
Abstract
Objectives
Despite the enormous prevalence of autism spectrum disorder (ASD), its global impact has yet to be realized. Millions of families worldwide need effective treatments to help them get through everyday challenges like eating, sleeping, digestion, and social interaction. Qigong Sensory Training (QST) is a nonverbal, parent-delivered intervention recently shown to be effective at reducing these everyday challenges in children with ASD. This study tested the feasibility of a protocol for investigating QST’s neural mechanism.
Methods
During a single visit, 20 children, 4- to 7-year-old, with ASD viewed images of emotional faces before and after receiving QST or watching a video (controls). Heart rate variability was recorded throughout the visit, and power in the high frequency band (0.15–0.4 Hz) was calculated to estimate parasympathetic tone in 5-s nonoverlapping windows. Cerebral oximetry of prefrontal cortex was recorded during rest and while viewing emotional faces.
Results
95% completion rate and 7.6% missing data met a priori standards confirming protocol feasibility for future studies. Preliminary data suggest: (1) during the intervention, parasympathetic tone increased more in children receiving massage (M = 2.9, SD = 0.3) versus controls (M = 2.5, SD = 0.5); (2) while viewing emotional faces post-intervention, parasympathetic tone was more affected (reduced) in the massage group (p = 0.036); and (3) prefrontal cortex response to emotional faces was greater after massage compared to controls. These results did not reach statistical significance in this small study powered to test feasibility.
Discussion/Conclusion
This study demonstrates solid protocol feasibility. If replicated in a larger sample, these findings would provide important clues to the neural mechanism of action underlying QST’s efficacy for improving sensory, social, and communication difficulties in children with autism.
Keywords
Introduction
Background and Significance
Despite the enormous prevalence of autism spectrum disorder (ASD), with estimates ranging from 1 in 45 1 in the United States to 1 in 160 2 worldwide, its global impact has yet to be realized. Autism is a bio-neurological developmental disability generally appearing before the age of 3 that impacts normal development of the central nervous system (CNS) in the areas of social interaction, communication skills, and cognitive function—collectively referred to as executive function. 3
In addition to impaired CNS development, individuals with autism often suffer from numerous comorbid medical conditions associated with largely involuntary functions mediated by the autonomic nervous system (ANS) such as heart rate, respiration, emotional arousal, digestion, and sleep.4–8 These and other ANS-mediated functions are regulated by the constantly shifting tone between 2 divisions of the ANS: the sympathetic (“fight or flight”) nervous system responsible for responding to high-salience situations, and the parasympathetic (“rest and digest”) nervous system responsible for nonemergency maintenance functions. 8 Although many CNS structures involved in ANS control are known to be abnormal in autism, including amygdala and hypothalamus,9–13 the exact nature of the relationship between ANS and CNS function in children with autism has not been well characterized to date. 14 Massage therapy has been shown to affect ANS activity by increasing parasympathetic tone.15,16 Thus, understanding interactions between ANS and CNS activity in the context of interventions for autism such as massage has important implications for both (1) understanding neural underpinnings of autism and (2) improving clinical outcomes of children with autism.
Sensory Dysregulation in Autism
In addition to the previously described symptoms and conditions, people with autism frequently experience sensory abnormalities, and it is becoming increasingly clear that sensory difficulties are intrinsically linked with many of the struggles faced by children with autism.
17
For instance, estimates of the prevalence of sensory symptoms of people with ASD range from 69% to 93% in children and adults
18
and were recently added as a diagnostic criterion of ASD in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-V). Although the full nature of the relationship between sensory abnormalities and autism is not yet clear, a neural pathway recently implicated in auditory sensitivity of children with autism
19
may be involved. This pathway, termed the nonclassical auditory pathway by Moller and Rollins,
20
is illustrated along with its classical counterpart in Figure 1. The key difference between the 2 pathways is that while one travels directly to primary sensory cortex from thalamus (classical), the other (nonclassical) travels through limbic structures known to be well-connected with ANS, including amygdala and hypothalamus, before reaching cortex, thus allowing sensory input to modulate ANS activity via amygdala and hypothalamus. A parallel tactile pathway is known to exist,
21
but whether it plays a role in the tactile dysregulation experienced by children with autism has not yet been established.
