it is possible that health records of participants could differ from the health problems they self-identified. Our study includes a number of strengths. We elicited exactly what factors of these Boston communities serve as stress sources from individuals that would know this best—the residents. We were able to examine the residents’ perception of what neighborhood characteristics and stress-related behaviors negatively affect their community, and we were able to contrast these findings with what stress-related health problems they experience personally.
Despite spending more in the health-care sector, the United States still trails behind high-income nations in many health measures, including rates of cardiovascular disease, obesity, diabetes, and self-reported stress levels. 30 While much focus has been placed on mitigating the impact stress has on individuals, there have been few interventions aimed specifically at alleviating stressors that are structurally and socially embedded into neighborhoods. Understanding how these factors are uniquely intertwined within neighborhoods and communities is essential in identifying areas of intervention to reduce the negative effect of stress in health and disease. Our study extends current neighborhood health research by investigating how specific structural and social determinants of health can be embedded within specific neighborhoods and how the stress-related behavior and health morbidities can be distinct despite small geographic separation between neighborhoods. Our results suggest that the health of communities could benefit from tailored, neighborhood-level interventions that aim to reduce the unique stress burden that is present in neighborhoods. Further work is needed to elucidate how the unique stress landscape of a neighborhood can influence the health outcomes and behavior of its residents.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.