Nonclassical auditory and tactile neural pathways include limbic system (left) in contrast to classical paths to primary sensory cortex (gray arrow on right) (diagram adapted from Noise and Health, 2000, http://www.noiseandhealth.org/viewimage.asp?img=NoiseHealth_2000_2_7_49_31742_1.jpg).19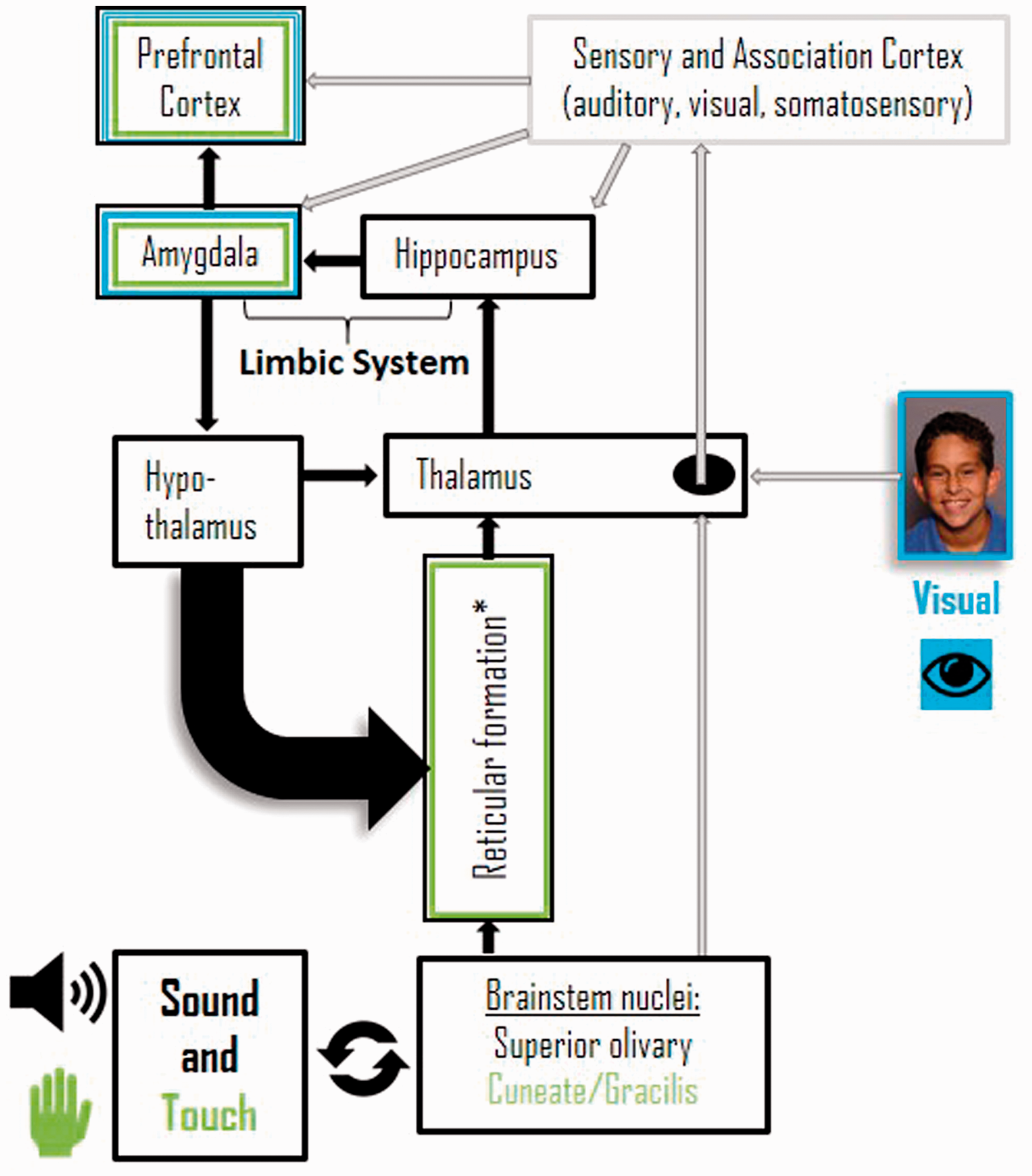
{kind=link}
Qigong Sensory Training
Qigong Sensory Training (QST) is a specific massage protocol derived from Traditional Chinese Medicine for children with ASD. 22 QST is carried out by parents for 15 to 20 min each day and supported by a trained therapist once a week for the first 20 weeks. Silva et al.23–27 tested this methodology in multiple clinical trials documenting QST’s safety and efficacy over the past 12 years. Their most recent 24-month follow-up study reported marked improvements in tactile responses (normalized by 72%, with 32% falling into normal range by 24 months from initiation of treatment). They also reported significant normalization of nontactile sensory responses, ANS-controlled functions including sleep and digestion, and CNS-controlled functions including social interaction and receptive/expressive language. Mean autism severity assessed using the Childhood Autism Rating Scale 28 was reported to decrease by 44%, with 26% of children moving out of autistic range during the course of this 2-year study. 29
Study Focus
This study sought to provide a first step toward generating specific hypotheses regarding the neural mechanisms underlying QST’s reported efficacy for improving both ANS-controlled and CNS-controlled symptoms of autism. In the process, we seek improved understanding of the relationship between ANS-controlled symptoms (including sleep, digestion, and emotional arousal) and CNS-controlled symptoms (including social, communicative, and sensory symptoms) in children with autism. Toward this long-term goal, the current study aimed to (1) assess feasibility of a study protocol designed to investigate the effect of a single QST treatment session on both CNS and ANS activity during an emotional processing task and (2) collect preliminary data to generate hypotheses of the neural mechanism of QST for improving symptoms of children with autism.
Methods
The following methods were reviewed and approved by the University of North Carolina at Chapel Hill Institutional Review Board.
Study Preparations
Twenty children, 4- to 7-year-old, were recruited using university-wide, institutional Review Board-approved emails directing potential participants to the study website. To be included, families were required to (1) provide written documentation of their child’s age and the diagnosis of ASD, (2) arrange to have one parent available to be present with the child throughout the single, 90-min study visit, and (3) indicate that the child was able to follow verbal or gestural instructions such as, “Please sit down” or “Please put your hand here,” with parent assistance. Children who had experienced any seizures within the past 12 months were excluded. Medications and additional conditions or limitations beyond ASD were recorded. Parents completed the sensory portion of the Sense and Self-Regulation Checklist 30 and were sent a reminder email a few days before their visit with a link to a social story of the upcoming study visit to review with their child.
Measure Selection
We selected one measure (listed in parentheses) for exploring each of 3 demonstrated areas of clinical improvement following treatment with QST: (1) nontactile sensory normalization (auditory sensitivity to noise), (2) ANS-controlled regulation functions such as digestion and sleep (parasympathetic tone, calculated from heart rate variability [HRV]), and (3) CNS-controlled functions requiring information synthesis such as social interaction, communication, and emotional processing (prefrontal cortex [PFC] activity in response to viewing emotional faces, measured with cerebral oximetry).
Expected Results
In vivo intracellular and juxtacellular electrophysiological studies in rodents suggest that basolateral amygdala stimulation inhibits PFC via local inhibitory interneurons.31,32 It is also known that under stress, human amygdala output is increased, inhibiting PFC,
33
and that inhibition of this part of the brain leads to increased use of oxygen,
34
probably by local inhibitory interneurons. Thus, we expected that:
During QST, the opposite would occur. That is, nonstressful tactile stimulation would lead to decreased amygdala output, with resulting disinhibition of PFC reflected in decreased use of oxygen; and, During viewing of emotional faces, a task requiring processing by PFC,35,36 more inhibitory interneuron activity compared to rest periods would lead to increased use of oxygen. We did not anticipate the effect of massage on this process.
Study Visit
After receiving written parental consent, 2 cerebral oxi-metry sensors (left and right side of the forehead) and 2 cardiac sensors attached to a wireless, Firstbeat Bodyguard 2 HRV monitor were applied per device instructions.
Video recording began and participants were presented with recordings of crowd/restaurant noise via headphones, 37 having been instructed with the help of the parent, to indicate when the sound “gets too loud or starts to bother you.” The volume was increased by 10% every 5 s until the child indicated the threshold had been reached by raising a hand.
Baseline PFC oxygenation was recorded for 5 min with a Somanetics INVOS 5100C cerebral oximeter, after which children were presented with 120, randomly ordered images of children with angry, sad, happy, or neutral facial expressions on a computer screen in four 2-min blocks with 1 min rest between blocks. Valid and reliable images were obtained from the Child Affective Facial Expression set (CAFE). 38
Then the child either received the QST massage, administered by a licensed massage therapist, certified in delivering the Qigong Sensory Training protocol described in detail elsewhere 22 or watched a video of the massage, followed by a second 5-min rest period and presentation of emotional faces. After viewing the faces for the second time, the child received the intervention not yet received.
Feasibility Data.

Data Analysis
Statistical analyses were performed using SPSS (V. 24.0) and STATA SE v.15.
Auditory sensitivity
To assess differences in auditory sensitivity between conditions, means and standard deviations were calculated for each intervention group. In addition, the number of subjects demonstrating increased sensitivity to sound (lower volume threshold), decreased sensitivity, or no change was calculated for each intervention group.
PFC activity
Separate 2 by 2, condition (massage/video) by time (pre/post) multivariate analyses of variance (M-ANOVAs) were performed to assess differences in cerebral oxygenation between conditions in the left and right PFC. In addition, separate 2 by 2, condition (massage/movie) by time (immediately preceding rest period/presentation of emotional faces) M-ANOVAs were performed to assess differences in cerebral oxygenation between conditions in the left and right PFC for each emotion separately and combined over emotional blocks.
Parasympathetic tone
Interbeat interval data were analyzed in a series of 5-min windows corresponding to the pre/post rest periods, presentation of emotional faces (one window), and intervention (video and massage). Using HRV software (Kubios HRV Standard, 3.0.0), fast-Fourier transforms (FFTs) were calculated and 50% window overlap was used to estimate power in the high frequency band (0.15–0.4 Hz). Means and standard deviations of high frequency power were calculated for the rest, emotional faces, and intervention periods. Log transformations of these values were calculated to normalize variance across subjects. Time and condition interactions were assessed using a linear regression model. In addition, the time series curve of high frequency power during each intervention was fit with a quadratic regression model to assess changes in parasympathetic tone over time. We evaluated the trajectory of change in HRV using a random effects model with a quadratic term to compare the massage and video groups.
Results
Recruitment and Feasibility
Out of 44 people expressing interest, 26 people completed the screening survey, and the first 20 who were eligible were scheduled (Table 1). Two people cancelled prior to their study visit; there were no missed appointments (“no-shows”). All but one visit was completed in less than 2 h. In the exit survey (Table 1), all participants (n=20) indicated they would like to be contacted about future studies. 95% (19/20) responded “Yes” to the question, “Would you like to bring your child back for additional massage sessions, if there were 2 research sessions like this and 8 other sessions with massage only or massage resting measurements?” The positive aspects of the study most reported were the massage itself (11), watching how the child responded to the massage (3), watching the child relax (3), and learning ways to help the child relax (3). The negative aspects of the study most cited were watching the images of emotional faces, especially the sad ones (5) and sticker/sensor removal (3). Ten families chose to send descriptions of their child during the 48 h following the study visit (50%). The most common responses involved increased sleep (5), being more relaxed (4), and increased irritability/hyperactivity (3). Other responses included increased bowel movements and acceptance of new foods.
Participant Characteristics
Sensory Scores from Sensory and Self-Regulation Checklist.
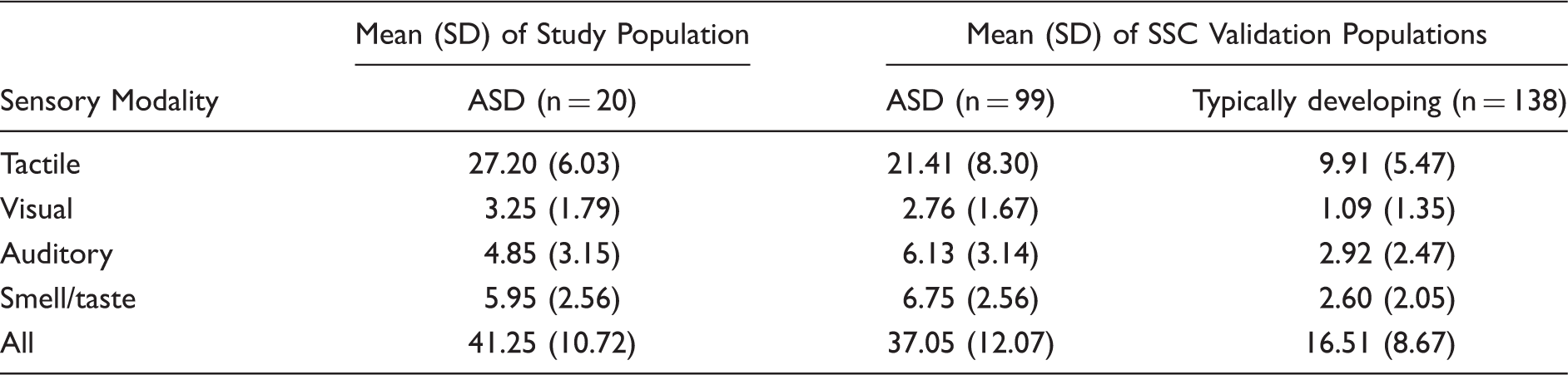
ASD: autism spectrum disorder; SSC: Sensory and Self-Regulation Checklist
Nontactile Sensory Changes/Auditory Sensitivity
Missing data (25%) were mostly due to discomfort with the headphones. Auditory thresholds for both the massage and the video groups were lower after the intervention (means of 11.8 and 11.7, respectively). However, 89% of the massage group (n = 9) showed a post-intervention change in threshold compared to only 50% of the video group (n = 6).
ANS Activity/Parasympathetic Tone
Missing data (6.25%) were due to technical malfunction due to staff error (incomplete adhesive removal for one sticker and use of older sensors for first subject led to poor conductivity) and one incomplete study visit terminated due to child anxiety.
Log transformations of mean power in the high frequency band (0.15–0.4 Hz) during the massage and video interventions are shown in Figure 2. During the first 3.5-min analysis window, the means of the video and massage groups were nearly identical at 2.60 (SD = 0.31) and 2.58 (SD = 0.46). They continued to be very close for the first 7 min, but the parasympathetic tone began to increase more in the massage group than the video group beginning at 7 min and reaching their maximal difference just after the halfway time of the interventions, at which point the means of the massage and video groups was 2.85 (SD = 0.30) and 2.47 (SD = 0.50), respectively. Means for the group who received massage after viewing the video are shown in gray. Although they show the same shape, peaking during the fourth data window, the starting point is higher (2.92, SD = 0.36), possibly because it was later in the visit and so the participants had more time to become acclimated to the environment.
Group mean parasympathetic tone (log10 of high frequency power) during QST massage (blue and gray) or while watching a video about QST massage (orange). The blue and orange groups were treated identically until the start of the intervention (0:00). About 7 min into the intervention, the groups began to diverge, with the measure of parasympathetic tone (HF power) decreasing for the video group and continuing to increase slightly for the massage group. The gray group includes the same children as the orange group, who received the massage at the end of the study visit. We evaluated the trajectory of change in heart rate variability, comparing the massage and video groups (blue and orange lines) using a random effects model with a quadratic term. The model suggested that the trajectories of the 2 groups were different, but the difference did not reach statistical significance at the 0.05 alpha level in this small study, powered for feasibility testing.
Heart Rate Variability Results.

CNS Activity/PFC Oxygenation
Missing data (9%) were due to technical malfunction related to cerebral oximetry (bad sensor, loose cable connection) and the one incomplete study visit due to child anxiety.
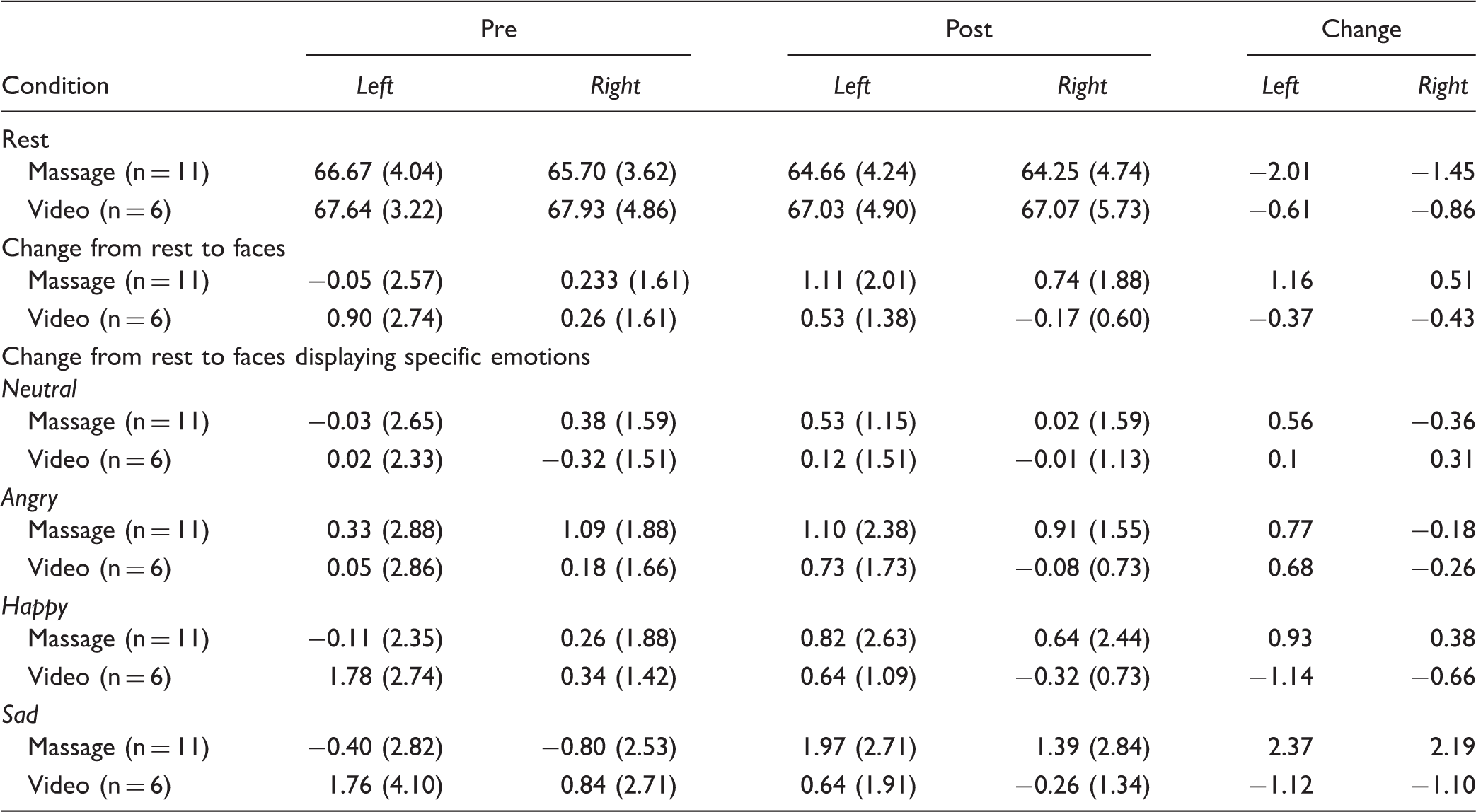
Overall, both the video and massage groups showed a mean decrease in PFC oxygenation during rest after the intervention compared to baseline that mirrored the gradual increase in parasympathetic tone (left column of Figure 3). Although the decrease was more pronounced in the massage group, this difference did not reach statistical significance. Compared to rest, mean PFC oxygenation while viewing emotional faces post-intervention (all blocks combined) decreased slightly for the video group, but increased for the massage group (right column of Figure 3).
Comparison of group means and standard errors (next to each endpoint) of CO and HRV measures before and after receiving QST massage (blue) or watching a video about QST massage (orange). The left column shows CO drifting downward (indicating less inhibitory activity) over time during rest, while HRV (high frequency power) increases slightly, indicating greater parasympathetic tone. These changes are seen equally for both groups and likely reflect gradual relaxation as they adapt to the study environment. In contrast, the right column, which shows the mean change from the preceding rest period to the period of viewing emotional faces (to control for drift), shows the groups diverging. While the video group mean reflected a pattern of relaxation (less inhibition, lower oxygen use) or remained the same (HRV), the massage group mean change showed increased CO (more inhibition, more processing) and lower parasympathetic tone while viewing emotional faces. Except for the change in HRV from rest to faces (bottom right, p = 0.036), none of the groups are statistically distinct in this small sample. However, patterns in mean changes may be useful for generating hypotheses to be tested in subsequent studies.
Mean Percent Oxygenation of Prefrontal Cortex.
Observed Behavior
It appeared to study staff that children tended to avoid looking at the faces with negative emotional tone following massage, and many became visibly agitated. Several children actually burst into tears after (not before) massage when viewing angry or sad faces. None of the children in the video group did this or were noted to avoid looking at sad or angry faces.
Discussion
Feasibility
The primary aim of this study was to assess protocol feasibility. Ease of recruitment, high rate of completed study visits (95%), and low amount of missing data (7.6% overall) indicate that the methodology of this study is highly feasible. Factors that may have contributed to its feasibility included creation of a social story to prepare participants for the study visit, selection and development of comfortable, noninvasive measures and methodology, and preparation of appropriate study facilities (see Methods).
Hypothesis-Generation
The secondary aim of this study was to generate preliminary data for hypothesis-generation. Although the study was powered for testing feasibility rather than hypotheses, and few of our results reached statistical significance, key findings useful for hypothesis-generation included: (1) increased parasympathetic tone during QST and (2) decreased parasympathetic tone in response to emotional faces after massage. In addition, decreased parasympathetic tone during emotional faces after massage was accompanied by increased mean PFC oxygenation, suggesting work was being done by inhibitory interneurons (see Measure Selection subsection). 34 These results are consistent with parents’ report of increased irritability during the 24 to 48 h following their study visit. Together, these findings suggest increased sensory and emotional sensitivity following the single application of QST. Combining our preliminary data with the clinical findings of others, we hypothesize that the flood of nonsalient tactile input provided by QST leads to (1) decreased amygdala stimulation of PFC inhibitory interneurons, resulting in greater PFC sensitivity, and (2) a change in hypothalamic activity that results in increased parasympathetic tone.
Interpretation of Results
Placing our results in the context of previous studies, it is important to note that while previous studies of QST observed greater emotional stability at 5, 9, 12, and 24 months after initiating QST, we observed less emotional stability after a single QST massage. To explain this apparent discrepancy, we considered a possible training effect over time. That is, decreased PFC inhibition after a single massage, associated with less emotional stability, could encourage dendritic growth in PFC over weeks and months that allows children to selectively manage emotions more effectively over time. These new connections could serve to offset documented reductions in the rate of PFC dendritic growth observed in children aged 2 to 9 with autism 39 which coincide precisely with the usual time of rapid development of dendritic arbors of pyramidal neurons in layer III. 40 This interpretation is consistent with improved emotional stability and social interaction reported after 5 months of daily QST. Our ANS results coincide with the literature in that the increased parasympathetic tone observed during a single session of QST is consistent with previously reported ANS-controlled clinical changes following 5 months of QST, including improved digestion and sleep.
Limitations
The primary limitations of this study were its small sample size, which precluded drawing any statistical conclusions beyond protocol feasibility, and the fact that there was only one study visit. Less significant limitations included: (1) difficulty determining auditory thresholds in this population, (2) lost data due to detachment of cerebral oxygenation sensors when children moved, and (3) lack of eye tracking. In reviewing the study video, it seemed that after massage, children tended to avoid direct eye contact with those photos of children displaying angry and sad emotions. Thus, eye tracking would be useful in future studies for quantifying time spent looking at the emotional faces, especially the eyes.
Future Studies
In addition to verifying the reliability of these observations in larger groups over a longer course of treatment, we plan to directly address study limitations and investigate the hypothesis generated by this study. In a study with multiple study visits and a longer course of treatment, we anticipate that shifts to parasympathetic tone noted in this study would likely be amplified due to development of familiarity with study staff, facilities, and procedures, as well as the massage itself.
Implications and potential benefits of this line of research include the following: (1) Having a clear understanding of QST’s mechanism of action will be helpful to clinicians preparing a comprehensive treatment plan for children with autism in the same way knowing a medication’s mechanism of action is helpful to clinicians pairing it with other medications or treatments; and (2) the noninvasive, lightweight, wireless technology and methods of this line of research are being optimized for future field use training practitioners and evaluating implementation of QST and other interventions. If the proposed hypothesis is supported in future studies, it would underscore the importance of early intervention and provide a specific method for stimulating needed PFC development in children with autism.
Conclusion
This study demonstrates solid protocol feasibility. If replicated in a larger sample, these findings would provide important clues to the neural mechanism of action underlying QST’s efficacy for improving sensory, social, and communication difficulties in children with autism.
Footnotes
Acknowledgments
Special thanks are given to Eric Hodges and Brant Nix of the Biobehavioral Laboratory in the University of North Carolina’s School of Nursing for managing outstanding study facilities with the highest professional standards.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the North Carolina Translational Clinical Sciences Institute.